

Stratification of Pediatric COVID-19 Cases Using Inflammatory Biomarker Profiling and Machine Learning
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design
2.2. Methods
2.2.1. Serum Protein/Laboratory Data/EHR Data Collection
2.2.2. Confirmation of SARS-CoV-2 Infection
2.2.3. Cytokine/Chemokine Profiling
2.2.4. Computation
2.2.5. Univariate Discrimination with the Wilcoxon Rank-Sum Test
2.2.6. Multivariate Cross-Validated L1 Regularized Logistic Regression Classification
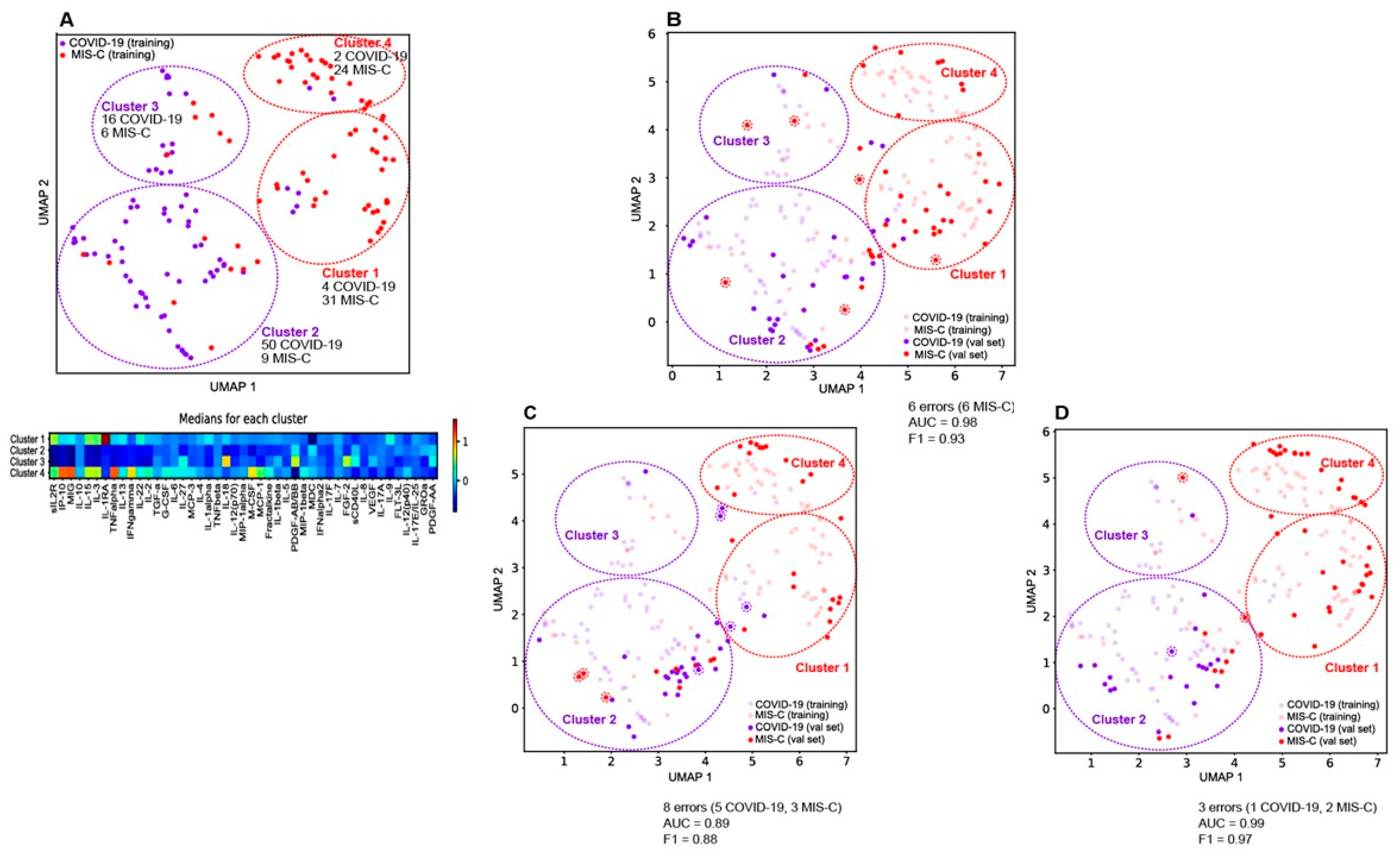
2.2.7. Multidimensional Data Representation
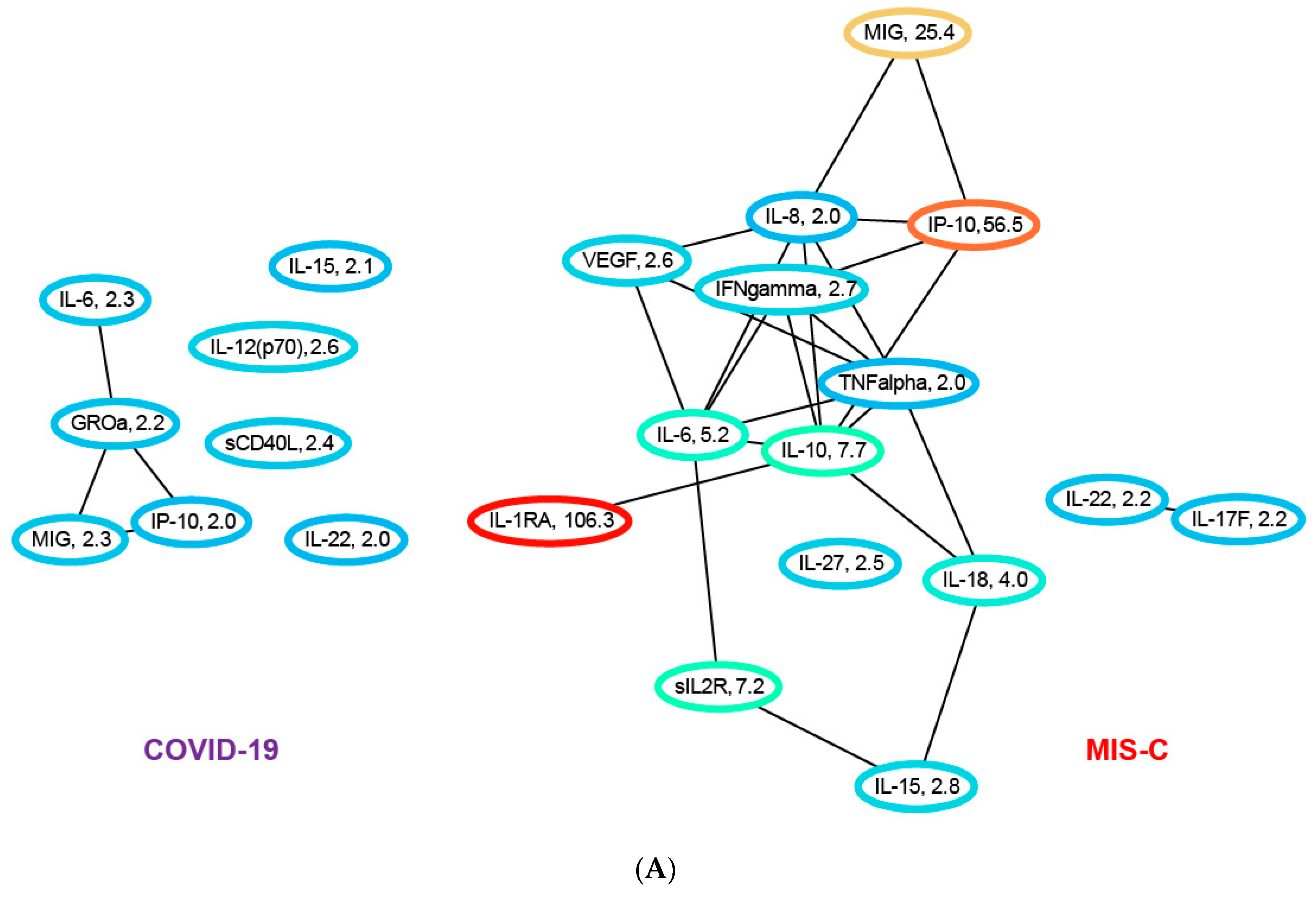
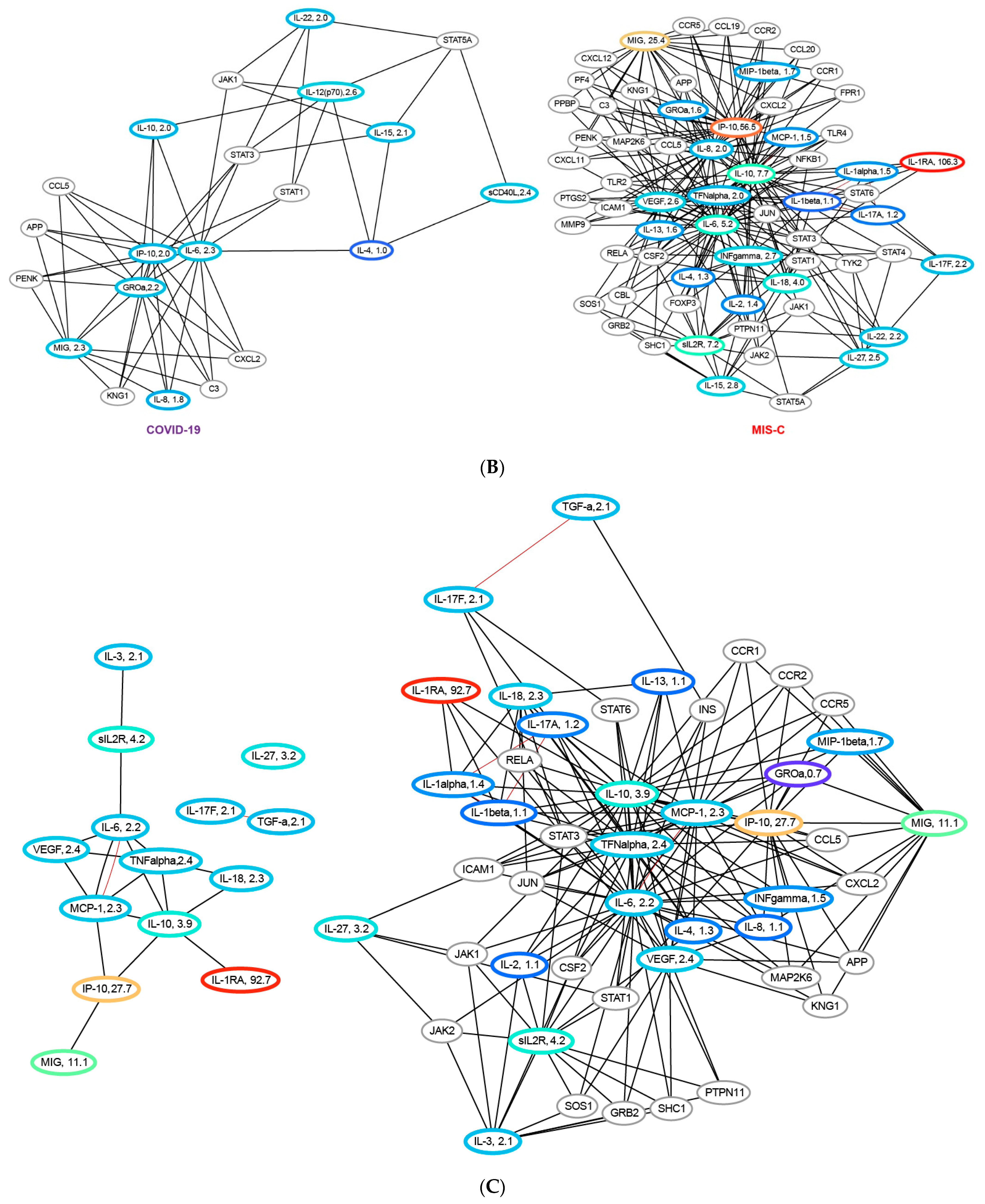
2.2.8. Network Analysis
3. Results
3.1. Clinical Characteristics of the Training Cohort and Validation Sets
3.2. Laboratory Characteristics of the Training Cohort and Validation Sets
3.3. Cytokine/Chemokine Profiles of the Training Cohort
3.4. Machine Learning Models Differentiating COVID-19 from MIS-C
3.5. Generalizability of Model to New Validation Sets
3.6. Network Analysis of the Cytokine/Chemokine Training Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Castagnoli, R.; Votto, M.; Licari, A.; Brambilla, I.; Bruno, R.; Perlini, S.; Rovida, F.; Baldanti, F.; Marseglia, G.L. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: A systematic review. JAMA Pediatr. 2020, 174, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Vogel, T.P.; Top, K.A.; Karatzios, C.; Hilmers, D.C.; Tapia, L.I.; Moceri, P.; Giovannini-Chami, L.; Wood, N.; Chandler, R.E.; Klein, N.P.; et al. Multisystem inflammatory syndrome in children and adults (MIS-C/A): Case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2021, 39, 3037–3049. [Google Scholar] [PubMed]
- Kwak, J.H.; Lee, S.-Y.; Choi, J.-W.; Disease, T.K.S.O.K. Clinical features, diagnosis, and outcomes of multisystem inflammatory syndrome in children associated with coronavirus disease 2019. Clin. Exp. Pediatr. 2021, 64, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.E.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA 2020, 324, 259–269. [Google Scholar] [CrossRef]
- Melo, A.K.G.; Milby, K.M.; Caparroz, A.L.M.A.; Pinto, A.C.P.N.; Santos, R.R.P.; Rocha, A.P.; Ferreira, G.A.; Souza, V.A.; Valadares, L.D.A.; Vieira, R.M.R.A.; et al. Biomarkers of cytokine storm as red flags for severe and fatal COVID-19 cases: A living systematic review and meta-analysis. PLoS ONE 2021, 16, e0253894. [Google Scholar] [CrossRef]
