

Predictors of 30-Day Postoperative Outcome after Elective Endovascular Abdominal Aortic Aneurysm Repair: A Tertiary Referral Center Experience
 , , , , , ,
, , , , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Postoperative Surveillance
2.4. Definitions
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Primary Outcome—Overall Postoperative Morbidity and Mortality
3.2. Secondary Outcome
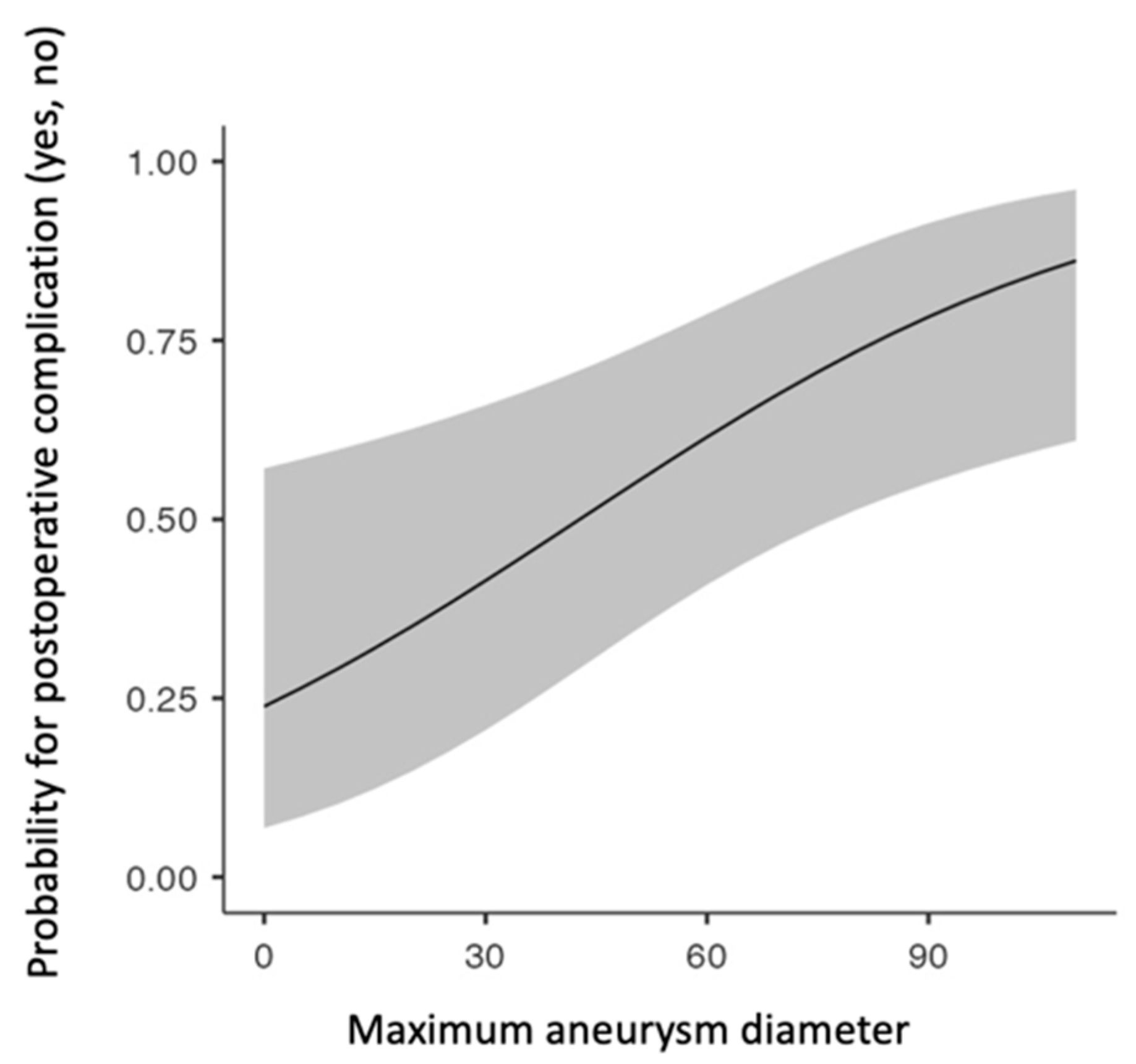
3.2.1. Overall Complications
3.2.2. Major Complications—MACEs
3.2.3. Major Complications—AKI
3.2.4. Minor Complications
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; Van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [PubMed]
- Spanos, K.; Nana, P.; Behrendt, C.-A.; Kouvelos, G.; Panuccio, G.; Heidemann, F.; Matsagkas, M.; Debus, S.; Giannoukas, A.; Kölbel, T. Management of Abdominal Aortic Aneurysm Disease: Similarities and Differences Among Cardiovascular Guidelines and NICE Guidance. J. Endovasc. Ther. 2020, 27, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Stather, P.W.; Sidloff, D.; Dattani, N.; Choke, E.; Bown, M.J.; Sayers, R.D. Systematic Review and Meta-Analysis of the Early and Late Outcomes of Open and Endovascular Repair of Abdominal Aortic Aneurysm. Br. J. Surg. 2013, 100, 863–872. [Google Scholar] [CrossRef]
- Landry, G.J.; Liem, T.K.; Abraham, C.Z.; Jung, E.; Moneta, G.L. Predictors of Perioperative Morbidity and Mortality in Open Abdominal Aortic Aneurysm Repair. Am. J. Surg. 2019, 217, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Katsargyris, A.; Lenhardt Michael Florian, C.; Marques De Marino, P.; Botos, B.; Verhoeven, E.L. Reasons for and Outcomes of Open Abdominal Aortic Repair in the Endovascular Era. Ann. Vasc. Surg. 2021, 73, 417–422. [Google Scholar] [CrossRef]
- Alberga, A.J.; Karthaus, E.G.; Van Zwet, E.W.; De Bruin, J.L.; Van Herwaarden, J.A.; Wever, J.J.; Verhagen, H.J.M.; Van Den Akker, P.J.; Akkersdijk, G.J.; Akkersdijk, G.P.; et al. Outcomes in Octogenarians and the Effect of Comorbidities After Intact Abdominal Aortic Aneurysm Repair in the Netherlands: A Nationwide Cohort Study. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 920–928. [Google Scholar] [CrossRef]
