
Descemet’s Membrane Detachment during Phacocanaloplasty: Case Series and In-Depth Literature Review
 , ,
, ,
Abstract
:1. Introduction
2. Case Series
2.1. Surgical Method
2.2. Case 1
2.3. Case 2
2.4. Case 3
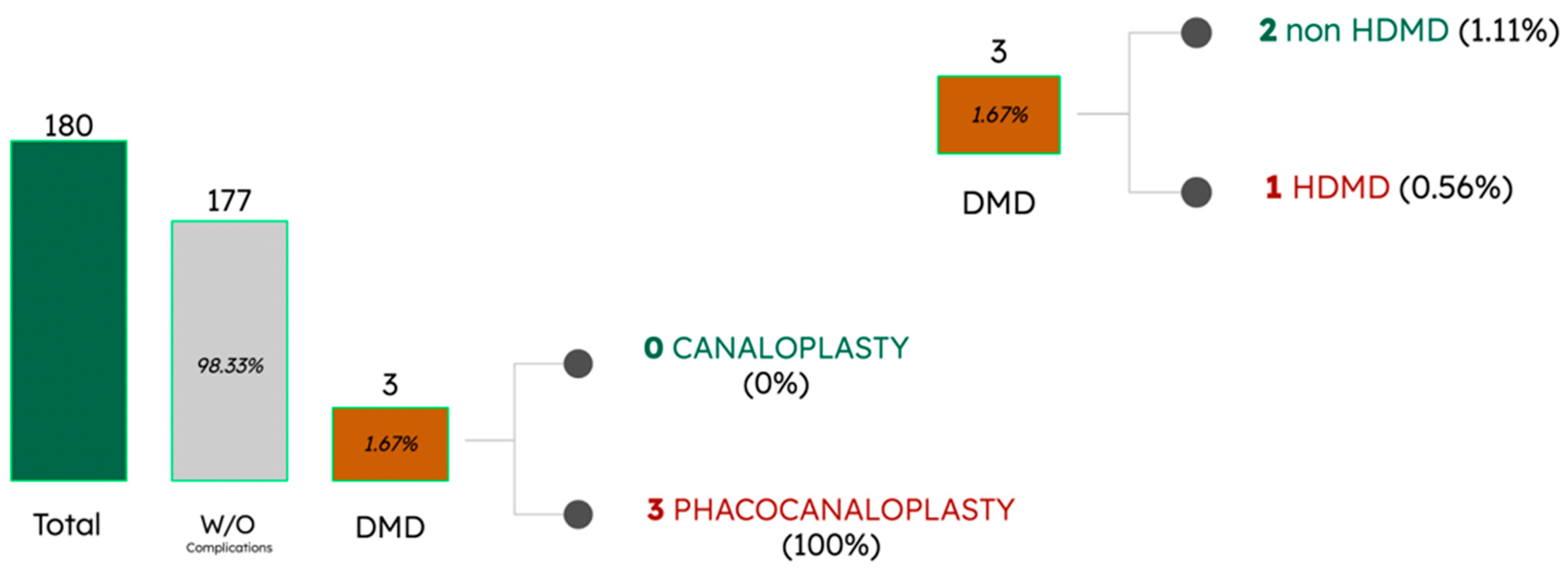
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robert, M.-C.; Harasymowycz, P. Hemorrhagic Descemet Detachment After Combined Canaloplasty and Cataract Surgery. Cornea 2013, 32, 712–713. [Google Scholar] [CrossRef] [PubMed]
- Beres, H.; Scharioth, G.B. Canaloplasty in the spotlight: Surgical alternatives and future perspectives. Rom. J. Ophthalmol. 2022, 66, 225–232. [Google Scholar] [CrossRef]
- Zhang, B.; Kang, J.; Chen, X. A System Review and Meta-Analysis of Canaloplasty Outcomes in Glaucoma Treatment in Comparison with Trabeculectomy. J. Ophthalmol. 2017, 2017, 2723761. [Google Scholar] [CrossRef] [PubMed]
- Konopińska, J.; Mariak, Z.; Rękas, M. Improvement of the safety profile of canaloplasty and phacocanaloplasty: A review of complications and their management. J. Ophthalmol. 2020, 2020, 8352827. [Google Scholar] [CrossRef] [PubMed]
- Alobeidan, S.A.; Almobarak, F.A. Incidence and management of haemorrhagic Descemet membrane detachment in canaloplasty and phacocanaloplasty. Acta Ophthalmol. 2015, 94, e298–e304. [Google Scholar] [CrossRef] [PubMed]
- Grieshaber, M.C. Viscocanalostomy and Canaloplasty: Ab Externo Schlemm’s Canal Surgery. Dev. Ophthalmol. 2017, 59, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Byszewska, A.; Konopińska, J.; Kicińska, A.K.; Mariak, Z.; Rękas, M. Canaloplasty in the Treatment of Primary Open-Angle Glaucoma: Patient Selection and Perspectives. Clin. Ophthalmol. 2019, 13, 2617–2629. [Google Scholar] [CrossRef]
- Khaimi, M.A. Canaloplasty: A minimally invasive and maximally effective glaucoma treatment. J. Ophthalmol. 2015, 2015, 485065. [Google Scholar] [CrossRef]
- Vold, S.D.; Williamson, B.K.; Hirsch, L.; Aminlari, A.E.; Cho, A.S.; Nelson, C.; Dickerson, J.E., Jr. Canaloplasty and trabeculotomy with the OMNI system in pseudophakic patients with open-angle glaucoma: The ROMEO study. Ophthalmol. Glaucoma 2021, 4, 173–181. [Google Scholar] [CrossRef]
- Schoenberg, E.D.; Chaudhry, A.L.; Chod, R.; Zurakowski, D.; Ayyala, R.S. Comparison of surgical outcomes between phacocanaloplasty and phacotrabeculectomy at 12 months’ follow-up: A longitudinal cohort study. J. Glaucoma 2015, 24, 543–549. [Google Scholar] [CrossRef]
- Brüggemann, A.; Despouy, J.T.; Wegent, A.; Müller, M. Intraindividual comparison of Canaloplasty versus trabeculectomy with mitomycin C in a single-surgeon series. J. Glaucoma 2013, 22, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.A.; von Wolff, K.; Tetz, M.; Korber, N.; Kearney, J.R.; Shingleton, B.; Samuelson, T.W. Canaloplasty: Circumferential viscodilation and tensioning of Schlemm’s canal using a flexible microcatheter for the treatment of open-angle glaucoma in adults. J. Cataract. Refract. Surg. 2007, 33, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Koch, J.M.; Heiligenhaus, A.; Heinz, C. Canaloplasty and transient anterior chamber haemorrhage: A prognostic factor? Klin. Monbl. Augenheilkd. 2011, 228, 465–467. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Cardoso, I.; Esteves, F.; Amorim, M.; Calvão-Santos, G.; Freitas, M.L.; Salgado-Borges, J. Viscocanalostomía circunferencial con sutura de tensión en el canal de Schlemm (canaloplastia): Un año de experiencia. Arch. Soc. Esp. Oftalmol. 