
Is Histamine and Not Acetylcholine the Missing Link between ADHD and Allergies? Speer Allergic Tension Fatigue Syndrome Re-Visited


Abstract
:1. Introduction
“One of the most significant developments in contemporary medicine has been the increasing recognition that the soma and the psyche are not distinct and unrelated, but are so closely bound together as to make proper investigation of both a necessary part of the management of disease.”Frederic Speer (The allergic tension-fatigue syndrome, 1954)
2. Speer Allergic Tension-Fatigue Syndrome (SATFS)
2.1. Behavioral Allergic Traits
2.2. Constitutional Allergic Traits
2.3. A Misstep? Speer’s Cholinergic Theory
3. Histamine
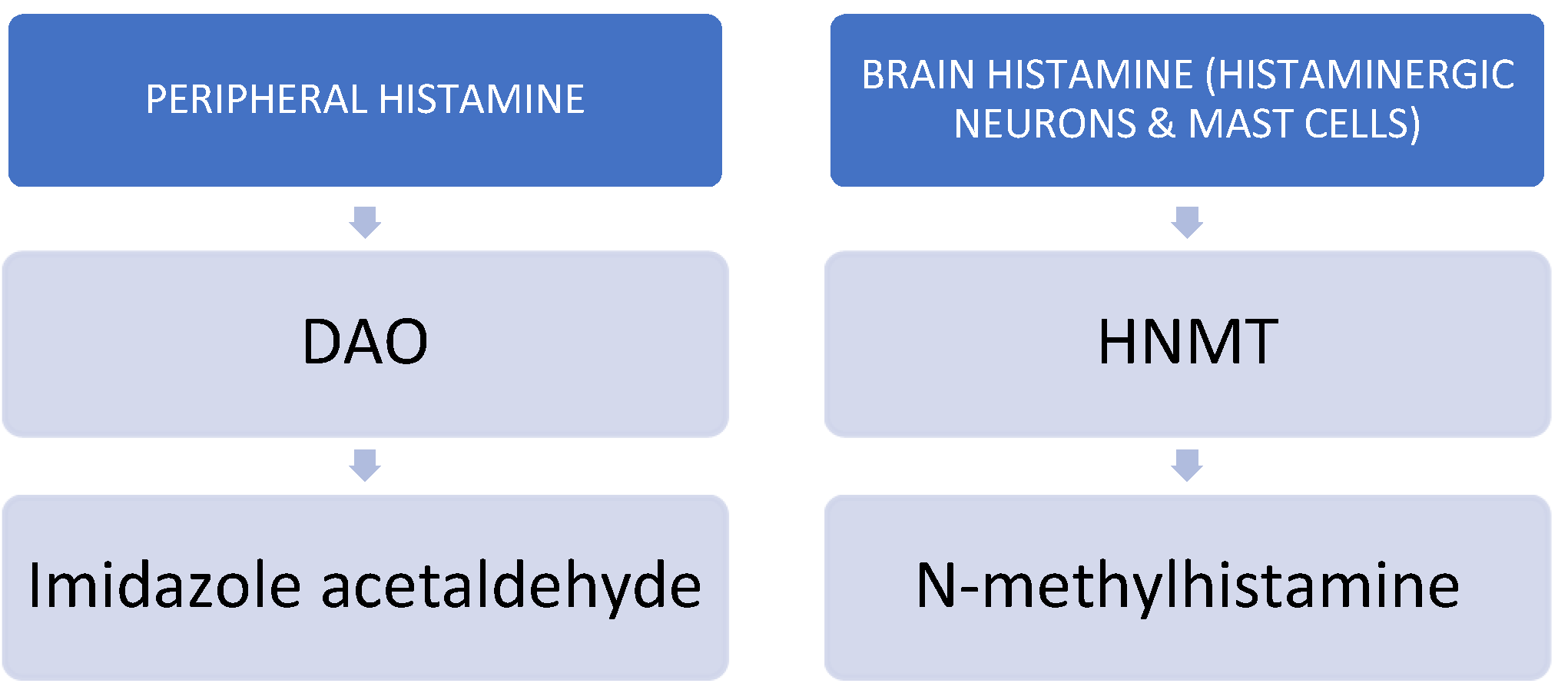
3.1. Body Histamine
3.1.1. Histamine and the Immune System
3.1.2. Histamine and the Digestive System
3.1.3. Histamine and Migraines
3.1.4. Histamine and Histamine Intolerance (HIT)
3.1.5. DAO Deficiency and Histamine-Related Diseases, including Histamine Intolerance (HIT)
3.2. Brain (CNS) Histamine
4. Speer Allergic Tension-Fatigue Syndrome (SATFS) Re-Visited
- Hypothesis 1: SATFS is probably one of the first and best historical descriptions of patients with ADHD;
- Hypothesis 2: SATFS (ADHD for me) is a systemic disease;
- Hypothesis 3: Histamine is key for understanding the pathophysiology of the typical medical comorbidities displayed by patients with ADHD; and
- Hypothesis 4: The DAO enzyme may play a key role in the pathophysiology of ADHD. A decreased DAO activity may lead to an accumulation of histamine, which could contribute to ADHD symptoms.
4.1. Might the Behavior Displayed by Patients Diagnosed with SATFS Be an Initial Description of ADHD? (Hypothesis 1)
4.2. The Constitutional Component of SATFS: ADHD as a Systemic Disease. What Is the Evidence? (Hypothesis 2)
ADHD and the Immune System: A Focus on Inflammation, Allergy, and Autoimmune, Cancer, and Cardiovascular Comorbidities
4.3. Is Histamine the Missing Link between ADHD and Allergies? (Hypothesis 3)
4.3.1. A Little Bit of History—The Physiopathological Foundations of ADHD
4.3.2. ADHD and Histamine-Mediated Comorbid Disorders
4.3.3. ADHD and Histamine: What Is the Evidence?
- (1)
- One of the most relevant lines of evidence comes from the deleterious effects produced by some antihistaminergic drugs. Traditionally, first-generation antihistamines (i.e., diphenhydramine) were characterized by readily crossing the BBB, thus leading to significant CNS side effects such as altered mood, reduced wakefulness, drowsiness, and impaired psychomotor and cognitive performance (i.e., vigilance, divided attention, and working memory) even in the absence of self-reported sleepiness [109]. In other words, antihistamines produce side effects that are very similar to some ADHD symptoms.
