
Serum Fibrinogen and Renal Dysfunction as Important Predictors of Left Atrial Thrombosis in Patients with Atrial Fibrillation
 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Data Collection
2.3. Transesophageal Echocardiography
2.4. Genetic Analysis
2.5. Study Endpoint
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Thromboembolic Risk
3.3. Propensity Score Matching (PSM)
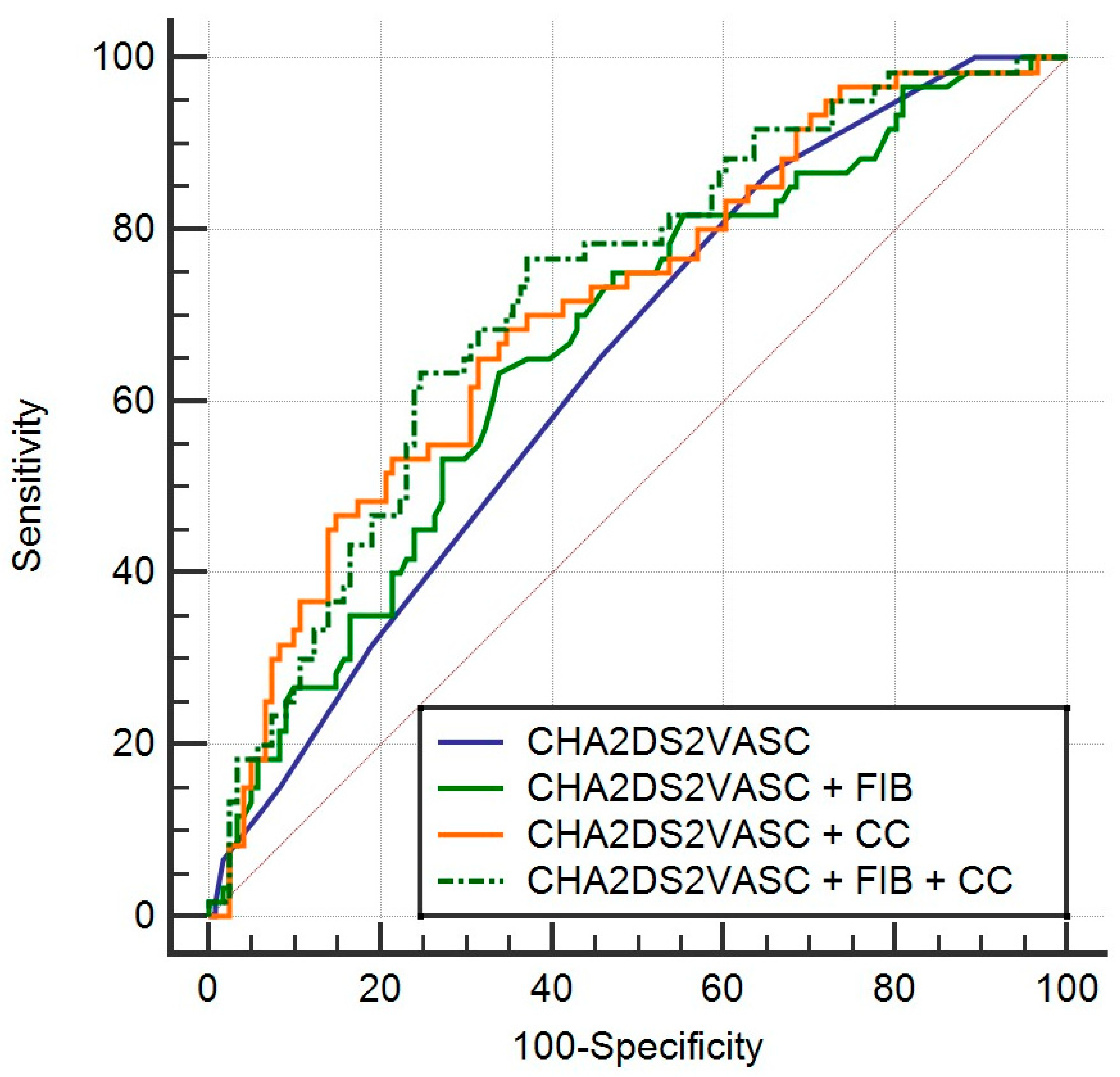
3.4. Logistic Regression Models (LRM) with ROC Curves
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diamandopoulos, A.; Goudas, P.; Arvanitis, A. Comparison of estimated creatinine clearance among five formulae (Cockroft-Gault, Jelliffe, Sanaka, simplified 4-variable MDRD and DAF) and the 24hours-urine-collection creatinine clearance. Hippokratia 2010, 14, 98–104. [Google Scholar] [PubMed]
- Scicchitano, P.; Iacoviello, M.; Passantino, A.; Guida, P.; De Palo, M.; Piscopo, A.; Gesualdo, M.; Caldarola, P.; Massari, F. The Prognostic Impact of Estimated Creatinine Clearance by Bioelectrical Impedance Analysis in Heart Failure: Comparison of Different eGFR Formulas. Biomedicines 2021, 9, 1307. [Google Scholar] [CrossRef] [PubMed]
- Meus, R.; Son, M.; Sobczyk, D.; Undas, A. Prothrombotic State in Patients with a Left Atrial Appendage Thrombus of Unknown Origin and Cerebrovascular Events. Stroke 2016, 47, 1872–1878. [Google Scholar] [CrossRef] [PubMed]
- Martiskainen, M.; Oksala, N.; Pohjasvaara, T.; Kaste, M.; Oksala, A.; Karhunen, P.J.; Erkinjuntti, T. Βeta-fibrinogen gene promoter A−455 allele associated with poor longterm survival among 55–71 years old Caucasian women in Finnish stroke cohort. BMC Neurol. 2014, 14, 137. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Wang, J.; Li, Y.; Wu, J.; Qiao, S.; Xu, S.; Huang, J.; Chen, L. The β-fibrinogen gene455G/A polymorphism associated with cardioembolic stroke in atrial fibrillation with low CHA2DS2-VaSc score. Sci. Rep. 2017, 7, 17517. [Google Scholar] [CrossRef]
- Chen, X.-C.; Xu, M.-T.; Zhou, W.; Han, C.-L.; Chen, W.-Q. A meta-analysis of beta-fibrinogen gene-455G/A polymorphism and plasma fibrinogen level in Chinese cerebral infarction patients. Biomed. Environ. Sci. 2007, 20, 366–372. [Google Scholar]
- Gu, L.; Wu, G.; Su, L.; Yan, Y.; Long, J.; Tan, J.; Liang, B.; Guo, X.; Huang, G. Genetic polymorphism of β-fibrinogen gene-455G/A can contribute to the risk of ischemic stroke. Neurol. Sci. 2013, 35, 151–161. [Google Scholar] [CrossRef]
