

The Effect of Telemedicine in Glycemic Control in Adult Patients with Diabetes during the COVID-19 Era—A Systematic Review

Abstract
:1. Introduction
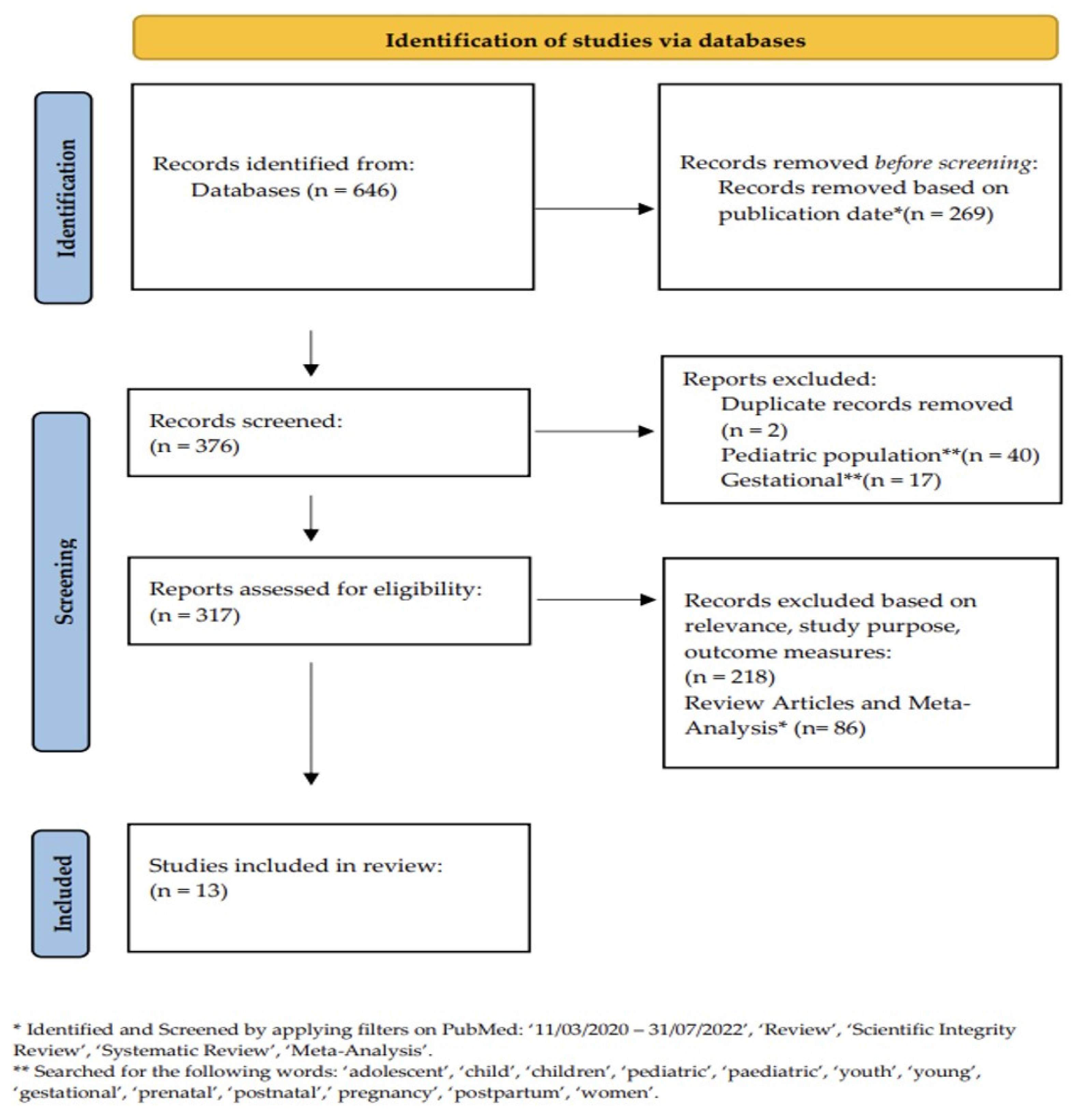
2. Methods
3. Results
3.1. Evidence from Retrospective Studies
3.2. Evidence from Prospective Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Centers for Disease Control and Prevention. By the Numbers: Diabetes in America. Available online: https://www.cdc.gov/diabetes/health-equity/diabetes-by-the-numbers.html (accessed on 25 October 2022).
