


Protocol Study for the Evaluation of Non-Opioid Balanced General Anaesthesia in Cardiac Surgery with Cardiopulmonary Bypass: A Randomised, Controlled, Multicentric Superiority Trial (OFACAR Study)
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Material and Methods
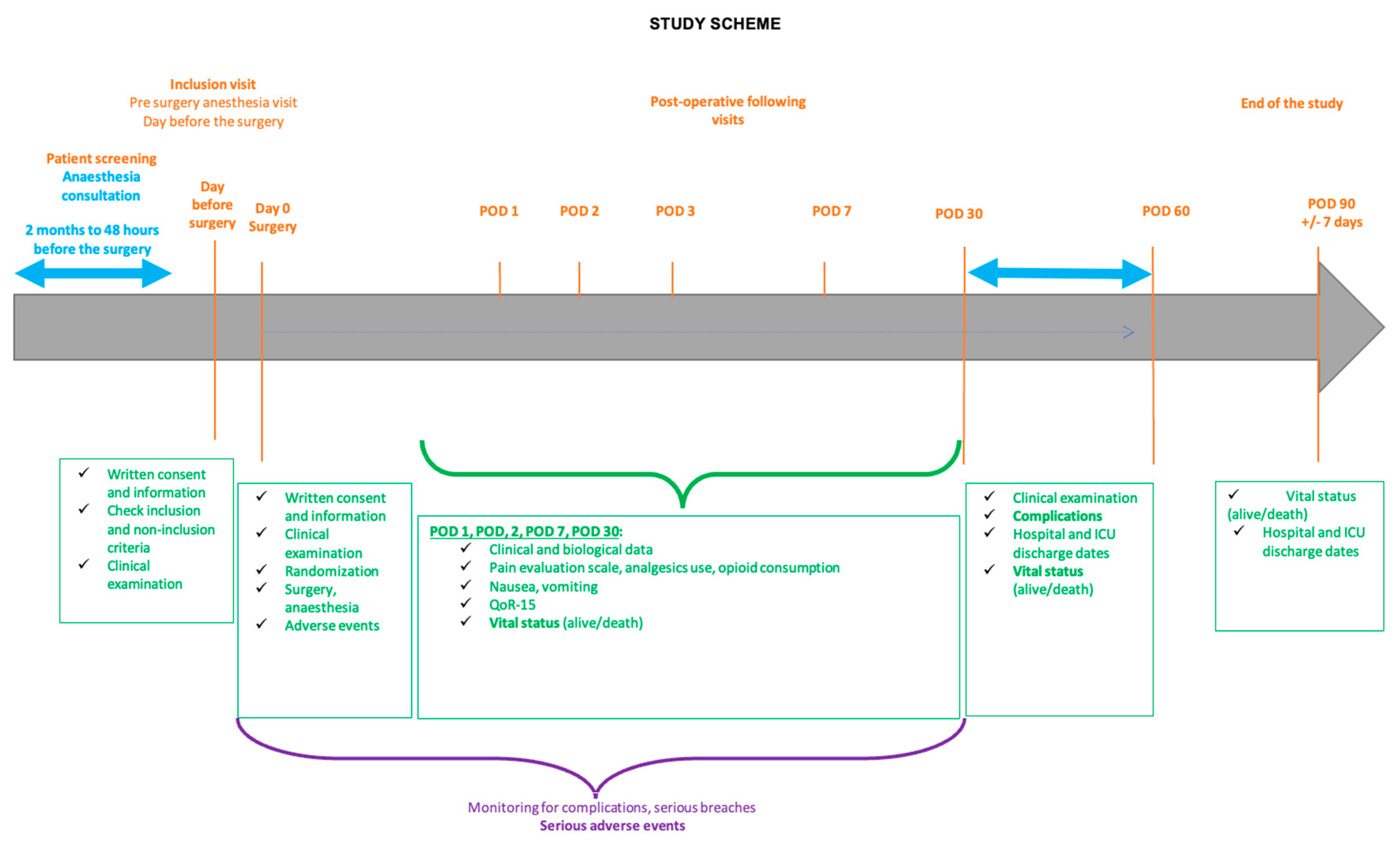
2.1. Study Design
2.2. Ethics Statement
2.3. Study Population
2.4. Randomisation
2.5. Study Intervention
2.5.1. OFA Group
2.5.2. Control Group
2.5.3. ICU Management
2.6. Data Collection
2.7. Objectives
2.8. Outcomes
2.9. Statistics
2.9.1. Sample Size Calculation
2.9.2. Data Analysis
2.9.3. Ancillary Study
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, E.N.; Pavone, K.J.; Naranjo, M. Multimodal General Anesthesia: Theory and Practice. Anesth. Analg. 2018, 127, 1246–1258. [Google Scholar] [CrossRef]
- Colvin, L.A.; Bull, F.; Hales, T.G. Perioperative Opioid Analgesia-When Is Enough Too Much? A Review of Opioid-Induced Tolerance and Hyperalgesia. Lancet 2019, 393, 1558–1568. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P.; Estebe, J.-P. Opioid-Free Anesthesia: A Different Regard to Anesthesia Practice. Curr. Opin. Anaesthesiol. 2018, 31, 556–561. [Google Scholar] [CrossRef]
- Bakan, M.; Umutoglu, T.; Topuz, U.; Uysal, H.; Bayram, M.; Kadioglu, H.; Salihoglu, Z. Opioid-Free Total Intravenous Anesthesia with Propofol, Dexmedetomidine and Lidocaine Infusions for Laparoscopic Cholecystectomy: A Prospective, Randomized, Double-Blinded Study. Braz. J. Anesthesiol. 2015, 65, 191–199. [Google Scholar] [CrossRef]
- An, G.; Zhang, Y.; Chen, N.; Fu, J.; Zhao, B.; Zhao, X. Opioid-Free Anesthesia Compared to Opioid Anesthesia for Lung Cancer Patients Undergoing Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Study. PLoS ONE 2021, 16, e0257279. [Google Scholar] [CrossRef]
- Guinot, P.-G.; Spitz, A.; Berthoud, V.; Ellouze, O.; Missaoui, A.; Constandache, T.; Grosjean, S.; Radhouani, M.; Anciaux, J.-B.; Parthiot, J.-P.; et al. Effect of Opioid-Free Anaesthesia on Post-Operative Period in Cardiac Surgery: A Retrospective Matched Case-Control Study. BMC Anesthesiol. 2019, 19, 136. [Google Scholar] [CrossRef]
