
The Increase in Childhood Obesity and Its Association with Hypertension during Pandemics
 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methodology
3. The Well-Established Connection between Childhood Obesity and Hypertension Long before the COVID-19 Pandemic
4. Trends in Childhood Obesity and Hypertension Amidst the Pandemic
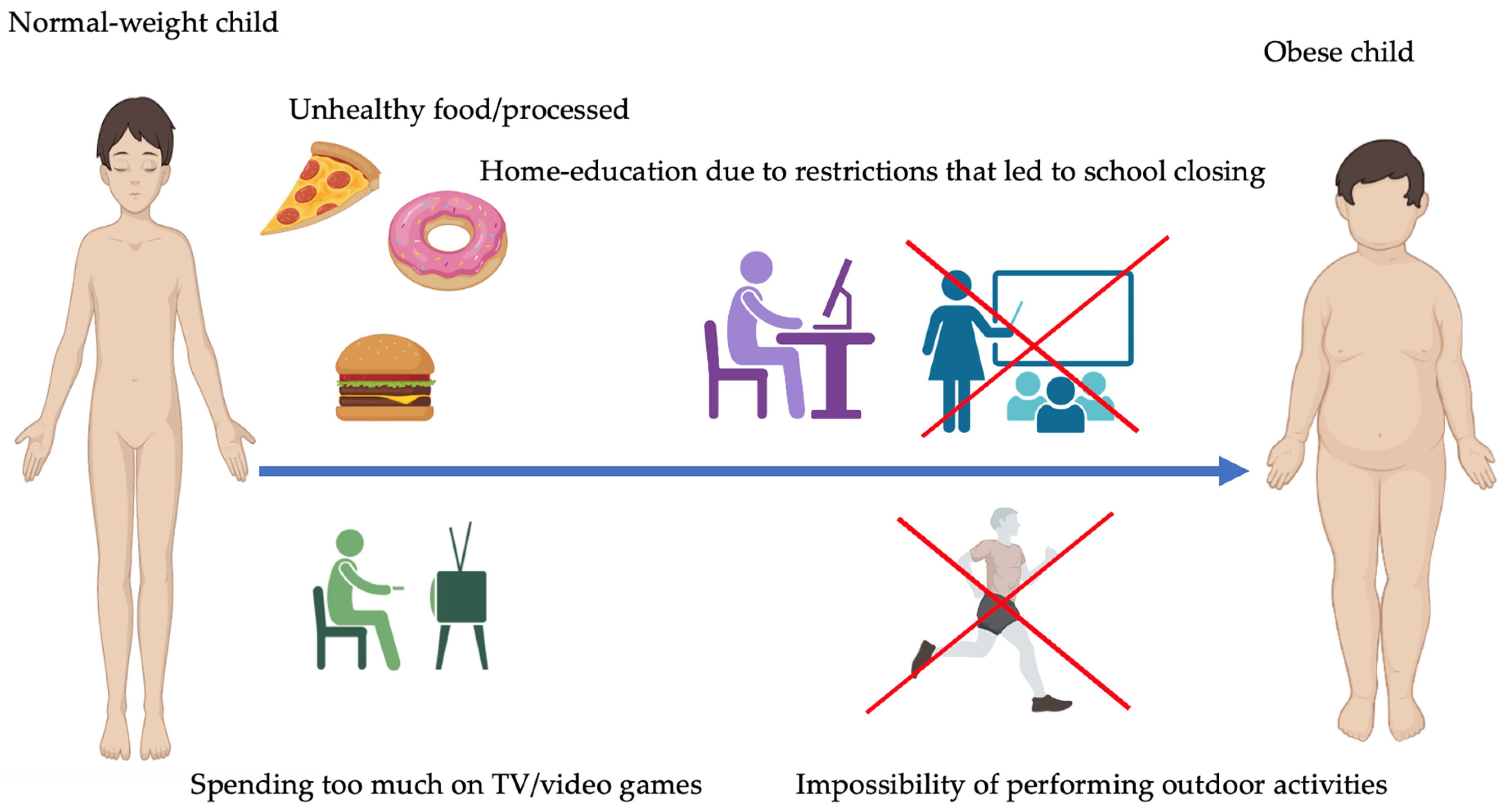
5. Factors Contributing to Childhood Obesity during Pandemics
6. Psychological Impact of Pandemics on Childhood Obesity
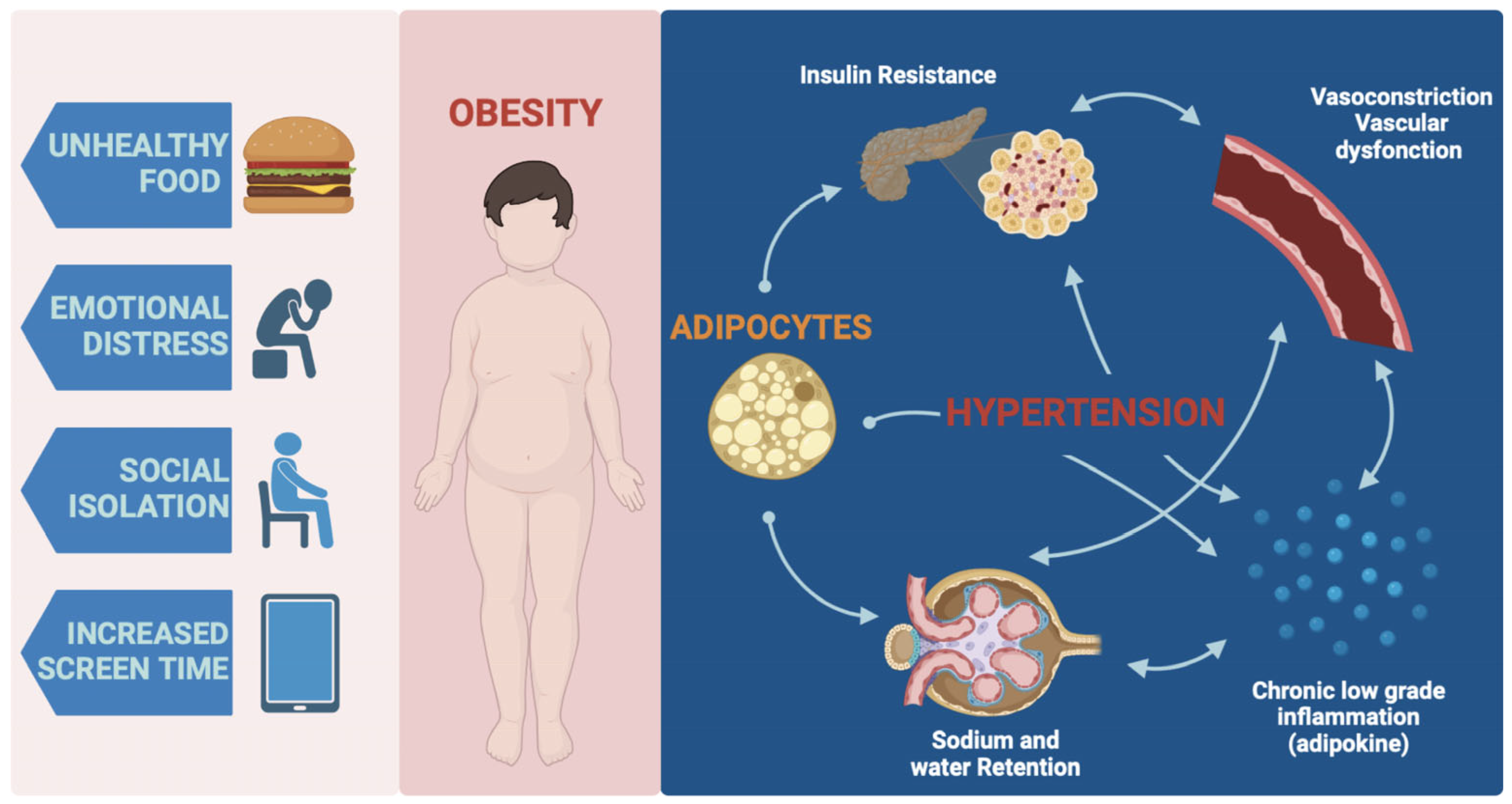
7. Association between Childhood Obesity and Hypertension
8. Underlying Genetics of Childhood Obesity
9. Implications for Public Health and Interventions
10. Future Directions and Research Needs
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pavone, P.; Ceccarelli, M.; Taibi, R.; La Rocca, G.; Nunnari, G. Outbreak of COVID-19 infection in children: Fear and serenity. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4572–4575. [Google Scholar] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: A Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Theberath, M.; Bauer, D.; Chen, W.; Salinas, M.; Mohabbat, A.B.; Yang, J.; Chon, T.Y.; Bauer, B.A.; Wahner-Roedler, D.L. Effects of COVID-19 pandemic on mental health of children and adolescents: A systematic review of survey studies. SAGE Open Med. 2022, 10, 20503121221086712. [Google Scholar] [CrossRef]
- Xu, S.; Xue, Y. Pediatric obesity: Causes, symptoms, prevention and treatment. Exp. Ther. Med. 2016, 11, 15–20. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Qi, X.; Locke, J.; Rehman, S. Childhood and Adolescent Obesity in the United States: A Public Health Concern. Glob. Pediatr. Health 2019, 6, 2333794X19891305. [Google Scholar] [CrossRef]
- Nicodemo, M.; Spreghini, M.R.; Manco, M.; Wietrzykowska Sforza, R.; Morino, G. Childhood Obesity and COVID-19 Lockdown: Remarks on Eating Habits of Patients Enrolled in a Food-Education Program. Nutrients 2021, 13, 383. [Google Scholar] [CrossRef] [PubMed]
- Chaves, E.; Reddy, S.D.; Cadieux, A.; Tomasula, J.; Reynolds, K. The Continued Impact of the COVID-19 Pandemic on Pediatric Obesity: A Commentary on the Return to a Healthy New “Normal”. Int. J. Environ. Res. Public Health 2022, 19, 5597. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Luo, B.; Zhao, L.; Liao, S. Influences of the COVID-19 Pandemic on Obesity and Weight-Related Behaviors among Chinese Children: A Multi-Center Longitudinal Study. Nutrients 2022, 14, 3744. [Google Scholar] [CrossRef]
- Salvadori, M.; Sontrop, J.M.; Garg, A.X.; Truong, J.; Suri, R.S.; Mahmud, F.H.; Macnab, J.J.; Clark, W.F. Elevated Blood Pressure in Relation to Overweight and Obesity Among Children in a Rural Canadian Community. Pediatrics 2008, 122, e821–e827. [Google Scholar] [CrossRef]