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Spanakis, E.K.; Yoo, A.; Ajayi, O.N.; Siddiqui, T.; Khan, M.M.; Seliger, S.L.; Klonoff, D.C.; Feng, Z.; Sorkin, J.D. Excess Mortality in COVID-19-Positive Versus COVID-19-Negative Inpatients with Diabetes: A Nationwide Study. Diabetes Care 2021, 44, e169–e170. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Aberer, F.; Hochfellner, D.A.; Mader, J.K. Application of Telemedicine in Diabetes Care: The Time is Now. Diabetes Ther. 2021, 12, 629–639. [Google Scholar] [CrossRef]
- Agarwal, K.M.; Mohapatra, S.; Sharma, P.; Sharma, S.; Bhatia, D.; Mishra, A. Study and overview of the novel corona virus disease (COVID-19). Sens. Int. 2020, 1, 100037. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.Y.; Mehrotra, A.; Huskamp, H.A.; Uscher-Pines, L.; Ganguli, I.; Barnett, M.L. Trends in Outpatient Care Delivery and Telemedicine During the COVID-19 Pandemic in the US. JAMA Intern. Med. 2021, 181, 388–391. [Google Scholar] [CrossRef]
- Dupraz, J.; Le Pogam, M.-A.; Peytremann-Bridevaux, I. Early impact of the COVID-19 pandemic on in-person outpatient care utilisation: A rapid review. BMJ Open 2022, 12, e056086. [Google Scholar] [CrossRef]
- Mann, D.M.; Chen, J.; Chunara, R.; Testa, P.A.; Nov, O. COVID-19 transforms health care through telemedicine: Evidence from the field. J. Am. Med Inform. Assoc. 2020, 27, 1132–1135. [Google Scholar] [CrossRef]
- Scott, S.N.; Fontana, F.Y.; Züger, T.; Laimer, M.; Stettler, C. Use and perception of telemedicine in people with type 1 diabetes during the COVID-19 pandemic—Results of a global survey. Endocrinol. Diabetes Metab. 2020, 4, e00180. [Google Scholar] [CrossRef]
- Telemedicine: A Guide to Assessing Telecommunications in Health Care; Field, M.J. (Ed.) National Academies Press: Washington, DC, USA, 1996. [Google Scholar]
- (CMS) CfMaMS. Medicare Telemedicine Health Care Provider Fact Sheet. 2020. Available online: https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet (accessed on 6 June 2023).
