
Perinatal Outcomes in Foetuses with Increased Nuchal Translucency and Normal Karyotype: A Retrospective Cohort Study from the United Arab Emirates

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Outcomes
2.2. Statistical Analyses
3. Results
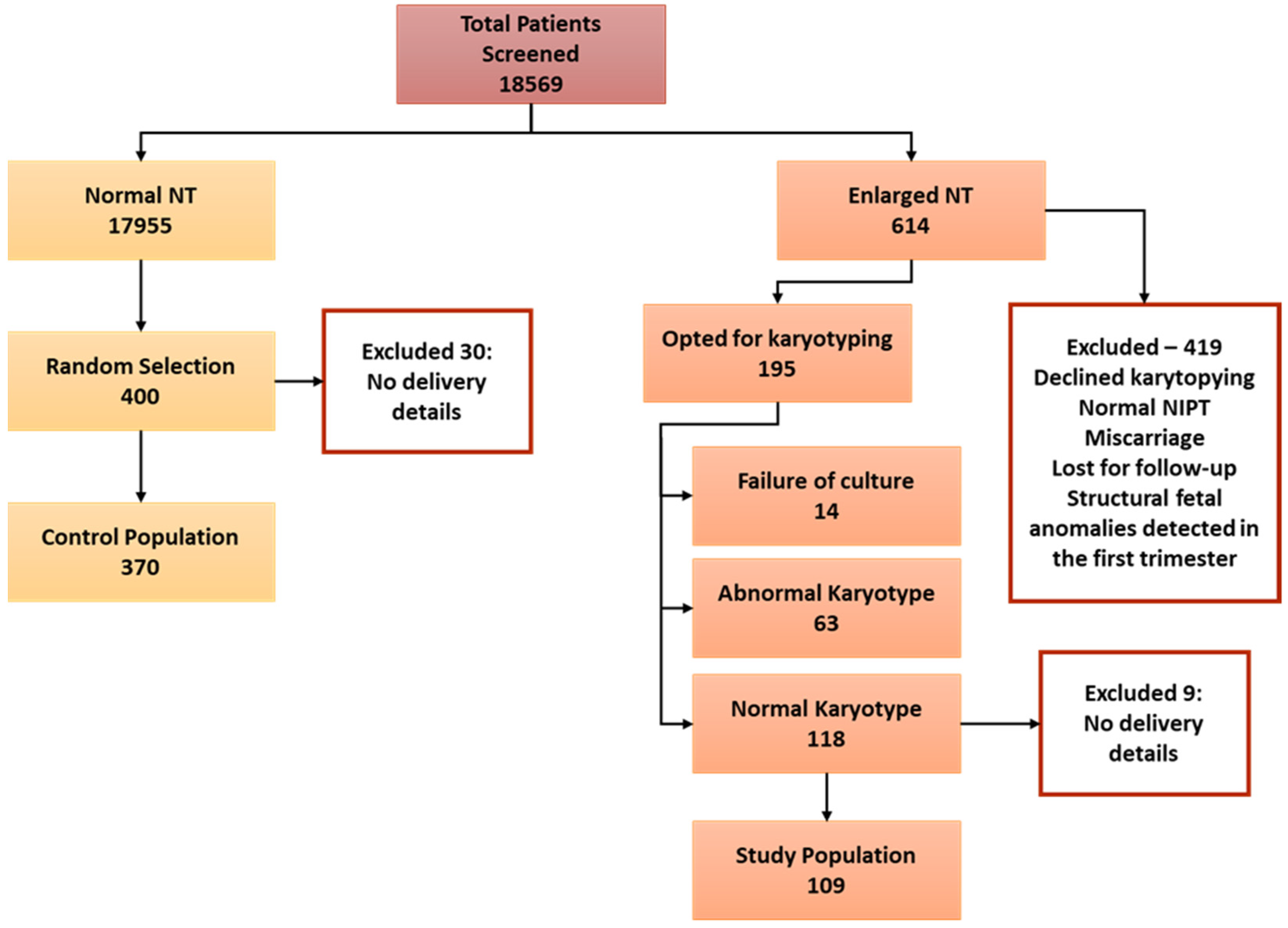
3.1. Study Population
3.2. Pregnancy and Delivery Outcomes
3.3. Factors Affecting Pregnancy and Delivery Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nicolaides, K.H.; Azar, G.; Byrne, D.; Mansur, C.; Marks, K. Fetal nuchal translucency: Ultrasound screening for chromosomal defects in first trimester of pregnancy. Br. Med. J. 1992, 304, 867–869. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, K.H.; Snijders, R.J.; Gosden, C.M.; Berry, C.; Campbell, S. Ultrasonographically detectable markers of fetal chromosomal abnormalities. Lancet 1992, 340, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Kagan, K.O.; Sonek, J.; Wagner, P.; Hoopmann, M. Principles of first trimester screening in the age of non-invasive prenatal diagnosis: Screening for chromosomal abnormalities. Arch. Gynecol. Obstet. 2017, 296, 645–651. [Google Scholar] [CrossRef]
- Bardi, F.; Bosschieter, P.; Verheij, J.; Go, A.; Haak, M.; Bekker, M.; Sikkel, E.; Coumans, A.; Pajkrt, E.; Bilardo, C. Is there still a role for nuchal translucency measurement in the changing paradigm of first trimester screening? Prenat. Diagn. 2020, 40, 197–205. [Google Scholar] [CrossRef]
- Miranda, J.; Paz y Miño, F.; Borobio, V.; Badenas, C.; Rodriguez-Revenga, L.; Pauta, M.; Borrell, A. Should cell-free DNA testing be used in pregnancy with increased fetal nuchal translucency? Ultrasound Obstet. Gynecol. 2020, 55, 645–651. [Google Scholar] [CrossRef]
- Zalel, Y.; Zemet, R.; Kivilevitch, Z. The added value of detailed early anomaly scan in fetuses with increased nuchal translucency. Prenat. Diagn. 2017, 37, 235–243. [Google Scholar] [CrossRef]
- Minnella, G.P.; Crupano, F.M.; Syngelaki, A.; Zidere, V.; Akolekar, R.; Nicolaides, K.H. Diagnosis of major heart defects by routine first-trimester ultrasound examination: Association with increased nuchal translucency, tricuspid regurgitation and abnormal flow in ductus venosus. Ultrasound Obstet. Gynecol. 2020, 55, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.A.; Pajkrt, E.; Bleker, O.P.; Bonsel, G.J.; Bilardo, C.M. Disappearance of enlarged nuchal translucency before 14 weeks’ gestation: Relationship with chromosomal abnormalities and pregnancy outcome. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2004, 24, 169–174. [Google Scholar] [CrossRef]
- Bakker, M.; Pajkrt, E.; Bilardo, C.M. Increased nuchal translucency with normal karyotype and anomaly scan: What next? Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 355–366. [Google Scholar] [CrossRef]
- Clur, S.A.; Ottenkamp, J.; Bilardo, C.M. The nuchal translucency and the fetal heart: A literature review. Prenat. Diagn. 2009, 29, 739–748. [Google Scholar] [CrossRef]
