
The Urinary Concentrations of Neutrophil Gelatinase-Associated Lipocalin, Cystatin C and Osteopontin in the Healthy Term and Stable Preterm Neonates: A Pilot Study

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Recruitment
2.2. Sample Collection
2.3. Determination of Basic Blood and Urine Parameters
2.4. Determination of the Urinary Concentration of Osteopontin, Cystatin C, and NGAL in the Urine
- For the assessment of osteopontin: working range—3.80–2000.00 ng/mL; sensitivity—1.70 ng/mL; intra-assay coefficient of variation—6%; and inter-assay coefficient of variation—12%;
- For the assessment of cystatin C: working range—0.16–40.00 ng/mL; sensitivity—0.077 ng/mL; intra-assay coefficient of variation—3%; and inter-assay coefficient of variation—20%;
- For the assessment of NGAL: working range—0.062–34.00 ng/mL; sensitivity—0.052 ng/mL; intra-assay coefficient of variation—6%; and inter-assay coefficient of variation—12%.
2.5. Determination of the Values of Osteopontin/cr., Cystatin C/cr., NGAL/cr. Ratios
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Group Comprising Term Neonates
3.2. Characteristics of the Group Comprising Preterm Neonates
3.3. The Analysis of the Parameters of Renal Function
3.4. The Analysis of the Concentrations of NGAL and the Values of NGAL/cr. Ratio
3.5. The Analysis of the Concentrations of Cystatin C and the Values of Cystatin C/cr. Ratio
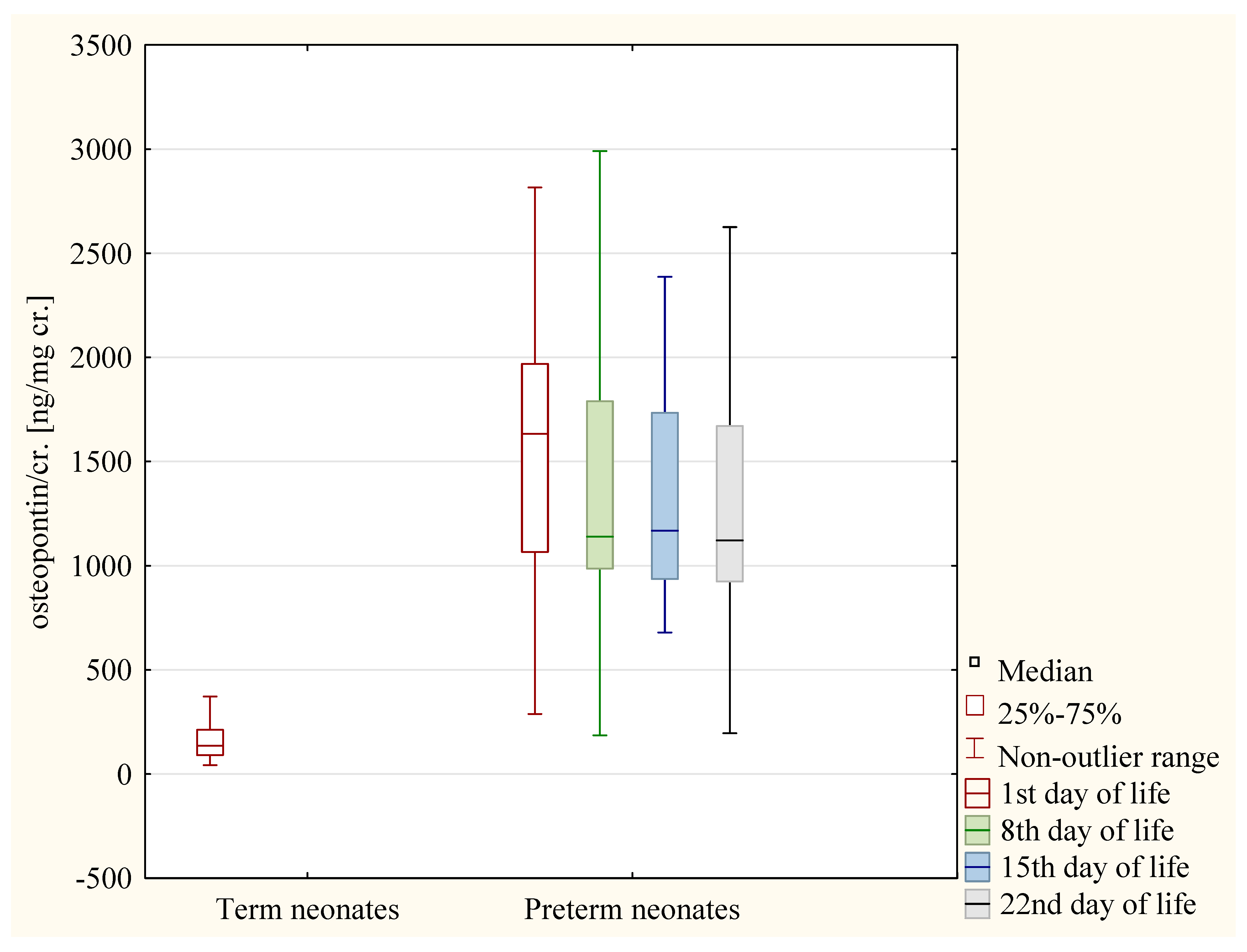
3.6. The Analysis of the Values of Osteopontin/cr. Ratio
3.7. The Analysis of the Correlations
- The value of the osteopontin/cr. ratio and value of the cystatin C/cr. ratio (R = 0.42, p < 0.01);
- The value of the cystatin C/cr. ratio and the value of the NGAL/cr. ratio (R = 0.39, p < 0.01).
3.8. The Analysis of 95% CI for the Biomarkers of Renal Function in Term Neonates
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Allegaert, K.; Smits, A.; Van Donge, T.; van den Anker, J.; Sarafidis, K.; Levtchenko, E.; Mekahli, D. Renal Precision Medicine in Neonates and Acute Kidney Injury: How to Convert a Cloud of Creatinine Observations to Support Clinical Decisions. Front. Pediatr. 2020, 8, 366. [Google Scholar] [CrossRef] [PubMed]
- Kastl, J.T. Renal function in the fetus and the neonate—The creatinine enigma. Semin. Fetal Neonatal Med. 2017, 22, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Schreuder, M.F.; Bueters, R.R.; Allegaert, K. The interplay between drugs and the kidney in premature neonates. Pediatr. Nephrol. 2014, 29, 2083–2091. [Google Scholar] [CrossRef] [PubMed]
- Modi, N.; Hutton, J.L. Urinary creatinine excretion and estimation of muscle mass in infants of 25–34 weeks gestation. Acta Paediatr. Scand. 1990, 79, 1156–1162. [Google Scholar] [CrossRef]
- Kamianowska, M.; Szczepański, M.; Wasilewska, A. Tubular and Glomerular Biomarkers of Acute Kidney Injury in Newborns. Curr. Drug Metab. 2019, 20, 332–349. [Google Scholar] [CrossRef]