- Guinot, P.-G.; Andrei, S.; Durand, B.; Martin, A.; Duclos, V.; Spitz, A.; Berthoud, V.; Constandache, T.; Grosjean, S.; Radhouani, M.; et al. Balanced Nonopioid General Anesthesia with Lidocaine Is Associated with Lower Postoperative Complications Compared with Balanced Opioid General Anesthesia with Sufentanil for Cardiac Surgery with Cardiopulmonary Bypass: A Propensity Matched Cohort Study. Anesth. Analg. 2023, 136, 965–974. [Google Scholar] [CrossRef]
- Guinot, P.-G.; Durand, B.; Besnier, E.; Michel, M.P.; Bernard, C.; Nguyen, M.; Berthoud, V.; Abou-Arab, O.; Bouhemad, B. Epidemiology, Risk Factors and Outcomes of Norepinephrine Use in Cardiac Surgery with Cardiopulmonary Bypass: A Multicentric Prospective Study. Anaesth. Crit. Care Pain Med. 2023, 42, 101200. [Google Scholar] [CrossRef]
- Sousa-Uva, M.; Head, S.J.; Milojevic, M.; Collet, J.-P.; Landoni, G.; Castella, M.; Dunning, J.; Gudbjartsson, T.; Linker, N.J.; Sandoval, E.; et al. 2017 EACTS Guidelines on Perioperative Medication in Adult Cardiac Surgery. Eur. J. Cardiothorac. Surg. 2018, 53, 5–33. [Google Scholar] [CrossRef] [PubMed]
- Mertes, P.-M.; Kindo, M.; Amour, J.; Baufreton, C.; Camilleri, L.; Caus, T.; Chatel, D.; Cholley, B.; Curtil, A.; Grimaud, J.-P.; et al. Guidelines on Enhanced Recovery after Cardiac Surgery under Cardiopulmonary Bypass or Off-Pump. Anaesth. Crit. Care Pain. Med. 2022, 41, 101059. [Google Scholar] [CrossRef] [PubMed]
- Task Force Members; Kunst, G.; Milojevic, M.; Boer, C.; De Somer, F.M.J.J.; Gudbjartsson, T.; van den Goor, J.; Jones, T.J.; Lomivorotov, V.; Merkle, F.; et al. 2019 EACTS/EACTA/EBCP Guidelines on Cardiopulmonary Bypass in Adult Cardiac Surgery. Br. J. Anaesth. 2019, 123, 713–757. [Google Scholar] [CrossRef] [PubMed]
- Joannes-Boyau, O.; Le Conte, P.; Bonnet, M.-P.; Cesareo, E.; Chousterman, B.; Chaiba, D.; Douay, B.; Futier, E.; Harrois, A.; Huraux, C.; et al. Guidelines for the Choice of Intravenous Fluids for Vascular Filling in Critically Ill Patients, 2021. Anaesth. Crit. Care Pain Med. 2022, 41, 101058. [Google Scholar] [CrossRef] [PubMed]
- Vallet, B.; Blanloeil, Y.; Cholley, B.; Orliaguet, G.; Pierre, S.; Tavernier, B. Société française d’anesthésie et de réanimation Guidelines for Perioperative Haemodynamic Optimization. Ann. Fr. D’anesth. Reanim. 2013, 32, e151–e158. [Google Scholar] [CrossRef]
- Abou-Arab, O.; Huette, P.; Martineau, L.; Beauvalot, C.; Beyls, C.; Josse, E.; Touati, G.; Bouchot, O.; Bouhemad, B.; Diouf, M.; et al. Hyperoxia during Cardiopulmonary Bypass Does Not Decrease Cardiovascular Complications Following Cardiac Surgery: The CARDIOX Randomized Clinical Trial. Intensive Care Med. 2019, 45, 1413–1421. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S.; et al. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar] [CrossRef]
