In Vitro Validation of a Novel Continuous Intra-Abdominal Pressure Measurement System (TraumaGuard)

 ,
,  , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. TraumaGuard System
- Connect the cable to the patient’s bedside monitor.
- Monitor that the atmospheric pressure equal to zero is shown.
- The LED on the cable should be white. If the LED is red, disconnect the cable from the patient’s bedside monitor and follow steps A–B. If the LED on the cable remains red, do not use the cable, and follow steps A–B with another TG cable.
- With the patient in the supine position, inflate the outer distal balloon:
- Connect a syringe with 6 mL of sterile water to the outer distal balloon valve (white port).
- Pull the vacuum to evacuate excess air from the manufacturing process.
- Inflate the outer distal balloon with exactly 6 mL of sterile water.
- With the patient in the supine position, connect the TG cable to the TG catheter.
- Insert the TG cable into the TG catheter by lining up two pins on the TG cable side, with two openings on the catheter side.
- Insert until firmly in place.
- Twist the locking mechanism clockwise until secure.
- The LED on the cable should be white.
- Reduce the volume in the outer distal balloon.
- Remove exactly 3 mL of sterile water from the outer distal balloon via the syringe on the outer distal balloon valve (white port).
- Disconnect the syringe.
- The monitor should now display the real-time unfiltered IAP with the patient in the supine position.
- To enter the supine filter mode, which gives the end-expiratory pressure, press the capture button on the cable for 3 s. The LED on the cable should be green.
2.2. CiMON System
2.3. Spiegelberg System
2.4. Serenno System
2.5. Accuryn System
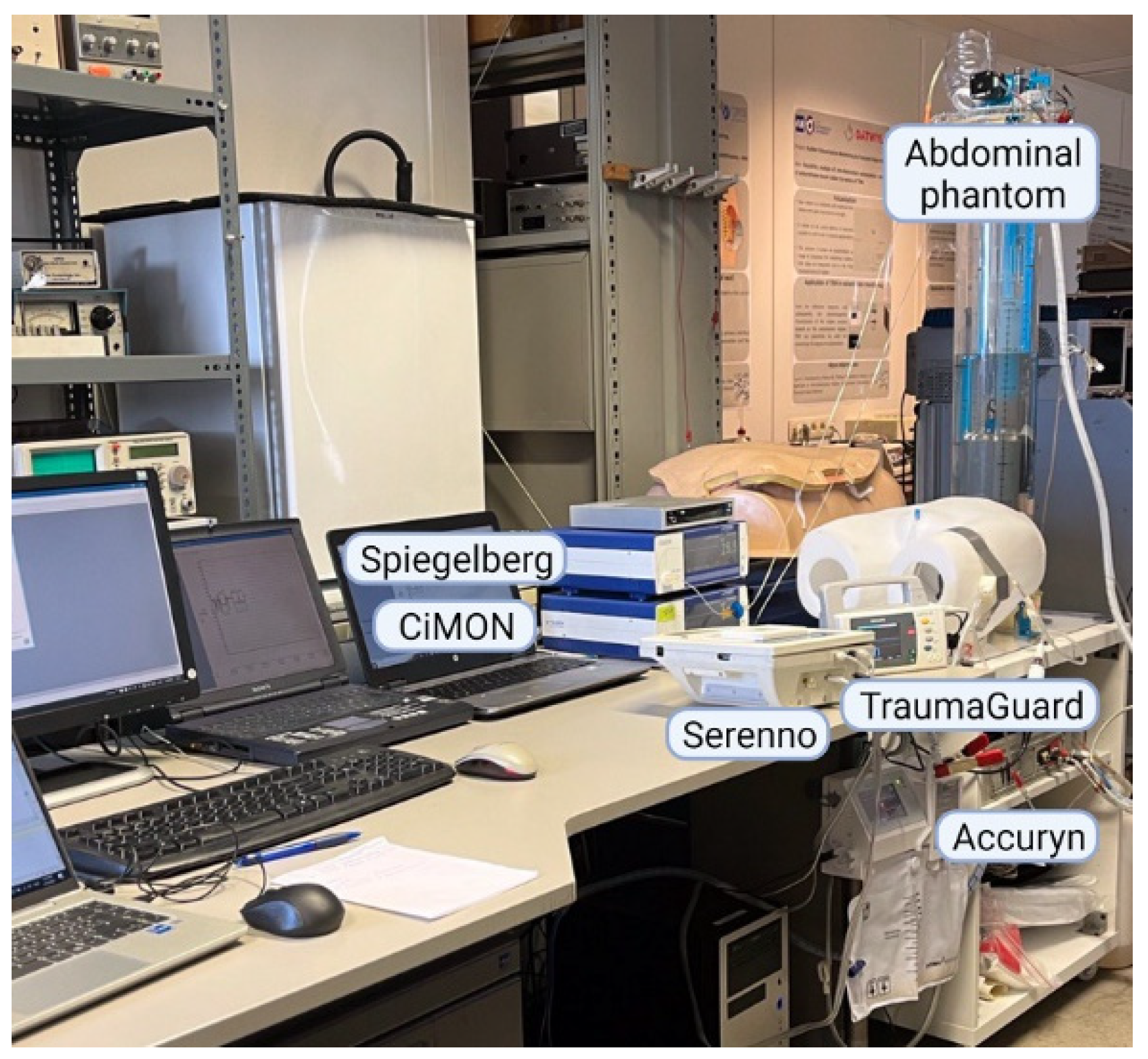
2.6. Abdominal Phantom
2.7. Study Design
2.8. Raw Data Processing
2.9. Statistical Analysis
3. Results
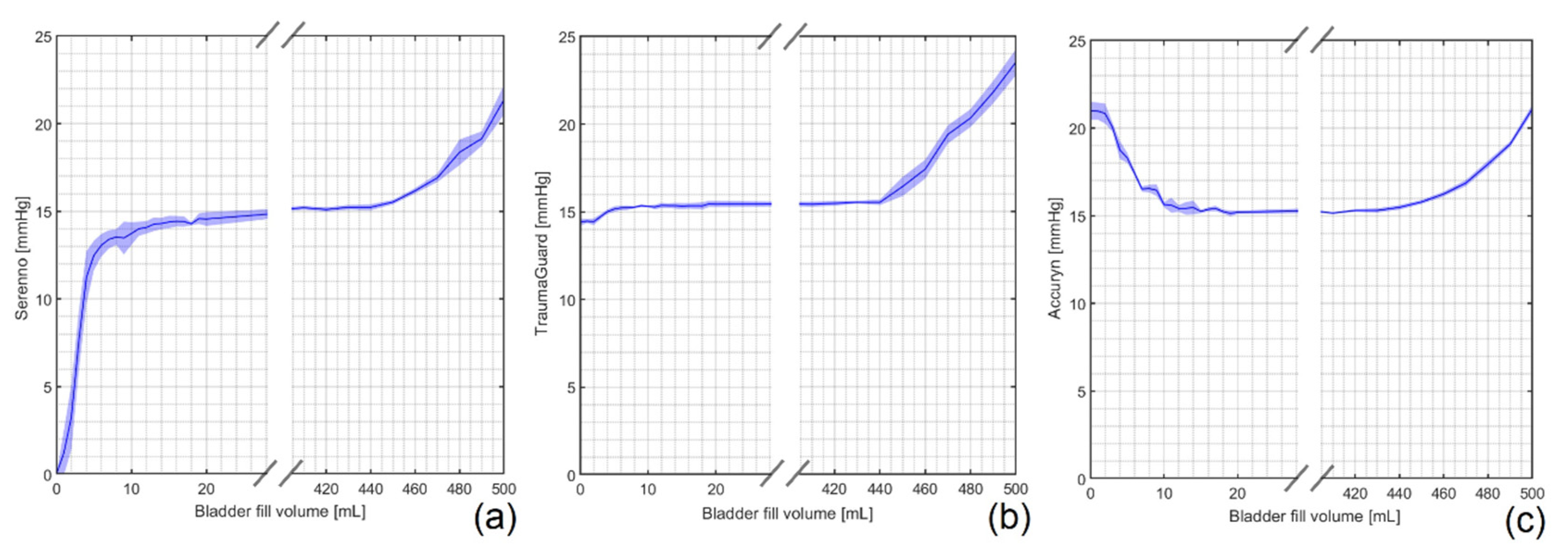
3.1. Impact of Bladder Fill Volume
3.2. Fluid (Body) Temperature
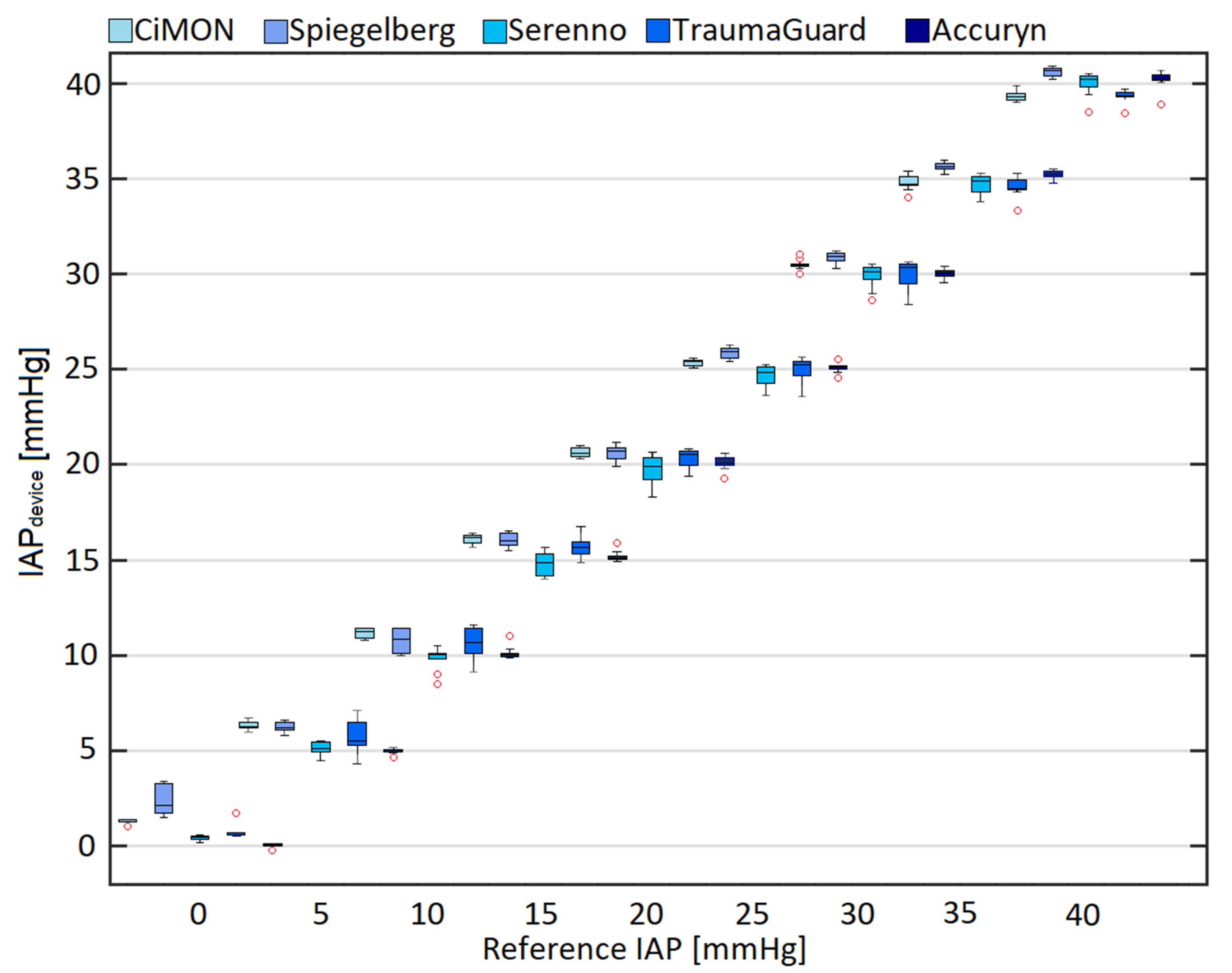
3.3. Comparison of IAPdevice and IAPH2O
3.4. Pearson’s, Lin’s, and Intra-Class Correlation Analyses
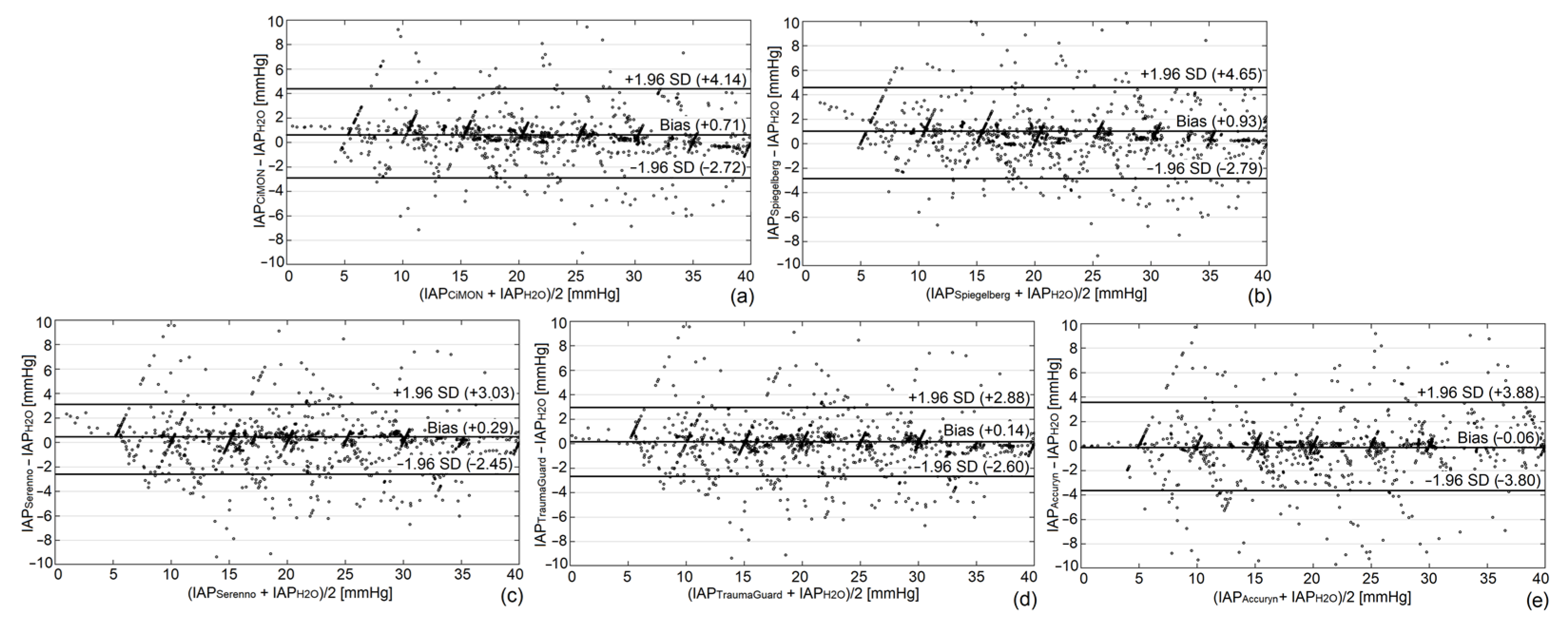
3.5. Bland and Altman Analysis
3.6. Concordance Analysis
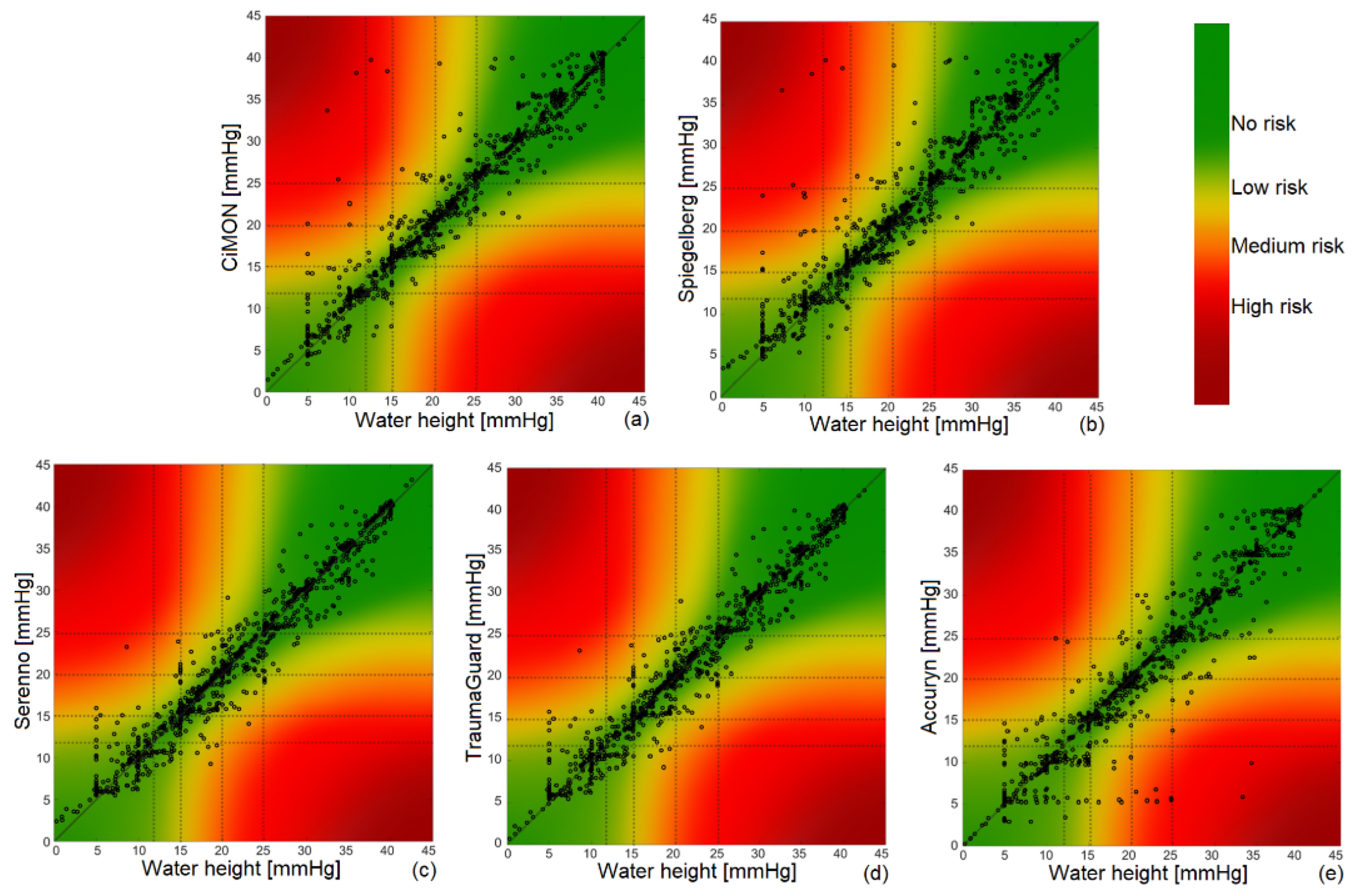
3.7. Error Grid Analysis
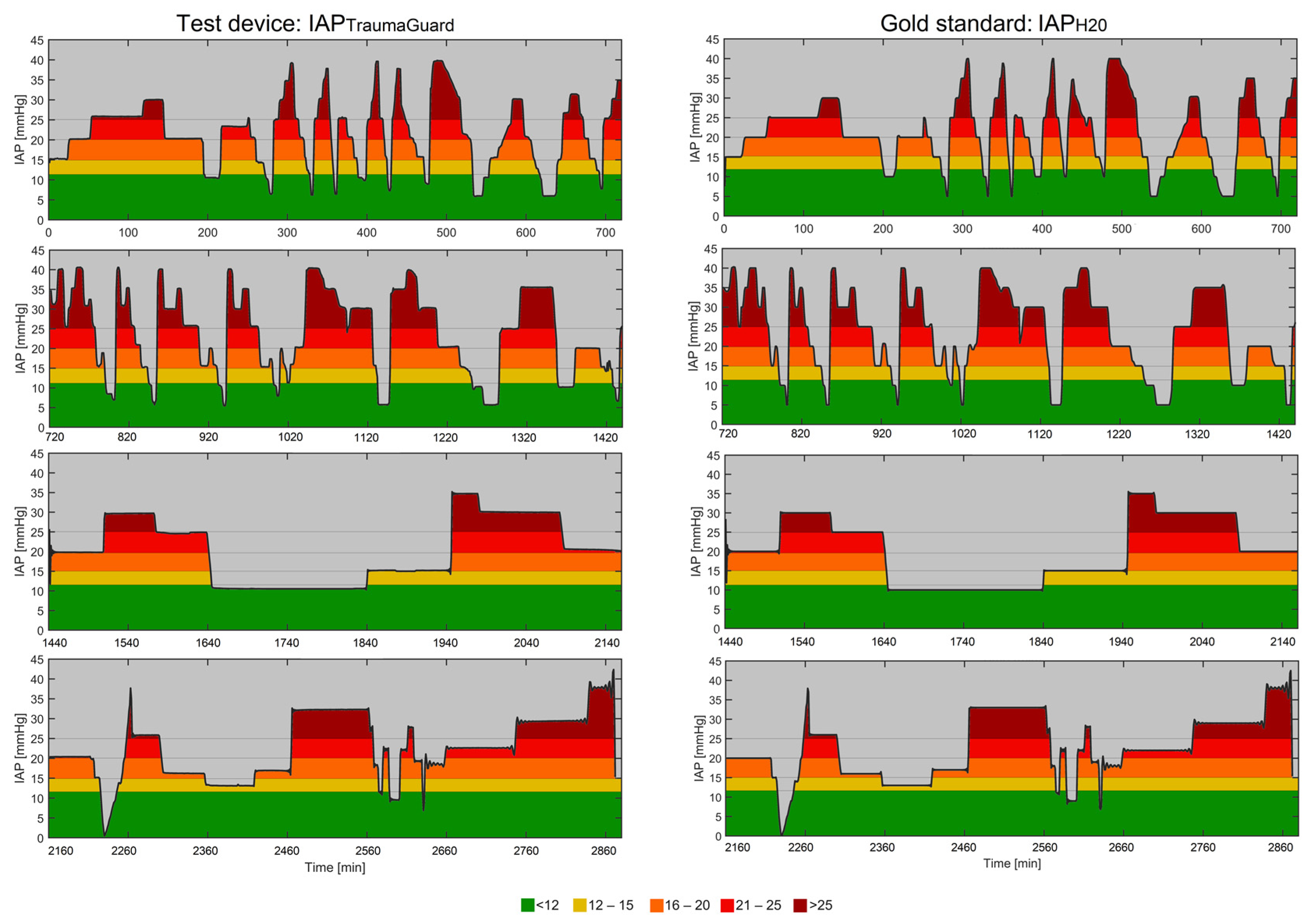
3.8. Analysis of Continuous Trends
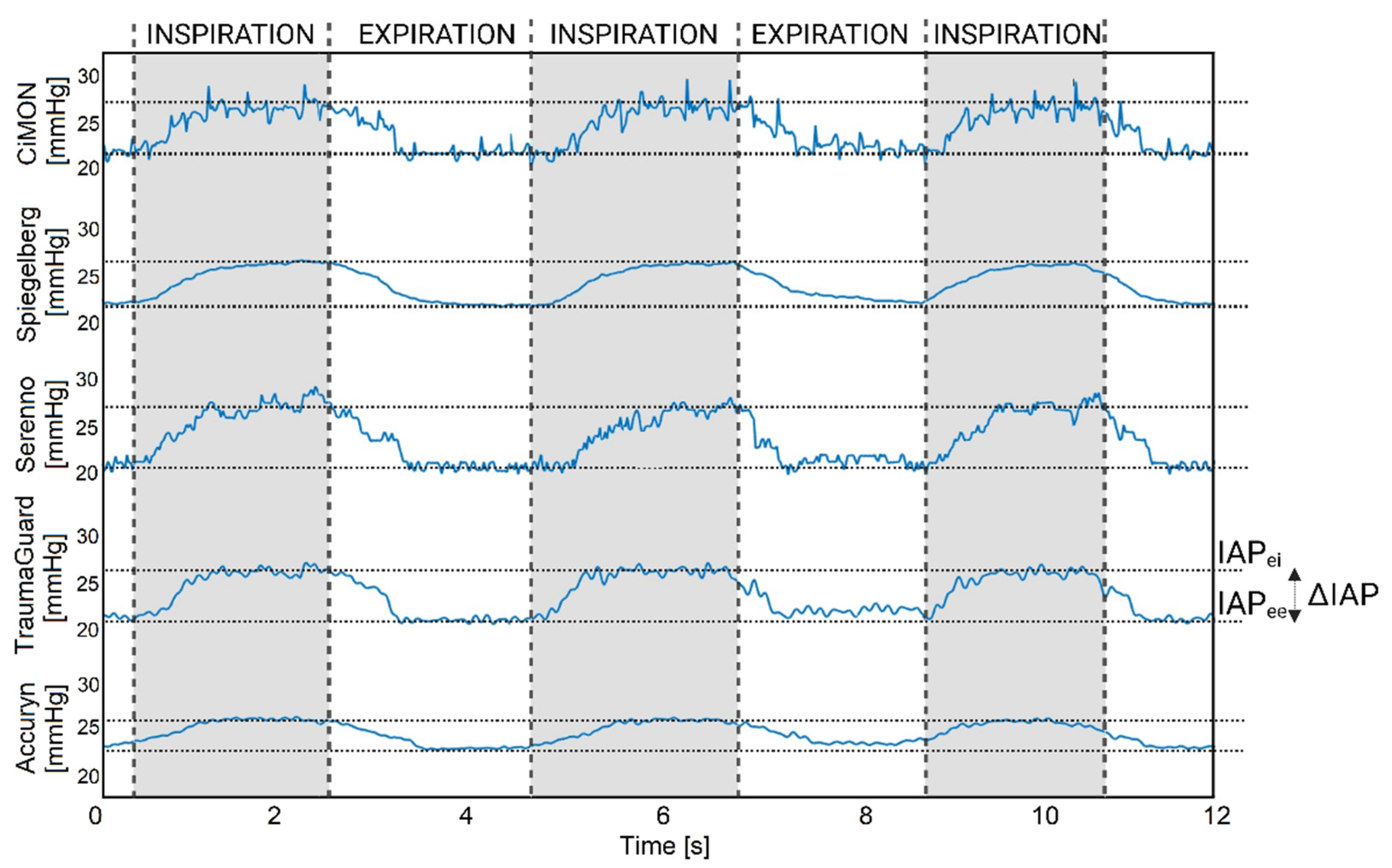
3.9. Dynamic Raw IAP Tracing (Impact of Respirations and Heartbeats)