- Guimarães, D.; Pissarra, R.; Reis-Melo, A.; Guimarães, H. Multisystem inflammatory syndrome in children (MISC): A systematic review. Int. J. Clin. Pract. 2021, 75, e14450. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. Ser. B Methodol. 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Ng, A.Y. Feature selection, L 1 vs. L 2 regularization, and rotational invariance. In Proceedings of the Twenty-First International Conference on Machine Learning, Banff, AB, Canada, 4–8 July 2004. [Google Scholar] [CrossRef]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. (Eds.) An Introduction to Statistical Learning; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- McInnes, L.; Healy, J.; Melville, J. Umap: Uniform manifold approximation and projection for dimension reduction. arXiv Prepr. 2018, arXiv:180203426. [Google Scholar]
- Dorrity, M.W.; Saunders, L.M.; Queitsch, C.; Fields, S.; Trapnell, C. Dimensionality reduction by UMAP to visualize physical and genetic interactions. Nat. Commun. 2020, 11, 1537. [Google Scholar] [CrossRef]
- Becht, E.; McInnes, L.; Healy, J.; Dutertre, C.-A.; Kwok, I.W.H.; Ng, L.G.; Ginhoux, F.; Newell, E.W. Dimensionality reduction for visualizing single-cell data using UMAP. Nat. Biotechnol. 2019, 37, 38–44. [Google Scholar] [CrossRef]
- Szklarczyk, D.; Gable, A.L.; Nastou, K.C.; Lyon, D.; Kirsch, R.; Pyysalo, S.; Doncheva, N.T.; Legeay, M.; Fang, T.; Bork, T.; et al. The STRING database in 2021: Customizable protein–protein networks, and functional characterization of user-uploaded gene/measurement sets. Nucleic Acids Res. 2021, 49, D605–D612. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Yin, L.; Patel, J.; Tang, L.; Huang, Y. The inflammatory markers of multisystem inflammatory syndrome in children (MIS-C) and adolescents associated with COVID-19: A meta-analysis. J. Med. Virol. 2021, 93, 4358–4369. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.Y.; Day-Lewis, M.; Henderson, L.A.; Friedman, K.G.; Lo, J.; Roberts, J.E.; Lo, M.S.; Platt, C.D.; Chou, J.; Hoyt, K.J.; et al. Distinct clinical and immunological features of SARS–CoV-2–induced multisystem inflammatory syndrome in children. J. Clin. Investig. 2020, 130, 5942–5950. [Google Scholar] [CrossRef] [PubMed]
- Peart Akindele, N.; Kouo, T.; Karaba, A.H.; Gordon, O.; Fenstermacher, K.Z.; Beaudry, J.; Rubens, J.H.; Atik, C.C.; Zhou, W.; Ji, H.; et al. Distinct cytokine and chemokine dysregulation in hospitalized children with acute coronavirus disease 2019 and multisystem inflammatory syndrome with similar levels of nasopharyngeal severe acute respiratory syndrome coronavirus 2 shedding. J. Infect. Dis. 2021, 224, 606–615. [Google Scholar] [CrossRef]
