Abstract
(1) Background: Fluid resuscitation is a necessary part of therapeutic measures to maintain sufficient hemodynamics in extracorporeal membrane oxygenation (ECMO) circulation. In a post-hoc analysis, we aimed to investigate the impact of increased volume therapy in veno-arterial ECMO circulation on renal function and organ edema in a large animal model. (2) Methods: ECMO therapy was performed in 12 female pigs (Deutsche Landrasse × Pietrain) for 10 h with subsequent euthanasia. Applicable volume, in regard to the necessary maintenance of hemodynamics, was divided into moderate and extensive volume therapy (MVT/EVT) due to the double quantity of calculated physiologic urine output for the planned study period. Respiratory and hemodynamic data were measured continuously. Additionally, renal function and organ edema were assessed by blood and tissue samples. (3) Results: Four pigs received MVT, and eight pigs received EVT. After 10 h of ECMO circulation, no major differences were seen between the groups in regard to hemodynamic and respiratory data. The relative change in creatinine after 10 h of ECMO support was significantly higher in EVT (1.3 ± 0.3 MVT vs. 1.8 ± 0.5 EVT; p = 0.033). No major differences were evident for lung, heart, liver, and kidney samples in regard to organ edema in comparison of EVT and MVT. Bowel tissue showed a higher percentage of edema in EVT compared to MVT (77 ± 2% MVT vs. 80 ± 3% EVT; p = 0.049). (4) Conclusions: The presented data suggest potential deterioration of renal function and intestinal mucosa function by an increase in tissue edema due to volume overload in ECMO therapy.
1. Introduction
Extracorporeal membrane oxygenation (ECMO) is frequently used in clinical practice for various indications [1]. The initial phase of ECMO therapy might be difficult to manage because of inadequate ECMO flow and severe hemodynamic decline [2,3]. Fluid resuscitation is a necessary part of therapeutic measures to maintain sufficient hemodynamic and ECMO circulation. Pathophysiologic conditions, such as shock, low cardiac output, and sepsis-like syndromes, additionally influence the requirement for volume administration [4]. Moreover, increased capillary leakage is known to contribute to a higher demand for fluids [5]. Several sepsis studies demonstrated the negative impact of excessive volume administration on the outcome of these patients [6,7,8,9,10,11]. In contrast, only a few clinical reports shed some light on the specifics of ECMO therapy and the impact of fluid resuscitation on patient outcomes [12,13,14]. In this regard, fluid overload was identified as having a negative impact on outcomes, especially in pediatric ECMO patients [15]. For adult veno-venous ECMO patients, a negative cumulative daily fluid balance was associated with improvement of respiratory function [16]. Therefore, balanced fluid management in ECMO patients is crucial to avoiding adverse outcomes. In this regard, several strategies are in use to assess fluid requirements in critically ill adults, such as fluid challenge [17], inferior vena cava assessment [18,19], passive leg raising [20], and end-expiratory occlusion maneuver [21].
A particular focus of the underlying study was to investigate the impact of increased volume therapy in ECMO circulation on organ edema by analyzing retrospective data from a large animal experimental protocol performed by our study group.
2. Materials and Methods
The study performed is a retrospective, not pre-planned, subanalysis of one particular study arm, which was part of a large animal experimental protocol investigating concomitant extracorporeal membrane oxygenation (ECMO) and intra-aortic balloon pumping (IABP) and was approved by the responsible ethical committee for animal care of the University of Cologne (LANUV, Bonn, Northrhine-Westphalia, Germany) [22]. Data were prospectively collected. The Koeln Fortune Program (343/2015), Faculty of Medicine, University of Cologne, funded this research. The experimental protocol and subsequent analysis were performed between May 2017 and December 2021 at the Experimental Medicine institute of the Faculty of Medicine Cologne and the Department of cardiothoracic surgery of the University Hospital Cologne. The study arm investigated in this report included twelve healthy pigs with ECMO circulation for 10 h.
2.1. Experimental Protocol
Twelve female pigs (Deutsche Landrasse × Pietrain) were included in this study. Animals were premedicated with xylazin (2 mg/kg), tiletamin (10–12.5 mg/kg i.m.), and zolazepam (10–12.5 mg/kg i.m.). Deep sedation was induced with the intravenous application of propofol (1.5–2.5 mg/kg). Neuromuscular blockade was achieved with pancuronium (0.2 mg/kg i.v.). After endotracheal intubation, continuous anesthesia and analgesia were maintained with the intravenously administered propofol (4–6 mg/kg/h), midazolam (0.96–1.2 mg/kg/h), and fentanyl (0.012–0.025 mg/kg/h). Animals were ventilated with volume-controlled ventilation (Fabius GS, Dräger, Luebeck, Germany) using an air/oxygen mixture adjusted to keep arterial blood gas values in the physiologic range (partO2 100–150 mmHg, partCO2 35–45 mmHg, pH 7.35–7.45).
2.2. Placement of Measurement Catheters
Appropriate parts of the body were sterilized. A urine catheter was placed surgically into the bladder. The body temperature was measured through a rectal catheter. Afterwards, the right jugular vein and carotid artery were cannulated for measurements of the central venous pressure (8.5 Fr., Arrow International, Reading, PA, USA), the mean arterial pressure (20 G Leadercath, Vygon, Aachen, Germany), and for blood sampling. A contralateral carotid artery was prepared, and carotidal blood flow was measured by a transit time flow probe (Transonic Systems, Inc., New York, NY, USA). After sternotomy and pericardial incision, the pulmonary artery was cannulated for blood sampling and for pulmonary artery measurements (20 G Leadercath, Vygon, Aachen, Deutschland). Pressure transducertip catheters (Model SPC-350S, Millar Instruments, Inc., Houston, TX, USA) were placed into the right and left ventricles. Cardiac output (CO) was recorded by a transit time flow probe (Transonic Systems, Inc., New York, NY, USA) placed around the ascending aorta.
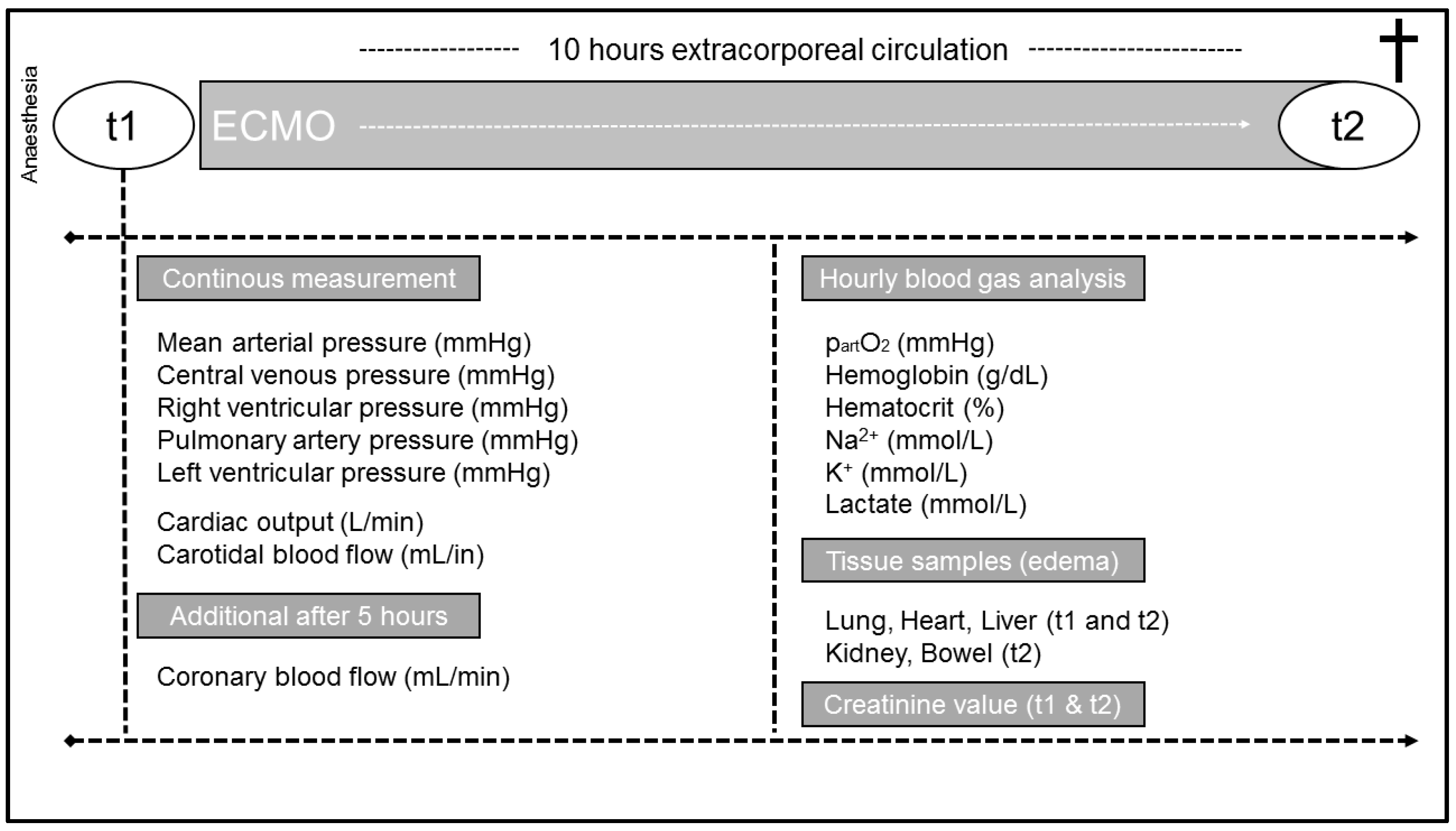
ECMO cannulas (HLS cannula, Getinge, Rastatt, Germany) were implanted through groin vessels (arterial: 17 Fr.; venous: 21 Fr.). Heparin was applied intravenously as an anticoagulant drug. Extracorporeal circulation (BIO MEDICUS Medtronic 540 Bio Console, Medtronic, Dublin, Ireland) was started after initial measurements and sampling of baseline parameters. An additional heater (BIO MEDICUS Medtronic BIO-CAL 370, Medtronic, Dublin, Ireland) was implemented into the ECMO circuit. The study protocol ended 10 h after the initiation of ECMO therapy (Figure 1). Animals were euthanized by applying an overdose of pentobarbital (80 mg/kg).