4. Discussion
Limitations and Future Perspective
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smit, M.; van Meurs, M.; Zijlstra, J.G. Intra-abdominal hypertension and abdominal compartment syndrome in critically ill patients: A narrative review of past, present, and future steps. Scand. J. Surg. 2022, 111, 14574969211030128. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.M.; Howard, C. A 6th Vital Sign—Potential Use of Nasogastric Tube for Intra-Abdominal Pressure Monitoring Method to Detect Feeding Intolerance in Very Low Birth-Weight Preterm Infants (<1500 g). Adv. Neonatal Care 2015, 15, 176–181. [Google Scholar] [PubMed]
- Cheatham, M.L. Abdominal compartment syndrome: Pathophysiology and definitions. Scand. J. Trauma Resusc. Emerg. Med. 2009, 17, 10. [Google Scholar] [CrossRef] [PubMed]
- Sugrue, M.; Bauman, A.; Jones, F.; Bishop, G.; Flabouris, A.; Parr, M.; Stewart, A.; Hillman, K.; Deane, S.A. Clinical examination is an inaccurate predictor of intraabdominal pressure. World J. Surg. 2002, 26, 1428–1431. [Google Scholar] [CrossRef]
- Kimball, E.J. Intra-abdominal hypertension and abdominal compartment syndrome: A current review. Curr. Opin. Crit. Care 2021, 27, 164–168. [Google Scholar] [CrossRef]
- Khot, Z.; Murphy, P.B.; Sela, N.; Parry, N.G.; Vogt, K.; Ball, I.M. Incidence of Intra-Abdominal Hypertension and Abdominal Compartment Syndrome: A Systematic Review. J. Intensive Care Med. 2021, 36, 197–202. [Google Scholar] [CrossRef]
- Murphy, P.B.; Parry, N.G.; Sela, N.; Leslie, K.; Vogt, K.; Ball, I. Intra-Abdominal Hypertension Is More Common Than Previously Thought: A Prospective Study in a Mixed Medical-Surgical ICU. Crit. Care Med. 2018, 46, 958–964. [Google Scholar] [CrossRef]
- Strang, S.G.; Breederveld, R.S.; Cleffken, B.I.; Verhofstad, M.H.J.; Van Waes, O.J.F.; Van Lieshout, E.M.M. Prevalence of intra-abdominal hypertension and markers for associated complications among severe burn patients: A multicenter prospective cohort study (BURNIAH study). Eur. J. Trauma Emerg. Surg. 2022, 48, 1137–1149. [Google Scholar] [CrossRef]
- Pereira, R.; Buglevski, M.; Perdigoto, R.; Marcelino, P.; Saliba, F.; Blot, S.; Starkopf, J. Intra-abdominal hypertension and abdominal compartment syndrome in the critically ill liver cirrhotic patient-prevalence and clinical outcomes. A multicentric retrospective cohort study in intensive care. PLoS ONE 2021, 16, e0251498. [Google Scholar] [CrossRef]