- Sacco, K.; Castagnoli, R.; Vakkilainen, S.; Liu, C.; Delmonte, O.M.; Oguz, C.; Kaplan, I.M.; Alehashemi, S.; Burbelo, P.D.; Bhuyan, F.; et al. Immunopathological signatures in multisystem inflammatory syndrome in children and pediatric COVID-19. Nat. Med. 2022, 28, 1050–1062. [Google Scholar] [CrossRef]
- Gruber, C.N.; Patel, R.S.; Trachtman, R.; Lepow, L.; Amanat, F.; Krammer, F.; Wilson, K.M.; Onel, K.; Geanon, D.; Tuballes, K.; et al. Mapping systemic inflammation and antibody responses in multisystem inflammatory syndrome in children (MIS-C). Cell 2020, 183, 982–995.e14. [Google Scholar] [CrossRef]
- DeBiasi, R.L.; Harahsheh, A.S.; Srinivasalu, H.; Krishnan, A.; Sharron, M.P.; Parikh, K.; Smith, K.; Bell, M.; Michael, D.; Delaney, M.; et al. Multisystem inflammatory syndrome of children: Subphenotypes, risk factors, biomarkers, cytokine profiles, and viral sequencing. J. Pediatr. 2021, 237, 125–135.e18. [Google Scholar] [CrossRef]
- Diorio, C.; Shraim, R.; Vella, L.A.; Giles, J.R.; Baxter, A.E.; Oldridge, D.A.; Canna, S.W.; Henrickson, S.E.; McNerney, K.O.; Balamuth, F.; et al. Proteomic profiling of MIS-C patients indicates heterogeneity relating to interferon gamma dysregulation and vascular endothelial dysfunction. Nat. Commun. 2021, 12, 7222. [Google Scholar] [CrossRef]
- Ravichandran, S.; Tang, J.; Grubbs, G.; Lee, Y.; Pourhashemi, S.; Hussaini, L.; Lapp, S.A.; Jerris, R.C.; Singh, V.; Chahroudi, A.; et al. SARS-CoV-2 immune repertoire in MIS-C and pediatric COVID-19. Nat. Immunol. 2021, 22, 1452–1464. [Google Scholar] [CrossRef]
- Esteve-Sole, A.; Anton, J.; Pino-Ramirez, R.M.; Sanchez-Manubens, J.; Fumadó, V.; Fortuny, C.; Rios-Barnes, M.; Sanchez-De-Toledo, J.; Girona-Alarcón, M.; Mosquera, J.M.; et al. Similarities and differences between the immunopathogenesis of COVID-19–related pediatric multisystem inflammatory syndrome and Kawasaki disease. J. Clin. Investig. 2021, 131, e144554. [Google Scholar] [CrossRef]
- Coperchini, F.; Chiovato, L.; Ricci, G.; Croce, L.; Magri, F.; Rotondi, M. The cytokine storm in COVID-19: Further advances in our understanding the role of specific chemokines involved. Cytokine Growth Factor Rev. 2021, 58, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Gurlevik, S.L.; Ozsurekci, Y.; Sağ, E.; Oygar, P.D.; Kesici, S.; Akca, K.; Cuceoglu, M.K.; Basaran, O.; Göncü, S.; Karakaya, J.; et al. The difference of the inflammatory milieu in MIS-C and severe COVID-19. Pediatr. Res. 2022, 92, 1805–1814. [Google Scholar] [CrossRef]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; Tan, Z.; Zicari, S.; Ruggiero, A.; Pascucci, G.R.; et al. The immunology of multisystem inflammatory syndrome in children with COVID-19. Cell 2020, 183, 968–981.e7. [Google Scholar] [CrossRef]