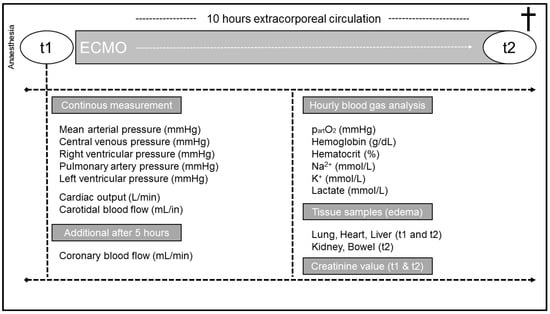
Figure 1.
Flow chart of the study protocol and assessed parameters.
2.3. Hemodynamic Measurements
Hemodynamic measurements were performed during stable hemodynamic and respiratory conditions before extracorporeal circulation (t1) and 10 h after initiation of ECMO circulation (t2). All data were digitalized at a rate of 500 Hz using a 16-channel hemodynamic set-up and subsequently analyzed (Hugo Sachs Elektronik-Harvard Apparatus GmbH, March-Hugstetten, Germany).
2.4. Laboratory Parameters
Blood gas analysis was performed hourly. Additionally, creatinine values were sampled and analyzed for t1 and t2.
2.5. Target Parameters and Settings during ECMO Circulation
Particular hemodynamic and respiratory parameters during ECMO circulation were targeted as follows:
ECMO-flow → 50 mL/kg/min/m2 (indexed)
MAP → 60–70 mmHg
partO2 → 120–200 mmHg
2.6. Fluid Resuscitation during ECMO Circulation
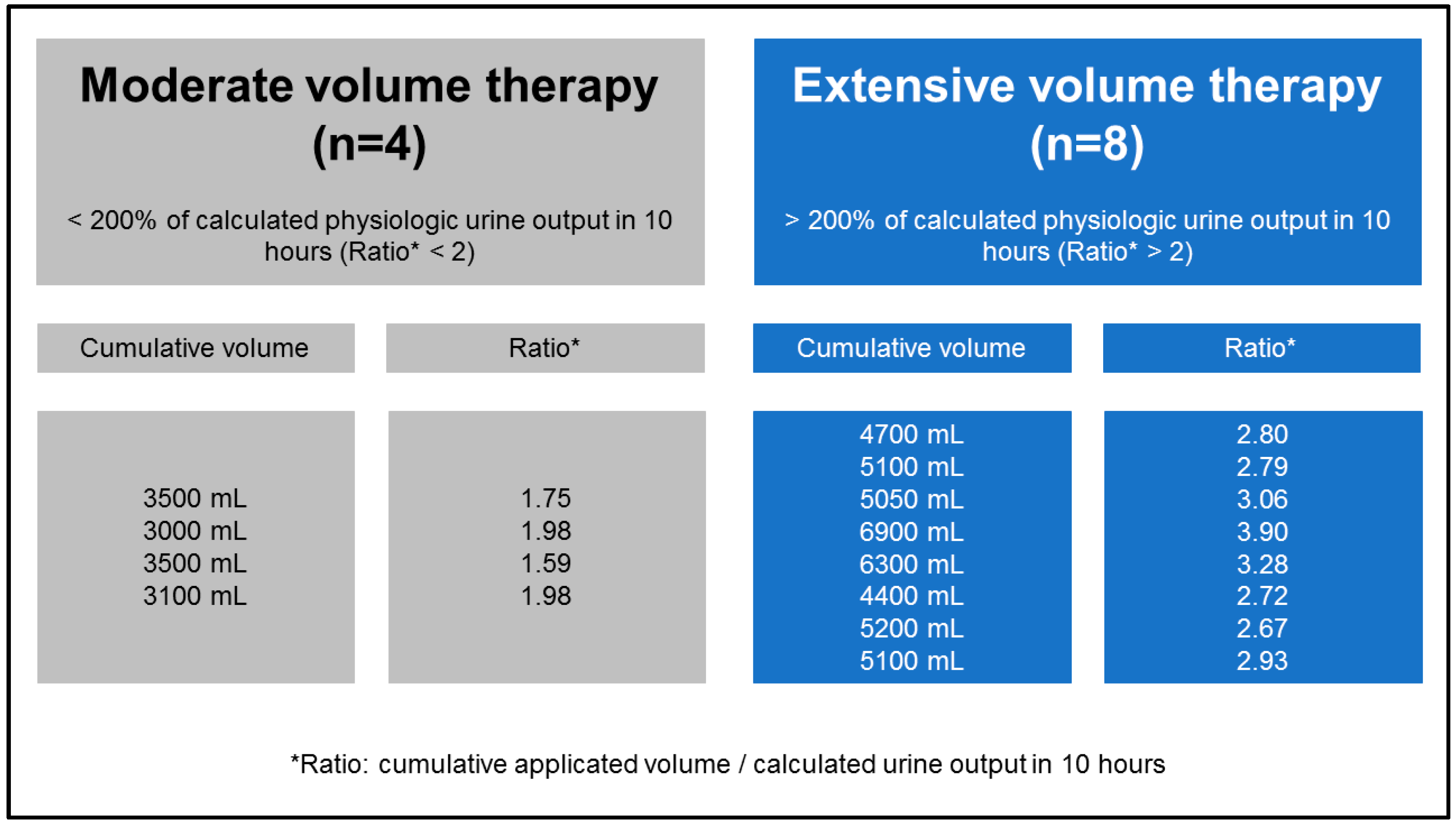
To maintain targeted mean arterial pressure, a fluid resuscitation protocol was tracked with a ratio of colloids and crystalloids of approximately 1:3. The study protocol strictly excluded blood transfusions. As the animals included in the previous investigation were retrospectively analyzed, the full population was divided into pigs who received moderate volume therapy and those receiving extensive volume therapy (Figure 2). The criteria used for allocating pigs to cohorts was the scaling of volume application, which was based on the double quantity of calculated physiologic urine output (0.05 mL/kg/min) for the planned study period [23].
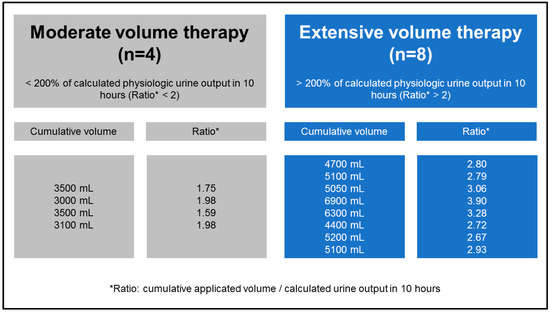
Figure 2.
Presentation of groups after dichotomization in moderate and extensive volume therapy.
2.7. Organ Edema
The primary outcome of this study was the relationship between organ edema. Tissue samples of the lung, heart, and liver were obtained at t1 and t2, and tissue samples of the kidneys and bowel were obtained only at t2. Probes were weighed (wet weight) and then freeze-dried after lyophilization. Dry weights were measured after the incubation of specimens at 110 °C for 2 days and corrected for residual water content. Organ edema was calculated by using the formula: % tissue water = (wet weight dry weight) wet weight and expressed as a percentage of the wet weight. All measurements were performed in duplicate, and the average was taken to balance the influence of hydrostatic distribution on the different organ tissue water contents.
