
Evaluation of Intraoral Full-Arch Scan versus Conventional Preliminary Impression
 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Impressions
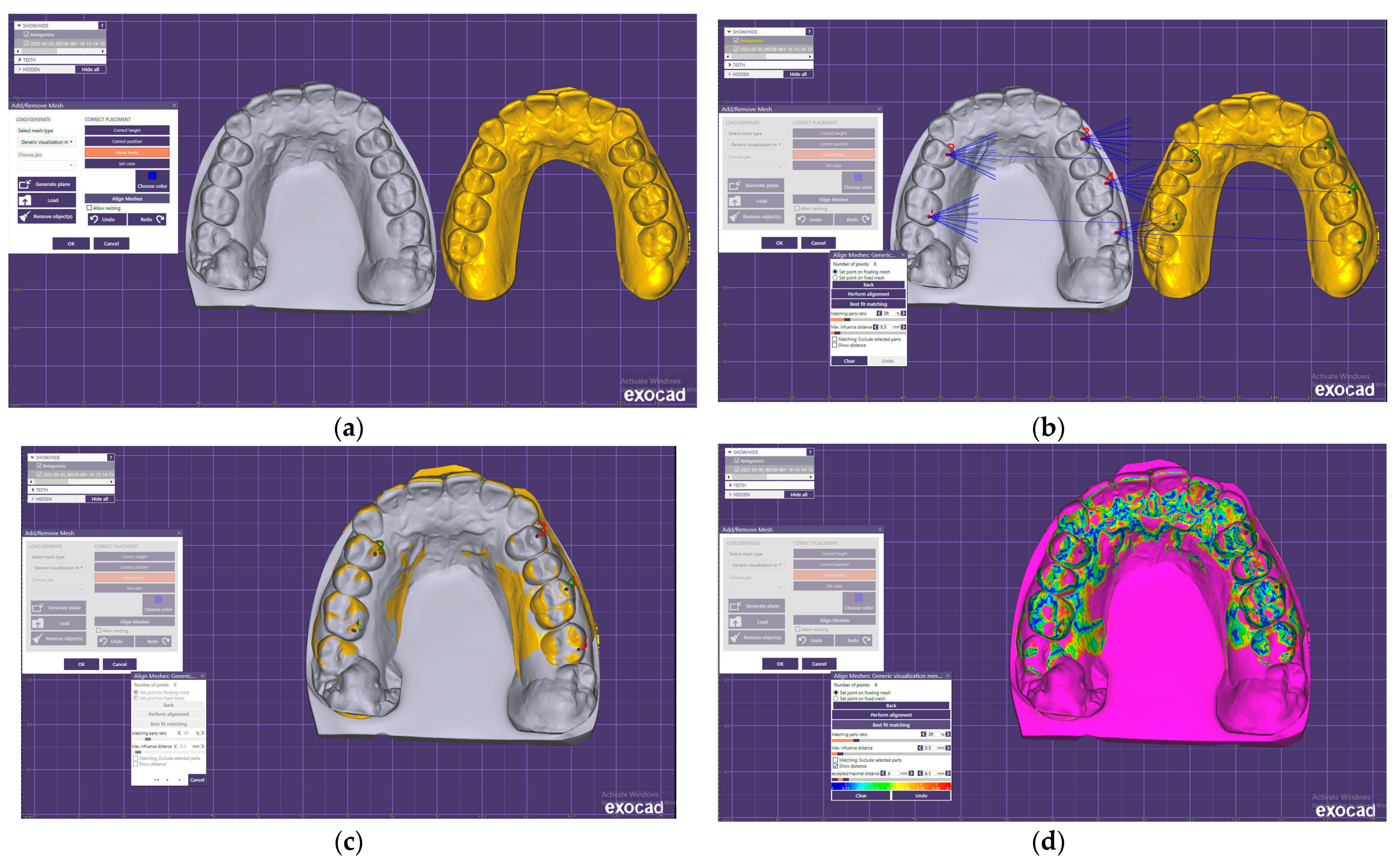
2.2. Comparison of the STL Files
2.3. Time Efficiency, Patient Point of View
2.4. Statistical Analysis
- There are no significant differences between the conventional preliminary impression technique and intraoral scan trueness.
