
Prognostic Factors for Postoperative Chronic Pain after Knee or Hip Replacement in Patients with Knee or Hip Osteoarthritis: An Umbrella Review

 ,
,  ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Systematic Literature Search
- Population:
- Exposure:
- Comparator:
- Outcome:
2.2. Eligibility Criteria
2.3. Screening, Selection Process, and Data Extraction
2.4. Assessment of Risk of Bias (RoB)
3. Results
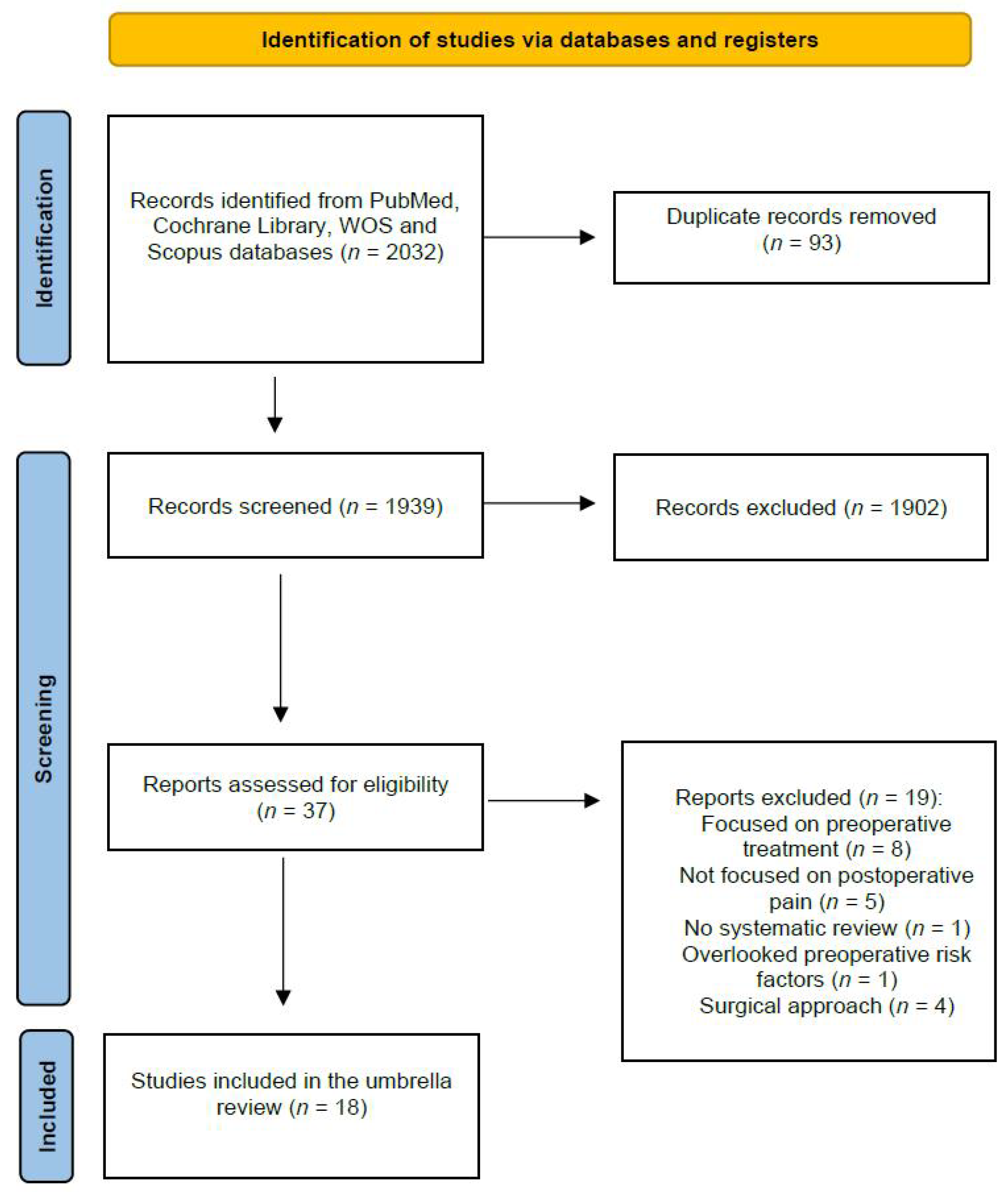
3.1. Study Selection
3.2. Study Characteristics
3.3. Sociodemographic Prognostic Factors
3.4. Clinical Prognostic Factors
3.5. Psychological Prognostic Factors
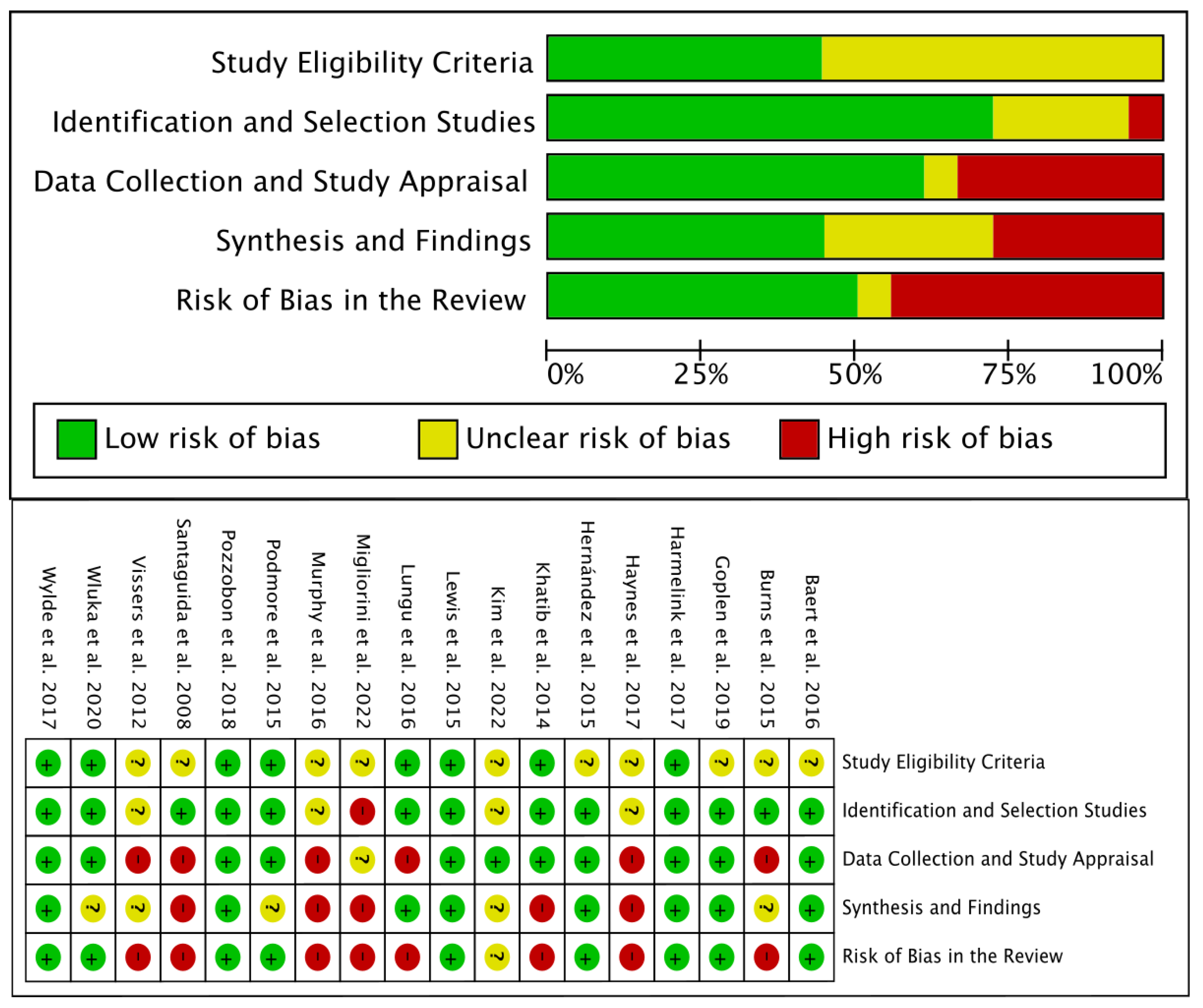
3.6. Risk of Bias
3.7. Synthesis of Results
4. Discussion
4.1. Findings
4.2. Sociodemographic Preoperative Factors
4.3. Clinical and Sensory Preoperative Factors
4.4. Psychological and Cognitive Preoperative Factors
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Long, H.; Liu, Q.; Yin, H.; Wang, K.; Diao, N.; Zhang, Y.; Lin, J.; Guo, A. Prevalence Trends of Site-Specific Osteoarthritis from 1990 to 2019: Findings from the Global Burden of Disease Study 2019. Arthritis Rheumatol. 2022, 74, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Judge, A.; Cooper, C.; Williams, S.; Dreinhoefer, K.; Dieppe, P. Patient-reported outcomes one year after primary hip replacement in a European Collaborative Cohort. Arthritis Care Res. 2010, 62, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.K.; Vaegter, H.B.; Stubhaug, A.; Wolff, A.; Scammell, B.E.; Arendt-Nielsen, L.; Larsen, D.B. The predictive value of quantitative sensory testing: A systematic review on chronic postoperative pain and the analgesic effect of pharmacological therapies in patients with chronic pain. Pain 2021, 162, 31–44. [Google Scholar] [CrossRef]
- Kurien, T.; Arendt-Nielsen, L.; Petersen, K.K.; Graven-Nielsen, T.; Scammell, B.E. Preoperative Neuropathic Pain-like Symptoms and Central Pain Mechanisms in Knee Osteoarthritis Predicts Poor Outcome 6 Months after Total Knee Replacement Surgery. J. Pain 2018, 19, 1329–1341. [Google Scholar] [CrossRef]
- Larsen, D.B.; Laursen, M.; Edwards, R.R.; Simonsen, O.; Arendt-Nielsen, L.; Petersen, K.K. The Combination of Preoperative Pain, Conditioned Pain Modulation, and Pain Catastrophizing Predicts Postoperative Pain 12 Months after Total Knee Arthroplasty. Pain Med. 2021, 22, 1583–1590. [Google Scholar] [CrossRef]