- Souka, A.P.; von Kaisenberg, C.S.; Hyett, J.A.; Sonek, J.D.; Nicolaides, K.H. Increased nuchal translucency with normal karyotype. Am. J. Obstet. Gynecol. 2005, 192, 1005–1021. [Google Scholar] [CrossRef]
- Snijders, R.J.M.; Noble, P.; Sebire, N.; Souka, A.; Nicolaides, K.H. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10–14 weeks of gestation. Lancet 1998, 352, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Souka, A.P.; Snijders, R.J.M.; Novakov, A.; Soares, W.; Nicolaides, K.H. Defects and syndromes in chromosomally normal fetuses with increased nuchal translucency thickness at 10–14 weeks of gestation. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 1998, 11, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Souka, A.P.; Krampl, E.; Bakalis, S.; Heath, V.; Nicolaides, K.H. Outcome of pregnancy in chromosomally normal fetuses with increased nuchal translucency in the first trimester. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2001, 18, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Michailidis, G.D.; Economides, D.L. Nuchal translucency measurement and pregnancy outcome in karyotypically normal fetuses. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2001, 17, 102–105. [Google Scholar] [CrossRef]
- De Domenico, R.; Faraci, M.; Hyseni, E.; Di Prima, F.A.F.; Valenti, O.; Monte, S.; Giorgio, E.; Renda, E. Increased nuchal traslucency in normal karyotype fetuses. J. Prenat. Med. 2011, 5, 23–26. [Google Scholar]
- Kelley, J.; McGillivray, G.; Meagher, S.; Hui, L. Increased nuchal translucency after low-risk noninvasive prenatal testing: What should we tell prospective parents? Prenat. Diagn. 2021, 41, 1305–1315. [Google Scholar] [CrossRef]
- Bilardo, C.M.; Müller, M.A.; Pajkrt, E.; Clur, S.A.; van Zalen, M.M.; Bijlsma, E.K. Increased nuchal translucency thickness and normal karyotype: Time for parental reassurance. Ultrasound Obstet. Gynecol. 2007, 30, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, R.; Omann, C.; Gaynor, J.W.; Rode, L.; Ekelund, C.K.; Hjortdal, V.E. Increased nuchal translucency in children with congenital heart defects and normal karyotype—Is there a correlation with mortality? Front. Pediatr. 2023, 11, 1104179. [Google Scholar] [CrossRef] [PubMed]
- Buffin, R.; Fichez, A.; Decullier, E.; Roux, A.; Bin, S.; Combourieu, D.; Pastor-Diez, B.; Huissoud, C.; Picaud, J.C.; collaborating authors. Neurodevelopmental outcome at 2 years of corrected age in fetuses with increased nuchal translucency thickness and normal karyotype compared with matched controls. Ultrasound Obstet. Gynecol. 2021, 57, 790–797. [Google Scholar] [CrossRef]