- The digital impression is more comfortable and less time-consuming than the conventional preliminary impression.
3. Results
4. Discussion
5. Conclusions
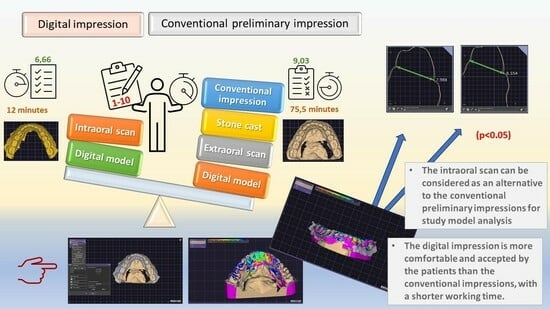
- The intraoral scan can be considered as an alternative to the conventional preliminary impression for performing study model analysis during orthodontic treatment planning.
- The digital impression is more comfortable and accepted by the patients than the conventional impression and has a shorter working time.
- The performance of the impression techniques used can be corrected with experience and good clinical skills.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gjelvold, B.; Chrcanovic, B.R.; Korduner, E.K.; Collin-Bagewitz, I.; Kisch, J. Intraoral Digital Impression Technique Compared to Conventional Impression Technique. A Randomized Clinical Trial. J. Prosthodont. 2016, 25, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Son, K.; Lee, K.B. Marginal and Internal Fit of Ceramic Restorations Fabricated Using Digital Scanning and Conventional Impressions: A Clinical Study. J. Clin. Med. 2020, 9, 4035. [Google Scholar] [CrossRef]
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014, 14, 10. [Google Scholar] [CrossRef]
- Alikhasi, M.; Siadat, H.; Nasirpour, A.; Hasanzade, M. Three-Dimensional Accuracy of Digital Impression versus Conventional Method: Effect of Implant Angulation and Connection Type. Int. J. Dent. 2018, 2018, 3761750. [Google Scholar] [CrossRef] [PubMed]
- Farhan, F.A.; Sahib, A.J.; Fatalla, A.A. Comparison of the accuracy of intraoral digital impression system and conventional impression techniques for multiple implants in the full-arch edentulous mandible. J. Clin. Exp. Dent. 2021, 13, e487–e492. [Google Scholar] [CrossRef]
- Kernen, F.; Schlager, S.; Seidel Alvarez, V.; Mehrhof, J.; Vach, K.; Kohal, R.; Nelson, K.; Flügge, T. Accuracy of intraoral scans: An in vivo study of different scanning devices. J. Prosthet. Dent. 2022, 128, 1303–1309. [Google Scholar] [CrossRef]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans-Part 1: Influence of ambient scanning light conditions on the accuracy (trueness and precision) of different intraoral scanners. J. Prosthet. Dent. 2020, 124, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.S.; Lim, Y.J.; Kim, B.; Kim, M.J.; Kwon, H.B.; Baek, Y.W. Influence of Scanning-Aid Materials on the Accuracy and Time Efficiency of Intraoral Scanners for Full-Arch Digital Scanning: An In Vitro Study. Materials 2021, 14, 2340. [Google Scholar] [CrossRef]
- Sfondrini, M.F.; Gandini, P.; Malfatto, M.; Di Corato, F.; Trovati, F.; Scribante, A. Computerized Casts for Orthodontic Purpose Using Powder-Free Intraoral Scanners: Accuracy, Execution Time, and Patient Feedback. Biomed. Res. Int. 2018, 2018, 4103232. [Google Scholar] [CrossRef]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implants Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Joda, T.; Brägger, U. Patient-centered outcomes comparing digital and conventional implant impression procedures: A randomized crossover trial. Clin. Oral Implants Res. 2016, 27, e185–e189. [Google Scholar] [CrossRef] [PubMed]