- (2)
- (3)
- Two frequently used drugs for treating ADHD (methylphenidate and atomoxetine) increase histamine availability in the pre-frontal cortex [113,114]. Thus, the therapeutic effects of ADHD medications may partly be due to increasing histamine release, in addition to the well-known increasing effect of dopamine and noradrenaline in ADHD [115]. A third drug, lisdexamfetamine dimesylate, an amphetamine approved for the treatment of ADHD, promoted a strong upregulation of DAO mRNA levels, suggesting that this drug may induce DAO activity [116], thus helping to decrease blood histamine levels. This finding is interesting because, with a single drug, we may “kill two birds with one shot”, as we may be treating not only core ADHD symptoms but also allergies.
- (4)
- (5)
- There is increasing evidence concerning the potential therapeutic use of drugs acting on the histaminergic system in patients diagnosed with ADHD. In 1985, a case study reported that an antihistamine, anti-motion sickness drug might exert some improvement in ADHD [123]. While the precise mechanisms underlying the relationship between histamine and ADHD are still unclear, several preclinical and clinical studies have suggested that H3R antagonists, such as Pitolisant, may be effective in treating ADHD symptoms. These drugs increase histamine release and have been shown to improve cognitive function [124] and reduce hyperactivity in individuals with ADHD [106]. However, some studies using anti-H3R drugs for the treatment of ADHD have yielded negative results [125,126].
4.3.4. The Interaction between Histaminergic and Acetylcholine Systems
4.4. Might DAO Enzyme Deficiency Play a Role in the Pathophysiology of Core ADHD Symptoms and Somatic Comorbidities (Hypothesis 4)?
5. Conclusions, Limitations, and Future Directions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Speer, F. The allergic tension-fatigue syndrome. Pediatr. Clin. N. Am. 1954, 1, 1029–1037. [Google Scholar] [CrossRef]
- Speer, F. The allergic tension-fatigue syndrome in children. Int. Arch. Allergy Immunol. 1958, 12, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A.; Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Chess, S. Diagnosis and treatment of the hyperactive child. N. Y. State J. Med. 1960, 60, 2379–2385. [Google Scholar] [PubMed]
- Speer, F. The allergic tension-fatigue syndrome. In Allergy of the Nervous System; Speer, F., Ed.; Charles C Thomas: Springfield, IL, USA, 1970; pp. 14–27. [Google Scholar]
- Marshall, P. Attention deficit disorder and allergy: A neurochemical model of the relation between the illnesses. Psychol. Bull. 1989, 106, 434–446. [Google Scholar] [CrossRef]
- Pelsser, L.M.; Buitelaar, J.K.; Savelkoul, H.F. ADHD as a (non) allergic hypersensitivity disorder: A hypothesis. Pediatr. Allergy Immunol. 2009, 20, 107–112. [Google Scholar] [CrossRef]
- Roth, N.; Beyreiss, J.; Schlenzka, K.; Beyer, H. Coincidence of attention deficit disorder and atopic disorders in children: Empirical findings and hypothetical background. J. Abnorm. Child Psychol. 1991, 19, 1–13. [Google Scholar] [CrossRef]
- Gould, H.J.; Sutton, B.J. IgE in allergy and asthma today. Nat. Rev. Immunol. 2008, 8, 205–217. [Google Scholar] [CrossRef]
- Comas-Basté, O.; Sánchez-Pérez, S.; Veciana-Nogués, M.T.; Latorre-Moratalla, M.; Vidal-Carou, M.D.C. Histamine Intolerance: The Current State of the Art. Biomolecules 2020, 10, 1181. [Google Scholar] [CrossRef]
- Maintz, L.; Novak, N. Histamine and histamine intolerance. Am. J. Clin. Nutr. 2007, 85, 1185–1196. [Google Scholar] [CrossRef]
- Maintz, L.; Yu, C.F.; Rodríguez, E.; Baurecht, H.; Bieber, T.; Illig, T.; Weidinger, S.; Novak, N. Association of single nucleotide polymorphisms in the diamine oxidase gene with diamine oxidase serum activities. Allergy 2011, 66, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Kitanaka, J.; Kitanaka, N.; Tsujimura, T.; Terada, N.; Takemura, M. Expression of diamine oxidase (histaminase) in guinea-pig tissues. Eur. J. Pharmacol. 2002, 437, 179–185. [Google Scholar] [CrossRef]
- Haas, H.L.; Sergeeva, O.A.; Selbach, O. Histamine in the nervous system. Physiol. Rev. 2008, 88, 1183–1241. [Google Scholar] [CrossRef] [PubMed]
- Panula, P. Histamine receptors, agonists, and antagonists in health and disease. Handb. Clin. Neurol. 2021, 180, 377–387. [Google Scholar] [CrossRef]
- Thangam, E.B.; Jemima, E.A.; Singh, H.; Baig, M.S.; Khan, M.; Mathias, C.B.; Church, M.K.; Saluja, R. The Role of Histamine and Histamine Receptors in Mast Cell-Mediated Allergy and Inflammation: The Hunt for New Therapeutic Targets. Front. Immunol. 2018, 9, 1873. [Google Scholar] [CrossRef] [PubMed]
- Branco, A.; Yoshikawa, F.S.Y.; Pietrobon, A.J.; Sato, M.N. Role of Histamine in Modulating the Immune Response and Inflammation. Mediat. Inflamm. 2018, 2018, 9524075. [Google Scholar] [CrossRef]
- Bachert, C. Histamine—A major role in allergy? Clin. Exp. Allergy 1998, 28 (Suppl. S6), 15–19. [Google Scholar] [CrossRef]
- He, Y.; Chan, E.W.; Man, K.K.; Lau, W.C.; Leung, W.K.; Ho, L.M.; Wong, I.C. Dosage effects of histamine-2 receptor antagonist on the primary prophylaxis of non-steroidal anti-inflammatory drug (NSAID)-associated peptic ulcers: A retrospective cohort study. Drug Saf. 2014, 37, 711–721. [Google Scholar] [CrossRef]