- Kovacs, V.A.; Gabor, A.; Fajcsak, Z.; Martos, E. Role of waist circumference in predicting the risk of high blood pressure in children. Int. J. Pediatr. Obes. 2010, 5, 143–150. [Google Scholar] [CrossRef]
- Mehdad, S.; Hamrani, A.; El Kari, K.; El Hamdouchi, A.; El Mzibri, M.; Barkat, A.; Aguenaou, H.; Mokhtar, N. Prevalence of elevated blood pressure and its relationship with fat mass, body mass index and waist circumference among a group of Moroccan overweight adolescents. Obes. Res. Clin. Pract. 2012, 7, e284–e289. [Google Scholar] [CrossRef] [PubMed]
- Meydanlioglu, A.; Akcan, A.; Oncel, S.; Adibelli, D.; Gumus, E.C.; Sarvan, S.; Kavla, I. Prevalence of obesity and hypertension in children and determination of associated factors by CHAID analysis. Arch. Pédiatr. 2022, 29, 30–35. [Google Scholar] [CrossRef]
- Rebelo, D.; Teixeira, J.; Marques-Vidal, P.; Oliveira, J.M. Obesity markers and blood pressure in a sample of Portuguese children and adolescents. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Shi, P.; Luo, C.-Y.; Zhou, Y.-F.; Yu, H.-T.; Guo, C.-Y.; Wu, F. Prevalence of hypertension in overweight and obese children from a large school-based population in Shanghai, China. BMC Public Health 2013, 13, 24. [Google Scholar] [CrossRef] [PubMed]
- Dulskiene, V.; Kuciene, R.; Medzioniene, J.; Benetis, R. Association between obesity and high blood pressure among Lithuanian adolescents: A cross-sectional study. Ital. J. Pediatr. 2014, 40, 102. [Google Scholar] [CrossRef]
- Carducci, B.; Keats, E.C.; Ruel, M.; Haddad, L.; Osendarp, S.J.M.; Bhutta, Z.A. Food systems, diets and nutrition in the wake of COVID-19. Nat. Food 2021, 2, 68–70. [Google Scholar] [CrossRef]
- Okado, Y.; Scaramella, C.; Nguyen, H.M.; Mendoza, B.; Watarastaporn, T. Psychosocial adjustment of U.S. college students in the early months of the COVID-19 pandemic. J. Am. Coll. Health 2021, 71, 1281–1292. [Google Scholar] [CrossRef]
- Jha, S.; Mehendale, A.M. Increased Incidence of Obesity in Children and Adolescents Post-COVID-19 Pandemic: A Review Article. Cureus 2022, 14, e29348. [Google Scholar] [CrossRef]
- Qiu, N.; He, H.; Qiao, L.; Ding, Y.; Ji, S.; Guo, X.; Luo, J.; Luo, Z.; Li, Y.; Pang, H.; et al. Sex differences in changes in BMI and blood pressure in Chinese school-aged children during the COVID-19 quarantine. Int. J. Obes. 2021, 45, 2132–2136. [Google Scholar] [CrossRef]
- Rundle, A.G.; Park, Y.; Herbstman, J.B.; Kinsey, E.W.; Wang, Y.C. COVID-19–Related School Closings and Risk of Weight Gain Among Children. Obesity 2020, 28, 1008–1009. [Google Scholar] [CrossRef]
- Browne, N.T.; Snethen, J.A.; Greenberg, C.S.; Frenn, M.; Kilanowski, J.F.; Gance-Cleveland, B.; Burke, P.J.; Lewandowski, L. When Pandemics Collide: The Impact of COVID-19 on Childhood Obesity. J. Pediatr. Nurs. 2021, 56, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Dallolio, L.; Marini, S.; Masini, A.; Toselli, S.; Stagni, R.; Bisi, M.C.; Gori, D.; Tessari, A.; Sansavini, A.; Lanari, M.; et al. The impact of COVID-19 on physical activity behaviour in Italian primary school children: A comparison before and during pandemic considering gender differences. BMC Public Health 2022, 22, 52. [Google Scholar] [CrossRef] [PubMed]