2.8. Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences, version 23.0 (SPSS IBM, Chicago, IL, USA). Data were evaluated for normality using one sample Kolmogorov-Smirnov test and expressed as the mean ± standard deviation. Univariate analysis was performed using either the Student t or Mann-Whitney U test for normally and non-normally distributed continuous variables, respectively. p-values < 0.05 were considered statistically significant.
3. Results
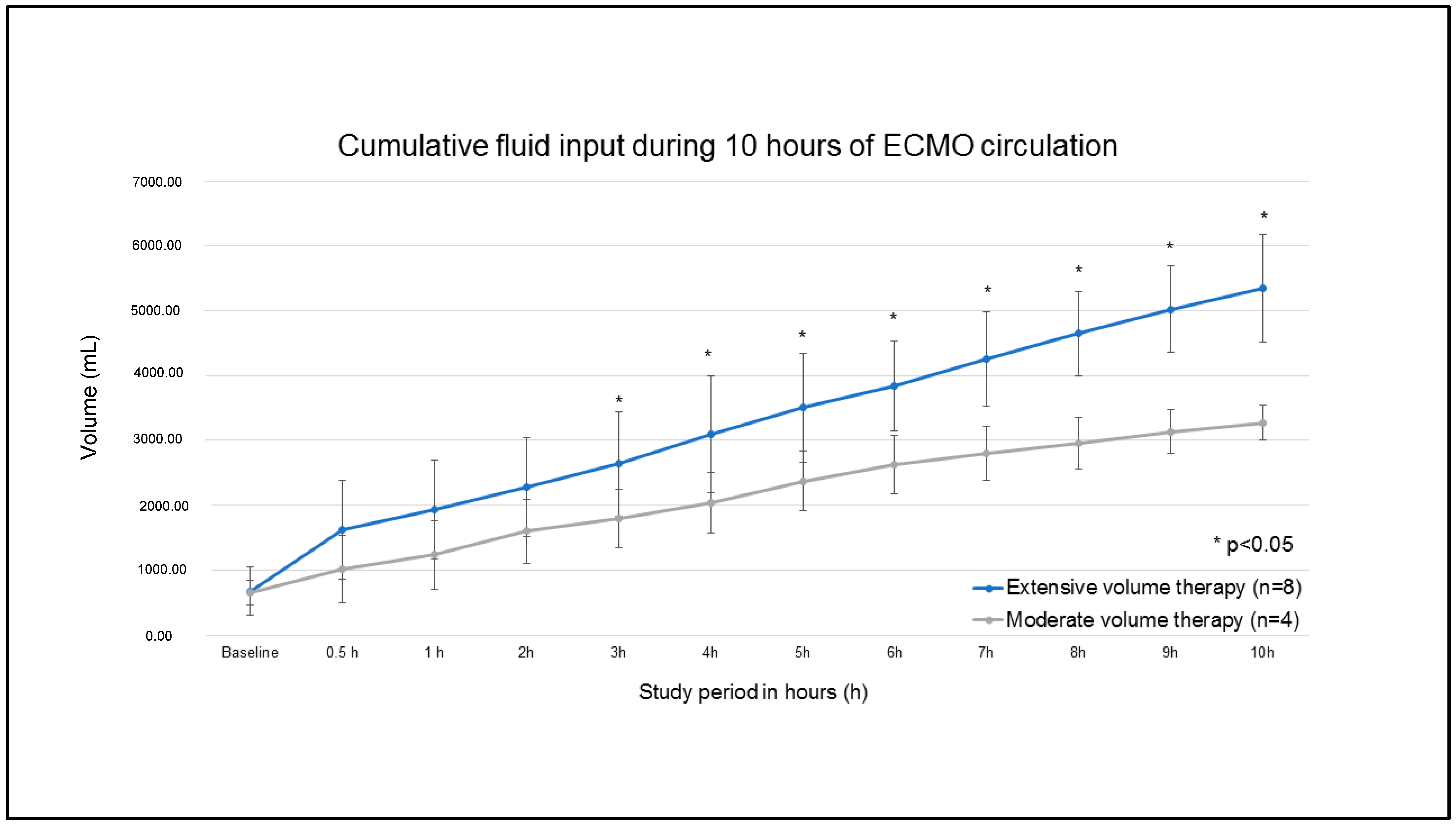
After dichotomization of fluid administration within the study period, four pigs were included in the moderate volume therapy (MVT) group, and eight pigs were analyzed in the extensive volume therapy (EVT) group (Figure 2). Cumulative volume administration differed significantly after the third hour of ECMO circulation (Figure 3). Cumulative fluid administration after 10 h of ECMO circulation (t2) was significantly different (3275 ± 263 mL MVT vs. 5344 ± 834 mL EVT; p < 0.01).
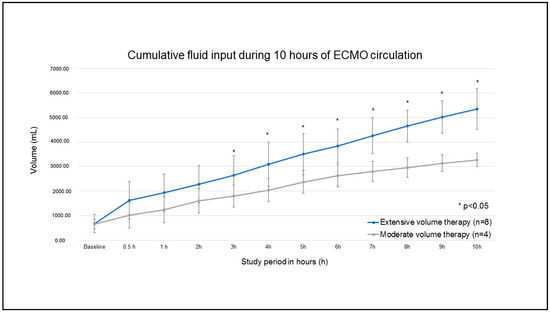
Figure 3.
Cumulative fluid input during 10 h of ECMO circulation for the EVT and MVT groups.
3.1. Hemodynamics, Respiratory Data, and Blood Gas Analysis
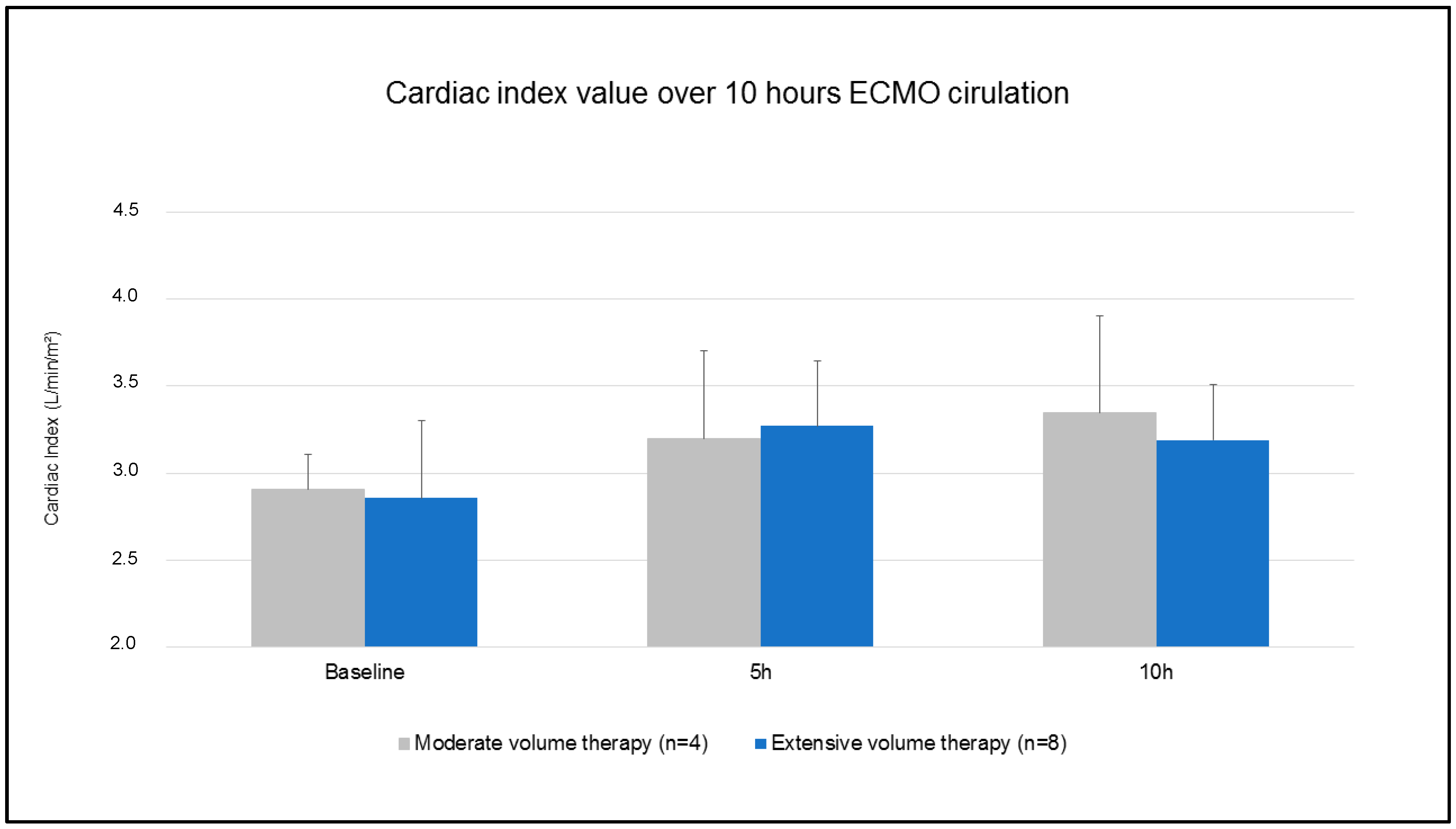
Baseline data are summarized in Table 1. Hemodynamic parameters were comparable between the groups at t1 (cardiac output: 3.1 ± 0.2 L/min MVT vs. 3.0 ± 0.5 L/min EVT; p = 0.666/MAP: 71 ± 9 mmHg MVT vs. 66 ± 11 mmHg EVT; p = 0.417/CVP: 12 ± 1 mmHg MVT vs. 13 ± 4 mmHg EVT; p = 0.683), except for a higher mean pulmonary arterial pressure in MVT (25 ± 1 mmHg MVT vs. 23 ± 3 mmHg EVT; p = 0.041). Additionally, respiratory data showed no statistical difference. FIO2 did not differ between the groups. The cardiac index was adjusted in regard to the targeted values and showed no difference between the groups during the study period (Figure 4). After 10 h of ECMO circulation, cumulative urine output did not differ between the groups (776 ± 495 mL MVT vs. 1003 ± 504 mL EVT; p = 0.484). Hemodynamic data showed no difference in accordance with the volume applied after 10 h of ECMO therapy (Table 2). Blood flow in the ascending aorta decreased significantly in both groups, with no difference between MVT and EVT (0.2 ± 0.1 L/min MVT vs. 0.5 ± 0.4 L/min EVT; p = 0.128). Carotidal and coronary flow were comparable. Moreover, MVT did not impact respiratory data (Table 2). Blood gas analysis showed a significant higher decrease of hemoglobin (7.9 ± 0.4 g/dL MVT vs. 6.7 ± 1.2 g/dL EVT; p = 0.035) and haematocrit (25 ± 1% MVT vs. 21 ± 4% EVT; p = 0.036) in EVT. Lactic acid levels were higher in EVT.

