1. Introduction
Classically located within 2–7 cm of its distal insertion on the calcaneus [
1], tears of the Achilles tendon (AT), the strongest tendon in the human body [
2], are frequently not diagnosed in a timely fashion, and a rupture with a delay in diagnosis or treatment for more than 6 weeks is considered a chronic tear [
1].
Tendon transfer procedures can be used in Achilles tendinopathy and chronic ruptures [
3,
4]. Various techniques have been described for AT reconstruction and augmentation, including local tendon transfers (flexor hallucis longus, peroneus brevis, flexor digitorum longus, and peroneus longus) and grafts (autograft, allograft, and synthetic graft) [
5].
The transfer of the flexor hallucis longus (FHL) tendon was first described by Hansen in 1991 [
6]. Several modifications have been described since, including single or double incisions, short or long transfer, different methods of fixation, and an open or endoscopic approach, and it is now the most commonly published technique to reconstruct a chronic tear [
4]. This procedure has several advantages: the FHL tendon is easy to harvest given its proximity to the AT and can be harvested with small incisions, minimizing the risk of neurovascular injury and wound healing complications [
4]. Transfer of the peroneus brevis (PB) tendon was popularized by Perez-Teuffer in 1974 [
7]. PB is suitable for patients with a tendon gap inferior to 6 cm and has a low rate of wound healing complications [
8]. The transfer of the flexor digitorum longus (FDL) tendon was described by Mann et al. in 1991 [
9]. It is an alternative in the treatment of these injuries, with low complications and donor site morbidity [
10]. Transfers of the peroneus longus (PL) tendon have also been reported but are less commonly used in clinical practice [
11]. The choice of the optimal technique is still debated, and no consensus has been reached. The present study analyzes in a systematic fashion the differences between the various local tendon transfers in the management of chronic Achilles tendon ruptures, evaluating clinical outcomes, complications, and return to sport.
2. Material and Methods
2.1. Search Strategy
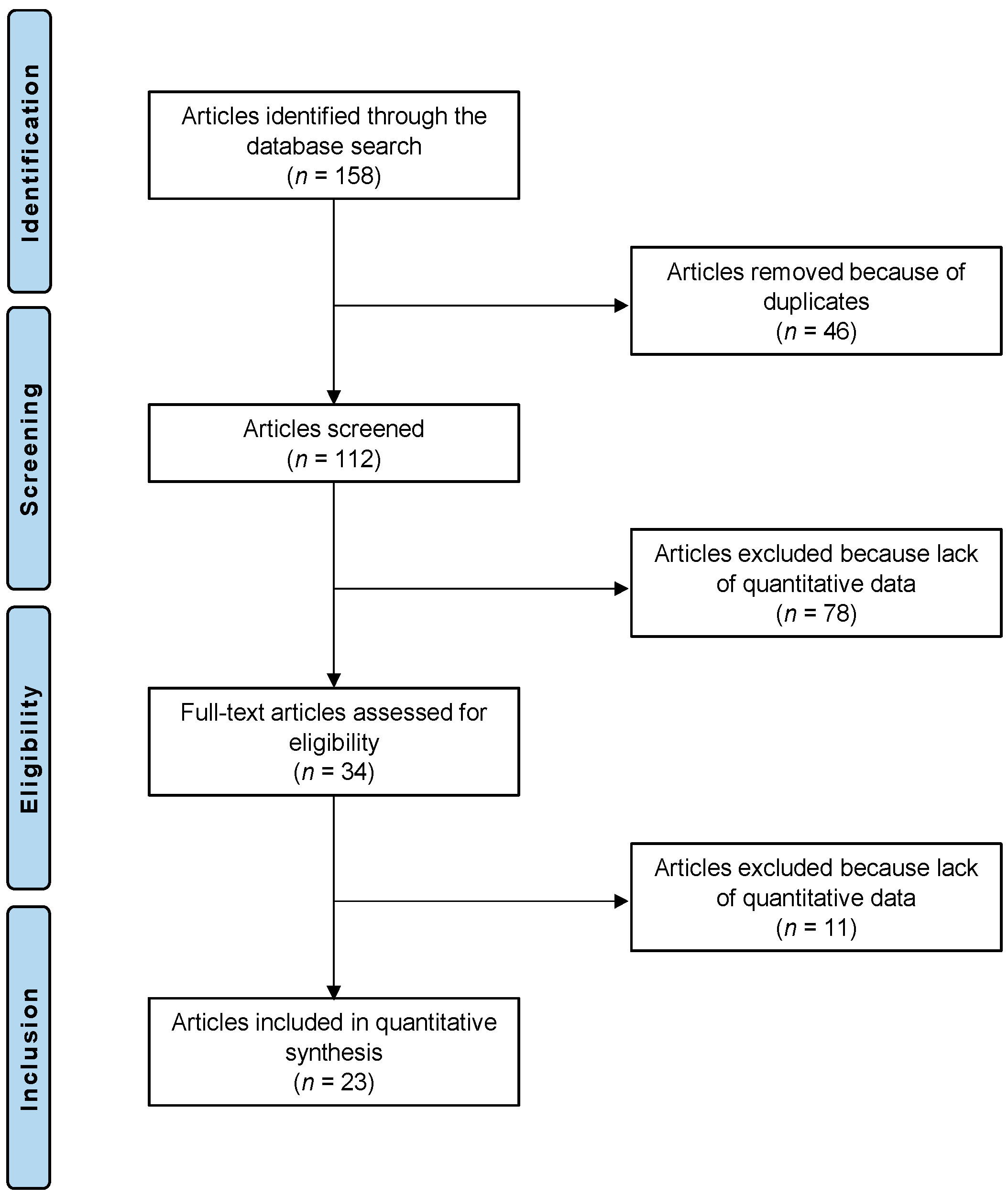
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the 2020 PRISMA statement [
12]. It was registered on the International Prospective Register of Systematic Reviews (PROSPERO; Registration No. CRD42022384213).