- Kumar, D.; Rostad, C.A.; Jaggi, P.; Nunez, D.S.V.; Prince, C.; Lu, A.; Hussaini, L.; Nguyen, T.H.; Malik, S.; Ponder, L.A.; et al. Distinguishing immune activation and inflammatory signatures of multisystem inflammatory syndrome in children (MIS-C) versus hemophagocytic lymphohistiocytosis (HLH). J. Allergy Clin. Immunol. 2022, 149, 1592–1606.e16. [Google Scholar] [CrossRef] [PubMed]
- Reiff, D.D.; Cron, R.Q. Who Would Have Predicted Multisystem Inflammatory Syndrome in Children? Curr. Rheumatol. Rep. 2022, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Grazioli, S.; Tavaglione, F.; Torriani, G.; Wagner, N.; Rohr, M.; L’huillier, A.G.; Leclercq, C.; Perrin, A.; Bordessoule, A.; Beghetti, M.; et al. Immunological assessment of pediatric multisystem inflammatory syndrome related to coronavirus disease 2019. J. Pediatr. Infect. Dis. Soc. 2021, 10, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rubio, M.; Menéndez-Suso, J.J.; Cámara-Hijón, C.; Río-García, M.; Laplaza-González, M.; Amores-Hernández, I.; Romero-Gómez, M.P.; Álvarez-Rojas, E.; Salas-Mera, D.; López-Granados, E.; et al. Cytokine profile in children with severe multisystem inflammatory syndrome related to the coronavirus disease 2019. J. Pediatr. Intensive Care 2021, 11, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Lapp, S.A.; Abrams, J.; Lu, A.T.; Hussaini, L.; Kao, C.M.; Hunstad, D.A.; Rosenberg, R.B.; Zafferani, M.J.; Ede, K.C.; Ballan, W.; et al. Serologic and cytokine signatures in children with multisystem inflammatory syndrome and coronavirus disease 2019. Open Forum Infect. Dis. 2022, 9, ofac070. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) | ||||||
|---|---|---|---|---|---|---|
| COVID-19 Training (N = 72) | MIS-C Training (N = 66) | p-Value | ||||
| Age at sample collection Med/IQR (yrs) | 14 (6–18) | 9 (6–14) | 0.013 | |||
| BMI Med/IQR | 20.8 (17.6–30.5) | 19.4 (17.1–25.8) | 0.4 | |||
| Gender | 0.03 | |||||
| M/F% | 46/54 | 62/38 | ||||
| Race | 0.95 | |||||
| White% | 65.7 | 63.7 | ||||
| African American% | 28.7 | 28.9 | ||||
| Asian% | 2.8 | 4.3 | ||||
| Other% | 2.8 | 2.9 | ||||
| Ethnicity | 0.65 | |||||
| Hispanic% | 54 | 49 | ||||
| not Hispanic% | 46 | 51 | ||||
| SARS-CoV-2 test | 1.3 × 10−11 | |||||
| PCR% | 90 | 0 | ||||
| Antibody% | 10 | 100 | ||||
| unknown% | 0 | 0 | ||||
| IVIg/steroids 7 dys before collection. % | 33 | 46 | 0.08 | |||
| IVIg/steroid from collection days | −8.5 (−41, −1) | 0 (−2.75, 1) | 4.9 × 10−10 | |||
| LOS in hospital day | 5.5 (2.8, 12.3) | 7.8 (5.3, 11.5) | 0.03 | |||
| ICU LOS days | 0 (0, 4.5) | 3.4 (1.5, 6.7) | 0.002 | |||