- Hudkins, K.L.; Giachelli, C.M.; Cui, Y.; Couser, W.G.; Johnson, R.J.; Alpers, C.E. Osteopontin expression in fetal and mature human kidney. J. Am. Soc. Nephrol. 1999, 10, 444–457. [Google Scholar] [CrossRef]
- Kaleta, B. The role of osteopontin in kidney diseases. Inflamm. Res. 2019, 68, 93–102. [Google Scholar] [CrossRef]
- Yu, X.Q.; Wu, L.L.; Huang, X.R.; Yang, N.; Gilbert, R.E.; Cooper, M.E.; Johnson, R.J.; Lai, K.N.; Lan, H.Y. Osteopontin expression in progressive renal injury in remnant kidney: Role of angiotensin II. Kidney Int. 2000, 58, 1469–1480. [Google Scholar] [CrossRef]
- Westhuyzen, J. Cystatin C: A promising marker and predictor of im paired renal function. Ann. Clin. Lab. Sci. 2006, 36, 387–394. [Google Scholar]
- Ferguson, T.W.; Komenda, P.; Tangri, N. Cystatin C as a biomarker for estimating glomerular filtration rate. Curr. Opin. Nephrol. Hypertens. 2015, 24, 295–300. [Google Scholar] [CrossRef]
- Mussap, M.; Plebani, M. Biochemistry and clinical role of human cystatin C. Crit. Rev. Clin. Lab. Sci. 2004, 41, 467–550. [Google Scholar] [CrossRef]
- Park, M.Y.; Choi, S.J.; Kim, J.K.; Hwang, S.D.; Lee, Y.W. Urinary cystatin C levels as a diagnostic and prognostic biomarker in patients with acute kidney injury. Nephrology 2013, 18, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Marakala, V. Neutrophil gelatinase-associated lipocalin (NGAL) in kidney injury—A systematic review. Clin. Chim. Acta 2022, 536, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Ott, K.M. Neutrophil gelatinase-associated lipocalin as a biomarker of acute kidney injury—Where do we stand today? Nephrol. Dial. Transplant. 2011, 26, 762–764. [Google Scholar] [CrossRef] [PubMed]
- Devarajan, P.; Ronco, C.; Bellomo, R.; Kellum, J.A. Acute Kidney Injury. Contrib. Nephrol. 2007, 156, 203–212. [Google Scholar]
- Bolignano, D.; Donato, V.; Coppolino, G.; Campo, S.; Buemi, A.; Lacquaniti, A.; Buemi, M. Neutrophil Gelatinase–Associated Lipocalin (NGAL) as a Marker of Kidney Damage. Am. J. Kidney Dis. 2008, 52, 595–605. [Google Scholar] [CrossRef]
- Mori, K.; Lee, H.T.; Rapoport, D.; Drexler, I.R.; Foster, K.; Yang, J.; Schmidt-Ott, K.M.; Chen, X.; Li, J.Y.; Weiss, S.; et al. Endocytic delivery of lipocalin-siderophore-iron complex rescues the kidney from ischemia-reperfusion injury. J. Clin. Investig. 2005, 115, 610–621. [Google Scholar] [CrossRef]
- Mori, K.; Nakao, K. Neutrophil gelatinase-associated lipocalin as the real-time indicator of active kidney damage. Kidney Int. 2007, 71, 967–970. [Google Scholar] [CrossRef]
- Pan, J.J.; Sun, Z.Y.; Zhou, X.Y.; Hu, Y.H.; Cheng, R.; Chen, X.Q.; Yang, Y. Is neutrophil gelatinase-associated lipocalin a good diagnostic marker for renal injury in asphyxiated preterm infants? J. Res. Med. Sci. 2018, 23, 90. [Google Scholar]
- Koyner, J.L.; Bennett, M.R.; Worcester, E.M.; Ma, Q.; Raman, J.; Jeevanandam, V.; Kasza, K.E.; O’Connor, M.F.; Konczal, D.J.; Trevino, S.; et al. Urinary cystatin C as an early biomarker of acute kidney injury following adult cardiothoracic surgery. Kidney Int. 2008, 74, 1059–1069. [Google Scholar] [CrossRef]