- Alberga, A.J.; Karthaus, E.G.; Wilschut, J.A.; De Bruin, J.L.; Akkersdijk, G.P.; Geelkerken, R.H.; Hamming, J.F.; Wever, J.J.; Verhagen, H.J.M.; Van Den Akker, P.J.; et al. Treatment Outcome Trends for Non-Ruptured Abdominal Aortic Aneurysms: A Nationwide Prospective Cohort Study. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 275–283. [Google Scholar] [CrossRef]
- Nejim, B.; Zarkowsky, D.; Hicks, C.W.; Locham, S.; Dakour Aridi, H.; Malas, M.B. Predictors of In-Hospital Adverse Events after Endovascular Aortic Aneurysm Repair. J. Vasc. Surg. 2019, 70, 80–91. [Google Scholar] [CrossRef]
- Noori, V.J.; Healey, C.T.; Eldrup-Jorgensen, J.; Blazick, E.; Hawkins, R.E.; Bloch, P.H.S.; Nolan, B.W. Comparison of Major Adverse Event Rates after Elective Endovascular Aneurysm Repair in New England Using a Novel Measure of Complication Severity. J. Vasc. Surg. 2019, 70, 74–79. [Google Scholar] [CrossRef]
- Castiglione, D.; Easwaran, A.; Prashar, A.; La Grutta, L.; Krokidis, M.; Shaida, N. Assessment of EVAR Complications Using CIRSE Complication Classification System in the UK Tertiary Referral Centre: A ∼6-Year Retrospective Analysis (2014–2019). Cardiovasc. Int. Radiol. 2021, 44, 1174–1183. [Google Scholar] [CrossRef]
- Moll, F.L.; Powell, J.T.; Fraedrich, G.; Verzini, F.; Haulon, S.; Waltham, M.; Van Herwaarden, J.A.; Holt, P.J.E.; Van Keulen, J.W.; Rantner, B.; et al. Management of Abdominal Aortic Aneurysms Clinical Practice Guidelines of the European Society for Vascular Surgery. Eur. J. Vasc. Endovasc. Surg. 2011, 41, S1–S58. [Google Scholar] [CrossRef] [PubMed]
- Ntalouka, M.P.; Nana, P.; Kouvelos, G.N.; Stamoulis, K.; Spanos, K.; Giannoukas, A.; Matsagkas, M.; Arnaoutoglou, E. Association of Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratio with Adverse Events in Endovascular Repair for Abdominal Aortic Aneurysm. J. Clin. Med. 2021, 10, 1083. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; De Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- MD+CALC. Available online: https://www.mdcalc.com/creatinine-clearance-cockcroft-gault-equation (accessed on 1 March 2016).