- Pereira, B.; Dorigatti, A.; Melek, M.; Dos Santos, J.; Ferreira, M.; Calderan, T.; Carmona, C.; Fraga, G. Septic shock patients admitted to the intensive care unit with higher SOFA score tend to have higher incidence of abdominal compartment syndrome—A preliminary analysis. Anaesthesiol. Intensive Ther. 2019, 51, 370–372. [Google Scholar] [CrossRef]
- Muturi, A.; Ndaguatha, P.; Ojuka, D.; Kibet, A. Prevalence and predictors of intra-abdominal hypertension and compartment syndrome in surgical patients in critical care units at Kenyatta National Hospital. BMC Emerg. Med. 2017, 17, 10. [Google Scholar] [CrossRef]
- Shaheen, A.W.; Crandall, M.L.; Nicolson, N.G.; Smith-Singares, E.; Merlotti, G.J.; Jalundhwala, Y.; Issa, N.M. Abdominal compartment syndrome in trauma patients: New insights for predicting outcomes. J. Emerg. Trauma Shock 2016, 9, 53–57. [Google Scholar] [PubMed]
- Dalfino, L.; Sicolo, A.; Paparella, D.; Mongelli, M.; Rubino, G.; Brienza, N. Intra-abdominal hypertension in cardiac surgery. Interact. CardioVascular Thorac. Surg. 2013, 17, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Mao, E.Q.; Tang, Y.Q.; Fei, J.; Qin, S.; Wu, J.; Li, L.; Min, D.; Zhang, S.D. Fluid therapy for severe acute pancreatitis in acute response stage. Chin. Med. J. 2009, 122, 169–173. [Google Scholar] [PubMed]
- Kyoung, K.H.; Hong, S.K. The duration of intra-abdominal hypertension strongly predicts outcomes for the critically ill surgical patients: A prospective observational study. World J. Emerg. Surg. 2015, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Iyer, D.; Rastogi, P.; Åneman, A.; D’Amours, S. Early screening to identify patients at risk of developing intra-abdominal hypertension and abdominal compartment syndrome. Acta Anaesthesiol. Scand. 2014, 58, 1267–1275. [Google Scholar] [CrossRef]
- Al-Hwiesh, A.; Al-Mueilo, S.; Saeed, I.; Al-Muhanna, F.A. Intraperitoneal pressure and intra-abdominal pressure: Are they the same? Perit. Dial. Int. 2011, 31, 315–319. [Google Scholar] [CrossRef]
- Iacubovici, L.; Karol, D.; Baar, Y.; Beri, A.; Herzberg, H.; Zarour, S.; Goren, O.; Cohen, B. Assessment of Intra-Abdominal Pressure with a Novel Continuous Bladder Pressure Monitor-A Clinical Validation Study. Life 2023, 13, 384. [Google Scholar] [CrossRef]
- Gutting, M.; Klischke, L.; Kaussen, T. Hands off Trans-Femoral Venous Intra-Abdominal Pressure Estimates in Children: Results of a Sobering Single-Center Study. Life 2023, 13, 872. [Google Scholar] [CrossRef]