- Askenazi, D.J.; Montesanti, A.; Hunley, H.; Koralkar, R.; Pawar, P.; Shuaib, F.; Liwo, A.; Devarajan, P.; Ambalavanan, N. Urine biomarkers predict acute kidney injury and mortality in very low birth weight infants. J. Pediatr. 2011, 159, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Sarafidis, K.; Tsepkentzi, E.; Agakidou, E.; Diamanti, E.; Taparkou, A.; Soubasi, V.; Papachristou, F.; Drossou, V. Serum and urine acute kidney injury biomarkers in asphyxiated neonates. Pediatr. Nephrol. 2012, 27, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- Brott, D.; Adler, S.H.; Arani, R.; Lovick, S.C.; Pinches, M.; Furlong, S.T. Characterization of renal biomarkers for use in clinical trials: Biomarker evaluation in healthy volunteers. Drug Des. Dev. Ther. 2014, 8, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Askenazi, D.J.; Koralkar, R.; Patil, N.; Halloran, B.; Ambalavanan, N.; Griffin, R. Acute Kidney Injury Urine Biomarkers in Very Low-Birth-Weight Infants. Clin. J. Am. Soc. Nephrol. 2016, 11, 1527–1535. [Google Scholar] [CrossRef]
- Barbati, A.; Cappuccini, B.; Aisa, M.C.; Grasselli, C.; Zamarra, M.; Bini, V.; Bellomo, G.; Orlacchio, A.; Di Renzo, G.C. Increased Urinary Cystatin-C Levels Correlate with Reduced Renal Volumes in Neonates with Intrauterine Growth Restriction. Neonatology 2016, 109, 154–160. [Google Scholar] [CrossRef]
- DeFreitas, M.J.; Seeherunvong, W.; Katsoufis, C.P.; RamachandraRao, S.; Duara, S.; Yasin, S.; Zilleruelo, G.; Rodriguez, M.M.; Abitbol, C.L. Longitudinal patterns of urine biomarkers in infants across gestational ages. Pediatr. Nephrol. 2016, 31, 1179–1188. [Google Scholar] [CrossRef]
- Khosravi, N.; Zadkarami, M.; Chobdar, F.; Hoseini, R.; Khalesi, N.; Panahi, P.; Karimi, A. The Value of Urinary Cystatin C Level to Predict Neonatal Kidney Injury. Curr. Pharm. Des. 2018, 24, 3002–3004. [Google Scholar] [CrossRef]
- Sridharan, K.; Al Jufairi, M.; Al Segai, O.; Al Ansari, E.; Ahmed, H.H.; Shaban, G.H.; Malalla, Z.; Al Marzooq, R.; Al Madhoob, A.; Tabbara, K.S. Biomarkers in neonates receiving potential nephrotoxic drugs. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7078–7088. [Google Scholar]
- Li, B.; Zamzam, A.; Syed, M.H.; Jahanpour, N.; Jain, S.; Abdin, R.; Qadura, M. Urinary Cystatin C Has Prognostic Value in Peripheral Artery Disease. Biomolecules 2022, 12, 860. [Google Scholar]
- Coskun, Y.; Demirel, O.U.; Bayram, T.; Akman, I.; Hacihamdioglu, D.O. Estimating glomerular filtration rate via cystatin-C in preterm infants: A comparative analysis. Paediatr. Indones. 2022, 62, 223–231. [Google Scholar] [CrossRef]