2.2. Eligibility Criteria
All the prospective and retrospective studies reporting local tendon transfer for the management of chronic Achilles tendon tears were accessed. According to the authors language capabilities, articles in English, Italian, German, and Spanish were eligible. Reviews, opinions, letters, and editorials were not considered. Animal, biomechanics, computational, and cadaveric studies were not eligible.
The PICOT algorithm was preliminarily pointed out:
P (Problem): Chronic rupture of the mid-portion Achilles tendon;
I (Intervention): Transfer;
C (Comparison): FHL, PB, FDL, and PL tendon transfers;
O (Outcomes): Clinical outcomes, complications, and return to sport;
T (Timing): ≥6 months of follow-up.
In November 2022, PubMed, Web of Science, Google Scholar, and Embase databases were accessed. No time constraints were used for the search. The following keywords were used in combination: Achilles tendon, tendon transfer, mid-portion Achilles chronic ruptures, mid portion Achilles rupture, main body Achilles rupture, main body Achilles chronic rupture.
2.3. Selection and Data Collection
Two authors independently performed the database search. All the resulting titles were screened, and if suitable, the abstracts were accessed. The full text of the abstracts that matched the topic of interest was accessed. The bibliography of the full-text articles was also screened by hand to identify other eligible articles for inclusion. Disagreements were debated, and the final decision was made by a third senior author.
2.4. Methodological Quality Assessment
Two authors independently performed the methodological quality assessment using the Coleman Methodology Score (CMS). The CMS is a 10 item scale designed to rate the methodological quality of the included studies [
13]. These items evaluated study size, mean follow-up, number of surgical procedures, type of study, diagnostic certainty, description of surgical procedure, postoperative rehabilitation, outcome measures, outcome assessment, and selection process. The final score ranges between 0 and 100, with a score of 100 indicating the highest reported methodological quality [
13]. (
Table 1 and
Table 2).
2.5. Data items
Two authors independently performed data extraction. The following data were extracted: generalities (author, year, and type of study), demographic baseline (number of samples and mean age), mean follow-up, mean BMI, and surgical intervention (FHL transfer and PB transfer). The primary outcome of interest was the clinical outcome: the Visual Analogue Scale (VAS), the American Orthopaedic Foot and Ankle Society (AOFAS), and the Achilles tendon Total Rupture Score (ATRS). The secondary outcome of interest was complications. The third outcome of interest was a return to sports.
2.6. Outcomes
The scales used to evaluate clinical outcome were the VAS, AOFAS, and ATRS.
In 1921, Hayes and Patterson introduced the Visual Analogue Scale (VAS) as a pain rating scale [
34], measuring the frequency and intensity of pain. It consists of a 10 cm line, the left end of which represents a state of “no pain”, while the right one represents “the worst pain”. The patients mark on the line the point that matches their perception of their current state [
35].
The American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Score combined a clinical reported (developed by Kitaoka et al. in 1994 [
36]) and a patient reported part to evaluate the outcome of treatment in patients with ankle or hindfoot injury. This rating system is divided into three categories: pain (40 points), function (50 points), and alignment (10 points), with nine questions in each for a total of 100 points. Zero stands for severe pain or impairment; 100 for no pain. Though widely used, the AOFAS score has not been validated.
The Achilles tendon Total Rupture Score (ATRS) measures the outcome related to symptoms and physical activity after treatment in patients with total AT rupture. The scale ranged from 0 = major limitations/symptoms to 100 = no limitations/symptoms and has now been cross-culturally validated in several languages [
37]. To date, only the ATRS is a condition-specific PROM.
2.7. Statistical Analysis
The statistical analysis was performed using IBM SPSS version 25. Mean and standard deviation were used for descriptive statistics. For continuous variables, the mean difference effect measure was used. The paired t-test was used with values of p < 0.05 considered statistically significant.