- Heidari-Beni, M.; Bemanalizadeh, M.; Heshmat, R.; Qorbani, M.; Kelishadi, R. Changes in Lifestyle Behaviors of Children and Adolescents during the COVID-19 Pandemic and the Impact on the Development of Non-Communicable Diseases: A Narrative Review. Med. J. Islam. Repub. Iran 2022, 36, 1285–1290. [Google Scholar] [CrossRef]
- Nowicka, P.; Ek, A.; Jurca-Simina, I.E.; Bouzas, C.; Argelich, E.; Nordin, K.; García, S.; Barquero, M.Y.V.; Hoffer, U.; Richards, H.R.; et al. Explaining the complex impact of the COVID-19 pandemic on children with overweight and obesity: A comparative ecological analysis of parents’ perceptions in three countries. BMC Public Health 2022, 22, 1000. [Google Scholar] [CrossRef] [PubMed]
- McNicholas, J.; Hammersley, M.L.; Hopkins, S.; McDermott, S.; Plaskett, J. The Impact of COVID-19 Restrictions on the Healthy Eating and Movement Behaviors of 0–12-Year-Old Children in Western Sydney, Australia. Front. Public Health 2022, 10, 841178. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, A.S.; Schmidt, L.; Beck, A.; Kepper, M.M.; Mazzucca, S.; Eyler, A. Associations of physical activity and sedentary behaviors with child mental well-being during the COVID-19 pandemic. BMC Public Health 2021, 21, 1770. [Google Scholar] [CrossRef]
- Singh, S.; Roy, D.; Sinha, K.; Parveen, S.; Sharma, G.; Joshi, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 2020, 293, 113429. [Google Scholar] [CrossRef]
- Dalton, L.; Rapa, E.; Stein, A. Protecting the psychological health of children through effective communication about COVID-19. Lancet Child Adolesc. Health 2020, 4, 346–347. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Jiao, W.Y.; Wang, L.N.; Liu, J.; Fang, S.F.; Jiao, F.Y.; Pettoello-Mantovani, M.; Somekh, E. Behavioral and Emotional Disorders in Children during the COVID-19 Epidemic. J. Pediatr. 2020, 221, 264–266.e1. [Google Scholar] [CrossRef]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef] [PubMed]
- Pietrabissa, G.; Volpi, C.; Bottacchi, M.; Bertuzzi, V.; Usubini, A.G.; Löffler-Stastka, H.; Prevendar, T.; Rapelli, G.; Cattivelli, R.; Castelnuovo, G.; et al. The Impact of Social Isolation during the COVID-19 Pandemic on Physical and Mental Health: The Lived Experience of Adolescents with Obesity and Their Caregivers. Int. J. Environ. Res. Public Health 2021, 18, 3026. [Google Scholar] [CrossRef] [PubMed]
- Bzdok, D.; Dunbar, R.I.M. Social isolation and the brain in the pandemic era. Nat. Hum. Behav. 2022, 6, 1333–1343. [Google Scholar] [CrossRef]