- Wasilewska, A.; Taranta-Janusz, K.; Kuroczycka-Saniutycz, E.; Zwierz, W.Z. Urinary OPN excretion in children with glomerular proteinuria. Adv. Med. Sci. 2011, 56, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Al-Malki, A.L. Assessment of urinary osteopontin in association with podocyte for early predication of nephropathy in diabetic patients. Dis. Markers 2014, 2014, 493736. [Google Scholar] [CrossRef] [PubMed]
- Miklaszewska, M.; Korohoda, P.; Drożdż, D.; Zachwieja, K.; Tomasik, T.; Moczulska, A.; Korzeniecka-Kozerska, A.; Kwinta, P. eGFR values and selected renal urine biomarkers in preterm neonates with uncomplicated clinical course. Adv. Clin. Exp. Med. 2019, 28, 1657–1666. [Google Scholar] [CrossRef] [PubMed]
- Suchojad, A.; Tarko, A.; Smertka, M.; Majcherczyk, M.; Brzozowska, A.; Wroblewska, J.; Maruniak-Chudek, I. Factors limiting usefulness of serum and urinary NGAL as a marker of acute kidney injury in preterm newborns. Ren. Fail. 2015, 37, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-N.; Chou, C.-H.; Jeng, S.-F.; Tsai, I.-J.; Chen, P.-C.; Chen, C.-Y.; Chou, H.-C.; Tsao, P.-N.; Hsieh, W.-S. Urinary neutrophil gelatinase-associated lipocalin levels in neonates. Pediatr. Neonatol. 2016, 57, 207–212. [Google Scholar] [CrossRef]
- Kamianowska, M.; Wasilewska, A.; Szczepański, M.; Kulikowska, E.; Bebko, B.; Koput, A. Health term-born girls had higher levels of urine neutrophil gelatinase-associated lipocalin than boys during the first postnatal days. Acta Paediatr. 2016, 105, 1105–1108. [Google Scholar] [CrossRef]
- De Mul, A.; Parvex, P.; Wilhelm-Bals, A. Neutrophil gelatinase-associated lipocalin distribution in preterm newborns without acute kidney injury as defined by a reference method. J. Matern. Fetal Neonatal Med. 2022, 35, 4956–4960. [Google Scholar] [CrossRef]
- Galteau, M.M.; Guyon, M.; Gueguen, R.; Siest, G. Determination of serum cystatin C: Biological variation and reference values. Clin. Chem. Lab. Med. 2001, 39, 850–857. [Google Scholar] [CrossRef]
- Trostel, J.; Truong, L.D.; Roncal-Jimenez, C.; Miyazaki, M.; Miyazaki-Anzai, S.; Kuwabara, M.; McMahan, R.; Andres-Hernando, A.; Sato, Y.; Jensen, T.; et al. Different effects of global osteopontin and macrophage osteopontin in glomerular injury. Am. J. Physiol. Ren. Physiol. 2018, 315, F759–F768. [Google Scholar] [CrossRef]
- Xie, Y.; Sakatsume, M.; Nishi, S.; Narita, I.; Arakawa, M.; Gejyo, F. Expression, roles, receptors, and regulation of osteopontin in the kidney. Kidney Int. 2001, 60, 1645–1657. [Google Scholar] [CrossRef]
- Krzeminska, E.; Wyczalkowska-Tomasik, A.; Korytowskam, N.; Paczekm, L. Comparison of Two Methods for Determination of NGAL Levels in Urine: ELISA and CMIA. J. Clin. Lab. Anal. 2016, 30, 956–960. [Google Scholar] [CrossRef] [PubMed]