- Brown, O.S.; Hu, L.; Demetriou, C.; Smith, T.O.; Hing, C.B. The effects of kinesiophobia on outcome following total knee replacement: A systematic review. Arch. Orthop. Trauma Surg. 2020, 140, 2057–2070. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid.-Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; ROBIS group. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef]
- Hayden, J.; Tougas, M.; Riley, R.; Iles, R.; Pincus, T. Individual recovery expectations and prognosis of outcomes in non-specific low back pain: Prognostic factor exemplar review. Cochrane Database Syst. Rev. 2014, 9, CD011284. [Google Scholar] [CrossRef]
- Walton, D.M. An Overview of Systematic Reviews on Prognostic Factors in Neck Pain: Results from the International Collaboration on Neck Pain (ICON) Project. Open Orthop. J. 2013, 7, 494–505. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, I.N.; Bennell, K.L. Does pre-operative physiotherapy improve outcomes from lower limb joint replacement surgery? A systematic review. Aust. J. Physiother. 2004, 50, 25–30. [Google Scholar] [CrossRef]
- Aydin, D.; Klit, J.; TRoelsen, A.; Husted, H. No major effects of preoperative education in patients undergoing hip or knee replacement—A systematic review. Dan. Med. J. 2015, 67, A5106. [Google Scholar]
- Jordan, R.W.; Smith, N.A.; Chahal, G.S.; Casson, C.; Reed, M.R.; Sprowson, A.P. Enhanced education and physiotherapy before knee replacement; is it worth it? A systematic review. Physiotherapy 2014, 100, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Heredia, J.; Loza, E.; Cebreiro, I.; Ruiz Iban, M.Á. Preventive analgesia in hip or knee arthroplasty: A systematic review. Rev. Española Cirugía Ortopédica Traumatol. Engl. Ed. 2015, 59, 73–90. [Google Scholar] [CrossRef]
- Kwok, I.H.Y.; Paton, B.; Haddad, F.S. Does Pre-Operative Physiotherapy Improve Outcomes in Primary Total Knee Arthroplasty?—A Systematic Review. J. Arthroplasty. 2015, 30, 1657–1663. [Google Scholar] [CrossRef]
- Moyer, R.; Ikert, K.; Long, K.; Marsh, J. The Value of Preoperative Exercise and Education for Patients Undergoing Total Hip and Knee Arthroplasty. JBJS Rev. 2017, 5, E2. [Google Scholar] [CrossRef]
- Dennis, J.; Wylde, V.; Gooberman-Hill, R.; Blom, A.W.; Beswick, A.D. Effects of presurgical interventions on chronic pain after total knee replacement: A systematic review and meta-analysis of randomised controlled trials. BMJ Open 2020, 10, e033248. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, H.; Zhang, H.; Guo, M.; Gao, Y.; Du, C. Local infiltration vs epidural analgesia for postoperative pain control after total knee or hip arthroplasty: A meta-analysis of randomized controlled trials. Medicine 2020, 99, e22674. [Google Scholar] [CrossRef]