- Kawashima, R.; Tamaki, S.; Kawakami, F.; Maekawa, T.; Ichikawa, T. Histamine H2-Receptor Antagonists Improve Non-Steroidal Anti-Inflammatory Drug-Induced Intestinal Dysbiosis. Int. J. Mol. Sci. 2020, 21, 8166. [Google Scholar] [CrossRef]
- Alstadhaug, K.B. Histamine in migraine and brain. Headache 2014, 54, 246–259. [Google Scholar] [CrossRef]
- Yuan, H.; Silberstein, S.D. Histamine and Migraine. Headache 2018, 58, 184–193. [Google Scholar] [CrossRef]
- Lehane, L.; Olley, J. Histamine fish poisoning revisited. Int. J. Food Microbiol. 2000, 58, 1–37. [Google Scholar] [CrossRef]
- Hungerford, J.M. Scombroid poisoning: A review. Toxicon 2010, 56, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Maintz, L.; Benfadal, S.; Allam, J.P.; Hagemann, T.; Fimmers, R.; Novak, N. Evidence for a reduced histamine degradation capacity in a subgroup of patients with atopic eczema. J. Allergy Clin. Immunol. 2006, 117, 1106–1112. [Google Scholar] [CrossRef]
- Mayo-Yáñez, M.; Díaz-Díaz, A.; Calvo-Henríquez, C.; Lechien, J.R.; Vaira, L.A.; Figueroa, A. Diamine Oxidase Activity Deficit and Idiopathic Rhinitis: A New Subgroup of Non-Allergic Rhinitis? Life 2023, 13, 240. [Google Scholar] [CrossRef]
- Matkar, N.M.; Rupwate, R.U.; Desai, N.K.; Kamat, S.R. Comparative study of platelet histamine and serotonin with their corresponding plasma oxidases in asthmatics with normals. J. Assoc. Physicians India 1999, 47, 878–882. [Google Scholar] [PubMed]
- Schnedl, W.J.; Meier-Allard, N.; Michaelis, S.; Lackner, S.; Enko, D.; Mangge, H.; Holasek, S.J. Serum Diamine Oxidase Values, Indicating Histamine Intolerance, Influence Lactose Tolerance Breath Test Results. Nutrients 2022, 14, 2026. [Google Scholar] [CrossRef]
- Griauzdaitė, K.; Maselis, K.; Žvirblienė, A.; Vaitkus, A.; Jančiauskas, D.; Banaitytė-Baleišienė, I.; Kupčinskas, L.; Rastenytė, D. Associations between migraine, celiac disease, non-celiac gluten sensitivity and activity of diamine oxidase. Med. Hypotheses 2020, 142, 109738. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo-Casas, J.; Comas-Basté, O.; Latorre-Moratalla, M.L.; Lorente-Gascón, M.; Duelo, A.; Vidal-Carou, M.C.; Soler-Singla, L. Low serum diamine oxidase (DAO) activity levels in patients with migraine. J. Physiol. Biochem. 2018, 74, 93–99. [Google Scholar] [CrossRef]
- Okutan, G.; Ruiz Casares, E.; Perucho Alcalde, T.; Sánchez Niño, G.M.; Penadés, B.F.; Terrén Lora, A.; Torrente Estríngana, L.; López Oliva, S.; San Mauro Martín, I. Prevalence of Genetic Diamine Oxidase (DAO) Deficiency in Female Patients with Fibromyalgia in Spain. Biomedicines 2023, 11, 660. [Google Scholar] [CrossRef]
- Nazar, W.; Plata-Nazar, K.; Sznurkowska, K.; Szlagatys-Sidorkiewicz, A. Histamine Intolerance in Children: A Narrative Review. Nutrients 2021, 13, 1486. [Google Scholar] [CrossRef] [PubMed]
- Wantke, F.; Götz, M.; Jarisch, R. Histamine-free diet: Treatment of choice for histamine-induced food intolerance and supporting treatment for chronic headaches. Clin. Exp. Allergy 1993, 23, 982–985. [Google Scholar] [CrossRef] [PubMed]
- Panula, P.; Nuutinen, S. The histaminergic network in the brain: Basic organization and role in disease. Nat. Rev. Neurosci. 2013, 14, 472–487. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.C.; Arrang, J.M.; Garbarg, M.; Pollard, H.; Ruat, M. Histaminergic transmission in the mammalian brain. Physiol. Rev. 1991, 71, 1–51. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.E.; Stevens, D.R.; Haas, H.L. The physiology of brain histamine. Prog. Neurobiol. 2001, 63, 637–672. [Google Scholar] [CrossRef]
- Cheng, L.; Liu, J.; Chen, Z. The Histaminergic System in Neuropsychiatric Disorders. Biomolecules 2021, 11, 1345. [Google Scholar] [CrossRef]
- Mayes, S.D.; Calhoun, S.L.; Waschbusch, D.A. Relationship between sluggish cognitive tempo and sleep, psychological, somatic, and cognitive problems and impairment in children with autism and children with ADHD. Clin. Child Psychol. Psychiatry 2021, 26, 518–530. [Google Scholar] [CrossRef]
- Hersey, M.; Hashemi, P.; Reagan, L.P. Integrating the monoamine and cytokine hypotheses of depression: Is histamine the missing link? Eur. J. Neurosci. 2022, 55, 2895–2911. [Google Scholar] [CrossRef]
- Hegvik, T.A.; Waløen, K.; Pandey, S.K.; Faraone, S.V.; Haavik, J.; Zayats, T. Druggable genome in attention deficit/hyperactivity disorder and its co-morbid conditions. New avenues for treatment. Mol. Psychiatry 2021, 26, 4004–4015. [Google Scholar] [CrossRef]
- Garcia-Argibay, M.; du Rietz, E.; Lu, Y.; Martin, J.; Haan, E.; Lehto, K.; Bergen, S.E.; Lichtenstein, P.; Larsson, H.; Brikell, I. The role of ADHD genetic risk in mid-to-late life somatic health conditions. Transl. Psychiatry 2022, 12, 152. [Google Scholar] [CrossRef]
- Du Rietz, E.; Brikell, I.; Butwicka, A.; Leone, M.; Chang, Z.; Cortese, S.; D’Onofrio, B.M.; Hartman, C.A.; Lichtenstein, P.; Faraone, S.V.; et al. Mapping phenotypic and aetiological associations between ADHD and physical conditions in adulthood in Sweden: A genetically informed register study. Lancet Psychiatry 2021, 8, 774–783. [Google Scholar] [CrossRef]