- Xu, X.; Li, J.; Sheng, W.; Liu, L. Meta-analysis of genetic studies from journals published in China of ischemic stroke in the Han Chinese population. Cerebrovasc. Dis. 2008, 26, 48–62. [Google Scholar] [CrossRef]
- Luo, H.; Li, X.; Jiang, A.; Zhang, B.; Bi, P.; Dong, Y.; Guo, Y. Associations of β-Fibrinogen Polymorphisms with the Risk of Ischemic Stroke: A Meta-analysis. J. Stroke Cerebrovasc. Dis. 2019, 28, 243–250. [Google Scholar] [CrossRef]
- Albert, M.A.; Pare, G.; Morris, A.; Rose, L.; Buring, J.; Ridker, P.M.; Zee, R.Y. Candidate genetic variants in the fibrinogen, methylenetetrahydrofolate reductase, and intercellular adhesion molecule-1 genes and plasma levels of fibrinogen, homocysteine, and intercellular adhesion molecule-1 among various race/ethnic groups: Data from the Women’s Genome Health Study. Am. Heart J. 2009, 157, 777–783.e1. [Google Scholar]
- Zito, F.; Di Castelnuovo, A.; D’Orazio, A.; Negrini, R.; De Lucia, D.; Donati, M.B.; Iacoviello, L. Helicobacter pylori infection and the risk of myocardial infarction: Role of fibrinogen and its genetic control. Thromb. Haemost. 1999, 82, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Komitopoulou, A.; Platokouki, H.; Kapsimali, Z.; Pergantou, H.; Adamtziki, E.; Aronis, S. Mutations and polymorphisms in genes affecting hemostasis proteins and homocysteine metabolism in children with arterial ischemic stroke. Cerebrovasc. Dis. 2006, 22, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Tybjaerg-Hansen, A.; Agerholm-Larsen, B.; Humphries, S.E.; Abildgaard, S.; Schnohr, P.; Nordestgaard, B.G. A common mutation (G-455--> A) in the beta-fibrinogen promoter is an independent predictor of plasma fibrinogen, but not of ischemic heart disease. A study of 9,127 individuals based on the Copenhagen City Heart Study. J. Clin. Investig. 1997, 99, 3034–3039. [Google Scholar] [CrossRef] [PubMed]
- Renner, W.; Cichocki, L.; Forjanics, A.; Köppel, H.; Gasser, R.; Pilger, E. G-455A polymorphism of the fibrinogen beta gene and deep vein thrombosis. Eur. J. Clin. Investig. 2002, 32, 755–758. [Google Scholar] [CrossRef]
- Bautista, J.; Bella, A.; Chaudhari, A.; Pekler, G.; Sapra, K.J.; Carbajal, R.; Baumstein, D. Advanced chronic kidney disease in non-valvular atrial fibrillation: Extending the utility of R2CHADS2 to patients with advanced renal failure. Clin. Kidney J. 2015, 8, 226–231. [Google Scholar] [CrossRef]