- Spataro, E.; Cordisco, A.; Luchi, C.; Filardi, G.R.; Masini, G.; Pasquini, L. Increased nuchal translucency with normal karyotype and genomic microarray analysis: A multicenter observational study. Int. J. Gynecol. Obstet. 2023, 161, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Haak, M.C.; van Vugt, J.M. Pathophysiology of increased nuchal translucency: A review of the literature. Hum. Reprod. Update 2003, 9, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.; Muscatello, A.; Angelini, E.; Capponi, A. Abnormal cardiac function in fetuses with increased nuchal translucency. Ultrasound Obstet. Gynecol. 2003, 21, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Bellini, C.; Rutigliani, M.; Boccardo, F.M.; Bonioli, E.; Campisi, C.; Grillo, F.; Bellini, T.; Valenzano, M.; Fulcheri, E. Nuchal translucency and lymphatic system maldevelopment. J. Perinat. Med. 2009, 37, 673–676. [Google Scholar] [CrossRef]
- Böhlandt, S.; Von Kaisenberg, C.S.; Wewetzer, K.; Christ, B.; Nicolaides, K.H.; Brand-Saberi, B. Hyaluronan in the nuchal skin of chromosomally abnormal fetuses. Hum. Reprod. 2000, 15, 1155–1158. [Google Scholar] [CrossRef][Green Version]
- Souka, A.P.; Skentou, H.; Geerts, L.; Bower, S.; Nicolaides, K.H. Congenital nephrotic syndrome presenting with increased nuchal translucency in the first trimester. Prenat. Diagn. Publ. Affil. Int. Soc. Prenat. Diagn. 2002, 22, 93–95. [Google Scholar] [CrossRef]
- Sebire, N.J.; Bianco, D.; Snijders, R.J.M.; Zuckerman, M.; Nicolaides, K.H. Increased fetal nuchal translucency thickness at 10–14 weeks: Is screening for maternal–fetal infection necessary? BJOG Int. J. Obstet. Gynaecol. 1997, 104, 212–215. [Google Scholar] [CrossRef]
- Bilardo, C.M.; Pajkrt, E.; De Graaf, I.; Mol, B.W.; Bleker, O.P. Outcome of fetuses with enlarged nuchal translucency and normal karyotype. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 1998, 11, 401–406. [Google Scholar] [CrossRef]
- Mula, R.; Goncé, A.; Bennásar, M.; Arigita, M.; Meler, E.; Nadal, A.; Sánchez, A.; Botet, F.; Borrell, A. Increased nuchal translucency and normal karyotype: Perinatal and pediatric outcomes at 2 years of age. Ultrasound Obstet. Gynecol. 2012, 39, 34–41. [Google Scholar] [CrossRef]
- Saldanha, F.A.T.; Brizot, M.d.L.; Moraes, E.A.d.; Lopes, L.M.; Zugaib, M. Increased fetal nuchal translucency thickness and normal karyotype: Prenatal and postnatal follow-up. Rev. Da Assoc. Médica Bras. 2009, 55, 575–580. [Google Scholar] [CrossRef]
- Ozyuncu, O.; Tanacan, A.; Fadiloglu, E.; Unal, C.; Ziyadova, G.; Deren, O. Impact of Increased Nuchal Translucency Values on Pregnancy Outcomes: A Tertiary Center Experience. Fetal Pediatr. Pathol. 2021, 40, 189–197. [Google Scholar] [CrossRef]
- Becker, R.; Keller, T.; Wegner, R.-D.; Neitzel, H.; Stumm, M.; Knoll, U.; Stärk, M.; Fangerau, H.; Bittles, A. Consanguinity and pregnancy outcomes in a multi-ethnic, metropolitan European population. Prenat. Diagn. 2015, 35, 81–89. [Google Scholar] [CrossRef][Green Version]
- Pajkrt, E.; Mol, B.W.J.; Bleker, O.P.; Bilardo, C.M. Pregnancy outcome and nuchal translucency measurements in fetuses with a normal karyotype. Prenat. Diagn. Publ. Affil. Int. Soc. Prenat. Diagn. 1999, 19, 1104–1108. [Google Scholar] [CrossRef]