Table 1.
Baseline data prior to ECMO circulation.
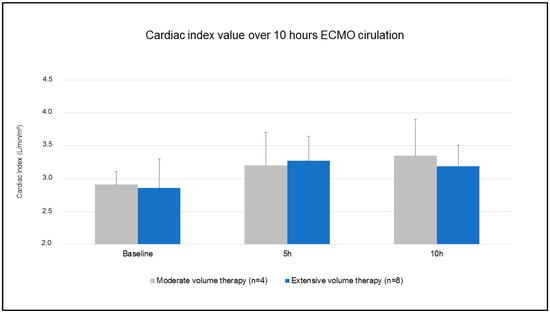
Figure 4.
Cardiac index value over 10 h ECMO circulation.
Table 2.
Assessed data after 10 h of ECMO circulation.
3.2. Relative Creatinine Change
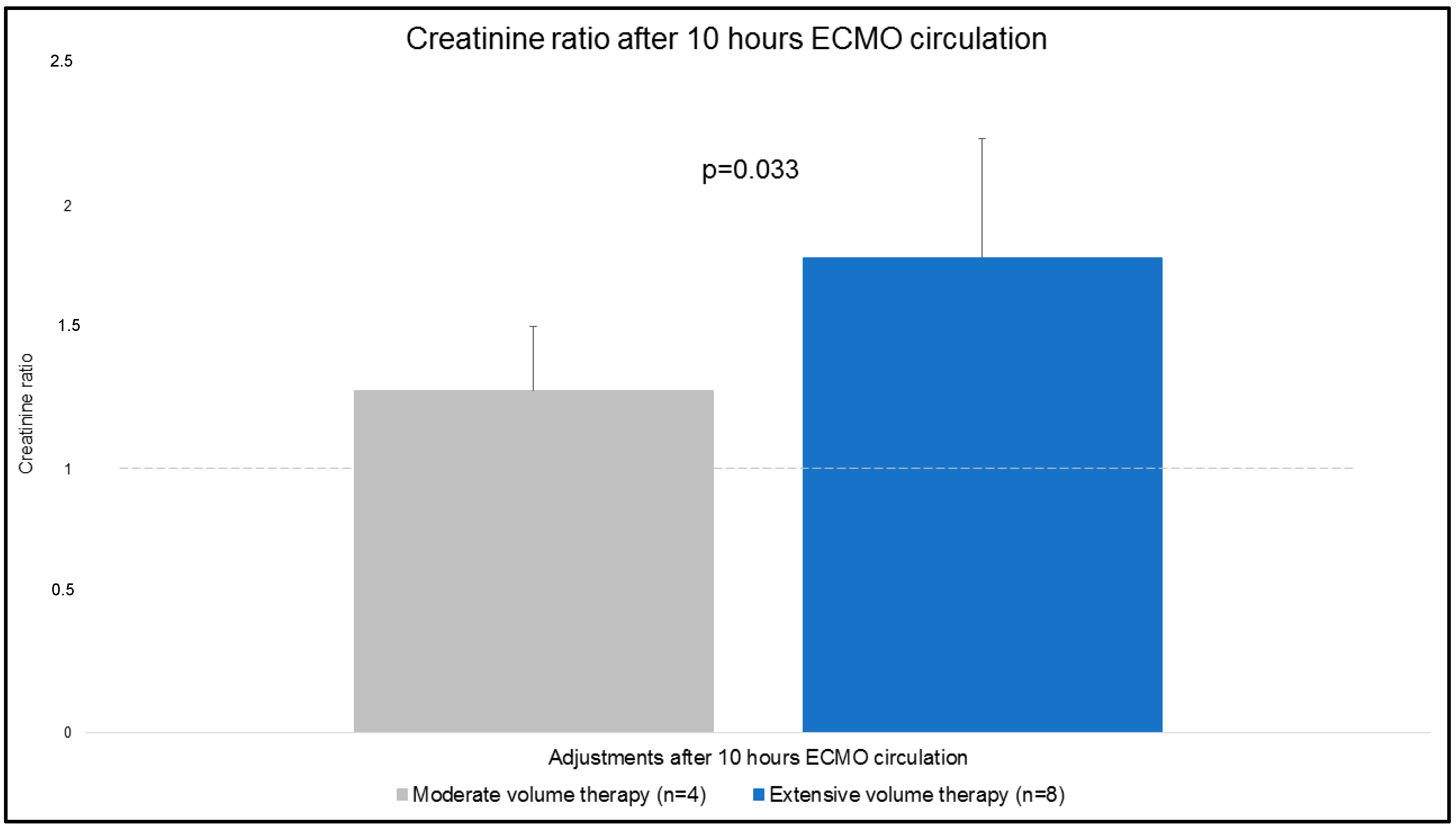
Creatinine values were obtained at t1 and t2. Relative changes (creatinine ratio) of absolute values for both groups are presented in Figure 5. The creatinine ratio was significantly higher in EVT compared to MVT (1.3 ± 0.3 MVT vs. 1.8 ± 0.5 EVT; p = 0.033).
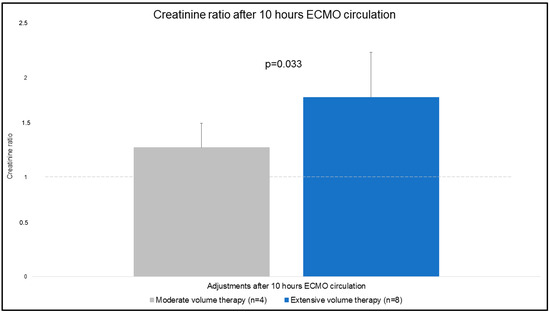
Figure 5.
Creatinine ratio after 10 h ECMO circulation.