- de Figueiredo, C.S.; Sandre, P.C.; Portugal, L.C.L.; Mázala-De-Oliveira, T.; da Silva Chagas, L.; Raony, Í.; Ferreira, E.S.; Giestal-De-Araujo, E.; dos Santos, A.A.; Bomfim, P.O.-S. COVID-19 pandemic impact on children and adolescents’ mental health: Biological, environmental, and social factors. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 106, 110171. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.; Thapaliya, G.; Aghababian, A.; Sadler, J.; Smith, K.; Carnell, S. Parental stress, food parenting practices and child snack intake during the COVID-19 pandemic. Appetite 2021, 161, 105119. [Google Scholar] [CrossRef]
- Titis, E. Parental Perspectives of the Impact of COVID-19 Lockdown on Food-Related Behaviors: Systematic Review. Foods 2022, 11, 2851. [Google Scholar] [CrossRef]
- Kombanda, K.T.; Margerison, C.; Booth, A.; Worsley, A. The Impact of the COVID-19 Pandemic on Young Australian Adults’ Food Practices. Curr. Dev. Nutr. 2022, 6, nzac009. [Google Scholar] [CrossRef]
- Melamed, O.C.; Selby, P.; Taylor, V.H. Mental Health and Obesity During the COVID-19 Pandemic. Curr. Obes. Rep. 2022, 11, 23–31. [Google Scholar] [CrossRef]
- Samji, H.; Wu, J.; Ladak, A.; Vossen, C.; Stewart, E.; Dove, N.; Long, D.; Snell, G. Review: Mental health impacts of the COVID-19 pandemic on children and youth—A systematic review. Child Adolesc. Ment. Health 2022, 27, 173–189. [Google Scholar] [CrossRef]
- Riazi, N.A.; Battista, K.; Duncan, M.J.; Wade, T.J.; Pickett, W.; Ferro, M.A.; Leatherdale, S.T.; Patte, K.A. Stronger together: Coping behaviours and mental health changes of Canadian adolescents in early phases of the COVID-19 pandemic. BMC Public Health 2023, 23, 319. [Google Scholar] [CrossRef]
- Brady, T.M. Obesity-Related Hypertension in Children. Front. Pediatr. 2017, 5, 197. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jimenez, F.; Almahmeed, W.; Bays, H.; Cuevas, A.; Di Angelantonio, E.; le Roux, C.W.; Sattar, N.; Sun, M.C.; Wittert, G.; Pinto, F.J.; et al. Obesity and cardiovascular disease: Mechanistic insights and management strategies. A joint position paper by the World Heart Federation and World Obesity Federation. Eur. J. Prev. Cardiol. 2022, 29, 2218–2237. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, G. Insulin and insulin resistance. Clin. Biochem. Rev. 2005, 26, 19–39. [Google Scholar] [PubMed]
- Al-Beltagi, M.; Bediwy, A.S.; Saeed, N.K. Insulin-resistance in paediatric age: Its magnitude and implications. World J. Diabetes 2022, 13, 282–307. [Google Scholar] [CrossRef]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Patimah, I.; KhazáAi, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef]
- Kwaifa, I.K.; Bahari, H.; Yong, Y.K.; Noor, S.M. Endothelial Dysfunction in Obesity-Induced Inflammation: Molecular Mechanisms and Clinical Implications. Biomolecules 2020, 10, 291. [Google Scholar] [CrossRef]