- Westin, M.; Saltvedt, S.; Almström, H.; Grunewald, C.; Valentin, L. By how much does increased nuchal translucency increase the risk of adverse pregnancy outcome in chromosomally normal fetuses? A study of 16,260 fetuses derived from an unselected pregnant population. Ultrasound Obstet. Gynecol. 2007, 29, 150–158. [Google Scholar] [CrossRef]
- Blair, I.; Sharif, A.A. Population structure and the burden of disease in the United Arab Emirates. J. Epidemiol. Glob. Health 2012, 2, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Bilardo, C.M.; Timmerman, E.; Pajkrt, E.; Van Maarle, M. Increased nuchal translucency in euploid fetuses—What should we be telling the parents? Prenat. Diagn. Publ. Affil. Int. Soc. Prenat. Diagn. 2010, 30, 93–102. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Control | Study | p-Value | |||
|---|---|---|---|---|---|
| N = 370 | N = 109 | ||||
| Age | 32.28 | ±5.094 | 33.78 | ±6.139 | 0.0077 |
| BMI (kg/m2) | 28.06 | ±5.726 | 27.14 | ±4.594 | 0.2466 |
| Parity | |||||
| <4 | 245 | 66.2% | 73 | 67.0% | 0.883 |
| ≥4 | 125 | 33.8% | 36 | 33.0% | |
| Type of Conception | |||||
| Assisted | 10 | 2.7% | 1 | 0.9% | 0.273 |
| Spontaneous | 359 | 97.3% | 108 | 99.1% | |
| Consanguinity | 0.650 | ||||
| No | 235 | 63.7% | 72 | 66.1% | |
| Yes | 134 | 36.3% | 37 | 33.9% | |
| Consanguinity Group | 0.643 | ||||
| None | 235 | 63.7% | 72 | 66.1% | |
| First-degree cousin | 104 | 28.5% | 32 | 29.4% | |
| Second-degree cousin | 26 | 7.1% | 5 | 4.6% | |
| CRL (mm) | 64.58 | ±8.719 | 64.63 | ±10.99 | 0.9507 |
| NT (mm) | 1.747 | ±0.306 | 4.368 | ±1.932 | <0.0001 |
| Control | Study | p-Value | |||
|---|---|---|---|---|---|
| Second Trimester Scan Result | N = 364 | N = 103 | <0.001 | ||
| Abnormal | 7 | 1.9% | 29 | 28.2% | |
| Normal | 357 | 98.1% | 74 | 71.8% | |
| Miscarriage (Before 22 weeks) | N = 370 | N = 109 | <0.001 | ||
| No | 366 | 98.9% | 99 | 90.8% | |
| Yes | 4 | 1.1% | 10 | 9.2% | |
| Foetal Demise (After 22 weeks) | N = 370 | N = 109 | 0.001 | ||
| No | 370 | 100.0% | 106 | 97.2% | |
| Yes | 0 | 0.0% | 3 | 2.8% | |
| Spontaneous Preterm Birth | N = 370 | N = 109 | 0.020 | ||
| No | 352 | 95.1% | 97 | 89.0% | |
| Yes | 18 | 4.9% | 12 | 11.0% | |
| Termination of Pregnancy | N = 370 | N = 109 | <0.001 | ||
| No | 370 | 100% | 105 | 96.3% | |
| Yes | 0 | 0% | 4 | 3.7% |
| Control | Study | p-Value | |||
|---|---|---|---|---|---|
| Live Birth | N = 370 | N = 109 | <0.001 | ||
| No | 22 | 5.9% | 28 | 25.7% | |
| Yes | 348 | 94.1% | 81 | 74.3% | |
| Still Birth | N = 370 | N = 109 | |||
| No | 370 | 100% | 104 | 96.3% | <0.001 |
| Yes | 0 | 0% | 4 | 3.7% | |
| Birth Weight Percentile | N = 365 | N = 91 | 0.444 | ||
| ≤10th | 53 | 14.5% | 16 | 17.6% | |
| 11–89th | 303 | 83.0% | 71 | 78.0% | |
| ≥90th | 9 | 2.5% | 4 | 4.4% | |
| Z Score | N = 365 | N = 91 | 0.671 | ||
| Severely growth restricted | 82 | 22.5% | 23 | 25.3% | |