- Aboyans, V.; Ricco, J.-B.; Bartelink, M.-L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in Collaboration with the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef] [PubMed]
- Arnaoutoglou, E.; Kouvelos, G.; Papa, N.; Kallinteri, A.; Milionis, H.; Koulouras, V.; Matsagkas, M. Prospective Evaluation of Post-Implantation Inflammatory Response After EVAR for AAA: Influence on Patients’ 30 Day Outcome. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 175–183. [Google Scholar] [CrossRef]
- Walther, C.P.; Podoll, A.S.; Finkel, K.W. Summary of Clinical Practice Guidelines for Acute Kidney Injury. Hosp. Pract. 2014, 42, 7–14. [Google Scholar] [CrossRef]
- Hooton, T.M.; Bradley, S.F.; Cardenas, D.D.; Colgan, R.; Geerlings, S.E.; Rice, J.C.; Saint, S.; Schaeffer, A.J.; Tambayh, P.A.; Tenke, P.; et al. Diagnosis, Prevention, and Treatment of Catheter-Associated Urinary Tract Infection in Adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 625–663. [Google Scholar] [CrossRef]
- Aldecoa, C.; Bettelli, G.; Bilotta, F.; Sanders, R.D.; Audisio, R.; Borozdina, A.; Cherubini, A.; Jones, C.; Kehlet, H.; MacLullich, A.; et al. European Society of Anaesthesiology Evidence-Based and Consensus-Based Guideline on Postoperative Delirium. Eur. J. Anaesthesiol. 2017, 34, 192–214. [Google Scholar] [CrossRef]
- Powell, J.T.; Sweeting, M.J.; Ulug, P.; Blankensteijn, J.D.; Lederle, F.A.; Becquemin, J.-P.; Greenhalgh, R.M.; Greenhalgh, R.M.; Beard, J.D.; Buxton, M.J.; et al. Meta-Analysis of Individual-Patient Data from EVAR-1, DREAM, OVER and ACE Trials Comparing Outcomes of Endovascular or Open Repair for Abdominal Aortic Aneurysm over 5 Years. Br. J. Surg. 2017, 104, 166–178. [Google Scholar] [CrossRef]
- Donas, K.P.; Torsello, G. Complications and Reinterventions after EVAR: Are They Decreasing in Incidence? J. Cardiovasc. Surg. 2011, 52, 189–192. [Google Scholar]
- Qrareya, M.; Zuhaili, B. Management of Postoperative Complications Following Endovascular Aortic Aneurysm Repair. Surg. Clin. N. Am. 2021, 101, 785–798. [Google Scholar] [CrossRef]
- Peterson, L.; Schweitzer, G.; Simone, A.; Zielke, T.; DeJong, M.; Penton, A.; Blecha, M. The Effect of Smoking Status on Perioperative Morbidity and Mortality after Open and Endovascular Abdominal Aortic Aneurysm Repair. Ann. Vasc. Surg. 2023, 88, 373–384. [Google Scholar] [CrossRef]
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Mastracci, T.M.; Mell, M.; Murad, M.H.; Nguyen, L.L.; et al. The Society for Vascular Surgery Practice Guidelines on the Care of Patients with an Abdominal Aortic Aneurysm. J. Vasc. Surg. 2018, 67, 2–77.e2. [Google Scholar] [CrossRef] [PubMed]
- Ramos, C.; Pujari, A.; Rajani, R.R.; Escobar, G.A.; Rubin, B.G.; Jordan, W.D.; Benarroch-Gampel, J. Perioperative Outcomes for Abdominal Aortic Aneurysm Repair Based on Aneurysm Diameter. Vasc. Endovascular Surg. 2020, 54, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Mastracci, T.M.; Greenberg, R.K.; Hernandez, A.V.; Morales, C. Defining High Risk in Endovascular Aneurysm Repair. J. Vasc. Surg. 2010, 51, 1088–1095.e1. [Google Scholar] [CrossRef]