- Craig, S.G.; Weiss, M.D.; Hudec, K.L.; Gibbons, C. The Functional Impact of Sleep Disorders in Children with ADHD. J. Atten. Disord. 2017, 24, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Faraone, S.V. Attention-deficit hyperactivity disorder. Lancet 2005, 366, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Wilens, T.E.; Martelon, M.; Joshi, G.; Bateman, C.; Fried, R.; Petty, C.; Biederman, J. Does ADHD predict substance-use disorders? A 10-year follow-up study of young adults with ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Moreira-Maia, C.R.; St Fleur, D.; Morcillo-Peñalver, C.; Rohde, L.A.; Faraone, S.V. Association between ADHD and Obesity: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2016, 173, 34–43. [Google Scholar] [CrossRef]
- Medzhitov, R. Inflammation 2010: New adventures of an old flame. Cell 2010, 140, 771–776. [Google Scholar] [CrossRef]
- Galaburda, A.M. The testosterone hypothesis: Assessment since Geschwind and Behan, 1982. Ann. Dyslexia 1990, 40, 18–38. [Google Scholar] [CrossRef]
- Geschwind, N.; Galaburda, A.M. Cerebral lateralization. Biological mechanisms, associations, and pathology: I. A hypothesis and a program for research. Arch. Neurol. 1985, 42, 428–459. [Google Scholar] [CrossRef]
- Geschwind, N.; Galaburda, A.M. Cerebral lateralization. Biological mechanisms, associations, and pathology: II. A hypothesis and a program for research. Arch. Neurol. 1985, 42, 521–552. [Google Scholar] [CrossRef]
- Schmitt, J.; Romanos, M.; Schmitt, N.M.; Meurer, M.; Kirch, W. Atopic eczema and attention-deficit/hyperactivity disorder in a population-based sample of children and adolescents. JAMA 2009, 301, 724–726. [Google Scholar] [CrossRef]
- Romanos, M.; Gerlach, M.; Warnke, A.; Schmitt, J. Association of attention-deficit/hyperactivity disorder and atopic eczema modified by sleep disturbance in a large population-based sample. J. Epidemiol. Community Health 2010, 64, 269–273. [Google Scholar] [CrossRef]
- Camfferman, D.; Kennedy, J.D.; Gold, M.; Simpson, C.; Lushington, K. Sleep and neurocognitive functioning in children with eczema. Int. J. Psychophysiol. 2013, 89, 265–272. [Google Scholar] [CrossRef]
- Tsai, J.D.; Chang, S.N.; Mou, C.H.; Sung, F.C.; Lue, K.H. Association between atopic diseases and attention-deficit/hyperactivity disorder in childhood: A population-based case-control study. Ann. Epidemiol. 2013, 23, 185–188. [Google Scholar] [CrossRef]
- Yaghmaie, P.; Koudelka, C.W.; Simpson, E.L. Mental health comorbidity in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2013, 131, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Genuneit, J.; Braig, S.; Brandt, S.; Wabitsch, M.; Florath, I.; Brenner, H.; Rothenbacher, D. Infant atopic eczema and subsequent attention-deficit/hyperactivity disorder—A prospective birth cohort study. Pediatr. Allergy Immunol. 2014, 25, 51–56. [Google Scholar] [CrossRef]
- Chen, M.H.; Su, T.P.; Chen, Y.S.; Hsu, J.W.; Huang, K.L.; Chang, W.H.; Chen, T.J.; Pan, T.L.; Bai, Y.M. Is atopy in early childhood a risk factor for ADHD and ASD? a longitudinal study. J. Psychosom. Res. 2014, 77, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Lee, M.Y.; Ha, M.; Yoo, S.J.; Paik, K.C.; Lim, J.H.; Sakong, J.; Lee, C.G.; Kang, D.M.; Hong, S.J.; et al. The associations between ADHD and asthma in Korean children. BMC Psychiatry 2014, 14, 70. [Google Scholar] [CrossRef]
- Suwan, P.; Akaramethathip, D.; Noipayak, P. Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD). Asian Pac. J. Allergy Immunol. 2011, 29, 57–65. [Google Scholar] [PubMed]
- Gaitens, T.; Kaplan, B.J.; Freigang, B. Absence of an association between IgE-mediated atopic responsiveness and ADHD symptomatology. J. Child Psychol. Psychiatry 1998, 39, 427–431. [Google Scholar] [CrossRef] [PubMed]
- McGee, R.; Stanton, W.R.; Sears, M.R. Allergic disorders and attention deficit disorder in children. J. Abnorm. Child Psychol. 1993, 21, 79–88. [Google Scholar] [CrossRef]
- Tsai, C.J.; Chou, P.H.; Cheng, C.; Lin, C.H.; Lan, T.H.; Lin, C.C. Asthma in patients with attention-deficit/hyperactivity disorder: A nationwide population-based study. Ann. Clin. Psychiatry 2014, 26, 254–260. [Google Scholar] [PubMed]
- Yuksel, H.; Sogut, A.; Yilmaz, O. Attention deficit and hyperactivity symptoms in children with asthma. J. Asthma 2008, 45, 545–547. [Google Scholar] [CrossRef] [PubMed]
- Blackman, J.A.; Gurka, M.J. Developmental and behavioral comorbidities of asthma in children. J. Dev. Behav. Pediatr. 2007, 28, 92–99. [Google Scholar] [CrossRef]
- Mogensen, N.; Larsson, H.; Lundholm, C.; Almqvist, C. Association between childhood asthma and ADHD symptoms in adolescence—A prospective population-based twin study. Allergy 2011, 66, 1224–1230. [Google Scholar] [CrossRef] [PubMed]
- Hak, E.; de Vries, T.W.; Hoekstra, P.J.; Jick, S.S. Association of childhood attention-deficit/hyperactivity disorder with atopic diseases and skin infections? A matched case-control study using the General Practice Research Database. Ann. Allergy Asthma Immunol. 2013, 111, 102–106.E2. [Google Scholar] [CrossRef]
- Holmberg, K.; Lundholm, C.; Anckarsater, H.; Larsson, H.; Almqvist, C. Impact of asthma medication and familial factors on the association between childhood asthma and attention-deficit/hyperactivity disorder: A combined twin- and register-based study: Epidemiology of Allergic Disease. Clin. Exp. Allergy 2015, 45, 964–973. [Google Scholar] [CrossRef]
- Biederman, J.; Milberger, S.; Faraone, S.V.; Guite, J.; Warburton, R. Associations between childhood asthma and ADHD: Issues of psychiatric comorbidity and familiality. J. Am. Acad. Child Adolesc. Psychiatry 1994, 33, 842–848. [Google Scholar] [CrossRef]