4. Discussion
Several local tendon transfers have been described, but the tendons most commonly used in transfers for chronic ruptures of the Achilles tendon are those of the FHL and PB.
The transfer of the flexor hallucis longus (FHL) tendon is the most reported, carrying, at least theoretically, a series of advantages over other local tendon transfers:
The FHL is the second strongest plantar flexor muscle of the ankle;
Its axis of action is in line with that of the AT;
It maintains normal ankle muscle balance;
Its harvest carries a low risk of iatrogenic neurovascular injury;
It increases the vascularity of the reconstruction given its low-lying muscle belly [
32].
A potential undesired effect of FHL harvest is the loss of plantar flexion of the interphalangeal joint of the hallux, with decreased plantar flexion and push-off strength [
5]. However, despite the weakness of plantar flexion of the hallux, most patients do not report noticeable deformities or weakness and resume their pre-injury daily activities [
14].
The morbidity associated with FHL tendon transfer seems not to be clinically relevant, even in running sports that require good push-off or balance [
5].
In the present systematic review, the rate of complications following the use of FHL transfers is 14.8%. Of the 338 patients, the major complications were one deep vein thrombosis, four deep infections, and one re-rupture [
17] (
Table 5).
The tendon of the peroneus brevis (PB) is well vascularized. The transfer allows the blood supply from the musculotendinous junction to be maintained, providing a robust reinforcement to the AT [
38].
The two peroneal muscles contribute only 4% of the capacity for plantar flexion, while the PB tendon contributes approximately 28% of the total eversion strength [
38]. Intuitively, the use of the PB tendon may cause a strength deficit in eversion of the ankle and not affect plantar flexion [
30]. The peroneus longus is the major evertor of the hindfoot, and it may take over some of the functions of the PB, reducing subjective weakness in ankle function after PB tendon transfer [
39]. Human cadaveric models have been used to assess the mechanical properties of AT reconstruction with the PB and FHL [
40]. The outcomes were similar in terms of stiffness (16.5 ± 6.3 N/mm (PB) vs. 14.0 ± 3.8 N/mm (FHL)), energy to failure (3656.0 ± 2720.3 J (PB) vs. 2406.7 ± 1621.8 J (FHL)), and mode of failure. The force to failure of the PB tendon transfer was higher compared to the FHL (348.8 ± 124.9 N (PB) vs. 241.5 ±8 2.2 N (FHL)), and this difference was statistically significant, although it may not be clinically relevant. The authors of [
40] reported good clinical results in the use of PB, with a final ATRS of 92.5 associated with a low rate of complications. In fact, patients did not experience deep vein thrombosis nor re-rupture, and five superficial infections were managed with oral antibiotics [
8].
The present systematic review reported a rate of complications in the use of PB tendon transfer of 7% in 128 patients, five of whom experienced superficial infections and four wound complications (
Table 5). Due to the lack of relevant data, it was not possible to directly compare the complications of FHL and PB or to analyse which surgical technique leads to a higher rate of complications.
The return to daily activities and the return to sport were only reported in three and four studies, respectively; seventy-nine and ninety-nine patients were evaluated; patients were able to return to daily activities in 13.7 weeks and return to sport in 19.6 weeks. Maffulli et al. reported a slower return to sport in PB tendon transfer patients compared to FHL transfer patients, but a higher percentage of PB transfer patients eventually returned to sport compared to FHL transfer patients [
25].
The use of flexor digitorum longus (FDL) tendon transfer has been described in two reports; however, these were excluded since they described its use in the management of Achilles tendinopathy. The FDL tendon transfer is an alternative operative technique that keeps the FHL tendon intact, preserves push-off strength, and minimizes gait disturbances [
10]. However, De Cesar Netto et al. reported a patient with weakness of plantar flexion of the lesser toes, without balance or gait disturbances [
10]. In addition to the transfer of the tendon of the FDL, they also performed a turndown of the central third of the proximal aspect of the AT or a hamstring allograft reconstruction [
10].
The peroneal longus (PL) tendon has a stronger failure load than the tendon of the PB [
11]. However, the use of the PL tendon may cause a long-lasting strength deficit in eversion of the ankle, especially at a higher angular velocity, more evident than in the transfer of the PB [
38].
This study has several limitations. First, the retrospective design and the lack of blinding in most of the included studies. Given the lack of quantitative data available for inclusion, it was not possible to analyze the results of each transfer separately. Moreover, we excluded several studies because most of them did not separate data on patients with chronic AT rupture from patients with Achilles tendinopathy and acute AT rupture, while others did not differentiate mid-portion ruptures from ruptures of the insertion of the AT. Furthermore, the inhomogeneity of the evaluation scales prevents an adequate comparison between the studies. Given the lack of relevant quantitative data, further subgroup analyses were not possible. Further investigations are required to validate the results of the present study in a clinical setting.


 ,
, 




{kind=link}