3.3. Organ Edema
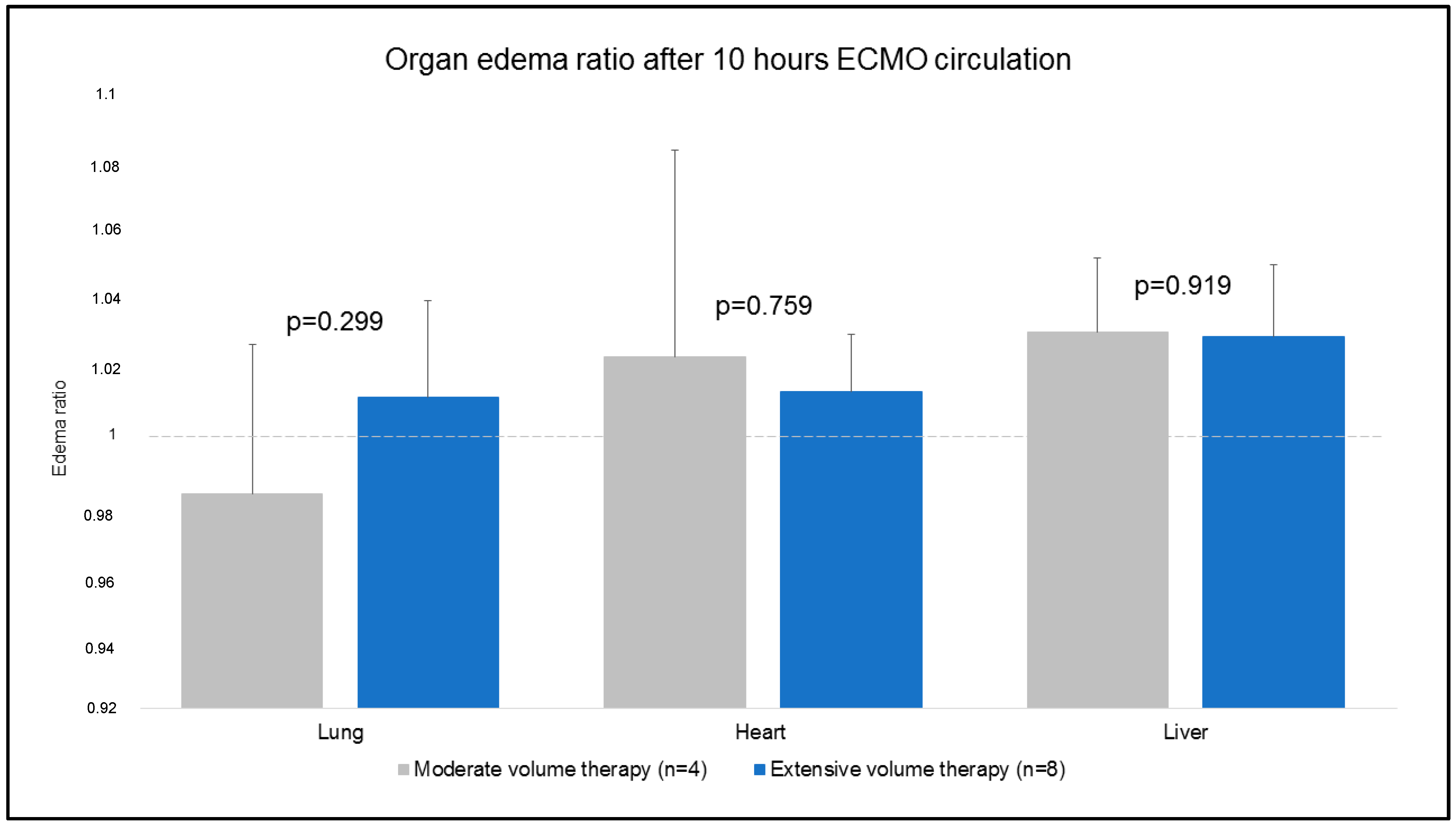
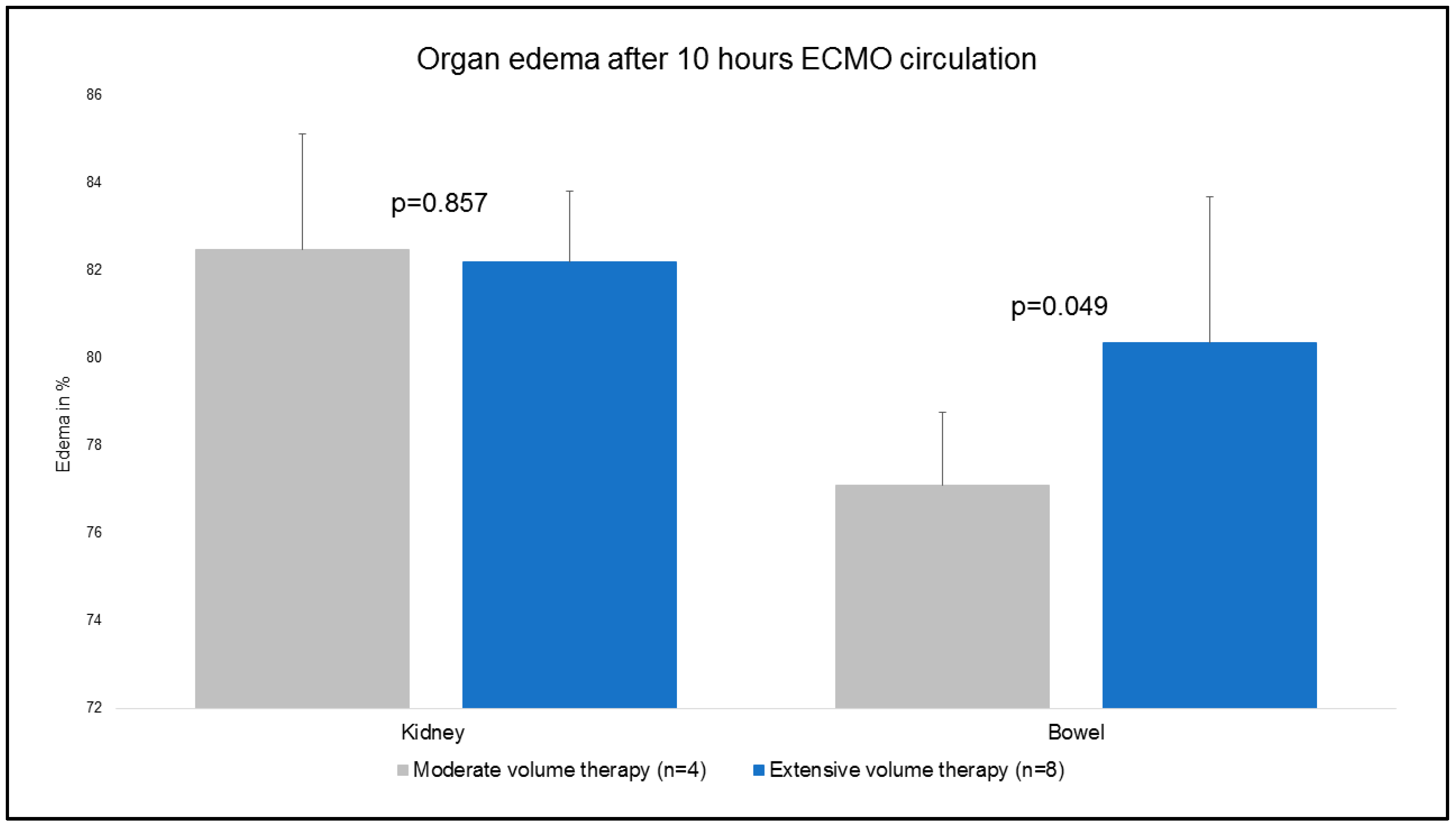
Tissue probes of the lung, heart, and liver were obtained at t1 and t2. The primary outcome showed that no major differences were evident for the mentioned organ samples in regard to the organ edema ratio (Figure 6). Due to the experimental protocol, tissue samples of the kidney and bowel were taken at t2 (Figure 7). Kidney samples were comparable (83 ± 3% MVT vs. 82 ± 2% EVT; p = 0.857). Bowel tissue showed a higher percentage of edema in EVT compared to MVT (77 ± 2% MVT vs. 80 ± 3 % EVT; p = 0.049).
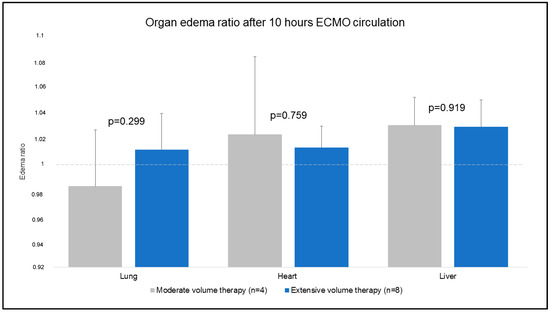
Figure 6.
Organ edema ratio after 10 h ECMO circulation.
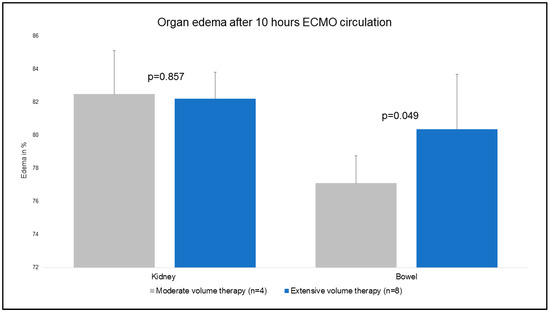
Figure 7.