- Barton, M.; Baretella, O.; Meyer, M.R. Obesity and risk of vascular disease: Importance of endothelium-dependent vasoconstriction. Br. J. Pharmacol. 2012, 165, 591–602. [Google Scholar] [CrossRef]
- Pecoraro, L.; Zoller, T.; Atkinson, R.L.; Nisi, F.; Antoniazzi, F.; Cavarzere, P.; Piacentini, G.; Pietrobelli, A. Supportive treatment of vascular dysfunction in pediatric subjects with obesity: The OBELIX study. Nutr. Diabetes 2022, 12, 2. [Google Scholar] [CrossRef]
- Ait-Aissa, K.; Nguyen, Q.M.; Gabani, M.; Kassan, A.; Kumar, S.; Choi, S.-K.; Gonzalez, A.A.; Khataei, T.; Sahyoun, A.M.; Chen, C.; et al. MicroRNAs and obesity-induced endothelial dysfunction: Key paradigms in molecular therapy. Cardiovasc. Diabetol. 2020, 19, 136. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Kavey, R.E.W. Dyslipidemia and Pediatric Obesity. Pediatr. Clin. N. Am. 2011, 58, 1363–1373. [Google Scholar] [CrossRef] [PubMed]
- Angi, A.; Chiarelli, F. Obesity and Diabetes: A Sword of Damocles for Future Generations. Biomedicines 2020, 8, 478. [Google Scholar] [CrossRef]
- Leggio, M.; Lombardi, M.; Caldarone, E.; Severi, P.; D’Emidio, S.; Armeni, M.; Bravi, V.; Bendini, M.G.; Mazza, A. The relationship between obesity and hypertension: An updated comprehensive overview on vicious twins. Hypertens. Res. 2017, 40, 947–963. [Google Scholar] [CrossRef] [PubMed]
- Landsberg, L.; Aronne, L.J.; Beilin, L.J.; Burke, V.; Igel, L.I.; Lloyd-Jones, D.; Sowers, J. Obesity-related hypertension: Pathogenesis, cardiovascular risk, and treatment: A position paper of The Obesity Society and the American Society of Hypertension. J. Clin. Hypertens. 2013, 15, 14–33. [Google Scholar] [CrossRef]
- Hall, J.E.; do Carmo, J.M.; da Silva, A.A.; Wang, Z.; Hall, M.E. Obesity-Induced Hypertension: Interaction of neurohumoral and renal mechanisms. Circ. Res. 2015, 116, 991–1006. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef]
- Mahmoud, R.; Kimonis, V.; Butler, M.G. Genetics of Obesity in Humans: A Clinical Review. Int. J. Mol. Sci. 2022, 23, 11005. [Google Scholar] [CrossRef]
- Wardle, J.; Carnell, S.; Haworth, C.M.; Plomin, R. Evidence for a strong genetic influence on childhood adiposity despite the force of the obesogenic environment. Am. J. Clin. Nutr. 2008, 87, 398–404. [Google Scholar] [CrossRef]
- Farooqi, I.S. Genetic and hereditary aspects of childhood obesity. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 359–374. [Google Scholar] [CrossRef]
- Stefan, M.; Nicholls, R.D. What have rare genetic syndromes taught us about the pathophysiology of the common forms of obesity? Curr. Diabetes Rep. 2004, 4, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Loos, R.J.F.; Yeo, G.S.H. The genetics of obesity: From discovery to biology. Nat. Rev. Genet. 2022, 23, 120–133. [Google Scholar] [CrossRef] [PubMed]