- Kim, S.; Jeon-Slaughter, H.; Chen, X.; Ramanan, B.; Kirkwood, M.L.; Timaran, C.H.; Modrall, J.G.; Tsai, S. Effect of Abdominal Aortic Aneurysm Size on Mid-Term Mortality After Endovascular Repair. J. Surg. Res. 2021, 267, 443–451. [Google Scholar] [CrossRef]
- De Guerre, L.E.V.M.; Dansey, K.; Li, C.; Lu, J.; Patel, P.B.; Van Herwaarden, J.A.; Jones, D.W.; Goodney, P.P.; Schermerhorn, M.L. Late Outcomes after Endovascular and Open Repair of Large Abdominal Aortic Aneurysms. J. Vasc. Surg. 2021, 74, 1152–1160. [Google Scholar] [CrossRef]
- Diender, E.; Vermeulen, J.J.M.; Pisters, R.; Van Schaik, P.M.; Reijnen, M.M.P.J.; Holewijn, S. Major Adverse Cardiac Events after Elective Infrarenal Endovascular Aortic Aneurysm Repair. J. Vasc. Surg. 2022, 76, 1527–1536.e3. [Google Scholar] [CrossRef]
- Aday, A.W.; Matsushita, K. Epidemiology of Peripheral Artery Disease and Polyvascular Disease. Circ. Res. 2021, 128, 1818–1832. [Google Scholar] [CrossRef] [PubMed]
- Poredos, P.; Poredos, P. Peripheral Arterial Occlusive Disease and Perioperative Risk. Int. Angiol. 2018, 37, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Poredoš, P. Comment on Tsialtas et al., p. 443 Peripheral Arterial Occlusive Disease Increases the Risk of Perioperative Complications. Vasa 2014, 43, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Sirignano, P.; Speziale, F.; Capoccia, L.; Menna, D.; Mansour, W.; Montelione, N.; Setacci, F.; Galzerano, G.; Setacci, C. Iliac and Femoro-Popliteal Arteries Morphological CTA Features as Determinants of Outcome after Standard EVAR Procedures. J. Cardiovasc. Surg. 2019, 60, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Paraskevas, K.I.; Nordon, I.M.; Baxter, S.J.; Shearman, C.P.; Phillips, M.J. Abdominal Aortic Aneurysms, Peripheral Arterial Disease, and Carotid Artery Stenosis: Different Sides of the Same Coin? Angiology 2016, 67, 307–308. [Google Scholar] [CrossRef] [PubMed]
- Liang, P.; O’Donnell, T.F.X.; Swerdlow, N.J.; Li, C.; Lee, A.; Wyers, M.C.; Hamdan, A.D.; Schermerhorn, M.L. Preoperative Risk Score for Access Site Failure in Ultrasound-Guided Percutaneous Aortic Procedures. J. Vasc. Surg. 2019, 70, 1254–1262.e1. [Google Scholar] [CrossRef] [PubMed]
- Novak, Z.; Zaky, A.; Spangler, E.L.; McFarland, G.E.; Tolwani, A.; Beck, A.W. Incidence and Predictors of Early and Delayed Renal Function Decline after Aortic Aneurysm Repair in the Vascular Quality Initiative Database. J. Vasc. Surg. 2021, 74, 1537–1547. [Google Scholar] [CrossRef]
- Octeau, D.; Faries, C.; Barnes, H.; Nakazawa, K.R.; Rao, A.J.; Ting, W.; Marin, M.L.; Vouyouka, A.G.; Faries, P.L.; Tadros, R.O. Neutrophil-to-Lymphocyte Ratio Associated with Adverse Events After Endovascular Aneurysm Repair (EVAR). Ann. Vasc. Surg. 2021, 75, 45–54. [Google Scholar] [CrossRef]