- Sason, G.K.; Mistry, G.; Tabassum, R.; Shetty, O. A comparative evaluation of intraoral and extraoral digital impressions: An in vivo study. J. Indian Prosthodont. Soc. 2018, 18, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Kim, S.W.; Lee, J.J.; Cheong, C.W. Comparison of Intraoral and Extraoral Digital Scanners: Evaluation of Surface Topography and Precision. Dent. J. 2020, 8, 52. [Google Scholar] [CrossRef] [PubMed]
- Schlenz, M.A.; Stillersfeld, J.M.; Wöstmann, B.; Schmidt, A. Update on the Accuracy of Conventional and Digital Full-Arch Impressions of Partially Edentulous and Fully Dentate Jaws in Young and Elderly Subjects: A Clinical Trial. J. Clin. Med. 2022, 11, 3723. [Google Scholar] [CrossRef] [PubMed]
- Christopoulou, I.; Kaklamanos, E.G.; Makrygiannakis, M.A.; Bitsanis, I.; Perlea, P.; Tsolakis, A.I. Intraoral Scanners in Orthodontics: A Critical Review. Int. J. Environ. Res. Public Health 2022, 19, 1407. [Google Scholar] [CrossRef]
- Mutwalli, H.; Braian, M.; Mahmood, D.; Larsson, C. Trueness and Precision of Three-Dimensional Digitizing Intraoral Devices. Int. J. Dent. 2018, 2018, 5189761. [Google Scholar] [CrossRef]
- Siqueira, R.; Galli, M.; Chen, Z.; Mendonça, G.; Meirelles, L.; Wang, H.L.; Chan, H.L. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: A systematic review. Clin. Oral Investig. 2021, 25, 6517–6531. [Google Scholar] [CrossRef]
- Lee, K.C.; Park, S.-J. Digital Intraoral Scanners and Alginate Impressions in Reproducing Full Dental Arches: A Comparative 3D Assessment. Appl. Sci. 2020, 10, 7637. [Google Scholar] [CrossRef]
- Resende, C.C.D.; Barbosa, T.A.Q.; Moura, G.F.; Tavares, L.D.N.; Rizzante, F.A.P.; George, F.M.; Neves, F.D.D.; Mendonça, G. Influence of operator experience, scanner type, and scan size on 3D scans. J. Prosthet. Dent. 2021, 125, 294–299. [Google Scholar] [CrossRef]
- Rehmann, P.; Sichwardt, V.; Wöstmann, B. Intraoral Scanning Systems: Need for Maintenance. Int. J. Prosthodont. 2017, 30, 27–29. [Google Scholar] [CrossRef]
- Schmidt, A.; Klussmann, L.; Wöstmann, B.; Schlenz, M.A. Accuracy of Digital and Conventional Full-Arch Impressions in Patients: An Update. J. Clin. Med. 2020, 9, 688. [Google Scholar] [CrossRef] [PubMed]
- Schlenz, M.A.; Schubert, V.; Schmidt, A.; Wöstmann, B.; Ruf, S.; Klaus, K. Digital versus Conventional Impression Taking Focusing on Interdental Areas: A Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 4725. [Google Scholar] [CrossRef] [PubMed]
- Arakida, T.; Kanazawa, M.; Iwaki, M.; Suzuki, T.; Minakuchi, S. Evaluating the influence of ambient light on scanning trueness, precision, and time of intra oral scanner. J. Prosthodont. Res. 2018, 62, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Güth, J.F.; Keul, C.; Stimmelmayr, M.; Beuer, F.; Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Investig. 2013, 17, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Koller, C.; Rumetsch, M.; Ender, A.; Mehl, A. Precision of guided scanning procedures for full-arch digital impressions in vivo. J. Orofac. Orthop. 2017, 78, 466–471. [Google Scholar] [CrossRef]
- Sanda, M.; Miyoshi, K.; Baba, K. Trueness and precision of digital implant impressions by intraoral scanners: A literature review. Int. J. Implant Dent. 2021, 7, 97. [Google Scholar] [CrossRef] [PubMed]
- ISO 5725-1:1994; DIN Deutsches Institut für Normung, Accuracy (Trueness and Precision) of Measurement Methods and Results—Part 1: General Principles and Definitions. Beuth Verlag GmbH: Berlin, Germany, 1997.