Organ edema (%) after 10 h ECMO circulation.
4. Discussion
The main findings of our analysis investigating the impact of volume overload during ECMO circulation were:
- From our analysis excessive fluid resuscitation might affect intestinal tissue structure and contribute to dysfunction of the intestinal barrier.
- Higher renal dysfunction in EVT was shown.
4.1. Clinical Studies Indicating the Association of Fluid Overload with Adverse Outcomes
The reasons for fluid overload in ECMO patients are heterogeneous and multifactorial. In clinical practice, fluid administration in ECMO patients frequently depends on intravascular hypovolemia, which causes the suction phenomenon of the ECMO circuit. Moreover, maintenance of targeted mean arterial pressure (>60 mmHg) is achieved by simultaneous vasopressor and volume therapy. In patients with compromised hemodynamics, initial excessive volume application might stabilize the hemodynamic situation and result in suction-free ECMO circulation. On the other side, this overload might negatively impact the following days’ ECMO support. Schmidt and colleagues from Paris and Melbourne were the first to report the impact of fluid balance on outcome after ECMO therapy [12]. In their retrospective analysis of 172 patients treated with either veno-arterial or veno-venous ECMO, the authors could prove that early positive fluid balance at day 3 after ECMO initiation was an independent predictor of 90-day mortality, regardless of primary diagnosis, acute kidney injury (AKI), or required hemodialysis.
Another study group by Staudacher investigated 195 patients, showing that higher fluid balance was significantly associated with less survival in ECMO patients and might be useful for prognostication [13]. In regard to the outcome, the authors found no evidence supporting liberal volume therapy. Kim and colleagues from South Korea investigated 723 ECMO patients retrospectively and reported on a significantly increased risk of 90-day mortality in patients with higher fluid balance values, corroborating the findings of Schmidt and Staudacher [14]. The authors presented that mortality risk did not increase until a fluid balance of 82.3 mL/kg was reached in patients with cardiovascular causes for ECMO. In patients with pulmonary indications for ECMO, levels above 189.6 mL/kg were associated with an increase in mortality [14]. Additionally, Anton-Martin et al. recently presented congruent results for neonatal and pediatric ECMO patients in their observational retrospective analysis [24]. Fluid accumulation within the first day after ECMO implementation was significantly associated with increased ICU mortality, showing a higher proportion of AKI in non-survivors. These findings are consistent with the data provided by Selewski and colleagues [25]. Selewski investigated 756 children under ECMO support and showed that fluid overload was independently associated with adverse outcomes, including increased mortality and increased duration of extracorporeal membrane oxygenation [25].
Interestingly, in our analysis, lactate levels differed between the groups. The fact that the hemoglobin differed might contribute to these circumstances. However, hemoglobin differences are expressed by fluid overload. It is speculative if low hemoglobin concentrations affected lactate levels or if the proven renal and intestinal dysfunction was followed by a lactic acid increase.
Moreover, a fluid overload might lead to distension of the left ventricle, and physicians should be aware of such a complication. Actually, there are some strategies for ventricular unloading (Impella, IABP), and the right one depends on several parameters.
4.2. Excessive Volume Administration Might Trigger AKI in ECMO Patients
As fluid administration is essential for outcomes in ECMO patients, Bridges and colleagues recently published guidelines for fluid and electrolyte management in ECMO patients, with special attention to the development and therapeutic options of AKI [26]. The authors clearly stated that fluid overload and AKI are associated with increased morbidity and mortality in ECMO patients. These clinical findings are supported by our analysis. In comparison of MVT and EVT, our data showed that creatinine levels were significantly higher in EVT, suggesting a deterioration of renal function, whereas cumulative urine output did not differ between the groups (776 ± 495 mL MVT vs. 1003 ± 504 mL EVT; p = 0.484). As our volume administration was based on targeted cardiac index and mean arterial pressure, fluid overload in EVT might affect end organ function. In translation to clinical settings, a targeted higher ECMO blood flow will result in more frequent ECMO suction events and thereby trigger volume therapy in non-hypovolemic patients. This iatrogenic-induced hypervolemia is known to affect renal function. Recently, Murphy and colleagues reported on a multicenter study analyzing the impact of AKI, fluid overload, and renal replacement therapy on mortality in neonatal ECMO patients [27]. The authors showed that fluid overload (OR 1.20, 95% CL 1.11–1.30) and acute kidney injury requiring hemodialysis (OR 2.12, 95% CL 1.20–3.73) were independently associated with mortality [27].
Moreover, ECMO circulation itself is known to induce a systemic inflammatory response, requiring fluid resuscitation. In addition, ECMO has been described as a risk factor for AKI [28]. In clinical scenarios, AKI was shown to occur in 35.5–74.0% of patients treated with ECMO due to cardiogenic shock and cardiac arrest [29]. The contribution to AKI by ECMO is explainable by exposure to foreign membranes, non-pulsatile renal blood flow, increased blood shear stress, air and blood embolisms, hemolysis, and organ crosstalk of the heart, lung, and kidneys [30]. Yuan et al. demonstrated in an experimental cardiac arrest model that ECMO might alleviate AKI by downregulating AKI-related gene expression and apoptosis after cardiac arrest [31]. Further investigation is necessary to evaluate and translate the described findings.
To avoid the negative impact of fluid overload in ECMO patients, Thomas et al. suggest initiating in an early phase continuous renal replacement therapy (RRT) targeting in this way a negative fluid balance [32]. The authors showed that the patient groups with ECMO support and RRT with a negative fluid balance (−3840 mL vs. +425 mL; p ≤ 0.005) were associated with higher survival to discharge rates. In general, indications to implement RRT are varying. A multicentric survey of ECMO centers showed that the most frequent indications for RRT in ECMO patients were fluid overload (43%), the prevention of EVT (16%), and the occurrence of AKI (35%) [33]. The technical implementation of RRT in on-going ECMO support, whether directly into the ECMO circulation or in parallel, is a matter of current discussion [34]. In accordance with the published guidelines for fluid and electrolyte management in ECMO patients, early initiation of RRT should always be an integral part of therapeutic considerations to achieve solute clearance, adjust electrolyte discrepancies, and prevent EVT [26].
4.3. Impact of Excessive Fluid Resuscitation on Intestinal Edema and Function
As already mentioned, fluid overload is known to impact organ function. In our analysis, organ edema was assessed and analyzed in comparison to MVT and EVT. Interestingly, organ edema in intestinal tissue samples showed significantly higher manifestation in EVT (77 ± 2% MVT vs. 80 ± 3% EVT; p = 0.049). Impact on several other tissue samples (lung, heart, liver, and kidneys) was not shown.
In regard to fluid overload-induced intestinal microcirculatory damage, Behem and colleagues from Hamburg (Germany) reported on their large animal study investigating the impact of volume therapy on intestinal microcirculation [35]. They showed that ischemia-reperfusion led to impaired intestinal microcirculation, which was not restored by volume administration despite improved cardiac output [35]. In this regard, volume therapy should be titrated with meticulous care, particularly after ischemia-reperfusion injury, and ECMO therapy should be implemented in extracorporeal cardiopulmonary resuscitation. Additionally, unnecessary fluid loads may impair microcirculatory flow and worsen tissue edema, as we showed with our data. Several molecular-biological pathways are discussed to trigger an increase in edema in intestinal tissue; however, this particular point was not assessed in our study and needs further investigation. Kurundkar and colleagues presented results from their experimental study, showing an ECMO-induced rapid increase in gut mucosal permeability within the first 2 h of treatment, leading to a significant rise in circulating bacterial products [36]. Gut barrier dysfunction might be triggered in this way by ECMO, explaining the potential for plainer bacterial translocation. In contrast to the findings of Kurundkar, Liang and colleagues showed in their large-animal experimental protocol (CPR + ECMO vs. ECMO, n = 24) that intestinal mucosal epithelial cells in the CPR + ECMO group exhibited significantly reduced congestion and edema in comparison with those in the CPR group [37]. Moreover, expression of anti-apoptotic proteins in intestinal mucosa was higher in the ECMO + CPR group. In this regard, Ni et al. demonstrated in their pig-model (n = 21) that ECMO support aggravates intestinal mucosal injury early during ECMO support. However, protective effects on the intestinal mucosal barrier were shown 24 h after ECMO initiation, indicating a positive impact at a later stage of ECMO circulation [38]. He and colleagues provided an interesting study investigating the impact of RRT on the intestinal mucosal barrier during ECMO circulation [39]. 24 pigs were included in this study, and histopathologic findings showed that ECMO-induced intestinal edema and morphological distortion of epithelial cell structures were significantly improved by adding RRT to ECMO therapy. This finding supports the hypothesis that fluid overload negatively impacts the mucosal barrier, and the questionable impact of ECMO therapy on gut function should be the subject of further studies.