- Coleman, T.J.; Thomsen, J.C.; Maass, S.D.; Hsu, Y.; Nygaard, I.E.; Hitchcock, R.W. Development of a wireless intra-vaginal transducer for monitoring intra-abdominal pressure in women. Biomed Microdevices 2012, 14, 347–355. [Google Scholar] [CrossRef]
- MacDonald, A.; Paterson, P.J.; Baxter, J.N.; Finlay, I.G. Relationship between intra-abdominal and intrarectal pressure in the proctometrogram. Br. J. Surg. 1993, 80, 1070–1071. [Google Scholar] [CrossRef] [PubMed]
- Mahmutaj, D.; Braha, B.; Krasniqi, S.; Zhjeqi, V.; Rrusta, A. The Role of Biomarkers and Intra-Abdominal Pressure in Diagnosing and Predicting Mortality of Intra-Abdominal Infections. J. Int. Dent. Med. Res. 2019, 12, 1389–1396. [Google Scholar]
- See, K.C.; Tayebi, S.; Sum, C.L.; Phua, J.; Stiens, J.; Wise, R.; Mukhopadhyay, A.; Malbrain, M.L.N.G. Feasibility analysis of a novel non-invasive ultrasonographic method for the measurement of intra-abdominal pressure in the intensive care unit. J. Clin. Monit. Comput. 2023, 37, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Smereczyński, A.; Kołaczyk, K.; Bernatowicz, E. Ultrasonography in the diagnosis and monitoring of intra-abdominal hypertension and abdominal compartment syndrome: Ultrasonografia a nadciśnienie wewnątrzbrzuszne i zespół przedziału brzusznego. J. Ultrason. 2020, 20, e201–e204. [Google Scholar] [CrossRef]
- Tang, H.; Liu, D.; Guo, Y.; Zhang, H.; Li, Y.; Peng, X.; Wang, Y.; Jiang, D.; Zhang, L.; Wang, Z. A New Device for Measuring Abdominal Wall Tension and Its Value in Screening Abdominal Infection. Med. Devices 2021, 14, 119–131. [Google Scholar] [CrossRef]
- David, M.; Yellin, E.; Pracca, F.; Simini, F. Intra-Abdominal Pressure Monitoring by Surface Bioimpedance Estimation. J. Phys. Conf. Ser. 2019, 1272, 012013. [Google Scholar] [CrossRef]
- Tang, H.; Dai, Y.; Zhao, D.; Sun, Z.; Chen, F.; Zhu, Y.; Liang, H.; Cao, H.; Zhang, L. Deep Domain Adaptation for Predicting Intra-Abdominal Pressure with Multichannel Attention Fusion Radar Chip. Adv. Intell. Syst. 2022, 4, 2100209. [Google Scholar] [CrossRef]
- David, M.; Raviv, A.; Guttel, A.; García Reyes, V.; Simini, F.; Pracca, F. Non-invasive indirect monitoring of intra-abdominal pressure using microwave reflectometry: System design and proof-of-concept clinical trial. J. Clin. Monit. Comput. 2021, 35, 1437–1443. [Google Scholar] [CrossRef]