- Elings, J.; Hoogeboom, T.J.; van der Sluis, G.; van Meeteren, N. What preoperative patient-related factors predict inpatient recovery of physical functioning and length of stay after total hip arthroplasty? A systematic review. Clin. Rehabil. 2015, 29, 477–492. [Google Scholar] [CrossRef]
- Buirs, L.D.; van Beers, L.W.A.H.; Scholtes, V.A.B.; Pastoors, T.; Sprague, S.; Poolman, R.W. Predictors of physical functioning after total hip arthroplasty: A systematic review. BMJ Open 2016, 6, e010725. [Google Scholar] [CrossRef]
- Sun, K.; Li, H. Body mass index as a predictor of outcome in total knee replacement: A systemic review and meta-analysis. Knee 2017, 24, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Sayah, S.M.; Karunaratne, S.; Beckenkamp, P.R.; Horsley, M.; Hancock, M.J.; Hunter, D.J.; Herbert, R.D.; de Campos, T.F.; Steffens, D. Clinical Course of Pain and Function Following Total Knee Arthroplasty: A Systematic Review and Meta-Regression. J. Arthroplast. 2021, 36, 3993–4002.e37. [Google Scholar] [CrossRef]
- Hofstede, S.N.; Gademan, M.G.J.; Vliet Vlieland, T.P.M.; Nelissen, R.G.H.H.; Marang-Van De Mheen, P.J. Preoperative predictors for outcomes after total hip replacement in patients with osteoarthritis: A systematic review. BMC Musculoskelet. Disord. 2016, 17, 212. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P.; Thienpont, E. Pain after total knee arthroplasty: A narrative review focusing on the stratification of patients at risk for persistent pain. Bone Jt. J. 2015, 97 (Suppl. A), 45–48. [Google Scholar] [CrossRef]
- Miller, L.E.; Gondusky, J.S.; Bhattacharyya, S.; Kamath, A.F.; Boettner, F.; Wright, J. Does Surgical Approach Affect Outcomes in Total Hip Arthroplasty through 90 Days of Follow-Up? A Systematic Review with Meta-Analysis. J. Arthroplast. 2018, 33, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Chawla, A.; Underwood, M.; Price, A.J.; Metcalfe, A.; Hutchinson, C.; Warwick, J.; Seers, K.; Parsons, H.; Wall, P.D. Tourniquet use for knee replacement surgery. Cochrane Database Syst. Rev. 2020, 12, CD012874. [Google Scholar] [CrossRef]
- McCarthy Deering, E.; Hu, S.Y.; Abdulkarim, A. Does Tourniquet Use in TKA Increase Postoperative Pain? A Systematic Review and Meta-analysis. Clin. Orthop. Relat. Res. 2019, 477, 547–558. [Google Scholar] [CrossRef]
- Duan, G.; Liu, C.; Lin, W.; Shao, J.; Fu, K.; Niu, Y.; Wang, F. Different Factors Conduct Anterior Knee Pain Following Primary Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. J. Arthroplast. 2018, 33, 1962–1971.e3. [Google Scholar] [CrossRef]