- King, A.H.; Schmaier, A.H.; Harth, K.C.; Kumins, N.H.; Wong, V.L.; Zidar, D.A.; Kashyap, V.S.; Cho, J.S. Elevated Neutrophil-Lymphocyte Ratio Predicts Mortality Following Elective Endovascular Aneurysm Repair. J. Vasc. Surg. 2020, 72, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Caradu, C.; Coatsaliou, Q.; Colacchio, E.C.; Ducasse, E.; Lareyre, F.; Raffort, J. Incidence of Contrast-Induced Nephropathy and Post-Operative Outcomes in Patients Undergoing Chimney Endovascular Aortic Aneurysm Repair. Angiology 2022, 73, 852–862. [Google Scholar] [CrossRef]
- Martinelli, O.; Di Girolamo, A.; Irace, L.; Baratta, F.; Gossetti, B.; Gattuso, R. Post-Implantation Syndrome: The Impact of Different Devices for Endovascular Abdominal Aortic Aneurysm Repair and Related Etiopathogenetic Implications. Int. Angiol. 2020, 39, 398–404. [Google Scholar] [CrossRef]
- Lee, J.H.; Choi, J.-H.; Kim, E.-J. Volume of Mural Thrombus Plays a Role in the Elevation of Inflammatory Markers after Endovascular Aortic Repair. J. Cardiothorac. Surg. 2018, 13, 27. [Google Scholar] [CrossRef] [PubMed]
- Oddi, F.M.; Vacca, F.; Ciattaglia, R.; Fresilli, M.; Fazzini, S.; Ippoliti, A. Polyester Stent Graft Devices and Higher Risk of Post-Implantation Syndrome after EVAR: Single-Center Analysis of 367 Patients. Ann. Vasc. Surg. 2021, 75, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Bradley, N.A.; Roxburgh, C.; Khan, F.; Guthrie, G. Postimplantation Syndrome in Endovascular Aortic Aneurysm Repair—A Systematic Review. Vasa 2021, 50, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Siasos, G.; Tsigkou, V.; Kokkou, E.; Oikonomou, E.; Vavuranakis, M.; Vlachopoulos, C.; Verveniotis, A.; Limperi, M.; Genimata, V.; Papavassiliou, A.; et al. Smoking and Atherosclerosis: Mechanisms of Disease and New Therapeutic Approaches. Curr. Med. Chem. 2014, 21, 3936–3948. [Google Scholar] [CrossRef]
- Catanese, V.; Sangiorgi, G.; Sotgiu, G.; Saderi, L.; Settembrini, A.; Donelli, C.; Martelli, E. Clinical and anatomical variables associated in the literature to limb graft occlusion after endovascular aneurysm repair compared to the experience of a tertiary referral center. Minerva Chir. 2020, 75, 51–59. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (A) | ||
|---|---|---|
| Baseline Characteristics | Mean Value | Standard Deviation (SD) |
| Age | 72.3 | 7.21 |
| Preoperative aneurysm diameter (milimeter) | 59.2 | 12.7 |
| Preoperative WBC | 8419.3 | 7296.7 |
| Preoperative neutrophils | 3740.9 | 5480.8 |
| Preoperative lymphocytes | 1335.4 | 1201.7 |
| Preoperative platelets | 219.4 | 68.8 |
| Preoperative platelet/lymphocyte ratio | 128.0 | 68.9 |
| Preoperative neutrophils/lymphocytes ratio | 3.3 | 2.6 |
| Preoperative hemoglobin | 13.5 | 2.1 |
| Preoperative creatinine | 1.2 | 0.7 |
| (B) | ||
| Baseline Characteristics | Patients (N) | (%) |
| Males | 316 | 98.1 |
| Smoking | 203 | 70.3 |
| Current smoker | 106 | 34.1 |