- Kirkpatrick, A.W.; Sugrue, M.; McKee, J.L.; Pereira, B.M.; Roberts, D.J.; De Waele, J.J.; Leppaniemi, A.; Ejike, J.C.; Reintam Blaser, A.; D’Amours, S.; et al. Update from the Abdominal Compartment Society (WSACS) on intra-abdominal hypertension and abdominal compartment syndrome: Past, present, and future beyond Banff 2017. Anaesthesiol Intensive Ther. 2017, 49, 83–87. [Google Scholar] [CrossRef]
- Becker, V.; Schmid, R.M.; Umgelter, A. Comparison of a new device for the continuous intra-gastric measurement of intra-abdominal pressure (CiMon) with direct intra-peritoneal measurements in cirrhotic patients during paracentesis. Intensive Care Med. 2009, 35, 948–952. [Google Scholar] [CrossRef]
- Kaussen, T.; Gutting, M.; Lasch, F.; Boethig, D.; von Gise, A.; Dingemann, J.; Koeditz, H.; Jack, T.; Sasse, M.; Beerbaum, P.; et al. Continuous intra-gastral monitoring of intra-abdominal pressure in critically ill children: A validation study. Intensive Care Med. Exp. 2021, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; D’Attellis, N.; Emerson, D.; Moll, V.; Esmailian, F. Automated Intra-Abdominal Pressure Monitoring during Orthotopic Heart Transplant Leads to Early Diagnosis and Treatment of Intraoperative Abdominal Compartment Syndrome—A Case Report. Front. Surg. 2022, 9, 812288. [Google Scholar] [CrossRef]
- Early, G.L.; Wesp, J.; Augustin, S.M. Intra-abdominal hypertension and abdominal compartment syndrome. Mo Med. 2012, 109, 376–378. [Google Scholar] [PubMed]
- Tayebi, S.; Wise, R.; Pourkazemi, A.; Stiens, J.; Malbrain, M. Pre-Clinical Validation of A Novel Continuous Intra-Abdominal Pressure Measurement Equipment (SERENNO). Life 2022, 12, 1161. [Google Scholar] [CrossRef] [PubMed]
- Saugel, B.; Grothe, O.; Nicklas, J.Y. Error Grid Analysis for Arterial Pressure Method Comparison Studies. Anesth. Analg. 2018, 126, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Parkes, J.L.; Slatin, S.L.; Pardo, S.; Ginsberg, B.H. A new consensus error grid to evaluate the clinical significance of inaccuracies in the measurement of blood glucose. Diabetes Care 2000, 23, 1143–1148. [Google Scholar] [CrossRef]
- Lin, L.I. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Hiraishi, M.; Tanioka, K.; Shimokawa, T. Concordance rate of a four-quadrant plot for repeated measurements. BMC Med. Res. Methodol. 2021, 21, 270. [Google Scholar] [CrossRef]