- Chami, N.; Preuss, M.; Walker, R.W.; Moscati, A.; Loos, R.J.F. The role of polygenic susceptibility to obesity among carriers of pathogenic mutations in MC4R in the UK Biobank population. PLoS Med. 2020, 17, e1003196. [Google Scholar] [CrossRef] [PubMed]
- Ranadive, S.A.; Vaisse, C. Lessons from Extreme Human Obesity: Monogenic Disorders. Endocrinol. Metab. Clin. N. Am. 2008, 37, 733–751. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.T.; Yasin, M.; Kassem, A. Leptin in pediatrics: A hormone from adipocyte that wheels several functions in children. Indian J. Endocrinol. Metab. 2012, 16, S577–S587. [Google Scholar] [CrossRef]
- Friedman, J.M.; Halaas, J.L. Leptin and the regulation of body weight in mammals. Nature 1998, 395, 763–770. [Google Scholar] [CrossRef]
- Franks, P.W.; Brage, S.; Luan, J.; Ekelund, U.; Rahman, M.; Farooqi, I.S.; Halsall, I.; O’Rahilly, S.; Wareham, N.J. Leptin Predicts a Worsening of the Features of the Metabolic Syndrome Independently of Obesity. Obes. Res. 2005, 13, 1476–1484. [Google Scholar] [CrossRef]
- Singh, R.K.; Kumar, P.; Mahalingam, K. Molecular genetics of human obesity: A comprehensive review. C. R. Biol. 2017, 340, 87–108. [Google Scholar] [CrossRef]
- Farooqi, I.S.; Wangensteen, T.; Collins, S.; Kimber, W.; Matarese, G.; Keogh, J.M.; Lank, E.; Bottomley, B.; Lopez-Fernandez, J.; Ferraz-Amaro, I.; et al. Clinical and Molecular Genetic Spectrum of Congenital Deficiency of the Leptin Receptor. N. Engl. J. Med. 2007, 356, 237–247. [Google Scholar] [CrossRef]
- Mutch, D.M.; Clément, K. Unraveling the Genetics of Human Obesity. PLoS Genet. 2006, 2, e188. [Google Scholar] [CrossRef]
- Crocker, M.K.; Yanovski, J.A. Pediatric Obesity: Etiology and Treatment. Endocrinol. Metab. Clin. N. Am. 2009, 38, 525–548. [Google Scholar] [CrossRef] [PubMed]
- Huvenne, H.; Dubern, B.; Clément, K.; Poitou, C. Rare Genetic Forms of Obesity: Clinical Approach and Current Treatments in 2016. Obes. Facts 2016, 9, 158–173. [Google Scholar] [CrossRef] [PubMed]
- Hetherington, M.M.; Cecil, J.E. Gene-Environment Interactions in Obesity. Forum Nutr. 2009, 63, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Reddon, H.; Guéant, J.-L.; Meyre, D. The importance of gene–environment interactions in human obesity. Clin. Sci. 2016, 130, 1571–1597. [Google Scholar] [CrossRef]
- Castillo, J.J.; Orlando, R.A.; Garver, W.S. Gene-nutrient interactions and susceptibility to human obesity. Genes Nutr. 2017, 12, 29. [Google Scholar] [CrossRef]
- Heianza, Y.; Qi, L. Gene-Diet Interaction and Precision Nutrition in Obesity. Int. J. Mol. Sci. 2017, 18, 787. [Google Scholar] [CrossRef]
- Goodarzi, M.O. Genetics of obesity: What genetic association studies have taught us about the biology of obesity and its complications. Lancet Diabetes Endocrinol. 2018, 6, 223–236. [Google Scholar] [CrossRef]