- Hammerness, P.; Monuteaux, M.C.; Faraone, S.V.; Gallo, L.; Murphy, H.; Biederman, J. Reexamining the familial association between asthma and ADHD in girls. J. Atten. Disord. 2005, 8, 136–143. [Google Scholar] [CrossRef]
- Yang, M.T.; Lee, W.T.; Liang, J.S.; Lin, Y.J.; Fu, W.M.; Chen, C.C. Hyperactivity and impulsivity in children with untreated allergic rhinitis: Corroborated by rating scale and continuous performance test. Pediatr. Neonatol. 2014, 55, 168–174. [Google Scholar] [CrossRef]
- Chou, P.H.; Lin, C.C.; Lin, C.H.; Loh, E.W.; Chan, C.H.; Lan, T.H. Prevalence of allergic rhinitis in patients with attention-deficit/hyperactivity disorder: A population-based study. Eur. Child Adolesc. Psychiatry 2013, 22, 301–307. [Google Scholar] [CrossRef]
- Miyazaki, C.; Koyama, M.; Ota, E.; Swa, T.; Mlunde, L.B.; Amiya, R.M.; Tachibana, Y.; Yamamoto-Hanada, K.; Mori, R. Allergic diseases in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 120. [Google Scholar] [CrossRef] [PubMed]
- Schans, J.V.; Çiçek, R.; de Vries, T.W.; Hak, E.; Hoekstra, P.J. Association of atopic diseases and attention-deficit/hyperactivity disorder: A systematic review and meta-analyses. Neurosci. Biobehav. Rev. 2017, 74 Pt A, 139–148. [Google Scholar] [CrossRef]
- Chuang, Y.C.; Wang, C.Y.; Huang, W.L.; Wang, L.J.; Kuo, H.C.; Chen, Y.C.; Huang, Y.J. Two meta-analyses of the association between atopic diseases and core symptoms of attention deficit hyperactivity disorder. Sci. Rep. 2022, 12, 3377. [Google Scholar] [CrossRef] [PubMed]
- Dalsgaard, S. More Evidence Linking Autoimmune Diseases to Attention-Deficit/Hyperactivity Disorder. JAMA Pediatr. 2021, 175, e205502. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.R.; Benros, M.E.; Dalsgaard, S. Associations Between Autoimmune Diseases and Attention-Deficit/Hyperactivity Disorder: A Nationwide Study. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 234–240.E1. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.M.; Lee, C.C.; Lin, T.C.; Chung, C.H.; Chen, C.Y.; Chang, P.K.; Hsiao, C.W.; Sun, C.A.; Tzeng, N.S.; Chien, W.C. Risk of Colorectal Cancer in Patients with Attention-Deficit Hyperactivity Disorder: A Nationwide, Population-Based Cohort Study. Front. Psychiatry 2021, 12, 537137. [Google Scholar] [CrossRef]
- Jansson, A.K.; Söderling, J.; Reutfors, J.; Thor, A.; Sköld, C.; Cohn-Cedermark, G.; Ståhl, O.; Smedby, K.E.; Pettersson, A.; Glimelius, I. Risk and mortality of testicular cancer in patients with neurodevelopmental or other psychiatric disorders. Br. J. Cancer 2023, 128, 2261–2269. [Google Scholar] [CrossRef]
- Thapar, A. Discoveries on the Genetics of ADHD in the 21st Century: New Findings and Their Implications Intellectual Disability and Attention-Deficit/Hyperactivity Disorder: What Does the Clinical and Genetic Overlap Mean for Practice and Research? Am. J. Psychiatry 2018, 175, 943–950. [Google Scholar] [CrossRef]
- Li, H.; Xiao, Y.; Li, Q.; Yao, J.; Yuan, X.; Zhang, Y.; Yin, X.; Saito, Y.; Fan, H.; Li, P.; et al. The allergy mediator histamine confers resistance to immunotherapy in cancer patients via activation of the macrophage histamine receptor H1. Cancer Cell 2022, 40, 36–52.E9. [Google Scholar] [CrossRef]
- Yu, Y.; Sun, Y.; Wang, Y.; Wang, B.; Chen, C.; Tan, X.; Lu, Y.; Wang, N. Immune-mediated diseases and risk of incident cardiovascular diseases: A prospective cohort study. Rheumatology 2023, kead266. [Google Scholar] [CrossRef]
- Riksen, N.P.; Bekkering, S.; Mulder, W.J.M.; Netea, M.G. Trained immunity in atherosclerotic cardiovascular disease. Nat. Rev. Cardiol. 2023, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Saheera, S.; Potnuri, A.G.; Guha, A.; Palaniyandi, S.S.; Thandavarayan, R.A. Histamine 2 receptors in cardiovascular biology: A friend for the heart. Drug Discov. Today 2022, 27, 234–245. [Google Scholar] [CrossRef]
- O’Neill, L.A.; Kishton, R.J.; Rathmell, J. A guide to immunometabolism for immunologists. Nat. Rev. Immunol. 2016, 16, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Sarasola, M.P.; Táquez Delgado, M.A.; Nicoud, M.B.; Medina, V.A. Histamine in cancer immunology and immunotherapy. Current status and new perspectives. Pharmacol. Res. Perspect. 2021, 9, e00778. [Google Scholar] [CrossRef]
- Takahashi, N.; Nishimura, T.; Harada, T.; Okumura, A.; Iwabuchi, T.; Rahman, M.S.; Kuwabara, H.; Takagai, S.; Usui, N.; Makinodan, M.; et al. Interaction of genetic liability for attention deficit hyperactivity disorder (ADHD) and perinatal inflammation contributes to ADHD symptoms in children. Brain Behav. Immun. Health 2023, 30, 100630. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Lee, H.; Choi, Y.; Kang, H.; Jeon, S.J.; Ryu, J.H.; Kim, H.J.; Cheong, J.H.; Lim, S.; Kim, B.N.; et al. Maturational delay and asymmetric information flow of brain connectivity in SHR model of ADHD revealed by topological analysis of metabolic networks. Sci. Rep. 2020, 10, 3197. [Google Scholar] [CrossRef] [PubMed]
- Geschwind, N.; Behan, P. Left-handedness: Association with immune disease, migraine, and developmental learning disorder. Proc. Natl. Acad. Sci. USA 1982, 79, 5097–5100. [Google Scholar] [CrossRef]
- Speer, F. Allergy and migraine: A clinical study. Headache 1971, 11, 63–67. [Google Scholar] [CrossRef]