| ECMO% | 1.4 | 4.6 | 0.36 | |||
| Ventilator% | 17.1 | 30.8 | 0.035 | |||
| CPAP% | 15.7 | 24.6 | 0.16 | |||
| AKI% | 11.4 | 35.3 | 1.3 × 10−3 | |||
| Labs | ||||||
| Sodium mEq/L | 138 (136, 140) | 134 (131, 137) | 2.5 × 10−7 | |||
| Albumin g/dL | 4 (3.4, 4.6) | 3.3 (3.0, 3.7) | 9.7 × 10−7 | |||
| CO2 mEq/L | 26 (23, 28) | 24 (20, 26) | 3.8 × 10−3 | |||
| BNP pg/mL | 64.1 (18.5, 67.5) | 221.6 (49.8, 589.2) | 1.5 × 10−7 | |||
| TropI ng/mL | 0.02 (0.01, 0.07) | 0.02 (0.01, 0.08) | 0.12 | |||
| Platelets #/nL | 280 (176, 404) | 158 (123, 240) | 7.0 × 10−7 | |||
| Protime seconds | 14.6 (14, 14.9) | 15.4 (14.6, 16.5) | 1.6 × 10−4 | |||
| D-dimer μg/mL | 1.1 (0.5, 2.04) | 3.0 (1.7, 4.06) | 1.4 × 10−7 | |||
| Fibrinogen mg/dL | 402 (317, 459) | 513 (424, 600) | 1.8 × 10−5 | |||
| Procalcitonin ng/mL | 1.6 (0.1, 2.1) | 4.7 (1.6, 12.8) | 4.6 × 10−9 | |||
| CRP mg/dL | 2.1 (0.5, 5.7) | 15.9 (5.2, 24.3) | 5.2 × 10−10 | |||
| NLRatio | 2.5 (1.3, 5.4) | 8.0 (3.1, 14.6) | 3.3 × 10−4 | |||
| Ferritin ng/mL | 254 (97, 377) | 333 (166, 641) | 7.2 × 10−3 | |||
| (b) | ||||||
| COVID-19 Val Set 1 (N = 29) | MIS-C Val Set 1 (N = 43) | COVID-19 Val Set 2 (N = 30) | MIS-C Val Set 2 (N = 32) | COVID-19 Val Set 3 (N = 20) | MIS-C Val Set 3 (N = 46) | |
| Age at sample collect. Med/IQR | 13 (7, 19) | 9 (6.5, 11) | 14 (10, 20) | 11 (7, 14) | 11.5 (10, 15) | 10.5 (7.3, 14) |
| BMI Med/IQR | 21.2 (17.8, 28.7) | 21.2 (16.9, 23.2) | 26.2 (17.9, 32.1) | 19.4 (16.2, 21.2) | 18.9 (16.5, 31.4) | 18.9 (16.4, 21.0) |
| Gender | ||||||
| M/F% | 44/56 | 58/42 | 45/55 | 48/52 | 56/44 | 50/50 |
| Race | ||||||
| White% | 70.4 | 65.1 | 75.9 | 51.7 | 67.0 | 53.0 |
| African American % | 22.2 | 23.3 | 20.7 | 27.6 | 27.0 | 27.0 |
| Asian% | 7.4 | 7.0 | 3.4 | 13.8 | 6.0 | 13.0 |
| Other% | 0 | 4.6 | 0 | 6.9 | 0.0 | 7.0 |
| Ethnicity | ||||||
| Hispanic% | 48 | 56 | 69 | 24.1 | 55.5 | 66.7 |
| not Hispanic% | 52 | 44 | 31 | 75.9 | 44.5 | 33.3 |
| SARS-CoV-2 | ||||||
| PCR% | 100 | 0 | 100 | 0 | 100 | 0 |
| Antibody% | 0 | 100 | 0 | 100 | 0 | 100 |
| unknown% | 0 | 0 | 0 | 0 | 0 | 0 |
| LOS in hospital (days) | 3.8 (1.7, 13.2) | 6.7(5.6, 8.5) | 3.8(1.7, 13.2) | 6.0 (5.6, 8.5) | 0.5(0.0, 8.0) | 5.8 (4.1, 7.7) |
| ICU LOS (days) | 0 (0, 3.3) | 2.9 (0.8, 4.7) | 0 (0, 0) | 2.1 (1.3, 3.1) | 0(0, 0) | 1.9 (0.6, 3.0) |
| ECMO (%) | 3.7 | 4.7 | 3.4 | 0.0 | 0.0 | 0.0 |
| Ventilator (%) | 25.9 | 11.6 | 13.8 | 3.4 | 3.3 | 3.3 |
| CPAP (%) | 22.2 | 39.5 | 17.2 | 20.7 | 10.0 | 19.0 |
| AKI (%) | 11.1 | 30.2 | 17.2 | 24.1 | 10.0 | 22.6 |
| Labs | ||||||