- Parravicini, E.; Nemerofsky, S.L.; Michelson, K.A.; Huynh, T.K.; Sise, M.E.; Bateman, D.A.; Lorenz, J.M.; Barasch, J.M. Urinary neutrophil gelatinase-associated lipocalin is a promising biomarker for late onset culture-positive sepsis in very low birth weight infants. Pediatr. Res. 2010, 67, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Haase, M.; Bellomo, R.; Devarajan, P.; Schlattmann, P.; Haase-Fielitz, A.; NGAL Meta-Analysis Investigator Group. NGAL Meta-analysis Investigator Group. Accuracy of neutrophil gelatinase-associated lipocalin (NGAL) in diagnosis and prognosis in acute kidney injury: A systematic review and meta-analysis. Am. J. Kidney Dis. 2009, 54, 1012–1024. [Google Scholar] [CrossRef]
- Beghini, J.; Giraldo, P.C.; Linhares, I.M.; Ledger, W.J.; Witkin, S.S. Neutrophil Gelatinase-Associated Lipocalin Concentration in Vaginal Fluid: Relation to Bacterial Vaginosis and Vulvovaginal Candidiasis. Reprod. Sci. 2015, 22, 964–968. [Google Scholar] [CrossRef]
- Wróblewska-Seniuk, K.; Jarząbek-Bielecka, G.; Kędzia, W. Gynecological Problems in Newborns and Infants. J. Clin. Med. 2021, 10, 1071. [Google Scholar] [CrossRef] [PubMed]
- Wagner, B.D.; Accurso, F.J.; Laguna, T.A. The applicability of urinary creatinine as a method of specimen normalization in the cystic fibrosis population. J. Cyst. Fibros. 2010, 9, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Waikar, S.S.; Sabbisetti, V.S.; Bonventre, J.V. Normalization of urinary biomarkers to creatinine during changes in glomerular filtration rate. Kidney Int. 2010, 78, 486–494. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Term Neonates (N = 80) | Girls (N = 40) | Boys (N = 40) | p | |
|---|---|---|---|---|
| Median (Q1–Q3) | ||||
| Gestational age (weeks) | 39 (38–40) | 39 (39–40) | 39 (37–40) | 0.89 |
| Vaginal delivery/ Cesarean delivery | 41/39 | 22/18 | 19/21 | 0.65 |
| Anthropometric data | ||||
| Birth weight (g) | 3345 (3085–3755) | 3355 (3125–3805) | 3320 (2990–3710) | 0.66 |
| Birth weight (10th–50th percentile/ 51st–90th percentile) | 43/37 | 21/19 | 22/18 | 1.00 |
| Body length (cm) | 55 (54–57) | 55 (54–56) | 56 (54–57) | 0.49 |
| Head circumference (cm) | 34 (34–35) | 34 (34–35) | 35 (34–35) | 0.82 |
| All Preterm Neonates (N = 20) | Girls (N = 12) | Boys (N = 8) | p | |
|---|---|---|---|---|
| Median (Q1–Q3) | ||||
| Gestational age (weeks) | 30.5 (29.5–32.5) | 30.0 (28.5–31.5) | 31.0 (30.5–33.0) | 0.05 |
| Vaginal delivery/Cesarean delivery | 6/14 | 4/8 | 2/6 | 1.00 |
| Anthropometric data | ||||
| Birth weight (g) | 1600 (1220–1875) | 1305 (1200–1680) | 1875 (1600–2055) | 0.02 |
| Head circumference (cm) | 29.0 (27.5–30.5) | 29.0 (26.5–30.5) | 30.0 (29.0–32.0) | 0.10 |
| Body length (cm) | 45.0 (38.5–47.0) | 41.0 (37.5–46.5) | 46.0 (45.0–47.0) | 0.21 |
| Term Neonates | ||||
|---|---|---|---|---|
| Parameters | All Neonates (N = 80) | Girls (N = 40) | Boys (N = 40) | p |
| Median (Q1–Q3) | ||||
| Cystatin C/cr. (ng/mg cr.) | 7.26 (1.08–27.83) | 8.37 (1.60–30.29) | 4.31 (0.87–26.26) | 0.55 |
| Osteopontin/cr. (ng/mg cr.) | 135.86 (90.82–212.81) | 132.97 (86.57–216.83) | 138.79 (97.58–211.53) | 0.82 |
| NGAL/cr. (ng/mg cr.) | 61.48 (16.09–212.14) | 212.14 (94.74–643.90) | 27.12 (10.52–66.88) | 0.00 |