- Pozzobon, D.; Ferreira, P.H.; Blyth, F.M.; Machado, G.C.; Ferreira, M.L. Can obesity and physical activity predict outcomes of elective knee or hip surgery due to osteoarthritis? A meta-analysis of cohort studies. BMJ Open 2018, 8, e017689. [Google Scholar] [CrossRef] [PubMed]
- Goplen, C.M.; Verbeek, W.; Kang, S.H.; Jones, C.A.; Voaklander, D.C.; Churchill, T.A.; Beaupre, L.A. Preoperative opioid use is associated with worse patient outcomes after Total joint arthroplasty: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 234. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Pintore, A.; Eschweiler, J.; Oliva, F.; Hildebrand, F.; Maffulli, N. Factors influencing the outcomes of minimally invasive total hip arthroplasty: A systematic review. J. Orthop. Surg. Res. 2022, 17, 281. [Google Scholar] [CrossRef] [PubMed]
- Wluka, A.E.; Yan, M.K.; Lim, K.Y.; Hussain, S.M.; Cicuttini, F.M. Does preoperative neuropathic-like pain and central sensitisation affect the post-operative outcome of knee joint replacement for osteoarthritis? A systematic review and meta analysis. Osteoarthr. Cartil. 2020, 28, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Kim, J.J.; Kang, K.H.; Kim, M.J.; In, Y. Diagnosis of Central Sensitization and Its Effects on Postoperative Outcomes following Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 1248. [Google Scholar] [CrossRef]
- Podmore, B.; Hutchings, A.; van der Meulen, J.; Aggarwal, A.; Konan, S. Impact of comorbid conditions on outcomes of hip and knee replacement surgery: A systematic review and meta-analysis. BMJ Open 2018, 8, e021784. [Google Scholar] [CrossRef]
- Murphy, B.P.D.S.; Dowsey, M.M.; Choong, P.F.M. The Impact of Advanced Age on the Outcomes of Primary Total Hip and Knee Arthroplasty for Osteoarthritis. JBJS Rev. 2018, 6, e6. [Google Scholar] [CrossRef]
- Wylde, V.; Beswick, A.D.; Dennis, J.; Gooberman-Hill, R. Post-operative patient-related risk factors for chronic pain after total knee replacement: A systematic review. BMJ Open 2017, 7, e018105. [Google Scholar] [CrossRef]
- Haynes, J.; Nam, D.; Barrack, R. Obesity in total hip arthroplasty. Bone Jt. J. 2017, 99, 31–36. [Google Scholar] [CrossRef]
- Harmelink, K.E.M.; Zeegers, A.V.C.M.; Hullegie, W.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; Staal, J.B. Are There Prognostic Factors for One-Year Outcome after Total Knee Arthroplasty? A Systematic Review. J. Arthroplast. 2017, 32, 3840–3853.e1. [Google Scholar] [CrossRef]