2013, 88, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Singhal, D.; Sahay, P.; Goel, S.; Asif, M.I.; Maharana, P.K.; Sharma, N. Descemet membrane detachment. Surv. Ophthalmol. 2020, 65, 279–293. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo, A.; Foreman, J.; Ayyala, R.S. Descemet membrane detachment after canaloplasty: Incidence and management. J. Glaucoma 2014, 23, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Ayyala, R.S.; Chaudhry, A.L.; Okogbaa, C.B.; Zurakowski, D. Comparison of surgical outcomes between canaloplasty and trabeculectomy at 12 months’ follow-up. Ophthalmology 2011, 118, 2427–2433. [Google Scholar] [CrossRef] [PubMed]
- Bull, H.; von Wolff, K.; Körber, N.; Tetz, M. Three-year canaloplasty outcomes for the treatment of open-angle glaucoma: European study results. Graefe s Archive for Clinical and Experimental. Ophthalmology 2011, 249, 1537–1545. [Google Scholar] [CrossRef]
- Brusini, P. Canaloplasty in Open-Angle Glaucoma Surgery: A Four-Year Follow-Up. Sci. World J. 2014, 2014, 469609. [Google Scholar] [CrossRef]
- Djavanmardi, S.; Arciniegas-Perasso, C.A.; Duch, S.; Avila-Marrón, E.; Milla, E. Hemorrhagic Descemet’s membrane detachment in nonpenetrating glaucoma surgery: A rare and relevant complication. J. Glaucoma 2021, 30, 352–356. [Google Scholar] [CrossRef]
- Palmiero, P.-M.; Aktas, Z.; Lee, O.; Tello, C.; Sbeity, Z. Bilateral Descemet membrane detachment after canaloplasty. J. Cataract Refract. Surg. 2010, 36, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Bentley, M.D.; Hann, C.R.; Fautsch, M.P. Anatomical variation of human collector channel orifices. Investig. Ophthalmol. Vis. Sci. 2016, 57, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Irshad, F.A.; Mayfield, M.S.; Zurakowski, D.; Ayyala, R.S. Variation in schlemm’s canal diameter and location by ultrasound biomicroscopy. Ophthalmology 2010, 117, 916–920. [Google Scholar] [CrossRef] [PubMed]
- Rasouli, M.; Mather, R.; Tingey, D. Descemet membrane detachment following viscoelastic injection for posttrabeculectomy hypotony. J. Cataract Refract. Surg. 2008, 43, 254–255. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.A.; Agarwal, A.; Sivanganam, S.; Chandrasekar, R. Height-, extent-, length-, and pupil-based (HELP) algorithm to manage post-phacoemulsification Descemet membrane detachment. J. Cataract Refract. Surg. 2015, 41, 1945–1953. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Kim, M.J.; Tchah, H.; Kim, J.Y. Descemet membranotomy with an Nd:YAG laser can be used to treat pre-Descemet hemorrhage. Cornea 2012, 31, 206–208. [Google Scholar] [CrossRef] [PubMed]
- Weng, Y.; Ren, Y.-P.; Zhang, L.; Huang, X.-D.; Shen-Tu, X.-C. An alternative technique for Descemet’s membrane detachment following phacoemulsification: Case report and review of literature. BMC Ophthalmol. 2017, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- Hamid, M.; Thompson, P.; Harasymowycz, P. Novel treatment for hemorrhagic Descemet detachment after canaloplasty. Cornea 2015, 34, 1611–1612. [Google Scholar] [CrossRef]
- Desprendimiento de Membrana de Descemet Postquirúrgico, una Complicación Inusual, Pero Importante. FacoElche. 2019. Available online: Facoelche.com (accessed on 18 April 2023).