| All Preterm Neonates (N = 20) | Girls (N = 12) | Boys (N = 8) | p | |
|---|---|---|---|---|
| Median (Q1–Q3) | ||||
| 1st day of life | ||||
| Cystatin C/cr. (ng/mg cr.) | 439.49 (71.68–2580.43) | 701.02 (120.41–2906.65) | 399.75 (9.89–1630.24) | 0.34 |
| Osteopontin/cr. (ng/mg cr.) | 1633.37 (1065.31–1969.01) | 1749.04 (133.66–2014.50) | 1396.72 (654.99–1938.75) | 0.46 |
| NGAL/cr. (ng/mg cr.) | 194.59 (65.29–277.70) | 256.93 (168.13–644.88) | 65.29 (25.98–160.54) | 0.02 |
| 8th day of life | ||||
| Cystatin C/cr. (ng/mg cr.) | 41.94 (7.17–523.09) | 32.76 (5.50–523.09) | 72.21 (27.39–696.83) | 0.67 |
| Osteopontin/cr. (ng/mg cr.) | 1138.78 (985.50–1790.06) | 1334.29 (1033.66–2149.22) | 1100.65 (922.57–1318.56) | 0.23 |
| NGAL/cr. (ng/mg cr.) | 215.94 (37.66–1051.51) | 1006.35 (249.14–1427.86) | 45.96 (16.85–99.49) | 0.00 |
| 15th day of life | ||||
| Cystatin C/cr. (ng/mg cr.) | 205.52 (24.52–1270.72) | 205.52 (24.52–1562.29) | 257.02 (62.10–882.56) | 0.73 |
| Osteopontin/cr. (ng/mg cr.) | 1167.98 (935.20–1733.24) | 1345.531 (1074.78–2086.85) | 989.98 (839.99–1413.03) | 0.08 |
| NGAL/cr. (ng/mg cr.) | 231.59 (69.57–470.99) | 424.61 (249.96–657.23) | 53.16 (40.75–89.28) | 0.00 |
| 22nd day of life | ||||
| Cystatin C/cr. (ng/mg cr.) | 258.31 (53.25–372.734) | 233.20 (27.80–428.78) | 258.31 (156.58–327.42) | 0.96 |
| Osteopontin/cr. (ng/mg cr.) | 1121.38 (923.11–1670.59) | 974.93 (168.13–644.88) | 1320.22 (1077.69–2033.19) | 0.08 |
| NGAL/cr. (ng/mg cr.) | 59.60 (5.96–431.48) | 253.09 (95.21–764.86) | 5.13 (3.82–7.02) | 0.01 |
| Mean | 95% CI | |
|---|---|---|
| Cystatin C/cr. (ng/mg cr.) | 39.20 | 19.24–59.17 |
| Osteopontin/cr. (ng/mg cr.) | 195.44 | 147.92–242.77 |
| NGAL/cr. (ng/mg cr.)—boys | 58.74 | 26.97–90.50 |
| NGAL/cr. (ng/mg cr.)—girls | 1063.70 | 225.03–1902.37 |
| Authors | Year | Subjects | Results |
|---|---|---|---|
| Urinary Cystatin C | |||
| Koyner et al. [20] | 2008 | Acute kidney injury in adults undergoing cardiac surgery | Before surgery: median cystatin C/cr. ratio in patients who developed AKI after surgery and in patients who did not was similar: 50 and 60 ng/mg cr. After surgery: median cystatin C/cr. ratio in patients without AKI (290 ng/mg cr.) and was lower than in patients with AKI (1300 ng/mg cr.) (p < 0.001). |
| Askenazi et al. [21] | 2011 | Very low birth weight neonates | Median concentration of cystatin C in neonates without AKI: 2150 ng/mL. |
| Sarafidis et al. [22] | 2012 | Asphyxiated neonates and healthy term neonates | Median cystatin C/cr. ratio in healthy neonates on the 1st, 3rd, and 10th day of life: 148, 169, and 140 ng/mg cr., respectively. |
| Brott et al. [23] | 2014 | Healthy term neonates | 95% CI for the cystatin C/cr. ratio in healthy adults: 17.5–70.4 ng/mg cr. |
| Askenazi et al. [24] | 2016 | Very low birth weight neonates | Median cystatin C/cr. ratio in in neonates without AKI 7230 ng/mg cr. |