| Sodium Med/IQR mEq/L | 138 (136, 140) | 137 (135, 138) | 137.5 (136, 139) | 134 (132, 137) | 137 (136, 139) | 134 (130.5, 136) |
| Albumin Med/IQR g/dL | 4.2 (3.4, 4.4) | 3.3 (2.8, 3.7) | 3.7 (3.1, 4.1) | 3.5 (3.0, 3.9) | 3.6 (3.1, 3.8) | 3.3 (3.0, 3.8) |
| CO2 Med/IQR mEq/L | 26 (24, 28) | 24 (23, 26) | 25.5 (23, 29) | 25 (21.5, 26) | 26 (23, 28) | 24 (20.5, 25) |
| BNP Med/IQR pg/mL | 105.2 (34.2, 169) | 259.8 (124, 632) | 201 (110, 228) | 142.5 (55.3, 636) | 169 (100, 231) | 143 (65.3, 706) |
| Trop I Med/IQR ng/mL | 0.02 (0.00, 0.03) | 0.02 (0.01, 0.07) | 0.01 (0.01, 0.01) | 0.02 (0.01, 0.08) | 0.01 (0.01, 0.01) | 0.02 (0.01, 0.08) |
| Platelets Med/IQR #/nL | 264 (194.5, 356) | 177 (106, 265) | 233.5 (199, 275) | 199 (144, 267.5) | 230 (198, 279) | 199 (145, 270) |
| Protime Med/IQR sec | 15 (14.4, 15.2) | 15.1 (14.4, 15.6) | 14.2 (13.6, 14.4) | 14.9 (14.5, 15.6) | 14.4 (13.8, 14.5) | 14.9 (14.4, 15.5) |
| D-Dimer Med/IQR μg/mL | 2.4 (1.3, 2.9) | 2.9 (1.9, 3.8) | 1.6 (0.7, 3.8) | 2.8 (1.6, 3.8) | 2.8 (0.7, 4.2) | 2.7 (1.5, 3.6) |
| Fibrinogen Med/IQR mg/dL | 448 (430, 457) | 459 (359, 634) | 416 (350, 532) | 539 (393, 614) | 455 (377, 494) | 527 (393, 597) |
| Procalcitonin Med/IQR ng/mL | 1.5 (1.2, 1.6) | 4.6 (2.2, 14.2) | 0.4 (0.1, 0.5) | 2.2 (1.0, 4.8) | 0.4 (0.2, 0.5) | 1.8 (1.0, 4.8) |
| CRP Med/IQR mg/dL | 3.8 (0.5, 5.5) | 19.3 (5.1, 22.8) | 13 (4.0, 13.5) | 7.9 (4.3, 22.3) | 13.9 (4.3, 14.5) | 7.9 (4.8, 20.7) |
| NLRatio Med/IQR | 2.3 (1.0, 3.7) | 4.7 (2.9, 9.0) | 3.7 (2.1, 5.2) | 5.7 (2.7, 12.2) | 3.5 (2.0, 4.6) | 5.7 (2.3, 9.7) |
| Ferritin Med/IQR ng/mL | 239 (100, 253) | 282 (182, 472) | 211 (38.8, 400) | 334 (223.5, 597.5) | 277 (44, 592) | 302 (224, 532) |
| (c) | ||||||
| Cytokine (Pg/mL) | COVID-19 | MIS-C | p-Value | Specificity | Sensitivity | |
| sIL2R | 491.8 (388.1, 782.2) | 3576.6 (2270.0, 5475.0) | 1.97 × 1019 | 0.95 ± 0.07 | 0.8 ± 0.08 | |
| IP-10 | 175.9 (91.4, 494.0) | 9000.0 (1991.0, 15, 803.2) | 2.57 × 1017 | 0.93 ± 0.05 | 0.7 ± 0.08 | |
| MIG | 1395.0 (941.6, 2938.5) | 27764.5 (12, 618.8, 43, 215.0) | 2.71 × 1016 | 0.35 ± 0.43 | 0.94 ± 0.08 | |
| IL-10 | 25.6 (16.2, 59.2) | 191.6 (85.3, 368.5) | 6.77 × 1016 | 0.87 ± 0.08 | 0.7 ± 0.15 | |
| IL-15 | 15.7 (6.1, 23.8) | 39.2 (30.5, 54.2) | 4.55 × 1015 | 0.79 ± 0.19 | 0.79 ± 0.06 | |
| IL-3 | 1.2 (0.7, 1.9) | 3.3 (2.3, 4.8) | 4.19 × 1014 | 0.85 ± 0.1 | 0.76 ± 0.17 | |
| IL-1RA | 38.7 (21.6, 143.3) | 681.2 (155.9, 7816.2) | 8.13 × 1013 | 0.9 ± 0.13 | 0.54 ± 0.13 | |
| TNFalpha | 57.1 (44.3, 85.7) | 132.3 (88.7, 225.6) | 1.84 × 1011 | 0.8 ± 0.2 | 0.59 ± 0.21 | |
| IL-13 | 42.9 (37.4, 57.5) | 63.7 (56.5, 74.3) | 8.45 × 101 | 0.77 ± 0.14 | 0.64 ± 0.14 | |