- Aly, P.; Mohsen, C. Comparison of the Accuracy of Three-Dimensional Printed Casts, Digital, and Conventional Casts: An In Vitro Study. Eur. J. Dent. 2020, 14, 189–193. [Google Scholar] [CrossRef]
- Ajioka, H.; Kihara, H.; Odaira, C.; Kobayashi, T. Examination of the position accuracy of implant abutments reproduced by intra-oral optical impression. PLoS ONE 2016, 11, e0164048. [Google Scholar] [CrossRef]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar]
- Schirmer, U.R.; Wiltshire, W.A. Manual and computer-aided space analysis: A comparative study. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 676–680. [Google Scholar] [CrossRef]
- Hirogaki, Y.; Sohmura, T.; Satoh, H.; Takahashi, J.; Takada, K. Complete 3-D reconstruction of dental cast shape using perceptual grouping. IEEE Trans. Med. Imaging 2001, 20, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.; Ayoub, A.F.; Siebert, P. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models. J. Orthod. 2003, 30, 219–223. [Google Scholar] [CrossRef]
- Lo Giudice, R.; Galletti, C.; Tribst, J.P.M.; Melenchón, L.P.; Matarese, M.; Miniello, A.; Cucinotta, F.; Salmeri, F. In Vivo Analysis of Intraoral Scanner Precision Using Open-Source 3D Software. Prosthesis 2022, 4, 554–563. [Google Scholar] [CrossRef]
- Suese, K. Progress in digital dentistry: The practical use of intraoral scanners. Dent. Mater. J. 2020, 39, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Boeddinghaus, M.; Breloer, E.S.; Rehmann, P.; Wöstmann, B. Accuracy of single-tooth restorations based on intraoral digital and conventional impressions in patients. Clin. Oral Investig. 2015, 19, 2027–2034. [Google Scholar] [CrossRef]
- Chochlidakis, K.M.; Papaspyridakos, P.; Geminiani, A.; Chen, C.J.; Feng, I.J.; Ercoli, C. Digital versus conventional impressions for fixed prosthodontics: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 116, 184–190.e12. [Google Scholar] [CrossRef]
- Muallah, J.; Wesemann, C.; Nowak, R.; Robben, J.; Mah, J.; Pospiech, P.; Bumann, A. Accuracy of full-arch scans using intraoral and extraoral scanners: An in vitro study using a new method of evaluation. Int. J. Comput. Dent. 2017, 20, 151–164. [Google Scholar]
- Ender, A.; Zimmermann, M.; Attin, R.; Mehl, A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin. Oral Investig. 2015, 20, 1495–1504. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Mehl, A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro. Int. J. Comput. Dent. 2019, 22, 11–19. [Google Scholar]
- Kuhr, F.; Schmidt, A.; Rehmann, P.; Wöstmann, B. A new method for assessing the accuracy of full arch impressions in patients. J. Dent. 2016, 55, 68–74. [Google Scholar] [CrossRef]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Peutzfeldt, A.; Asmussen, E. Accuracy of alginate and elastomeric impression materials. Scand. J. Dent. Res. 1989, 97, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Punj, A.; Bompolaki, D.; Garaicoa, J. Dental Impression Materials and Techniques. Dent. Clin. N. Am. 2017, 61, 779–796. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.A.; Vitti, R.P.; Consani, S.; Sinhoreti, M.A.; Mesquita, M.F.; Consani, R.L. Linear dimensional change, compressive strength and detail reproduction in type IV dental stone dried at room temperature and in a microwave oven. J. Appl. Oral Sci. 2012, 20, 588–593. [Google Scholar] [CrossRef]