- Piccini, J.P.; Stevens, S.R.; Chang, Y.; Singer, D.E.; Lokhnygina, Y.; Go, A.S.; Patel, M.R.; Mahaffey, K.W.; Halperin, J.L.; Breithardt, G.; et al. Renal dysfunction as a predictor of stroke and systemic embolism in patients with nonvalvular atrial fibrillation: Validation of the R2CHADS2 index in the ROCKET AF (Rivaroxaban Once-daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk factors In Atrial fibrillation) study cohorts. Circulation 2013, 127, 224–232. [Google Scholar]
- Singer, D.E.; Chang, Y.; Borowsky, L.H.; Fang, M.C.; Pomernacki, N.K.; Udaltsova, N.; Reynolds, K.; Go, A.S. A new risk scheme to predict ischemic stroke and other thromboembolism in atrial fibrillation: The ATRIA study stroke risk score. J. Am. Heart Assoc. 2013, 2, e000250. [Google Scholar] [CrossRef]
- Kapłon-Cieślicka, A.; Budnik, M.; Gawałko, M.; Peller, M.; Gorczyca, I.; Michalska, A.; Babiarz, A.; Bodys, A.; Uliński, R.; Żochowski, M.; et al. Atrial fibrillation type and renal dysfunction as important predictors of left atrial thrombus. Heart 2019, 105, 1310–1315. [Google Scholar] [CrossRef]
- Zeng, W.T.; Sun, X.T.; Tang, K.; Mei, W.Y.; Liu, L.J.; Xu, Q.; Cheng, Y.J. Risk of thromboembolic events in atrial fibrillation with chronic kidney disease. Stroke 2015, 46, 157–163. [Google Scholar] [CrossRef]
- Kim, M.N.; Kim, S.A.; Choi, J.I.; Park, S.M.; Park, S.W.; Kim, Y.H.; Shim, W.J. Improvement of Predictive Value for Thromboembolic Risk by Incorporating Left Atrial Functional Parameters in the CHADS2 and CHA2DS2-VASc Scores. Int. Heart J. 2015, 56, 286–292. [Google Scholar] [CrossRef]
- Nunns, G.R.; Moore, E.E.; Chapman, M.P.; Moore, H.B.; Stettler, G.R.; Peltz, E.; Burlew, C.C.; Silliman, C.C.; Banerjee, A.; Sauaia, A. The hypercoagulability paradox of chronic kidney disease: The role of fibrinogen. Am. J. Surg. 2017, 214, 1215–1218. [Google Scholar] [CrossRef] [PubMed]
- Bozdemir, V.; Kirimli, O.; Akdeniz, B.; Ulgenalp, A.; Aslan, A.; Kala, V.; Ozel, E.; Senarslan, O.; Badak, O.; Baris, N.; et al. The association of beta-fibrinogen 455 G/A gene polymorphism with left atrial thrombus and severe spontaneous echo contrast in atrial fibrillation. Anatol. J. Cardiol. Anadolu Kardiyol. Derg. 2010, 10, 209–215. [Google Scholar] [CrossRef] [PubMed]