| IFNgamma | 7.0 (5.7, 10.8) | 17.2 (9.8, 32.0) | 4.47 × 109 | 0.84 ± 0.21 | 0.37 ± 0.21 | |
| IL-22 | 80.1 (68.2, 105.2) | 109.8 (94.5, 125.2) | 5.15 × 108 | 0.73 ± 0.18 | 0.6 ± 0.26 | |
| IL-2 | 3.7 (3.1, 4.7) | 5.0 (4.3, 5.9) | 1.50 × 107 | 0.78 ± 0.15 | 0.56 ± 0.22 | |
| TGF-a | 11.5 (8.0, 15.8) | 18.4 (14.0, 25.1) | 5.75 × 107 | 0.82 ± 0.08 | 0.46 ± 0.1 | |
| G-CSF | 66.1 (46.2, 116.1) | 155.7 (78.8, 339.3) | 6.64 × 107 | 0.92 ± 0.05 | 0.31 ± 0.12 | |
| IL-6 | 9.4 (4.5, 27.3) | 48.4 (12.7, 188.8) | 1.12 × 106 | 0.89 ± 0.07 | 0.41 ± 0.12 | |
| IL-27 | 2216.5 (1368.8, 3763.5) | 4241.5 (3043.2, 8846.8) | 3.05 × 106 | 0.0 ± 0.0 | 1.0 ± 0.0 | |
| MCP-3 | 48.4 (41.0, 57.6) | 62.3 (49.2, 88.6) | 4.14 × 106 | 0.83 ± 0.21 | 0.49 ± 0.22 | |
| IL-4 | 3.3 (2.1, 4.6) | 5.1 (3.5, 7.2) | 8.27 × 106 | 0.85 ± 0.16 | 0.31 ± 0.17 | |
| IL-1alpha | 27.2 (22.8, 39.3) | 39.0 (31.8, 50.8) | 1.77 × 105 | 0.79 ± 0.18 | 0.31 ± 0.1 | |
| TNFbeta | 15.0 (12.4, 18.5) | 18.8 (16.0, 22.3) | 1.93 × 105 | 0.75 ± 0.13 | 0.34 ± 0.17 | |
| IL-18 | 88.6 (54.2, 174.6) | 180.5 (128.8, 380.0) | 3.38 × 105 | 0.8 ± 0.12 | 0.37 ± 0.08 | |
| IL-12(p70) | 8.8 (7.5, 11.9) | 10.6 (9.4, 14.3) | 4.03 × 105 | 0.75 ± 0.14 | 0.39 ± 0.17 | |
| MIP-1alpha | 46.7 (40.3, 63.1) | 54.9 (48.7, 67.2) | 4.87 × 105 | 0.78 ± 0.25 | 0.1 ± 0.11 | |
| M-CSF | 709.8 (461.7, 1071.8) | 1073.0 (740.7, 1547.2) | 5.04 × 105 | 0.75 ± 0.16 | 0.5 ± 0.15 | |
| MCP-1 | 350.7 (210.6, 689.1) | 715.4 (316.7, 1423.0) | 1.12 × 104 | 0.8 ± 0.21 | 0.49 ± 0.15 | |
| Fractalkine | 191.1 (169.0, 240.4) | 244.8 (191.2, 286.6) | 1.16 × 104 | 0.76 ± 0.17 | 0.49 ± 0.14 | |
| IL-1beta | 20.8 (16.0, 28.3) | 26.1 (21.8, 35.1) | 2.16 × 104 | 0.78 ± 0.12 | 0.34 ± 0.12 | |
| IL-5 | 9.2 (6.4, 17.8) | 16.8 (9.1, 30.8) | 5.81 × 104 | 0.84 ± 0.17 | 0.17 ± 0.21 | |
| PDGF-AB/BB | 28685.5 (18, 716.2, 41, 657.2) | 21208.0 (11, 836.0, 28, 590.2) | 6.20 × 104 | 1.0 ± 0.0 | 0.0 ± 0.0 | |
| MIP-1beta | 25.7 (20.2, 40.7) | 37.1 (25.8, 48.3) | 7.40 × 104 | 0.75 ± 0.2 | 0.34 ± 0.15 | |
| MDC | 541.0 (294.7, 835.9) | 345.9 (190.7, 583.0) | 1.56 × 103 | 0.54 ± 0.1 | 0.7 ± 0.17 | |
| IFNalpha2 | 84.0 (73.1, 104.2) | 91.0 (83.9, 119.8) | 9.47 × 103 | 0.79 ± 0.16 | 0.3 ± 0.14 | |
| IL-17F | 35.6 (24.2, 76.7) | 46.5 (36.6, 96.2) | 1.01 × 102 | 0.81 ± 0.18 | 0.14 ± 0.19 | |
| IL-7 | 6.3 (3.7, 8.9) | 7.6 (5.3, 10.6) | 2.72 × 102 | 0.55 ± 0.28 | 0.37 ± 0.25 | |
| FGF-2 | 144.3 (122.7, 192.0) | 164.7 (131.7, 183.2) | 7.23 × 102 | 0.66 ± 0.23 | 0.21 ± 0.2 | |
| sCD40L | 2781.5 (928.0, 4929.8) | 1651.0 (923.7, 3796.0) | 7.34 × 102 | 0.68 ± 0.28 | 0.4 ± 0.33 | |