- Bouchard, L.; Drapeau, V.; Provencher, V.; Lemieux, S.; Chagnon, Y.; Rice, T.; Rao, D.; Vohl, M.-C.; Tremblay, A.; Bouchard, C.; et al. Neuromedin β: A strong candidate gene linking eating behaviors and susceptibility to obesity. Am. J. Clin. Nutr. 2004, 80, 1478–1486. [Google Scholar] [CrossRef]
- Grimm, E.R.; Steinle, N.I. Genetics of eating behavior: Established and emerging concepts. Nutr. Rev. 2011, 69, 52–60. [Google Scholar] [CrossRef]
- van der Klaauw, A.A.; Farooqi, I.S. The Hunger Genes: Pathways to Obesity. Cell 2015, 161, 119–132. [Google Scholar] [CrossRef]
- Martinez, J.A. Body-weight regulation: Causes of obesity. Proc. Nutr. Soc. 2000, 59, 337–345. [Google Scholar] [CrossRef]
- Rask-Andersen, M.; Karlsson, T.; Ek, W.E.; Johansson, Å. Gene-environment interaction study for BMI reveals interactions between genetic factors and physical activity, alcohol consumption and socioeconomic status. PLoS Genet. 2017, 13, e1006977. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Li, P.; Yang, X.; Li, W.; Qiu, X.; Zhu, S. From genetics and epigenetics to the future of precision treatment for obesity. Gastroenterol. Rep. 2017, 5, 266–270. [Google Scholar] [CrossRef]
- Bianco-Miotto, T.; Craig, J.M.; Gasser, Y.P.; Van Dijk, S.J.; Ozanne, S.E. Epigenetics and DOHaD: From basics to birth and beyond. J. Dev. Orig. Health Dis. 2017, 8, 513–519. [Google Scholar] [CrossRef]
- van Dijk, S.J.; Molloy, P.L.; Varinli, H.; Morrison, J.L.; Muhlhausler, B.S.; Buckley, M.; Clark, S.J.; McMillen, I.C.; Noakes, M.; Samaras, K.; et al. Epigenetics and human obesity. Int. J. Obes. 2015, 39, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Montalvo-Ortiz, J.L.; Holbrook, H.; O’Loughlin, K.; Orr, C.; Kearney, C.; Yang, B.-Z.; Wang, T.; Zhao, H.; Althoff, R.; et al. Adverse Childhood Experiences, Epigenetic Measures, and Obesity in Youth. J. Pediatr. 2018, 202, 150–156.e3. [Google Scholar] [CrossRef] [PubMed]
- Li, Y. Epigenetic Mechanisms Link Maternal Diets and Gut Microbiome to Obesity in the Offspring. Front. Genet. 2018, 9, 342. [Google Scholar] [CrossRef]
- Gardner, R.; Feely, A.; Layte, R.; Williams, J.; McGavock, J. Adverse childhood experiences are associated with an increased risk of obesity in early adolescence: A population-based prospective cohort study. Pediatr. Res. 2019, 86, 522–528. [Google Scholar] [CrossRef]
- Cheon, B.K.; Hong, Y.-Y. Mere experience of low subjective socioeconomic status stimulates appetite food intake. Proc. Natl. Acad. Sci. USA 2017, 114, 72–77. [Google Scholar] [CrossRef]
- Alegría-Torres, J.A.; Baccarelli, A.; Bollati, V.; Huang, Q.; Vucic, E.A.; Brown, C.J.; Lam, W.L.; Lewis, K.A.; Tollefsbol, T.O.; Bartosch, C.; et al. Epigenetics lifestyle. Epigenomics 2011, 3, 267–277. [Google Scholar] [CrossRef]
- Tiwari, A.; Balasundaram, P. Public Health Considerations Regarding Obesity. In Treasure Island; StatPearls Publishing: St. Petersburg, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK572122/ (accessed on 15 June 2023).