- Jammer, I.; Wickboldt, N.; Sander, M.; Smith, A.; Schultz, M.J.; Pelosi, P.; Leva, B.; Rhodes, A.; Hoeft, A.; Walder, B.; et al. Standards for Definitions and Use of Outcome Measures for Clinical Effectiveness Research in Perioperative Medicine: European Perioperative Clinical Outcome (EPCO) Definitions: A Statement from the ESA-ESICM Joint Taskforce on Perioperative Outcome Measures. Eur. J. Anaesthesiol. 2015, 32, 88–105. [Google Scholar] [CrossRef]
- Ely, E.W.; Inouye, S.K.; Bernard, G.R.; Gordon, S.; Francis, J.; May, L.; Truman, B.; Speroff, T.; Gautam, S.; Margolin, R.; et al. Delirium in Mechanically Ventilated Patients: Validity and Reliability of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). JAMA 2001, 286, 2703–2710. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Aronsohn, J.; Orner, G.; Palleschi, G.; Gerasimov, M. Opioid-Free Total Intravenous Anesthesia with Ketamine as Part of an Enhanced Recovery Protocol for Bariatric Surgery Patients with Sleep Disordered Breathing. J. Clin. Anesth. 2019, 52, 65–66. [Google Scholar] [CrossRef]
- Forget, P.; Cata, J. Stable Anesthesia with Alternative to Opioids: Are Ketamine and Magnesium Helpful in Stabilizing Hemodynamics during Surgery? A Systematic Review and Meta-Analyses of Randomized Controlled Trials. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 523–531. [Google Scholar] [CrossRef]
- Aboab, J.; Mayaud, L.; Sebille, V.; de Oliveira, R.; Jourdain, M.; Annane, D. Esmolol Indirectly Stimulates Vagal Nerve Activity in Endotoxemic Pigs. Intensive Care Med. Exp. 2018, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Boswell, M.R.; Moman, R.N.; Burtoft, M.; Gerdes, H.; Martinez, J.; Gerberi, D.J.; Wittwer, E.; Murad, M.H.; Hooten, W.M. Lidocaine for Postoperative Pain after Cardiac Surgery: A Systematic Review. J. Cardiothorac. Surg. 2021, 16, 157. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Niu, J.; Li, Z.; Lv, H.; Cai, H. The Efficacy and Safety of Dexmedetomidine in Cardiac Surgery Patients: A Systematic Review and Meta-Analysis. PLoS ONE 2018, 13, e0202620. [Google Scholar] [CrossRef]