| IL-8 | 23.5 (11.4, 50.8) | 26.8 (18.6, 45.0) | 8.08 × 102 | 0.33 ± 0.13 | 0.59 ± 0.15 | |
| VEGF | 142.7 (74.0, 224.3) | 153.9 (114.5, 276.9) | 8.81 × 102 | 0.78 ± 0.19 | 0.17 ± 0.12 | |
| IL-17A | 17.9 (11.9, 23.0) | 17.4 (14.9, 25.6) | 1.03 × 101 | 0.68 ± 0.34 | 0.21 ± 0.26 | |
| IL-9 | 32.6 (26.0, 43.9) | 36.8 (26.4, 50.4) | 1.65 × 101 | 0.69 ± 0.18 | 0.4 ± 0.1 | |
| FLT-3L | 40.5 (24.7, 63.9) | 42.7 (32.5, 62.6) | 1.80 × 101 | 0.54 ± 0.29 | 0.37 ± 0.25 | |
| IL-12(p40) | 110.7 (72.0, 158.8) | 107.3 (89.1, 162.6) | 2.88 × 101 | 0.39 ± 0.11 | 0.63 ± 0.11 | |
| IL-17E/IL-25 | 1908.5 (1601.5, 2447.0) | 1974.5 (1560.8, 2507.0) | 3.75 × 101 | 0.96 ± 0.09 | 0.04 ± 0.09 | |
| GROa | 55.4 (41.3, 76.3) | 58.7 (38.6, 87.2) | 3.98 × 101 | 0.68 ± 0.17 | 0.21 ± 0.13 | |
| PDGF-AA | 3404.5 (1553.2, 4519.0) | 2811.0 (1384.8, 4426.8) | 4.81 × 101 | 0.56 ± 0.46 | 0.46 ± 0.46 | |
| AUC | F1 | AUPRC | Accuracy | |
|---|---|---|---|---|
| Training set (72 C, 66 M) | 0.95 ± 0.02 | 0.91 ± 0.04 | 0.97 ± 0.01 | 0.92 ± 0.04 |
| Val set 1 (29 C, 43 M) | 0.98 | 0.93 | 0.99 | 6 errors (0 C, 6 M) |
| Val set 2 (30 C, 32 M) | 0.89 | 0.88 | 0.91 | 8 errors (5 C, 3 M) |
| Val set 3 (20 C, 46 M) | 0.99 | 0.97 | 0.99 | 3 errors (1 C, 2M) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Subramanian, D.; Vittala, A.; Chen, X.; Julien, C.; Acosta, S.; Rusin, C.; Allen, C.; Rider, N.; Starosolski, Z.; Annapragada, A.; et al. Stratification of Pediatric COVID-19 Cases Using Inflammatory Biomarker Profiling and Machine Learning. J. Clin. Med. 2023, 12, 5435. https://doi.org/10.3390/jcm12175435
Subramanian D, Vittala A, Chen X, Julien C, Acosta S, Rusin C, Allen C, Rider N, Starosolski Z, Annapragada A, et al. Stratification of Pediatric COVID-19 Cases Using Inflammatory Biomarker Profiling and Machine Learning. Journal of Clinical Medicine. 2023; 12(17):5435. https://doi.org/10.3390/jcm12175435
Chicago/Turabian StyleSubramanian, Devika, Aadith Vittala, Xinpu Chen, Christopher Julien, Sebastian Acosta, Craig Rusin, Carl Allen, Nicholas Rider, Zbigniew Starosolski, Ananth Annapragada, and et al. 2023. "Stratification of Pediatric COVID-19 Cases Using Inflammatory Biomarker Profiling and Machine Learning" Journal of Clinical Medicine 12, no. 17: 5435. https://doi.org/10.3390/jcm12175435
APA StyleSubramanian, D., Vittala, A., Chen, X., Julien, C., Acosta, S., Rusin, C., Allen, C., Rider, N., Starosolski, Z., Annapragada, A., & Devaraj, S. (2023). Stratification of Pediatric COVID-19 Cases Using Inflammatory Biomarker Profiling and Machine Learning. Journal of Clinical Medicine, 12(17), 5435. https://doi.org/10.3390/jcm12175435