- Weinstein, R.E.; Pieper, D.R. Altered cerebral dominance in an atopic population. Brain Behav. Immun. 1988, 2, 235–241. [Google Scholar] [CrossRef]
- Smith, J. Left-handedness: Its association with allergic disease. Neuropsychologia 1987, 25, 665–674. [Google Scholar] [CrossRef]
- Peters, M.; Reimers, S.; Manning, J.T. Hand preference for writing and associations with selected demographic and behavioral variables in 255,100 subjects: The BBC internet study. Brain Cogn. 2006, 62, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Biehl, K.; Frese, A.; Marziniak, M.; Husstedt, I.W.; Evers, S. Migraine and left-handedness are not associated. A new case-control study and meta-analysis. Cephalalgia 2008, 28, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Fasmer, O.B.; Akiskal, H.S.; Hugdahl, K.; Oedegaard, K.J. Non-right-handedness is associated with migraine and soft bipolarity in patients with mood disorders. J. Affect. Disord. 2008, 108, 217–224. [Google Scholar] [CrossRef]
- Aygül, R.; Dane, S.; Ulvi, H. Handedness, eyedness, and crossed hand-eye dominance in male and female patients with migraine with and without aura: A pilot study. Percept. Mot. Ski. 2005, 100 Pt 2, 1137–1142. [Google Scholar] [CrossRef]
- Endicott, N.A. Patterns of functional brain organization and migraine. Cephalalgia 2004, 24, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Hynd, G.W.; Semrud-Clikeman, M.; Lorys, A.R.; Novey, E.S.; Eliopulos, D. Brain morphology in developmental dyslexia and attention deficit disorder/hyperactivity. Arch. Neurol. 1990, 47, 919–926. [Google Scholar] [CrossRef]
- Hynd, G.W.; Hall, J.; Novey, E.S.; Eliopulos, D.; Black, K.; Gonzalez, J.J.; Edmonds, J.E.; Riccio, C.; Cohen, M. Dyslexia and corpus callosum morphology. Arch. Neurol. 1995, 52, 32–38. [Google Scholar] [CrossRef]
- Kibby, M.Y.; Kroese, J.M.; Krebbs, H.; Hill, C.E.; Hynd, G.W. The pars triangularis in dyslexia and ADHD: A comprehensive approach. Brain Lang. 2009, 111, 46–54. [Google Scholar] [CrossRef]
- Kibby, M.Y.; Pavawalla, S.P.; Fancher, J.B.; Naillon, A.J.; Hynd, G.W. The relationship between cerebral hemisphere volume and receptive language functioning in dyslexia and attention-deficit hyperactivity disorder (ADHD). J. Child Neurol. 2009, 24, 438–448. [Google Scholar] [CrossRef]
- Nastou, E.; Ocklenburg, S.; Hoogman, M.; Papadatou-Pastou, M. Handedness in ADHD: Meta-Analyses. Neuropsychol. Rev. 2022, 32, 877–892. [Google Scholar] [CrossRef]
- Goez, H.; Zelnik, N. Handedness in patients with developmental coordination disorder. J. Child Neurol. 2008, 23, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Sabuncuoglu, O. Traumatic dental injuries and attention-deficit/hyperactivity disorder: Is there a link? Dent. Traumatol. 2007, 23, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, R.; Kuban, M.E.; Klassen, P.; Dickey, R.; Christensen, B.K.; Cantor, J.M.; Blak, T. Self-reported head injuries before and after age 13 in pedophilic and nonpedophilic men referred for clinical assessment. Arch. Sex. Behav. 2003, 32, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, P.; Ruggiero, A.; Diociaiuti, L.; Paoletti, F.P.; Chiozza, M.L.; Caione, P. Primary nocturnal enuresis and left-handedness. Scand. J. Urol. Nephrol. 2001, 35, 184–185. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Goto, Y.; Lee, Y.A. Histamine H3 receptor antagonists ameliorate attention deficit/hyperactivity disorder-like behavioral changes caused by neonatal habenula lesion. Behav. Pharmacol. 2018, 29, 71–78. [Google Scholar] [CrossRef]
- Felger, J.C.; Lotrich, F.E. Inflammatory cytokines in depression: Neurobiological mechanisms and therapeutic implications. Neuroscience 2013, 246, 199–229. [Google Scholar] [CrossRef]
- Grisanti, L.A.; Perez, D.M.; Porter, J.E. Modulation of immune cell function by α(1)-adrenergic receptor activation. Curr. Top. Membr. 2011, 67, 113–138. [Google Scholar] [CrossRef]
- Kay, G.G.; Harris, A.G. Loratadine: A non-sedating antihistamine. Review of its effects on cognition, psychomotor performance, mood and sedation. Clin. Exp. Allergy 1999, 29 (Suppl. S3), 147–150. [Google Scholar] [CrossRef]
- Provensi, G.; Costa, A.; Izquierdo, I.; Blandina, P.; Passani, M.B. Brain histamine modulates recognition memory: Possible implications in major cognitive disorders. Br. J. Pharmacol. 2020, 177, 539–556. [Google Scholar] [CrossRef]
- Lin, C.H.; Lane, H.Y. Blood D-Amino Acid Oxidase Levels Increased with Cognitive Decline among People with Mild Cognitive Impairment: A Two-Year Prospective Study. Int. J. Neuropsychopharmacol. 2022, 25, 660–665. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Nakamura, T.; Yanai, K. Histamine N-Methyltransferase in the Brain. Int. J. Mol. Sci. 2019, 20, 737. [Google Scholar] [CrossRef]
- Horner, W.E.; Johnson, D.E.; Schmidt, A.W.; Rollema, H. Methylphenidate and atomoxetine increase histamine release in rat prefrontal cortex. Eur. J. Pharmacol. 2007, 558, 96–97. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.L.; Yang, J.; Lei, G.F.; Wang, G.J.; Wang, Y.W.; Sun, R.P. Atomoxetine increases histamine release and improves learning deficits in an animal model of attention-deficit hyperactivity disorder: The spontaneously hypertensive rat. Basic Clin. Pharmacol. Toxicol. 2008, 102, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Arnsten, A.F. Fundamentals of attention-deficit/hyperactivity disorder: Circuits and pathways. J. Clin. Psychiatry 2006, 67 (Suppl. S8), 7–12. [Google Scholar] [PubMed]