| Barbati et al. [25] | 2016 | Neonates with intrauterine growth retardation (IUGR) | Concentration of cystatin C in neonates with IUGR was significantly higher than in appropriate for gestational age children. |
| DeFreitas et al. [26] | 2016 | Preterm and term neonates | Cystatin C/cr. ratio in term neonates at birth (geometric mean, 95% CI): 210 (86, 513) ng/mg cr. Cystatin C/cr. ratio in preterm neonates at birth (geometric mean, 95% CI): 315 (195, 508) ng/mg cr. Cystatin C/cr. ratio did not change between birth and 3rd month of life. |
| Khosravi et al. [27] | 2018 | Neonates | The urinary cystatin C level could predict kidney injury and effectively discriminate kidney injury from normal kidney function (AUC = 0.868, 95% CI: 0.811–0.925, p < 0.001). |
| Sridahran et al. [28] | 2021 | Neonates receiving potentially nephrotoxic drugs | Median cystatin C/cr. ratio: 6.63 ng/mg cr. |
| Li et al. [29] | 2022 | Healthy adults | Median cystatin C/cr. ratio: 20.9 ng/mg cr. |
| Coskun et al. [30] | 2022 | Preterm neonates | Median concentration of cystatin C: on the 1st or 2nd day of life: 1600–9200 ng/mL; on the 7th day: 900–12,100 ng/mL; on the 14th day: 400–12,600 ng/mL; on the 21st day: 600–2000 ng/mL; on the 28th day: 0 ng/mL. |
| Urinary osteopontin | |||
| Wasilewska et al. [31] | 2011 | Healthy children | Median osteopontin/cr. ratio: 68.84 ng/mg cr. |
| Askenazi et al. [21] | 2011 | Preterm neonates | Median concentration of osteopontin in neonates with AKI vs. in neonates with normal renal functions: 217 vs. 468 ng/mL. |
| Al-Malki [32] | 2014 | Diabetic patients with nephropathy | The urinary level of osteopontin has a good accuracy in distinguishing between patients with nephropathy and healthy controls (AUC = 0.73, sensitivity = 92.3% and specificity = 89.9%. |
| Brott et al. [23] | 2014 | Healthy adults | 95% CI for the osteopontin/cr. ratio in healthy adults: 236–1459 ng/mg cr. |
| DeFreitas et al. [26] | 2016 | Preterm and term neonates | Osteopontin/cr. ratio in term neonates at birth (geometric mean, 95% CI): 377 (138, 1030) ng/mg cr. Osteopontin/cr. ratio in preterm neonates at birth (geometric mean, 95% CI): 670 (389, 1155) ng/mg cr. Osteopontin/cr. ratio decreased between birth and 3rd month of life. |
| Askenazi et al. [24] | 2016 | Very low birth weight neonates | Median osteopontin/cr. ratio in neonates without AKI: 4640 ng/mg cr. |
| Miklaszewska et al. [33] | 2019 | Premature children | Osteopontin/cr. ratio in LBW and VLBW neonates (geometric mean, 50%CI): in girls: 493.4 (234.4–1038.4) and 1478.9 (699.5–3126.8); in boys: 897.7 (518.9–1553.1) and 1754.8 (787.8–3908.8) ng/mg cr. Osteopontin/cr. ratio in LBW neonates was lower in the following 4 weeks of life, but the differences were not statistically significant. |
| Urinary NGAL | |||
| Askenazi et al. [21] | 2011 | Very low birth weight neonates | Median concentration of NGAL in neonates without AKI vs. in neonates with AKI: 458 vs. 985 ng/mL. |