- Garg, S.K.; Rodbard, D.; Hirsch, I.B.; Forlenza, G.P. Managing New-Onset Type 1 Diabetes during the COVID-19 Pandemic: Challenges and Opportunities. Diabetes Technol. Ther. 2020, 22, 431–439. [Google Scholar] [CrossRef]
- Pinsker, J.E.; Singh, H.; Malloy, M.M.; Constantin, A.; Leas, S.; Kriegel, K.; Habif, S. A Virtual Training Program for the Tandem t:slim X2 Insulin Pump: Implementation and Outcomes. Diabetes Technol. Ther. 2021, 23, 467–470. [Google Scholar] [CrossRef] [PubMed]
- de Kreutzenberg, S.V. Telemedicine for the Clinical Management of Diabetes; Implications and Considerations after COVID-19 Experience. High Blood Press. Cardiovasc. Prev. 2022, 29, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Longo, M.; Caruso, P.; Petrizzo, M.; Castaldo, F.; Sarnataro, A.; Gicchino, M.; Bellastella, G.; Esposito, K.; Maiorino, M.I. Glycemic control in people with type 1 diabetes using a hybrid closed loop system and followed by telemedicine during the COVID-19 pandemic in Italy. Diabetes Res. Clin. Pract. 2020, 169, 108440. [Google Scholar] [CrossRef] [PubMed]
- Boscari, F.; Ferretto, S.; Uliana, A.; Avogaro, A.; Bruttomesso, D. Efficacy of telemedicine for persons with type 1 diabetes during Covid19 lockdown. Nutr. Diabetes 2021, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- Alharthi, S.K.; Alyusuf, E.Y.; Alguwaihes, A.M.; Alfadda, A.; Al-Sofiani, M.E. The impact of a prolonged lockdown and use of telemedicine on glycemic control in people with type 1 diabetes during the COVID-19 outbreak in Saudi Arabia. Diabetes Res. Clin. Pract. 2021, 173, 108682. [Google Scholar] [CrossRef]
- Scoccimarro, D.; Giove, G.; Silverii, A.; Dicembrini, I.; Mannucci, E. Effects of home confinement during COVID-19 outbreak on glycemic control in patients with type 2 diabetes receiving telemedicine support. Acta Diabetol. 2021, 59, 281–284. [Google Scholar] [CrossRef]
- Mithal, A.; Dutta, A.; Mahendru, S.; Sharma, R.; Singh, A.; Jain, A.; Jevalikar, G. Video consultation versus in-person clinic visit for glycemic control in type 2 diabetes during COVID-19 pandemic (VIP-CD study). Indian J. Endocrinol. Metab. 2021, 25, 427–431. [Google Scholar] [CrossRef]
- AlMutairi, M.F.; Tourkmani, A.M.; Alrasheedy, A.A.; Alharbi, T.J.; Bin Rsheed, A.M.; Aljehani, M.; AlRuthia, Y. Cost-effectiveness of telemedicine care for patients with uncontrolled type 2 diabetes mellitus during the COVID-19 pandemic in Saudi Arabia. Ther. Adv. Chronic Dis. 2021, 12, 20406223211042542. [Google Scholar] [CrossRef]
- Woodhouse, A.G.; Orvin, C.; Rich, C.; Crosby, J.; Keedy, C.A. Diabetes outcomes before and during telehealth advancements surrounding COVID-19. J. Am. Pharm. Assoc. 2022, 62, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Onishi, Y.; Ichihashi, R.; Yoshida, Y.; Tahara, T.; Kikuchi, T.; Kobori, T.; Kubota, T.; Iwamoto, M.; Hamano, S.; Kasuga, M. Substitution of telemedicine for clinic visit during the COVID-19 pandemic of 2020: Comparison of telemedicine and clinic visit. J. Diabetes Investig. 2022, 13, 1617–1625. [Google Scholar] [CrossRef] [PubMed]
- Onishi, Y.; Yoshida, Y.; Takao, T.; Tahara, T.; Kikuchi, T.; Kobori, T.; Kubota, T.; Shimmei, A.; Iwamoto, M.; Kasuga, M. Diabetes management by either telemedicine or clinic visit improved glycemic control during the coronavirus disease 2019 pandemic state of emergency in Japan. J. Diabetes Investig. 2021, 13, 386–390. [Google Scholar] [CrossRef]
- Wong, V.W.; Wang, A.; Manoharan, M. Utilisation of telehealth for outpatient diabetes management during COVID-19 pandemic: How did the patients fare? Intern. Med. J. 2021, 51, 2021–2026. [Google Scholar] [CrossRef] [PubMed]