- Karnik, S.; Kanekar, A. Childhood Obesity: A Global Public Health Crisis. Int. J. Prev. Med. 2015, 3, 1–7. [Google Scholar] [CrossRef]
- Scapaticci, S.; Neri, C.R.; Marseglia, G.L.; Staiano, A.; Chiarelli, F.; Verduci, E. The impact of the COVID-19 pandemic on lifestyle behaviors in children and adolescents: An international overview. Ital. J. Pediatr. 2022, 48, 22. [Google Scholar] [CrossRef] [PubMed]
- Vine, M.; Hargreaves, M.B.; Briefel, R.R.; Orfield, C. Expanding the Role of Primary Care in the Prevention and Treatment of Childhood Obesity: A Review of Clinic- and Community-Based Recommendations and Interventions. J. Obes. 2013, 2013, 172035. [Google Scholar] [CrossRef] [PubMed]
- Tulchinsky, T.H.; Varavikova, E.A. Expanding the Concept of Public Health. In The New Public Health; Academic Press: Cambridge, MA, USA, 2014; pp. 43–90. [Google Scholar] [CrossRef]
- Pulimeno, M.; Piscitelli, P.; Colazzo, S.; Colao, A.; Miani, A. School as ideal setting to promote health and wellbeing among young people. Health Promot. Perspect. 2020, 10, 316–324. [Google Scholar] [CrossRef]
- Institute of Medicine (US) and National Research Council (US) Committee on Childhood Obesity Prevention Actions for Local Governments; Parker, L.; Burns, A.C.; Sanchez, E. (Eds.) Local Government Actions to Prevent Childhood Obesity; National Academies Press (US): Washington, DC, USA, 2009; p. 2. Available online: https://www.ncbi.nlm.nih.gov/books/NBK219685/ (accessed on 15 June 2023).
- Olstad, D.L.; Raine, K.D.; McCargar, L.J. Adopting and implementing nutrition guidelines in recreational facilities: Public and private sector roles. A multiple case study. BMC Public Health 2012, 12, 376. [Google Scholar] [CrossRef]
- Galuska, D.A.; Gunn, J.P.; O’connor, A.E.; Petersen, R. Addressing Childhood Obesity for Type 2 Diabetes Prevention: Challenges and Opportunities. Diabetes Spectr. 2018, 31, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Fruh, S.P.; Williams, S.P.; Hayes, K.; Hauff, C.; Hudson, G.M.P.; Sittig, S.; Graves, R.J.P.; Hall, H.P.; Barinas, J.M.S. A practical approach to obesity prevention: Healthy home habits. J. Am. Assoc. Nurse Pract. 2021, 33, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Day, R.E.; Bridge, G.; Austin, K.; Ensaff, H.; Christian, M.S. Parents’ awareness and perceptions of the Change4Life 100 cal snack campaign, and perceived impact on snack consumption by children under 11 years. BMC Public Health 2022, 22, 1012. [Google Scholar] [CrossRef]
- Dabravolskaj, J.; Montemurro, G.; Ekwaru, J.P.; Wu, X.Y.; Storey, K.; Campbell, S.; Veugelers, P.J.; Ohinmaa, A. Effectiveness of school-based health promotion interventions prioritized by stakeholders from health and education sectors: A systematic review and meta-analysis. Prev. Med. Rep. 2020, 19, 101138. [Google Scholar] [CrossRef]
- Romanelli, R.; Cecchi, N.; Carbone, M.G.; Dinardo, M.; Gaudino, G.; del Giudice, E.M.; Umano, G.R. Pediatric obesity: Prevention is better than care. Ital. J. Pediatr. 2020, 46, 103. [Google Scholar] [CrossRef]
- Gortmaker, S.L.; Wang, Y.C.; Long, M.W.; Giles, C.M.; Ward, Z.J.; Barrett, J.L.; Kenney, E.L.; Sonneville, K.R.; Afzal, A.S.; Resch, S.C.; et al. Three Interventions That Reduce Childhood Obesity Are Projected To Save More Than They Cost To Implement. Health Aff. 2015, 34, 1932–1939. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.A.; Raine, K.D. Insights on the Influence of Sugar Taxes on Obesity Prevention Efforts. Curr. Nutr. Rep. 2019, 8, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Young, J.; Conway, E.M.; Rother, K.I.; Sylvetsky, A.C. Low-calorie sweetener use, weight, and metabolic health among children: A mini-review. Pediatr. Obes. 2019, 14, e12521. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasile, C.M.; Padovani, P.; Rujinski, S.D.; Nicolosu, D.; Toma, C.; Turcu, A.A.; Cioboata, R. The Increase in Childhood Obesity and Its Association with Hypertension during Pandemics. J. Clin. Med. 2023, 12, 5909. https://doi.org/10.3390/jcm12185909
Vasile CM, Padovani P, Rujinski SD, Nicolosu D, Toma C, Turcu AA, Cioboata R. The Increase in Childhood Obesity and Its Association with Hypertension during Pandemics. Journal of Clinical Medicine. 2023; 12(18):5909. https://doi.org/10.3390/jcm12185909
Chicago/Turabian StyleVasile, Corina Maria, Paul Padovani, Stefan Dumitrache Rujinski, Dragos Nicolosu, Claudia Toma, Adina Andreea Turcu, and Ramona Cioboata. 2023. "The Increase in Childhood Obesity and Its Association with Hypertension during Pandemics" Journal of Clinical Medicine 12, no. 18: 5909. https://doi.org/10.3390/jcm12185909