- Tobajas, Y.; Alemany-Fornés, M.; Samarra, I.; Romero-Giménez, J.; Tintoré, M.; Del Pino, A.; Canela, N.; Del Bas, J.M.; Ortega-Olivé, N.; de Lecea, C.; et al. Interaction of Diamine Oxidase with Psychostimulant Drugs for ADHD Management. J. Clin. Med. 2023, 12, 4666. [Google Scholar] [CrossRef]
- Fuhrmann, S.; Tesch, F.; Romanos, M.; Abraham, S.; Schmitt, J. ADHD in school-age children is related to infant exposure to systemic H1-antihistamines. Allergy 2020, 75, 2956–2957. [Google Scholar] [CrossRef] [PubMed]
- Gober, H.J.; Li, K.H.; Yan, K.; Bailey, A.J.; Carleton, B.C. Hydroxyzine Use in Preschool Children and Its Effect on Neurodevelopment: A Population-Based Longitudinal Study. Front. Psychiatry 2021, 12, 721875. [Google Scholar] [CrossRef]
- Schmitt, J.; Buske-Kirschbaum, A.; Tesch, F.; Trikojat, K.; Stephan, V.; Abraham, S.; Bauer, A.; Nemat, K.; Plessow, F.; Roessner, V.; et al. Increased attention-deficit/hyperactivity symptoms in atopic dermatitis are associated with history of antihistamine use Prenatal and perinatal risk factors for attention-deficit/hyperactivity disorder. Allergy 2018, 73, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Buske-Kirschbaum, A.; Roessner, V. Is atopic disease a risk factor for attention-deficit/hyperactivity disorder? A systematic review. Allergy 2010, 65, 1506–1524. [Google Scholar] [CrossRef]
- Singer, A.G.; Kosowan, L.; Soller, L.; Chan, E.S.; Nankissoor, N.N.; Phung, R.R.; Abrams, E.M. Prevalence of Physician-Reported Food Allergy in Canadian Children. J. Allergy Clin. Immunol. Pract 2021, 9, 193–199. [Google Scholar] [CrossRef]
- Berkey, F.; Wiedemer, J. Atopic dermatitis: More than just a rash. J. Fam. Pract 2021, 70, 13–19. [Google Scholar] [CrossRef]
- Arnold, L.E.; Clark, D.L.; Sachs, L.A.; Jakim, S.; Smithies, C. Vestibular and visual rotational stimulation as treatment for attention deficit and hyperactivity. Am. J. Occup. Ther. 1985, 39, 84–91. [Google Scholar] [CrossRef]
- Sadek, B.; Saad, A.; Sadeq, A.; Jalal, F.; Stark, H. Histamine H3 receptor as a potential target for cognitive symptoms in neuropsychiatric diseases. Behav. Brain Res. 2016, 312, 415–430. [Google Scholar] [CrossRef] [PubMed]
- Herring, W.J.; Wilens, T.E.; Adler, L.A.; Baranak, C.; Liu, K.; Snavely, D.B.; Lines, C.R.; Michelson, D. Randomized controlled study of the histamine H3 inverse agonist MK-0249 in adult attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2012, 73, e891–e898. [Google Scholar] [CrossRef] [PubMed]
- Weisler, R.H.; Pandina, G.J.; Daly, E.J.; Cooper, K.; Gassmann-Mayer, C. Randomized clinical study of a histamine H3 receptor antagonist for the treatment of adults with attention-deficit hyperactivity disorder. CNS Drugs 2012, 26, 421–434. [Google Scholar] [CrossRef]
- Prast, H.; Tran, M.H.; Fischer, H.; Kraus, M.; Lamberti, C.; Grass, K.; Philippu, A. Histaminergic neurons modulate acetylcholine release in the ventral striatum: Role of H3 histamine receptors. Naunyn-Schmiedeberg’s Arch. Pharmacol. 1999, 360, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Hutson, P.H.; Heins, M.S.; Folgering, J.H. Effects of lisdexamfetamine alone and in combination with s-citalopram on acetylcholine and histamine efflux in the rat pre-frontal cortex and ventral hippocampus. J. Neurochem. 2015, 134, 693–703. [Google Scholar] [CrossRef]
- Tracey, K.J. The inflammatory reflex. Nature 2002, 420, 853–859. [Google Scholar] [CrossRef]
- Kutuk, M.O.; Tufan, A.E.; Guler, G.; Yalin, O.O.; Altintas, E.; Bag, H.G.; Uluduz, D.; Toros, F.; Aytan, N.; Kutuk, O.; et al. Migraine and associated comorbidities are three times more frequent in children with ADHD and their mothers. Brain Dev. 2018, 40, 857–864. [Google Scholar] [CrossRef]
- Hansen, T.F.; Hoeffding, L.K.; Kogelman, L.; Haspang, T.M.; Ullum, H.; Sorensen, E.; Erikstrup, C.; Pedersen, O.B.; Nielsen, K.R.; Hjalgrim, H.; et al. Comorbidity of migraine with ADHD in adults. BMC Neurol. 2018, 18, 147. [Google Scholar] [CrossRef]
- Meza-Velázquez, R.; López-Márquez, F.; Espinosa-Padilla, S.; Rivera-Guillen, M.; Ávila-Hernández, J.; Rosales-González, M. Association of diamine oxidase and histamine N-methyltransferase polymorphisms with presence of migraine in a group of Mexican mothers of children with allergies. Neurologia 2017, 32, 500–507. [Google Scholar] [CrossRef]
- Gaur, S. The Association between ADHD and Celiac Disease in Children. Children 2022, 9, 781. [Google Scholar] [CrossRef] [PubMed]
- Tryphonas, H.; Trites, R. Food allergy in children with hyperactivity, learning disabilities and/or minimal brain dysfunction. Ann. Allergy 1979, 42, 22–27. [Google Scholar] [PubMed]
- Sambu, S.; Hemaram, U.; Murugan, R.; Alsofi, A.A. Toxicological and Teratogenic Effect of Various Food Additives: An Updated Review. BioMed Res. Int. 2022, 2022, 6829409. [Google Scholar] [CrossRef]
- Stevenson, J.; Sonuga-Barke, E.; McCann, D.; Grimshaw, K.; Parker, K.M.; Rose-Zerilli, M.J.; Holloway, J.W.; Warner, J.O. The role of histamine degradation gene polymorphisms in moderating the effects of food additives on children’s ADHD symptoms. Am. J. Psychiatry 2010, 167, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhang, X.; Jin, H.; Chen, L.; Ji, J.; Zhang, Z. Histamine Intolerance—A Kind of Pseudoallergic Reaction. Biomolecules 2022, 12, 454. [Google Scholar] [CrossRef]