- Jain, R.; Murthy, S.I.; Basu, S.; Ali, M.H.; Sangwan, V.S. Anatomic and visual outcomes of descemetopexy in post-cataract surgery descemet’s membrane detachment. Ophthalmology 2013, 120, 1366–1372. [Google Scholar] [CrossRef]
- Fan, N.-W. Outcomes of repeat descemetopexy in post-cataract surgery descemet membrane detachment. Am. J. Ophthalmol. 2014, 157, 1330–1331. [Google Scholar] [CrossRef]
- Chow, V.W.S.; Agarwal, T.; Vajpayee, R.B.; Jhanji, V. Update on diagnosis and management of Descemetʼs membrane detachment. Curr. Opin. Ophthalmol. 2013, 24, 356–361. [Google Scholar] [CrossRef]
- Freiberg, F.J.; Salgado, J.P.; Grehn, F.; Klink, T. Intracorneal hematoma after canaloplasty and clear cornea phacoemulsification: Surgical management. Eur. J. Ophthalmol. 2012, 22, 823–825. [Google Scholar] [CrossRef]
- Gallego-Pinazo, R.; López-Sánchez, E.; Marín-Montiel, J. Hemorrhagic Descemet’s membrane detachment after viscocanalostomy. Arch. Soc. Esp. Oftalmol. 2010, 85, 110–113. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Baseline BCVA | Surgery | Type of Dmd | Location of DMD | BCVA after DMD | Intervention | BCVA after 3 Months | Cornea Status |
|---|---|---|---|---|---|---|---|---|
| 1 | 0.3 | Phacocanaloplasty | Non-HDMD | Infero-nasal and infero-temporal | 0.5 | Postoperative drainage | 0.9 | Clear |
| 2 | 0.4 | Phacocanaloplasty | HDMD | Infero-temporal | 0.7 | Observation | 1 | Remnants of HDMD |
| 3 | 0.6 | Phacocanaloplasty | Non-HDMD | Infero-temporal | 0.6 | Intraoperative surgical drainage and air injection | 0.9 | Disruption of DM with no edema |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orejudo de Rivas, M.; Martínez Morales, J.; Pardina Claver, E.; Pérez García, D.; Pérez Navarro, I.; Ascaso Puyuelo, F.J.; Aramburu Clavería, J.; Ibáñez Alperte, J. Descemet’s Membrane Detachment during Phacocanaloplasty: Case Series and In-Depth Literature Review. J. Clin. Med. 2023, 12, 5461. https://doi.org/10.3390/jcm12175461
Orejudo de Rivas M, Martínez Morales J, Pardina Claver E, Pérez García D, Pérez Navarro I, Ascaso Puyuelo FJ, Aramburu Clavería J, Ibáñez Alperte J. Descemet’s Membrane Detachment during Phacocanaloplasty: Case Series and In-Depth Literature Review. Journal of Clinical Medicine. 2023; 12(17):5461. https://doi.org/10.3390/jcm12175461
Chicago/Turabian StyleOrejudo de Rivas, Marta, Juana Martínez Morales, Elena Pardina Claver, Diana Pérez García, Itziar Pérez Navarro, Francisco J. Ascaso Puyuelo, Julia Aramburu Clavería, and Juan Ibáñez Alperte. 2023. "Descemet’s Membrane Detachment during Phacocanaloplasty: Case Series and In-Depth Literature Review" Journal of Clinical Medicine 12, no. 17: 5461. https://doi.org/10.3390/jcm12175461
APA StyleOrejudo de Rivas, M., Martínez Morales, J., Pardina Claver, E., Pérez García, D., Pérez Navarro, I., Ascaso Puyuelo, F. J., Aramburu Clavería, J., & Ibáñez Alperte, J. (2023). Descemet’s Membrane Detachment during Phacocanaloplasty: Case Series and In-Depth Literature Review. Journal of Clinical Medicine, 12(17), 5461. https://doi.org/10.3390/jcm12175461