- McKinney, T.B.; Babin, E.A.; Ciolfi, V.; McKinney, C.R.; Shah, N. Comparison of water and air charged transducer catheter pressures in the evaluation of cystometrogram and voiding pressure studies. Neurourol. Urodyn. 2018, 37, 1434–1440. [Google Scholar] [CrossRef]
- De Waele, J.J.; Cheatham, M.L.; Malbrain, M.L.; Kirkpatrick, A.W.; Sugrue, M.; Balogh, Z.; Ivatury, R.; De Keulenaer, B.; Kimball, E.J. Recommendations for Research from the International Conference of Experts on Intra-Abdominal Hypertension and Abdominal Compartment Syndrome. Acta Clin. Belg. 2009, 64, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Thangarasa, T.; Foisy, D.; Leidecker, J.; Corsi, D.J.; Meggison, H.; Blew, B.; Warren, J.; Zimmerman, D. In Search of a Simple and Reliable Method of Measuring Intra-abdominal Pressure in Peritoneal Dialysis Patients. Can. J. Kidney Health Dis. 2019, 6, 2054358119892695. [Google Scholar] [CrossRef]
- Akiode, O.; Moll, V.; Schears, G. Continuous Monitoring of Intra-Abdominal Pressure in Severe Acute Pancreatitis Leads to Early Detection of Abdominal Compartment Syndrome: A Case Report. Cureus 2022, 14, e24606. [Google Scholar] [CrossRef] [PubMed]
- de Cleva, R.; de Assumpção, M.S.; Sasaya, F.; Chaves, N.Z.; Santo, M.A.; Fló, C.; Lunardi, A.C.; Filho, W.J. Correlation between intra-abdominal pressure and pulmonary volumes after superior and inferior abdominal surgery. Clinics 2014, 69, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Vatankhah, S.; Sheikhi, R.A.; Heidari, M.; Moradimajd, P. The relationship between fluid resuscitation and intra-abdominal hypertension in patients with blunt abdominal trauma. Int. J. Crit. Illn. Inj. Sci. 2018, 8, 149–153. [Google Scholar] [PubMed]
- Dabrowski, W.; Rola, P.; Malbrain, M. Intra-abdominal pressure monitoring in cardiac surgery: Is this the canary in the coalmine for kidney injury? J. Clin. Monit. Comput. 2023, 37, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, A.R.; Pandya, J.S. Study of the occurrence of intra-abdominal hypertension and abdominal compartment syndrome in patients of blunt abdominal trauma and its correlation with the clinical outcome in the above patients. World J. Emerg. Surg. 2016, 11, 9. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Method | Mean IAP (mm Hg) | Bias (mm Hg) | Precision (mm Hg) | LLA (mm Hg) | ULA (mm Hg) | PE (%) |
|---|---|---|---|---|---|---|
| 48 h of continuous IAP tracings (n = 2880) | ||||||
| CiMON | 22.74 | +0.71 | 1.75 | −2.72 | +4.14 | 15.39 |
| Spiegelberg | 22.96 | +0.93 | 1.90 | −2.79 | +4.65 | 16.55 |