- Parise, M.; Tartaglione, L.; Cutruzzolà, A.; Maiorino, M.I.; Esposito, K.; Pitocco, D.; Gnasso, A.; Irace, C. Teleassistance for Patients With Type 1 Diabetes during the COVID-19 Pandemic: Results of a Pilot Study. J. Med. Internet Res. 2021, 23, e24552. [Google Scholar] [CrossRef] [PubMed]
- Zeller, W.P.; DeGraff, R. A novel telemedicine protocol improved outcomes for high-risk patients with type 1 diabetes: A 3-month quality improvement project during the COVID-19 pandemic. J. Clin. Transl. Endocrinol. Case Rep. 2021, 19, 100078. [Google Scholar] [CrossRef] [PubMed]
- Tourkmani, A.M.; Alharbi, T.J.; Rsheed, A.M.B.; Alrasheedy, A.A.; Almadani, W.; Aljuraisi, F.; AlOtaibi, A.F.; AlHarbi, M.; AlAbood, A.F.; Ibn Alshaikh, A.A. The impact of telemedicine on patients with uncontrolled type 2 diabetes mellitus during the COVID-19 pandemic in Saudi Arabia: Findings and implications. J. Telemed. Telecare 2021, 29, 390–398. [Google Scholar] [CrossRef]
- Monnier, L.; Colette, C.; Owens, D.R. Glycemic variability: The third component of the dysglycemia in diabetes. Is it important? How to measure it? J. Diabetes Sci. Technol. 2008, 2, 1094–1100. [Google Scholar] [CrossRef]
- Diabetes Control and Complications Trial Research Group; Nathan, D.M.; Genuth, S.; Lachin, J.; Cleary, P.; Crofford, O.; Davis, M.; Rand, L.; Siebert, C. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar] [CrossRef]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Lee, A.K.; Warren, B.; Lee, C.J.; McEvoy, J.W.; Matsushita, K.; Huang, E.S.; Sharrett, A.R.; Coresh, J.; Selvin, E. The Association of Severe Hypoglycemia With Incident Cardiovascular Events and Mortality in Adults With Type 2 Diabetes. Diabetes Care 2017, 41, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Holman, N.; Hillson, R.; Young, R.J. Excess mortality during hospital stays among patients with recorded diabetes compared with those without diabetes. Diabet. Med. 2013, 30, 1393–1402. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.; Lee, T.H. In-Person Health Care as Option B. N. Engl. J. Med. 2018, 378, 104–106. [Google Scholar] [CrossRef] [PubMed]
- Mushcab, H.; Kernohan, W.G.; Wallace, J.; Martin, S. Web-Based Remote Monitoring Systems for Self-Managing Type 2 Diabetes: A Systematic Review. Diabetes Technol. Ther. 2015, 17, 498–509. [Google Scholar] [CrossRef]
- Mobile Fact Sheet. 2021. Available online: https://www.pewresearch.org/internet/fact-sheet/mobile/ (accessed on 6 June 2023).
- Internet/Broadband Fact Sheet. 2021. Available online: https://www.pewresearch.org/internet/fact-sheet/internet-broadband/ (accessed on 6 June 2023).



{kind=link}
{kind=link}
| Ref. | Country | Population | Study Aim | DM Regimen | Glycemic Monitor | Results |
|---|---|---|---|---|---|---|
| [18] | Italy | T1DM a n = 30 | Evaluating the metrics of glycemic control in T1DM patients using HCL pumps across 4 different time points during lockdown (Time 0: pre-lockdown; Time 1: First 2 weeks of lockdown; Time 2: Last 2 weeks of lockdown; Time 3: post-lockdown). | CSII c | CGM g |
|
| [19] | Italy | T1 DM a n = 71 | Analyze data from CGM g or FGM h systems during the lockdown diabetes and compare data obtained 4 weeks before and 4 weeks after structured telephone visits. | MDI d and CSII c | CGM g FGM h |
|
| [20] | Saudi Arabia | T1 DM a n = 101 | Assess glycemic control in those who attended a telemedicine visit during the 6-week lockdown period vs. those who did not. | MDI d and CSII c | FGM h |
|
| [21] | Italy | T2DM b n = 269 | Difference in Hb A1c and body weight between May–June 2020 (after lockdown) vs. November–February 2020 (before lockdown). | Insulin OHA e GLP-1 f | N/A t |