In a clinical setting, intestinal dysfunction is of subordinate relevance next to cardiac, pulmonary, and cerebral failure and their importance in ECMO therapy. In regard to therapeutic measures, medication with ulinastatin is currently a topic of interest in ischemia-induced intestinal barrier dysfunction [40]. Ulinastatin is a serine protease inhibitor that has anti-inflammatory characteristics and has been widely used as a treatment for patients with inflammatory disorders. Zhang and colleagues could prove a protective role by decreasing oxidative stress in the intestinal mucosa of rats after cardiopulmonary resuscitation. These effects were enlarged by mild therapeutic hypothermia. In particular, this pharmacological approach might be of interest in ECMO-associated gut barrier failure and needs further research. However, our findings and studies discussed above might support and encourage ongoing investigation into this specific subject.
In general, patients receiving veno-arterial ECMO in a clinical scenario suffer some form of cardiogenic/hemodynamic severe compromise associated with capillary leak syndrome. This loss of intravascular volume to the interstitial space may significantly impact the findings of this study. Indeed, this situation may prompt further volume overload, interstitial edema, and, at least, more intestinal mucosa damage (and probably more edema in other organs). This assumption is somehow speculative and must be confirmed in further studies.
4.4. Study Limitations
As the study was not powered and designed with regard to the presented topic, results might be limited in this way. Moreover, the methodological classification of volume therapy in MVT and EVT was based on mathematical quantity and was not triggered by pathology-related thresholds. Furthermore, the division of the two cohorts is somehow arbitrary. In a clinical scenario, it may be difficult to objectively identify the point at which patients start to receive a liquid overload. By investigating healthy pigs in a purely experimental and artificial setting, the translation of our findings to clinical scenarios is somehow limited. Furthermore, 10 h of extracorporeal support does not correspond to clinical reality, in which systems are used for a significantly longer time. Therefore, our data cannot answer whether the observation time of 10 h is too short for changes in heart, lung, liver, or kidney tissue or whether fluid overload actually has no effect on these tissues. However, our data might encourage further investigation with a prospectively designed study protocol to address the impact of extensive volume therapy on ECMO circulation more explicitly.
5. Conclusions
In our post-hoc investigation of volume therapy’s associated impact on renal function and tissue edema in ECMO circulation, the presented data suggest deterioration of renal function and potential deterioration of intestinal mucosa function by an increase in tissue edema.
Author Contributions
Conceptualization, O.L., A.C.D., I.S., I.D. and T.W.; methodology, O.L., A.C.D., E.K., I.S. and I.D.; software, A.S.; validation, I.D. and A.C.D.; formal analysis I.D.; investigation, I.D., J.M.-T., M.E., T.M., A.M., P.R., S.G., A.C.D. and O.L.; resources, T.W. and O.L.; data curation, I.D. and A.C.D.; writing—original draft preparation, I.D. and A.C.D.; writing—review and editing, A.C.D., B.I. and I.K.; visualization, I.D.; supervision, T.W. and O.L.; project administration, I.D. and J.M.-T.; funding acquisition, A.C.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Koeln Fortune Program (343/2015).
Institutional Review Board Statement
The animal study protocol was approved by the responsible ethical committee for animal care of the University of Cologne (LANUV Northrhine-Westphalia, Recklinghausen, Germany) in compliance with the Directive 2010/63/EU of the European Parliament (protocol code: 84-02.04.2016.A245; date: 29 November 2016).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting the reported results can be provided on request by the corresponding author.
Acknowledgments
We thank the staff of the Experimental Medicine Department (University Hospital Cologne) for their support during the investigation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Abrams, D.; Combes, A.; Brodie, D. Extracorporeal membrane oxygenation in cardiopulmonary disease in adults. J. Am. Coll. Cardiol. 2014, 63, 2769–2778. [Google Scholar] [CrossRef] [PubMed]
- Sidebotham, D.; McGeorge, A.; McGuinness, S.; Edwards, M.; Willcox, T.; Beca, J. Extracorporeal membrane oxygenation for treating severe cardiac and respiratory failure in adults: Part 2-technical considerations. J. Cardiothorac. Vasc. Anesth. 2010, 24, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Sidebotham, D. Troubleshooting adult ECMO. J. Extra Corpor. Technol. 2011, 43, P27–P32. [Google Scholar] [PubMed]
- Adrie, C.; Adib-Conquy, M.; Laurent, I.; Monchi, M.; Vinsonneau, C.; Fitting, C.; Fraisse, F.; Dinh-Xuan, A.T.; Carli, P.; Spaulding, C.; et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation 2002, 106, 562–568. [Google Scholar] [CrossRef]
- Heradstveit, B.E.; Guttormsen, A.B.; Langorgen, J.; Hammersborg, S.M.; Wentzel-Larsen, T.; Fanebust, R.; Larsson, E.-M.; Heltne, J.-K. Capillary leakage in post-cardiac arrest survivors during therapeutic hypothermia—A prospective, randomised study. Scand. J. Trauma. Resusc. Emerg. Med. 2010, 18, 29. [Google Scholar] [CrossRef]
- Boyd, J.H.; Forbes, J.; Nakada, T.A.; Walley, K.R.; Russell, J.A. Fluid resuscitation in septic shock: A positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit. Care Med. 2011, 39, 259–265. [Google Scholar] [CrossRef]
- Durairaj, L.; Schmidt, G.A. Fluid therapy in resuscitated sepsis: Less is more. Chest 2008, 133, 252–263. [Google Scholar] [CrossRef]
- Acheampong, A.; Vincent, J.L. A positive fluid balance is an independent prognostic factor in patients with sepsis. Crit. Care 2015, 19, 251. [Google Scholar] [CrossRef]
- de Oliveira, F.S.; Freitas, F.G.; Ferreira, E.M.; de Castro, I.; Bafi, A.T.; de Azevedo, L.C.; de Azevedo, L.C.P.; Machado, F.R. Positive fluid balance as a prognostic factor for mortality and acute kidney injury in severe sepsis and septic shock. J. Crit. Care 2015, 30, 97–101. [Google Scholar] [CrossRef]
- Micek, S.T.; McEvoy, C.; McKenzie, M.; Hampton, N.; Doherty, J.A.; Kollef, M.H. Fluid balance and cardiac function in septic shock as predictors of hospital mortality. Crit. Care 2013, 17, R246. [Google Scholar] [CrossRef]
- Sirvent, J.M.; Ferri, C.; Baro, A.; Murcia, C.; Lorencio, C. Fluid balance in sepsis and septic shock as a determining factor of mortality. Am. J. Emerg. Med. 2015, 33, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Bailey, M.; Kelly, J.; Hodgson, C.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V.; Bellomo, R.; Pilcher, D. Impact of fluid balance on outcome of adult patients treated with extracorporeal membrane oxygenation. Intensive Care Med. 2014, 40, 1256–1266. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, D.L.; Gold, W.; Biever, P.M.; Bode, C.; Wengenmayer, T. Early fluid resuscitation and volume therapy in venoarterial extracorporeal membrane oxygenation. J. Crit. Care 2017, 37, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Paek, J.H.; Song, J.H.; Lee, H.; Jhee, J.H.; Park, S.; Yun, H.-R.; Kee, Y.K.; Han, S.H.; Yoo, T.-H.; et al. Permissive fluid volume in adult patients undergoing extracorporeal membrane oxygenation treatment. Crit. Care 2018, 22, 270. [Google Scholar] [CrossRef]