- de Maat, M.P. Effects of diet, drugs, and genes on plasma fibrinogen levels. Ann. N. Y. Acad. Sci. 2001, 936, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Hermida, R.C.; Calvo, C.; Ayala, D.E.; López, J.E.; Fernández, J.R.; Mojón, A.; Domínguez, M.J.; Covelo, M. Seasonal variation in plasma fibrinogen in dipper and non-dipper patients with mild-moderate essential hypertension. Med. Clin. 2003, 121, 6–11. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Jacquemin, B.; Antoniades, C.; Nyberg, F.; Plana, E.; Müller, M.; Greven, S.; Salomaa, V.; Sunyer, J.; Bellander, T.; Chalamandaris, A.-G.; et al. Common genetic polymorphisms and haplotypes of fibrinogen alpha, beta, and gamma chains affect fibrinogen levels and the response to proinflammatory stimulation in myocardial infarction survivors: The AIRGENE Study. J. Am. Coll. Cardiol. 2008, 52, 941–952. [Google Scholar] [CrossRef]
- Lam, K.S.; Ma, O.C.; Wat, N.M.; Chan, L.C.; Janus, E.D. Beta-fibrinogen gene G/A-455 polymorphism in relation to fibrinogen concentrations and ischaemic heart disease in Chinese patients with type II diabetes. Diabetologia 1999, 42, 1250–1253. [Google Scholar] [CrossRef]
- Morozumi, T.; Sharma, A.; De Nardin, E. The functional effects of the −455G/A polymorphism on the IL-6-induced expression of the beta-fibrinogen gene may be due to linkage disequilibrium with other functional polymorphisms. Immunol. Investig. 2009, 38, 311–323. [Google Scholar] [CrossRef]
- Cook, D.G.; Cappuccio, F.P.; Atkinson, R.W.; Wicks, P.D.; Chitolie, A.; Nakandakare, E.R.; Sagnella, G.A.; Humphries, S.E. Ethnic differences in fibrinogen levels: The role of environmental factors and the beta-fibrinogen gene. Am. J. Epidemiol. 2001, 153, 799–806. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| LAT Group (n = 60) | Control Group (n = 121) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p | |||||
| Age | 68 | 60.5–72.5 | 67 | 58–72 | 0.4747 | ||||
| n | % | n | % | ||||||
| Male sex | 33 | 55 | 93 | 76.9 | 0.0027 | ||||
| Smoking | 7 | 11.7 | 14 | 11.6 | 0.9848 | ||||
| AF parox | 5 | 8.3 | 29 | 24.0 | 0.0115 | ||||
| Hypertension | 49 | 81.7 | 86 | 71.1 | 0.1244 | ||||
| DM type II | 15 | 25.0 | 16 | 13.2 | 0.0484 | ||||
| Vascular disease | 20 | 33.3 | 18 | 14.9 | 0.0042 | ||||
| Liver disease | 1 | 1.7 | 5 | 4.1 | 0.3844 | ||||
| CHF | 35 | 58.3 | 42 | 34.7 | 0.0025 | ||||
| CHA2DS2VASc | 0.0025 | ||||||||
| 0–1 | 8 | 13.3 | 42 | 34.7 | |||||
| 2–8 | 52 | 86.7 | 79 | 65.3 | |||||
| LA enlargement | 52 | 86.7 | 96 | 79.3 | 0.2293 | ||||
| LVEF | 50 | 40–60 | 55 | 45–60 | 0.0903 | ||||
| FG plasma level | 3.9 | 3.3–5 | 3.6 | 3–4.225 | 0.0115 | ||||