| Sarafidis et al. [22] | 2012 | Asphyxiated neonates and healthy term neonates | Median NGAL/cr. ratio in healthy neonates on the 1st, 3rd, and 10th day of life: 14.5, 25.7, and 8 ng/mg cr. |
| Suchojad et al. [34] | 2015 | Preterm neonates without AKI | Median concentration of urinary NGAL: 144 ng/mL). |
| Askenazi et al. [24] | 2016 | Very low birth weight neonates | Median NGAL/cr. ratio in neonates without AKI: 3170 ng/mg cr. |
| Chen et al. [35] | 2016 | Term and preterm neonates | Median concentration of NGAL in term neonates on the 3rd day of life: 88.1 ng/mL. Median concentrations of NGAL in premature neonates on the 3rd, 7th, 14th, and 21st day of life were: 41.52, 35.82, 43.79, and 30.85 ng/mL, respectively (p > 0.05). |
| DeFreitas et al. [26] | 2016 | Preterm and term neonates | NGAL/cr. ratio in term neonates at birth (geometric mean, 95% CI): 335 (135, 834) ng/mg cr. NGAL/cr. ratio in preterm neonates at birth (geometric mean, 95% CI): 568 (347, 929) ng/mg cr. NGAL/cr. ratio in term neonates and preterm neonates at birth did not differ significantly (p = 0.33). NGAL/cr. ratio decreased between birth and 3rd month of life. |
| Kamianowska et. al. [36] | 2016 | Term neonates, first 48 h of life | Higher median NGAL/cr. ratio was observed in girls than in boys: 37.06 and 19.36 ng/mg cr., respectively. |
| Miklaszewska et al. [33] | 2019 | Preterm neonates | NGAL/cr. ratio decreased in the following weeks of life in LBW, VLBW, and ELBW male neonates. For female neonates, a similar trend was observed only in VLBW children. |
| Sridahran et al. [28] | 2021 | Neonates receiving potentially nephrotoxic drugs | Median NGAL/cr. ratio: 38.45 ng/mg creatinine. |
| De Mul at. al [37] | 2022 | Preterm neonates without AKI | Median concentration of urinary NGAL: 122.8 ng/mL. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamianowska, M.; Kamianowska, A.; Maciejczyk, M.; Kurowska, A.; Błażewicz, B.; Rogowska, A.M.; Wasilewska, A. The Urinary Concentrations of Neutrophil Gelatinase-Associated Lipocalin, Cystatin C and Osteopontin in the Healthy Term and Stable Preterm Neonates: A Pilot Study. J. Clin. Med. 2023, 12, 6512. https://doi.org/10.3390/jcm12206512
Kamianowska M, Kamianowska A, Maciejczyk M, Kurowska A, Błażewicz B, Rogowska AM, Wasilewska A. The Urinary Concentrations of Neutrophil Gelatinase-Associated Lipocalin, Cystatin C and Osteopontin in the Healthy Term and Stable Preterm Neonates: A Pilot Study. Journal of Clinical Medicine. 2023; 12(20):6512. https://doi.org/10.3390/jcm12206512
Chicago/Turabian StyleKamianowska, Monika, Aleksandra Kamianowska, Mateusz Maciejczyk, Anna Kurowska, Bożena Błażewicz, Agnieszka Maria Rogowska, and Anna Wasilewska. 2023. "The Urinary Concentrations of Neutrophil Gelatinase-Associated Lipocalin, Cystatin C and Osteopontin in the Healthy Term and Stable Preterm Neonates: A Pilot Study" Journal of Clinical Medicine 12, no. 20: 6512. https://doi.org/10.3390/jcm12206512