| Past smoker | 97 | 31.2 |
| Never smoked | 86 | 26.7 |
| Not applicable | 33 | 10.2 |
| Hypertension | 249 | 86.2 |
| Coronary artery disease | 138 | 47.8 |
| Cerebrovascular events | 24 | 8.3 |
| Peripheral arterial disease | 10 | 3.5 |
| Chronic obstructive pulmonary disease | 145 | 50.2 |
| Dyslipidemia | 228 | 78.9 |
| Diabetes mellitus | ||
| Type II | 49 | 17.0 |
| Type I | 0 | 0 |
| Chronic kindey disease | 22 | 7.6 |
| Venous thromboembolism | 3 | 1.0 |
| Malignancy | 18 | 6.2 |
| Postoperative Complications | N | % |
|---|---|---|
| (A) | ||
| Overall | 121 | 37.5 |
| Major | 18 | 5.6 |
| Minor | 103 | 31.9 |
| (B) | ||
| Major | 18 | 5.6 |
| MACEs * | 11 | 3.4 |
| AKI ** | 5 | 1.6 |
| Death | 2 | 0.6 |
| Minor | 103 | 31.9 |
| PIS *** | 77 | 23.9 |
| POD **** | 11 | 3.4 |
| UTI ***** | 11 | 3.4 |
| Technical graft failure | 4 | 1.2 |
| Morbidity | Parameter | Comparator | OR (95% CI) | p |
|---|---|---|---|---|
| Complications (n = 121) | Maximal aneurysm diameter | (-) | 1.28 (1.01–1.05) | 0.01 |
| PAD * (Reference level: No) | Yes | 4.65 (0.87–24.7) | 0.072 | |
| Smoking status (Reference level: Never) | Current | 0.84 (0.46–1.53) | 0.575 | |
| Past smoker | 0.38 (0.19–0.71) | 0.003 | ||
| MACEs ** | Venous thromboembolism | 0 (0-inf) | 1.000 | |
| PAD | Yes | 13.94 (2.4–81.16) | 0.003 | |
| COPD *** | Yes | 4.06 (0.81–20.39) | 0.086 | |
| AKI **** | Age | (-) | 0.91 (0.81–1.02) | 0.097 |
| Preoperative lymphocyte levels | (-) | 0.99 (0.99–1.00) | 0.136 | |
| Preoperative NLR ***** | (-) | 1.2 (1.01–1.43) | 0.036 | |
| PIS ****** | Preoperative lymphocyte value | (-) | 1.0 (1.0–1.0) | 0.084 |
| Smoking status (Reference level: Never) | Current | 1.24 (0.66–12.26) | 0.519 | |
| Past smoker | 0.36 (0.17–0.76) | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ntalouka, M.P.; Nana, P.; Brotis, A.; Chatzis, A.; Mermiri, M.; Stamoulis, K.; Bareka, M.; Giannoukas, A.; Matsagkas, M.; Arnaoutoglou, E. Predictors of 30-Day Postoperative Outcome after Elective Endovascular Abdominal Aortic Aneurysm Repair: A Tertiary Referral Center Experience. J. Clin. Med. 2023, 12, 6004. https://doi.org/10.3390/jcm12186004
Ntalouka MP, Nana P, Brotis A, Chatzis A, Mermiri M, Stamoulis K, Bareka M, Giannoukas A, Matsagkas M, Arnaoutoglou E. Predictors of 30-Day Postoperative Outcome after Elective Endovascular Abdominal Aortic Aneurysm Repair: A Tertiary Referral Center Experience. Journal of Clinical Medicine. 2023; 12(18):6004. https://doi.org/10.3390/jcm12186004
Chicago/Turabian StyleNtalouka, Maria P., Petroula Nana, Alexandros Brotis, Athanasios Chatzis, Maria Mermiri, Konstantinos Stamoulis, Metaxia Bareka, Athanasios Giannoukas, Miltiadis Matsagkas, and Eleni Arnaoutoglou. 2023. "Predictors of 30-Day Postoperative Outcome after Elective Endovascular Abdominal Aortic Aneurysm Repair: A Tertiary Referral Center Experience" Journal of Clinical Medicine 12, no. 18: 6004. https://doi.org/10.3390/jcm12186004