| Moderately growth restricted | 163 | 44.7% | 36 | 39.6% | |
| Normal | 120 | 32.9% | 32 | 35.2% | |
| Apgar (1 min) | N = 365 | N = 91 | <0.001 | ||
| <7 | 5 | 1.4% | 8 | 8.8% | |
| ≥7 | 360 | 98.6% | 83 | 91.2% | |
| Apgar (5 min) | N = 366 | N = 91 | 0.064 | ||
| <7 | 3 | 0.8% | 3 | 3.3% | |
| ≥7 | 363 | 99.2% | 88 | 96.7% | |
| Congenital Structural Anomalies | N = 366 | N = 100 | <0.001 | ||
| No | 354 | 96.7% | 79 | 79.0% | |
| Yes | 12 | 3.3% | 21 | 21.0% |
| 95% CI. | ||||
|---|---|---|---|---|
| Odds Ratio | Lower | Upper | p-Value | |
| Age | 1.034 | 0.959 | 1.115 | 0.387 |
| BMI | 0.960 | 0.894 | 1.031 | 0.265 |
| Parity | 1.786 | 0.761 | 4.193 | 0.183 |
| NT (mm) | 1.382 | 1.116 | 1.710 | 0.003 |
| Consanguinity | 1.181 | 0.539 | 2.588 | 0.678 |
| 2nd trimesters scan (normal) | 0.135 | 0.051 | 0.360 | <0.001 |
| Constant | 0.162 | 0.253 | ||
| Correlation Coefficient | p-Value | |
|---|---|---|
| Age | 0.92 * | 0.045 |
| BMI (kg/m2) | −0.033 | 0.468 |
| Parity | 0.061 | 0.185 |
| NT (mm) | 0.201 * | <0.001 |
| Consanguinity | 0.002 | 0.972 |
| 2nd-trimester scan (normal) | −0.364 * | <0.001 |
| Correlation Coefficient | p-Value | |
|---|---|---|
| Age | −0.013 | 0.775 |
| BMI (kg/m2) | 0.037 | 0.436 |
| Parity | −0.026 | 0.582 |
| NT (mm) | 0.147 * | 0.002 |
| Consanguinity | 0.041 | 0.377 |
| 2nd-trimester scan (normal) | −0.331 * | <0.001 |
| Birth Weight (g) | −0.156 * | <0.001 |
| Apgar 1 min | −0.278 * | <0.001 |
| Apgar 5 min | −0.104 * | 0.026 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khair, H.; Hilary, S.; Al Awar, S.; Zareba, K.; Maki, S.; Sayed, G.; Mutare, S.; El-Hattab, A.W.; Al Ibrahim, A.H. Perinatal Outcomes in Foetuses with Increased Nuchal Translucency and Normal Karyotype: A Retrospective Cohort Study from the United Arab Emirates. J. Clin. Med. 2023, 12, 6358. https://doi.org/10.3390/jcm12196358
Khair H, Hilary S, Al Awar S, Zareba K, Maki S, Sayed G, Mutare S, El-Hattab AW, Al Ibrahim AH. Perinatal Outcomes in Foetuses with Increased Nuchal Translucency and Normal Karyotype: A Retrospective Cohort Study from the United Arab Emirates. Journal of Clinical Medicine. 2023; 12(19):6358. https://doi.org/10.3390/jcm12196358
Chicago/Turabian StyleKhair, Howaida, Serene Hilary, Shamsa Al Awar, Kornelia Zareba, Sara Maki, Gehan Sayed, Sharon Mutare, Ayman W. El-Hattab, and Ali Hussein Al Ibrahim. 2023. "Perinatal Outcomes in Foetuses with Increased Nuchal Translucency and Normal Karyotype: A Retrospective Cohort Study from the United Arab Emirates" Journal of Clinical Medicine 12, no. 19: 6358. https://doi.org/10.3390/jcm12196358
APA StyleKhair, H., Hilary, S., Al Awar, S., Zareba, K., Maki, S., Sayed, G., Mutare, S., El-Hattab, A. W., & Al Ibrahim, A. H. (2023). Perinatal Outcomes in Foetuses with Increased Nuchal Translucency and Normal Karyotype: A Retrospective Cohort Study from the United Arab Emirates. Journal of Clinical Medicine, 12(19), 6358. https://doi.org/10.3390/jcm12196358