- Williams, J.B.; McConnell, G.; Allender, J.E.; Woltz, P.; Kane, K.; Smith, P.K.; Engelman, D.T.; Bradford, W.T. One-Year Results from the First US-Based Enhanced Recovery after Cardiac Surgery (ERAS Cardiac) Program. J. Thorac. Cardiovasc. Surg. 2019, 157, 1881–1888. [Google Scholar] [CrossRef]
- Hemmings, H.C.; Lambert, D.G. The Good, the Bad, and the Ugly: The Many Faces of Opioids. Br. J. Anaesth. 2019, 122, 705–707. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Inclusion criteria |
| |
| Non-inclusion criteria |
|
|
| Postoperative neurological dysfunction |
|
| Acute renal failure |
|
| Acute respiratory failure |
|
| Cardiovascular complications |
|
| Death at D30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guinot, P.-G.; Besch, G.; Hameury, B.; Grelet, T.; Mertes, P.M.; Nguyen, M.; Bouhemad, B.; on behalf of the OFACAR Study Group. Protocol Study for the Evaluation of Non-Opioid Balanced General Anaesthesia in Cardiac Surgery with Cardiopulmonary Bypass: A Randomised, Controlled, Multicentric Superiority Trial (OFACAR Study). J. Clin. Med. 2023, 12, 5473. https://doi.org/10.3390/jcm12175473
Guinot P-G, Besch G, Hameury B, Grelet T, Mertes PM, Nguyen M, Bouhemad B, on behalf of the OFACAR Study Group. Protocol Study for the Evaluation of Non-Opioid Balanced General Anaesthesia in Cardiac Surgery with Cardiopulmonary Bypass: A Randomised, Controlled, Multicentric Superiority Trial (OFACAR Study). Journal of Clinical Medicine. 2023; 12(17):5473. https://doi.org/10.3390/jcm12175473
Chicago/Turabian StyleGuinot, Pierre-Grégoire, Guillaume Besch, Bastien Hameury, Tommy Grelet, Paul Michel Mertes, Maxime Nguyen, Belaid Bouhemad, and on behalf of the OFACAR Study Group. 2023. "Protocol Study for the Evaluation of Non-Opioid Balanced General Anaesthesia in Cardiac Surgery with Cardiopulmonary Bypass: A Randomised, Controlled, Multicentric Superiority Trial (OFACAR Study)" Journal of Clinical Medicine 12, no. 17: 5473. https://doi.org/10.3390/jcm12175473
APA StyleGuinot, P.-G., Besch, G., Hameury, B., Grelet, T., Mertes, P. M., Nguyen, M., Bouhemad, B., & on behalf of the OFACAR Study Group. (2023). Protocol Study for the Evaluation of Non-Opioid Balanced General Anaesthesia in Cardiac Surgery with Cardiopulmonary Bypass: A Randomised, Controlled, Multicentric Superiority Trial (OFACAR Study). Journal of Clinical Medicine, 12(17), 5473. https://doi.org/10.3390/jcm12175473