- Nurhan, A.D.; Gani, M.A.; Budiatin, A.S.; Siswodihardjo, S.; Khotib, J. Molecular docking studies of Nigella sativa L. and Curcuma xanthorrhiza Roxb secondary metabolites against histamine N-methyltransferase with their ADMET prediction. J. Basic Clin. Physiol. Pharmacol. 2021, 32, 795–802. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Tension | Fatigue | ||
|---|---|---|---|
| Motor | Sensory | Motor | Sensory |
| Exaggerated, accelerated, and continuous motor function | Unusual sensitivity (oversensitivity) to innocuous stimuli (i.e., noise and temperature change, oversensitivity to pain) | Tiring very rapidly and easily | Being in an inactive, torpor, sluggish, sleepy, and apathetic |
| Impatient | Irritability | Complaints of muscular weakness and achiness | |
| Talkative | Distractibility | ||
| Fidgety | Short attention span | ||
| Poorly coordinated | Excitability | ||
| Accident prone | Insomnia | ||
| Histamine Receptor | Area and Cells | Function | CNS Pathology Involved |
|---|---|---|---|
| H1 | Cerebral cortex, thalamus, locus coeruleus, raphe nucleus, astrocytes | Arousal and sleep-wakefulness | Narcolepsy Schizophrenia Alzheimer’s Disease |
| H2 | Cerebral cortex, basal ganglia, hipoccampus, amygdala | Motoric | Schizophrenia Parkinson’s Disease Tourette’s syndrome |
| H3 | All CNS | Regulates the release of other neurotransmitters, such as glutamate, GABA, acetylcholine, and dopamine both in CNS and periphery | Schizophrenia Alzheimer’s Disease Parkinson’s Disease Tourette’s síndrome ADHD |
| H4 | Hematopoietic and immune cells (eosinophils, mast cells, and dendritic cells) | Inflammatory processes |
| SATFS | Somatic Diseases Associated with ADHD | HIT and/or DAO Deficiency (Histamine Receptors) |
|---|---|---|
| Gastrointestinal | Gastrointestinal | Gastrointestinal (H1/H2) |
| Bloating | ||
| Postprandial fullness | ||
| Diarrhea | Diarrhea/Loose stool | |
| Abdominal pain | Ulcer or chronic gastritis | Abdominal pain |
| Constipation | Constipation | |
| Colic | Acute appendicitis | Intestinal colic |
| Belching | ||
| Vomiting | Nausea/Vomiting | |
| Food and drug sensitivities (Gastrointestinal allergies) | Celiac disease and other food allergies | Food sensitivities and allergies |
| Increased salivation | ||
| Fatty and alcohol liver disease, gallstone disease | ||
| Inflammatory bowel disease | Chrohn/colitis | |
| Skin | Skin | Skin (H1) |
| Psoriasis | Pruritus | |
| Eczema | Atopia (Eczema) | Rash, eczema, urticaria |
| Edema (infraorbital) Deep red discoloration under the eyes | Swollen, reddened eyelids Flush | |
| Hyperhidrosis, lacrimation | Excessive sudden sweating | |
| Vitiligo (also autoimmune) | ||
| Nervous system | Nervous system | Nervous system (H3) |
| Sluggish, torpor | Sleep disorders | Dizziness |
| Headache (unilateral) | Headache (including Migraine) | Headache (Migraine) |
| Nightmares, bad sleep | Sleep problems (insomnia) | Insomnia, circadian rhythm problems, obstructive apnea |
| Epilepsy | ||
| Delirium | Dementia and Parkinson’s | |
| Circulatory system | Circulatory system | Circulatory system (H1/H2) |
| Tachycardia, palpitations, and/or arrhythmia | ||
| Peripheral vascular disease, hypertension | Hypotension | |
| Heart failure, ischemic heart disease, hypertension, stroke | Collapse | |
| Respiratory system | Respiratory system | Respiratory system (H1) |
| Blocked nose | Allergic rhinitis | Allergies (Rhinorrhea, nose congestion, sneezing) |
| Rapid fatigue | Chronic obstructive pulmonary disease (COPD) | Dyspnea, chronic coughing |
| Asthma | Asthma | Asthma |
| Musculoskeletal | Musculoskeletal | Musculoskeletal |
| Vague, widespread aching | Fibromyalgia | Fibromyalgia |
| Muscular weakness | Arthrosis, dorsalgia, rheumatoid arthritis | Muscle and joint pain |
| Genitourinary | Genitourinary | Genitourinary (H1/H2) |
| Enuresis, increased bladder tone | Enuresis | Enuresis, overactive bladder |
| Urinary infection | Urolithiasis and kidney infections | |
| Glomerular disease | Hypersensitivity to NSAIDs | |
| Dysmenorrhea, endometriosis | ||
| Endocrine, metabolic or autoimmune | Endocrine, metabolic or autoimmune | Endocrine, metabolic or autoimmune |
| Type 1 and 2 diabetes | ||
| Obesity | ||
| Thyroid disorders |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blasco-Fontecilla, H. Is Histamine and Not Acetylcholine the Missing Link between ADHD and Allergies? Speer Allergic Tension Fatigue Syndrome Re-Visited. J. Clin. Med. 2023, 12, 5350. https://doi.org/10.3390/jcm12165350
Blasco-Fontecilla H. Is Histamine and Not Acetylcholine the Missing Link between ADHD and Allergies? Speer Allergic Tension Fatigue Syndrome Re-Visited. Journal of Clinical Medicine. 2023; 12(16):5350. https://doi.org/10.3390/jcm12165350
Chicago/Turabian StyleBlasco-Fontecilla, Hilario. 2023. "Is Histamine and Not Acetylcholine the Missing Link between ADHD and Allergies? Speer Allergic Tension Fatigue Syndrome Re-Visited" Journal of Clinical Medicine 12, no. 16: 5350. https://doi.org/10.3390/jcm12165350
APA StyleBlasco-Fontecilla, H. (2023). Is Histamine and Not Acetylcholine the Missing Link between ADHD and Allergies? Speer Allergic Tension Fatigue Syndrome Re-Visited. Journal of Clinical Medicine, 12(16), 5350. https://doi.org/10.3390/jcm12165350