| Serenno | 22.32 | +0.29 | 1.40 | −2.45 | +3.03 | 12.54 |
| TraumaGuard | 22.17 | +0.14 | 1.40 | −2.60 | +2.88 | 12.62 |
| Accuryn | 21.97 | −0.06 | 1.90 | −3.80 | +3.66 | 17.29 |
| Intermittent IAP readings (n = 300) | ||||||
| CiMON | 19.75 | +0.87 | 0.54 | −0.19 | +1.93 | 5.46 |
| Spiegelberg | 20.02 | +1.15 | 0.76 | −0.34 | +2.63 | 7.59 |
| Serenno | 19.27 | +0.39 | 0.40 | −0.39 | +1.17 | 4.15 |
| TraumaGuard | 19.13 | +0.25 | 0.92 | −1.55 | +2.05 | 9.61 |
| Accuryn | 19.05 | +0.17 | 0.51 | −0.83 | +1.17 | 5.35 |
| No-Risk Region | Low-Risk Region | Medium-Risk Region | High-Risk Region | |
|---|---|---|---|---|
| CiMON | 92.93% | 5.20% | 1.04% | 0.83% |
| Spiegelberg | 92.04% | 5.65% | 1.45% | 0.86% |
| Serenno | 93.38% | 5.03% | 1.18% | 0.41% |
| TraumaGuard | 93.32% | 5.06% | 1.21% | 0.41% |
| Accuryn | 93.13% | 5.21% | 1.14% | 0.52% |
| TAT (min) | TAT (%) | |||||
|---|---|---|---|---|---|---|
| IAPgold | IAPTG | p-Value | IAPgold | IAPTG | p-Value | |
| <12 | 118.5 ± 63.4 | 115.5 ± 63.5 | NS | 52.2 ± 3.6 | 52.3 ± 3.8 | NS |
| >12 | 600 ± 63.3 | 603 ± 63.4 | NS | 47.8 ± 3.7 | 47.7 ± 3.8 | NS |
| 12–15 | 84 ± 15.2 | 41 ± 21.7 | 0.09 | 11.1 ± 0.5 | 11.0 ± 0.5 | 0.09 |
| 15–20 | 158.0 ± 58.1 | 141.8 ± 14.2 | NS | 15.2 ± 1.0 | 15.4 ± 1.0 | NS |
| 20–25 | 108.8 ± 22.3 | 147.8 ± 33.5 | NS | 10.3 ± 1.0 | 10.5 ± 0.9 | NS |
| >25 | 250 ± 39.6 | 273.3 ± 62.6 | NS | 11.2 ± 2.8 | 10.9 ± 2.8 | NS |
| AUC (min × mm Hg) | AUC (%) | |||||
| <12 | 8244.4 ± 139.9 | 8334.6 ± 104.9 | 0.05 | 52.2 ± 3.6 | 63.5 ± 3.8 | NS |
| >12 | 7599.2 ± 1026.9 | 7649.7 ± 1078 | NS | 47.8 ± 3.7 | 63.4 ± 3.8 | NS |
| 12–15 | 1754.5 ± 139.3 | 1754.4 ± 140.1 | NS | 11.1 ± 0.5 | 21.7 ± 0.5 | NS |
| 15–20 | 2411.0 ± 238.9 | 2457.5 ± 257 | NS | 15.2 ± 1.0 | 14.2 ± 1.0 | NS |
| 20–25 | 1635.6 ± 243.5 | 1676.6 ± 250.8 | 0.05 | 10.3 ± 1.0 | 33.5 ± 0.9 | NS |
| >25 | 1798.0 ± 540.1 | 1761.3 ± 553.7 | NS | 11.2 ± 2.8 | 62.6 ± 2.8 | 0.02 |
| Reference | CiMON | Spiegelberg | Serenno | TraumaGuard | Accuryn | |
|---|---|---|---|---|---|---|
| IAPei (mm Hg) | 25 | 25.88 ± 0.30 | 26.07 ± 0.08 | 26.29 ± 0.07 | 25.15 ± 0.22 | 25.72 ± 0.13 |
| IAPee (mm Hg) | 20 | 20.7 ± 0.20 | 21.59 ± 0.11 | 21.23 ± 0.47 | 20.27 ± 0.18 | 21.63 ± 0.07 |
| Mean IAP (mm Hg) | 22.5 | 23.29 ± 0.15 | 23.83 ± 0.09 | 23.76 ± 0.23 | 22.71 ± 0.13 | 23.78 ± 0.10 |
| ΔIAP (mm Hg) | 5 | 5.18 ± 0.41 | 4.48 ± 0.10 | 5.06 ± 0.48 | 4.88 ± 0.31 | 4.07 ± 0.27 |