|
| [22] | India | T2DM b n = 96 | Compare glycemic control in those evaluated through telemedicine vs. those evaluated in person (IPV) r | MDI d, OHA e, GLP-1 f | FPG i PPPG j |
|
| [23] | Saudi Arabia | T2DM b n = 200 | Impact of telemedicine on glycemic control on patients with uncontrolled diabetes (HbA1c > 9%) vs. traditional care mode between March and June 2020. | Insulin | SMBG k |
|
| [24] | United States | T2DM b n = 91 | Determine the overall change in A1C between August 2019 and February 2020 (pre- COVID-19 group) and March and October 2020 (COVID-19 group) in a pharmacy driven telehealth services during the COVID-19 public health emergency (PHE) in patients with HbA1c p > 8%. | N/A t | N/A t |
|
| [25] | Japan | T1DM a = 407 T2DM b = 6534 n = 6941 | Compare outpatient diabetes care and HbA1c p levels during the COVID-19 pandemic in 2020 with 2019. | MDI d, OHA e, GLP-1 f | N/A t |
|
| [26] | Japan | T1DM a = 171 T2DM b = 2556 n = 2727 | Assess the impact of telemedicine on HbA1c p between the pre-emergency period (February–April 2020) and the post-emergency period (May–July 2020). | N/A s | N/A t |
|
| [27] | Australia | T1DM a = 92 T2DM b = 412 n = 504 | Assess attendance rate, glycemic control, and unplanned hospital admissions between April 1st 2020 and September 2020 (visit A) compared to patients in the same time period in 2019 (visit B) and compared to patients that attended the clinic between April and September 2020 and had been attending the clinic for at least 12 months prior to the onset of the pandemic (Visit C). | MDI d | SBMG k |
|
| Ref. | Country | Population | Study Aim | DM Regimen | Glycemic Monitor | Results |
|---|---|---|---|---|---|---|
| [28] | Italy | T1DM a n = 166 | Assess glycemic control at baseline vs. follow up on patients that completed 2 virtual visits between 10 March 2020 and 3 June 2020. | MDI d CSII c | CGM g SMBG h |
|
| [29] | United States | T1DM a n = 87 | Impact of telemedicine on the number of hospitalizations for DKA n, incidence of severe hypoglycemia and GMI l among patients with GMI l > 9%s in a 3-month study compared with patient with uncontrolled DM in the T1D Exchange with HbA1c m > 9%. | MDI d CSII c | CGM g |
|
| [30] | Saudi Arabia | T2DM b n = 130 | Impact of telemedicine on glycemic control on high-risk patients (HbA1c m > 9%) attending a virtual integrated care clinic over a 4-month period during the pandemic | MDI d OHA e GLP-1 f | SMBG h |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sotomayor, F.; Hernandez, R.; Malek, R.; Parimi, N.; Spanakis, E.K. The Effect of Telemedicine in Glycemic Control in Adult Patients with Diabetes during the COVID-19 Era—A Systematic Review. J. Clin. Med. 2023, 12, 5673. https://doi.org/10.3390/jcm12175673
Sotomayor F, Hernandez R, Malek R, Parimi N, Spanakis EK. The Effect of Telemedicine in Glycemic Control in Adult Patients with Diabetes during the COVID-19 Era—A Systematic Review. Journal of Clinical Medicine. 2023; 12(17):5673. https://doi.org/10.3390/jcm12175673
Chicago/Turabian StyleSotomayor, Fiorella, Reynier Hernandez, Rana Malek, Nehu Parimi, and Elias K. Spanakis. 2023. "The Effect of Telemedicine in Glycemic Control in Adult Patients with Diabetes during the COVID-19 Era—A Systematic Review" Journal of Clinical Medicine 12, no. 17: 5673. https://doi.org/10.3390/jcm12175673
APA StyleSotomayor, F., Hernandez, R., Malek, R., Parimi, N., & Spanakis, E. K. (2023). The Effect of Telemedicine in Glycemic Control in Adult Patients with Diabetes during the COVID-19 Era—A Systematic Review. Journal of Clinical Medicine, 12(17), 5673. https://doi.org/10.3390/jcm12175673