| Anticoagulant | 55 | 91.7 | 112 | 92.6 | 0.8324 | ||||
| CVI/TIA | 2 | 3.3 | 4 | 3.3 | 0.9922 | ||||
| A+ | 30 | 50.0 | 63 | 52.1 | 0.7928 | ||||
| A/A | 4 | 6.7 | 8 | 13.4 | 0.092 | ||||
| eGFR Cockroft | 79.9 | 62–97.2 | 97.3 | 79.9–112.7 | <0.001 | ||||
| Thromb Group (n = 60) | Control Group (n = 60) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p | |||||
| Age | 68 | 60.5–72.5 | 68 | 62–72 | 0.9362 | ||||
| n | % | n | % | ||||||
| Male sex | 33 | 55.0 | 37 | 61.0 | 0.125 | ||||
| Smoking | 7 | 11.7 | 7 | 11.7 | 1 | ||||
| AF parox | 5 | 8.3 | 4 | 6.7 | 1 | ||||
| Hypertension | 49 | 81.7 | 47 | 78.3 | 0.5 | ||||
| DM type II | 15 | 25.0 | 11 | 18.3 | 0.125 | ||||
| Vascular disease | 20 | 33.3 | 16 | 26.7 | 0.125 | ||||
| Liver disease | 1 | 1.7 | 3 | 5.0 | 0.5 | ||||
| CHF | 35 | 58.3 | 38 | 63.3 | 0.25 | ||||
| CHA2DS2VASc | 1 | ||||||||
| 0–1 | 8 | 13.3 | 9 | 15.0 | |||||
| 2–8 | 52 | 86.7 | 51 | 85.0 | |||||
| LA enlargement | 52 | 86.7 | 50 | 83.3 | 0.5 | ||||
| LVEF | 50 | 40–60 | 45 | 37.5–55 | 0.3524 | ||||
| FG plasma level | 3.9 | 3.3–5 | 3.6 | 3.3–4.35 | 0.4295 | ||||
| Anticoagulant | 55 | 91.7 | 57 | 95.0 | 0.5 | ||||
| CVI/TIA | 2 | 3.3 | 1 | 1.7 | 1 | ||||
| A+ | 30 | 50.0 | 31 | 51.7 | 1 | ||||
| A/A | 4 | 6.7 | 4 | 6.7 | 1 | ||||
| eGFR Cockroft | 79.9 | 62–97.2 | 96.8 | 79.6–108.7 | 0.0131 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golubić, K.; Angebrandt Belošević, P.; Slišković, A.M.; Grubić, Z.; Štingl Janković, K.; Radeljić, V.; Delić Brkljačić, D. Serum Fibrinogen and Renal Dysfunction as Important Predictors of Left Atrial Thrombosis in Patients with Atrial Fibrillation. J. Clin. Med. 2023, 12, 6246. https://doi.org/10.3390/jcm12196246
Golubić K, Angebrandt Belošević P, Slišković AM, Grubić Z, Štingl Janković K, Radeljić V, Delić Brkljačić D. Serum Fibrinogen and Renal Dysfunction as Important Predictors of Left Atrial Thrombosis in Patients with Atrial Fibrillation. Journal of Clinical Medicine. 2023; 12(19):6246. https://doi.org/10.3390/jcm12196246
Chicago/Turabian StyleGolubić, Karlo, Petra Angebrandt Belošević, Ana Marija Slišković, Zorana Grubić, Katarina Štingl Janković, Vjekoslav Radeljić, and Diana Delić Brkljačić. 2023. "Serum Fibrinogen and Renal Dysfunction as Important Predictors of Left Atrial Thrombosis in Patients with Atrial Fibrillation" Journal of Clinical Medicine 12, no. 19: 6246. https://doi.org/10.3390/jcm12196246