- Bud, E.S.; Bocanet, V.I.; Muntean, M.H.; Vlasa, A.; Păcurar, M.; Zetu, I.N.; Soporan, B.I.; Bud, A. Extra-Oral Three-Dimensional (3D) Scanning Evaluation of Three Different Impression Materials-An In Vitro Study. Polymers 2022, 14, 3678. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef]
- Glisic, O.; Hoejbjerre, L.; Sonnesen, L. A comparison of patient experience, chair-side time, accuracy of dental arch measurements and costs of acquisition of dental models. Angle Orthod. 2019, 89, 868–875. [Google Scholar] [CrossRef]
- Mangano, A.; Beretta, M.; Luongo, G.; Mangano, C.; Mangano, F. Conventional Vs Digital Impressions: Acceptability, Treatment Comfort and Stress Among Young Orthodontic Patients. Open. Dent. J. 2018, 12, 118–124. [Google Scholar] [CrossRef]
- Schepke, U.; Meijer, H.J.; Kerdijk, W.; Cune, M.S. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J. Prosthet. Dent. 2015, 114, 403–406.e1. [Google Scholar] [CrossRef]
- Grünheid, T.; McCarthy, S.D.; Larson, B.E. Clinical use of a direct chairside oral scanner: An assessment of accuracy, time, and patient acceptance. Am. J. Orthod. Dentofacial Orthop. 2014, 146, 673–682. [Google Scholar] [CrossRef]
- Gallardo, Y.R.; Bohner, L.; Tortamano, P.; Pigozzo, M.N.; Laganá, D.C.; Sesma, N. Patient outcomes and procedure working time for digital versus conventional impressions: A systematic review. J. Prosthet. Dent. 2018, 119, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Burzynski, J.A.; Firestone, A.R.; Beck, F.M.; Fields, H.W., Jr.; Deguchi, T. Comparison of digital intraoral scanners and alginate impressions: Time and patient satisfaction. Am. J. Orthod. Dentofacial Orthop. 2018, 153, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Muhlemann, S.; Fehmer, V.; Hammerle, C.H.F.; Benic, G.I. Randomized controlled clinical trial of digital and conventional workflows for the fabrication of zirconia-ceramic fixed partial dentures. Part I: Time efficiency of complete-arch digital scans versus conventional impressions. J. Prosthet. Dent. 2019, 121, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Benic, G.I.; Mühlemann, S.; Fehmer, V.; Hämmerle, C.H.; Sailer, I. Randomized controlled within-subject evaluation of digital and conventional workflows for the fabrication of lithium disilicate single crowns. Part I: Digital versus conventional unilateral impressions. J. Prosthet. Dent. 2016, 116, 777–782. [Google Scholar] [CrossRef]
- Wismeijer, D.; Mans, R.; van Genuchten, M.; Reijers, H.A. Patients’ preferences when comparing analogue implant impressions using a polyether impression material versus digital impressions (Intraoral Scan) of dental implants. Clin. Oral Implants Res. 2014, 25, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Papi, P.; Di Murro, B.; Penna, D.; Pompa, G. Digital prosthetic workflow during COVID-19 pandemic to limit infection risk in dental practice. Oral Dis. 2021, 27, 723–726. [Google Scholar] [CrossRef] [PubMed]