- Selewski, D.T.; Cornell, T.T.; Blatt, N.B.; Han, Y.Y.; Mottes, T.R.; Kommareddi, M.; Gaies, M.G.; Annich, G.M.; Kershaw, D.B.; Shanley, T.P.; et al. Fluid overload and fluid removal in pediatric patients on extracorporeal membrane oxygenation requiring continuous renal replacement therapy. Crit. Care Med. 2012, 40, 2694–2699. [Google Scholar] [CrossRef] [PubMed]
- McCanny, P.; Smith, M.W.; O’Brien, S.G.; Buscher, H.; Carton, E.G. Fluid Balance and Recovery of Native Lung Function in Adult Patients Supported by Venovenous Extracorporeal Membrane Oxygenation and Continuous Renal Replacement Therapy. ASAIO J. 2019, 65, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.; Calabro, L.; Pugliese, L.; Lulja, A.; Sopuch, A.; Rosalba, D.; Morenghi, E.; Hernandez, G.; Monnet, X.; Cecconi, M. Fluid challenge in critically ill patients receiving haemodynamic monitoring: A systematic review and comparison of two decades. Crit. Care. 2022, 26, 186. [Google Scholar] [CrossRef] [PubMed]
- La Via, L.; Astuto, M.; Dezio, V.; Muscara, L.; Palella, S.; Zawadka, M.; Vignon, P.; Sanfilippo, F. Agreement between subcostal and transhepatic longitudinal imaging of the inferior vena cava for the evaluation of fluid responsiveness: A systematic review. J. Crit. Care 2022, 71, 154108. [Google Scholar] [CrossRef]
- Sanfilippo, F.; La Via, L.; Dezi, V.; Amelio, P.; Genoese, G.; Franchi, F.; Messina, A.; Robba, C.; Noto, A. Inferior vena cava distensibility from subcostal and trans-hepatic imaging using both M-mode or artificial intelligence: A prospective study on mechanically ventilated patients. Intensive Care Med. Exp. 2023, 11, 40. [Google Scholar] [CrossRef]
- Monnet, X.; Marik, P.; Teboul, J.T. Passive leg raising for predicting fluid responsiveness: A systematic review and meta-analysis. Intensive Care Med. 2016, 42, 1935–1947. [Google Scholar] [CrossRef]
- Georges, D.; de Courson, H.; Lanchon, R.; Sesay, M.; Nouette-Gaulain, K.; Biais, M. End-expiratory occlusion maneuver to predict fluid responsiveness in the intensive care unit: An echocardiographic study. Crit. Care 2018, 22, 32. [Google Scholar] [CrossRef]
- Djordjevic, I.; Liakopoulos, O.; Elskamp, M.; Maier-Trauth, J.; Gerfer, S.; Muhlbauer, T.; Slottosch, I.; Kuhn, E.; Sabashnikov, A.; Rademann, P.; et al. Concomitant Intra-Aortic Balloon Pumping Significantly Reduces Left Ventricular Pressure during Central Veno-Arterial Extracorporeal Membrane Oxygenation-Results from a Large Animal Model. Life 2022, 12. [Google Scholar] [CrossRef]
- Hannon, J.P.; Bossone, C.A.; Wade, C.E. Normal physiological values for conscious pigs used in biomedical research. Lab. Anim. Sci. 1990, 40, 293–298. [Google Scholar] [PubMed]
- Anton-Martin, P.; Quigley, R.; Dhar, A.; Bhaskar, P.; Modem, V. Early Fluid Accumulation and Intensive Care Unit Mortality in Children Receiving Extracorporeal Membrane Oxygenation. ASAIO J. 2020. [CrossRef] [PubMed]
- Selewski, D.T.; Askenazi, D.J.; Bridges, B.C.; Cooper, D.S.; Fleming, G.M.; Paden, M.L.; Verway, M.; Sahay, R.; King, E.; Zappitelli, M. The Impact of Fluid Overload on Outcomes in Children Treated With Extracorporeal Membrane Oxygenation: A Multicenter Retrospective Cohort Study. Pediatr. Crit. Care Med. 2017, 18, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Bridges, B.C.; Dhar, A.; Ramanathan, K.; Steflik, H.J.; Schmidt, M.; Shekar, K. Extracorporeal Life Support Organization Guidelines for Fluid Overload, Acute Kidney Injury, and Electrolyte Management. ASAIO J. 2022, 68, 611–618. [Google Scholar] [CrossRef]
- Mallory, P.P.; Selewski, D.T.; Askenazi, D.J.; Cooper, D.S.; Fleming, G.M.; Paden, M.L.; Murphy, L.; Sahay, R.; King, E.; Zappitelli, M.; et al. Acute Kidney Injury, Fluid Overload, and Outcomes in Children Supported With Extracorporeal Membrane Oxygenation for a Respiratory Indication. ASAIO J. 2020, 66, 319–326. [Google Scholar] [CrossRef]
- Chen, H.; Yu, R.G.; Yin, N.N.; Zhou, J.X. Combination of extracorporeal membrane oxygenation and continuous renal replacement therapy in critically ill patients: A systematic review. Crit. Care 2014, 18, 675. [Google Scholar] [CrossRef]
- Cheng, R.; Hachamovitch, R.; Kittleson, M.; Patel, J.; Arabia, F.; Moriguchi, J.; Esmailian, F.; Azarbal, B. Complications of Extracorporeal Membrane Oxygenation for Treatment of Cardiogenic Shock and Cardiac Arrest: A Meta-Analysis of 1,866 Adult Patients. Ann. Thorac. Surg. 2014, 97, 610–616. [Google Scholar] [CrossRef]
- Hamdi, T.; Palmer, B.F. Review of Extracorporeal Membrane Oxygenation and Dialysis-Based Liver Support Devices for the Use of Nephrologists. Am. J. Nephrol. 2017, 46, 139–149. [Google Scholar] [CrossRef]
- Yuan, X.-L.; Li, C.-S.; Zhang, Y.; Ling, J.-Y.; Zhang, Q.; Liang, Y.; Liu, B.; Zhao, L.-X. Extracorporeal Membrane Oxygenation Improving Survival and Alleviating Kidney Injury in a Swine Model of Cardiac Arrest Compared to Conventional Cardiopulmonary Resuscitation. Chin. Med. J. 2018, 131, 1840–1848. [Google Scholar] [CrossRef]
- Thomas, J.M.; Dado, D.N.; Basel, A.P.; Aden, J.K.; Thomas, S.B.; Piper, L.; Britton, G.W.; Cancio, L.C.; Batchinsky, A.; Mason, P.E.; et al. Adjunct Use of Continuous Renal Replacement Therapy with Extracorporeal Membrane Oxygenation Achieves Negative Fluid Balance and Enhances Oxygenation Which Improves Survival in Critically Ill Patients without Kidney Failure. Blood Purif. 2022, 51, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Fleming, G.M.; Askenazi, D.J.; Bridges, B.C.; Cooper, D.S.; Paden, M.L.; Selewski, D.T.; Zappitelli, M. A multicenter international survey of renal supportive therapy during ECMO: The Kidney Intervention During Extracorporeal Membrane Oxygenation (KIDMO) group. ASAIO J. 2012, 58, 407–414. [Google Scholar] [CrossRef]
- Selewski, D.T.; Wille, K.M. Continuous renal replacement therapy in patients treated with extracorporeal membrane oxygenation. Semin. Dial. 2021, 34, 537–549. [Google Scholar] [CrossRef] [PubMed]
- Behem, C.R.; Graessler, M.F.; Pinnschmidt, H.O.; Duprée, A.; Sandhu, H.K.; Debus, E.S.; Wipper, S.H.; Trepte, C.J. Volume Based Resuscitation and Intestinal Microcirculation after Ischaemia/Reperfusion Injury: Results of an Exploratory Aortic Clamping Study in Pigs. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Kurundkar, A.R.; Killingsworth, C.R.; McIlwain, R.B.; Timpa, J.G.; Hartman, Y.E.; He, D.; Karnatak, R.K.; Neel, M.L.; Clancy, J.P.; Anantharamaiah, G.M.; et al. Extracorporeal membrane oxygenation causes loss of intestinal epithelial barrier in the newborn piglet. Pediatr. Res. 2010, 68, 128–133. [Google Scholar] [CrossRef]
- Liang, Y.; Li, C.; Liu, B.; Zhang, Q.; Yuan, X.; Zhang, Y.; Ling, J.; Zhao, L. Protective effect of extracorporeal membrane oxygenation on intestinal mucosal injury after cardiopulmonary resuscitation in pigs. Exp. Ther. Med. 2019, 18, 4347–4355. [Google Scholar] [CrossRef]
- Ni, L.; Chen, Q.; Zhu, K.; Shi, J.; Shen, J.; Gong, J.; Gao, T.; Yu, W.; Li, J.; Li, N. The influence of extracorporeal membrane oxygenation therapy on intestinal mucosal barrier in a porcine model for post-traumatic acute respiratory distress syndrome. J. Cardiothorac. Surg. 2015, 10, 20. [Google Scholar] [CrossRef]
- He, C.; Yang, S.; Yu, W.; Chen, Q.; Shen, J.; Hu, Y.; Shi, J.; Wu, X.; Li, J.; Li, N. Effects of continuous renal replacement therapy on intestinal mucosal barrier function during extracorporeal membrane oxygenation in a porcine model. J. Cardiothorac. Surg. 2014, 9, 72. [Google Scholar] [CrossRef]
- Zhang, F.J.; Song, H.Q.; Li, X.M. Effect of ulinastatin combined with mild therapeutic hypothermia on intestinal barrier dysfunction following cardiopulmonary resuscitation in rats. Exp. Ther. Med. 2019, 18, 3861–3868. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).