| APV (%) | 22.22 | 22.24 ± 1.75 | 18.79 ± 0.29 | 21.27 ± 1.48 | 21.48 ± 1.01 | 17.20 ± 0.32 |
| HR (bpm) | 120 | 127.11 ± 4.59 | 84.04 ± 7.32 | 98.21 ± 6.48 | 125.16 ± 6.11 | 87.12 ± 8.41 |
| RR (rpm) | 16.21 | 16.07 ± 0.71 | 16.46 ± 0.84 | 17.05 ± 0.52 | 15.80 ± 0.85 | 16.14 ± 0.64 |
| Tinsp (sec) | 1.8 | 1.79 ± 0.12 | 1.79 ± 0.09 | 1.70 ± 0.12 | 1.86 ± 0.21 | 1.83 ± 0.02 |
| Texp (sec) | 1.9 | 1.96 ± 0.24 | 1.86 ± 0.13 | 1.80 ± 0.07 | 1.95 ± 0.04 | 1.88 ± 0.21 |
| I/E (ratio) | 0.95 | 0.93 ± 0.17 | 0.96 ± 0.02 | 0.96 ± 0.09 | 0.95 ± 0.11 | 0.97 ± 0.13 |
| Parameter | Intra-Gastric | Intra-Bladder | |||
|---|---|---|---|---|---|
| CiMON | Spiegelberg | Serenno | Accuryn | TraumaGuard | |
| Zeroing Procedure (autocalibration) | 5 | 5 | 5 | 5 | 4 |
| Accuracy | 4 | 4 | 5 | 5 | 5 |
| Precision | 4 | 4 | 5 | 4 | 4 |
| Respiration monitoring | 5 | 5 | 5 | 4 | 5 |
| Heartbeat monitoring | 5 | 4 | 4 | 4 | 4 |
| Associated risk level | 5 | 5 | 5 | 5 | 5 |
| Temperature dependency | 5 | 3 | 5 | 5 | 5 |
| Data extraction capability | 5 | 5 | 4 | 3 | 5 |
| Bladder fill volume dependency | NA | NA | 3 | 3 | 5 |
| Average in vitro score (scale from 1 to 5) | 4.75 ± 0.43 | 4.38 ± 0.69 | 4.50 ± 0.68 | 4.22 ± 0.78 | 4.67 ± 0.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tayebi, S.; Wise, R.; Zarghami, A.; Malbrain, L.; Khanna, A.K.; Dabrowski, W.; Stiens, J.; Malbrain, M.L.N.G. In Vitro Validation of a Novel Continuous Intra-Abdominal Pressure Measurement System (TraumaGuard). J. Clin. Med. 2023, 12, 6260. https://doi.org/10.3390/jcm12196260
Tayebi S, Wise R, Zarghami A, Malbrain L, Khanna AK, Dabrowski W, Stiens J, Malbrain MLNG. In Vitro Validation of a Novel Continuous Intra-Abdominal Pressure Measurement System (TraumaGuard). Journal of Clinical Medicine. 2023; 12(19):6260. https://doi.org/10.3390/jcm12196260
Chicago/Turabian StyleTayebi, Salar, Robert Wise, Ashkan Zarghami, Luca Malbrain, Ashish K. Khanna, Wojciech Dabrowski, Johan Stiens, and Manu L. N. G. Malbrain. 2023. "In Vitro Validation of a Novel Continuous Intra-Abdominal Pressure Measurement System (TraumaGuard)" Journal of Clinical Medicine 12, no. 19: 6260. https://doi.org/10.3390/jcm12196260
APA StyleTayebi, S., Wise, R., Zarghami, A., Malbrain, L., Khanna, A. K., Dabrowski, W., Stiens, J., & Malbrain, M. L. N. G. (2023). In Vitro Validation of a Novel Continuous Intra-Abdominal Pressure Measurement System (TraumaGuard). Journal of Clinical Medicine, 12(19), 6260. https://doi.org/10.3390/jcm12196260