- Chidambaranathan, A.S.; Balasubramanium, M. Comprehensive Review and Comparison of the Disinfection Techniques Currently Available in the Literature. J. Prosthodont. 2019, 28, e849–e856. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Upper Arch (mm) | Lower Arch (mm) | |||||
|---|---|---|---|---|---|---|
| 11 | 16 | 26 | 31 | 36 | 46 | |
| Minimum | 0.1700 | 0.1040 | 0.002000 | 0.1050 | 0.1320 | 0.000 |
| 25% Percentile | 0.1785 | 0.1670 | 0.2040 | 0.1673 | 0.1990 | 0.1320 |
| Median | 0.2290 | 0.2310 | 0.2675 | 0.2090 | 0.2390 | 0.2530 |
| 75% Percentile | 0.2980 | 0.3850 | 0.3480 | 0.2873 | 0.4530 | 0.3880 |
| Maximum | 0.3310 | 0.4970 | 0.6200 | 0.3460 | 0.6300 | 0.4410 |
| Range | 0.1610 | 0.3930 | 0.6180 | 0.2410 | 0.4980 | 0.4410 |
| Mean | 0.2355 | 0.2770 | 0.2581 | 0.2155 | 0.3171 | 0.2426 |
| Std. Deviation | 0.05577 | 0.1265 | 0.1552 | 0.07027 | 0.1560 | 0.1390 |
| Std. Error of Mean | 0.01054 | 0.02390 | 0.02932 | 0.01328 | 0.02948 | 0.02627 |
| Lower 95% CI of Mean | 0.2139 | 0.2279 | 0.1980 | 0.1883 | 0.2566 | 0.1887 |
| Upper 95% CI of Mean | 0.2571 | 0.3260 | 0.3183 | 0.2428 | 0.3776 | 0.2965 |
| Mann–Whitney | Difference | p-Value | |
|---|---|---|---|
| 11 vs. 31 | 301.5 | 0.02000 | 0.1394 |
| 16 vs. 46 | 338 | −0.02200 | 0.3808 |
| 26 vs. 36 | 364.5 | 0.02850 | 0.6571 |
| Mann–Whitney U | Difference | p-Value | |
|---|---|---|---|
| 11 vs. 16 | 353 | −0.00200 | 0.5279 |
| 11 vs. 26 | 302 | −0.03850 | 0.1418 |
| 16 vs. 26 | 378 | −0.03650 | 0.8229 |
| 31 vs. 46 | 350 | −0.04400 | 0.4963 |
| 31 vs. 36 | 236 | −0.03000 | 0.0098 ** |
| 36 vs. 46 | 295 | −0.01400 | 0.1129 |
| Conventional Impression | Digital Impression | p-Value | |
|---|---|---|---|
| Minimum | 4.000 | 8.000 | <0.0001 **** |
| Median | 6.750 | 9.000 | |
| Maximum | 8.500 | 10.00 | |
| Mean | 6.500 | 9.018 | |
| Std. Deviation | 1.333 | 0.7756 | |
| Std. Error of Mean | 0.2520 | 0.1466 | |
| Lower 95% CI | 5.983 | 8.717 | |
| Upper 95% CI | 7.017 | 9.319 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jánosi, K.M.; Cerghizan, D.; Mártha, K.I.; Elekes, É.; Szakács, B.; Elekes, Z.; Kovács, A.; Szász, A.; Mureșan, I.; Hănțoiu, L.G. Evaluation of Intraoral Full-Arch Scan versus Conventional Preliminary Impression. J. Clin. Med. 2023, 12, 5508. https://doi.org/10.3390/jcm12175508
Jánosi KM, Cerghizan D, Mártha KI, Elekes É, Szakács B, Elekes Z, Kovács A, Szász A, Mureșan I, Hănțoiu LG. Evaluation of Intraoral Full-Arch Scan versus Conventional Preliminary Impression. Journal of Clinical Medicine. 2023; 12(17):5508. https://doi.org/10.3390/jcm12175508
Chicago/Turabian StyleJánosi, Kinga Mária, Diana Cerghizan, Krisztina Ildikó Mártha, Éva Elekes, Brigitta Szakács, Zoltán Elekes, Alpár Kovács, Andrea Szász, Izabella Mureșan, and Liana Georgiana Hănțoiu. 2023. "Evaluation of Intraoral Full-Arch Scan versus Conventional Preliminary Impression" Journal of Clinical Medicine 12, no. 17: 5508. https://doi.org/10.3390/jcm12175508