- Lungu, E.; Maftoon, S.; Vendittoli, P.A.; Desmeules, F. A systematic review of preoperative determinants of patient-reported pain and physical function up to 2 years following primary unilateral total hip arthroplasty. Orthop. Traumatol. Surg. Res. 2016, 102, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Hernández, C.; Díaz-Heredia, J.; Berraquero, M.L.; Crespo, P.; Loza, E.; Ruiz Ibán, M.Á. Factores predictores prequirúrgicos de dolor posquirúrgico en pacientes sometidos a artroplastia de cadera o rodilla. Una revisión sistemática. Reum. Clin. 2015, 11, 361–380. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.N.; Rice, D.A.; McNair, P.J.; Kluger, M. Predictors of persistent pain after total knee arthroplasty: A systematic review and meta-analysis. Br. J. Anaesth. 2015, 114, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Burns, L.C.; Ritvo, S.E.; Ferguson, M.K.; Clarke, H.; Seltzer, Z.; Katz, J. Pain catastrophizing as a risk factor for chronic pain after total knee arthroplasty: A systematic review. J. Pain Res. 2015, 8, 21–32. [Google Scholar] [PubMed]
- Santaguida, P.L.; Hawker, G.A.; Hudak, P.L.; Glazier, R.; Mahomed, N.N.; Kreder, H.J.; Coyte, P.C.; Wright, J.G. Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: A systematic review. J. Can. Chir. 2008, 51, 428. [Google Scholar]
- Vissers, M.M.; Bussmann, J.B.; Verhaar, J.A.N.; Busschbach, J.J.V.; Bierma-Zeinstra, S.M.A.; Reijman, M. Psychological factors affecting the outcome of total hip and knee arthroplasty: A systematic review. Semin. Arthritis Rheum. 2012, 41, 576–588. [Google Scholar] [CrossRef]
- Khatib, Y.; Madan, A.; Naylor, J.M.; Harris, I.A. Do Psychological Factors Predict Poor Outcome in Patients Undergoing TKA? A Systematic Review. Clin. Orthop. Relat. Res. 2015, 473, 2630–2638. [Google Scholar] [CrossRef]
- Baert, I.A.C.; Lluch, E.; Mulder, T.; Nijs, J.; Noten, S.; Meeus, M. Does pre-surgical central modulation of pain influence outcome after total knee replacement? A systematic review. Osteoarthr. Cartil. 2016, 24, 213–223. [Google Scholar] [CrossRef]
- McMurtry, M.; Viswanath, O.; Cernich, M.; Strand, N.; Freeman, J.; Townsend, C.; Kaye, A.D.; Cornett, E.M.; Wie, C. The Impact of the Quantity and Quality of Social Support on Patients with Chronic Pain. Curr. Pain. Headache Rep. 2020, 24, 72. [Google Scholar] [CrossRef]
- López-Martínez, A.E.; Esteve-Zarazaga, R.; Ramírez-Maestre, C. Perceived Social Support and Coping Responses Are Independent Variables Explaining Pain Adjustment among Chronic Pain Patients. J. Pain 2008, 9, 373–379. [Google Scholar] [CrossRef]
- Yang, M.M.H.; Hartley, R.L.; A Leung, A.; E Ronksley, P.; Jetté, N.; Casha, S.; Riva-Cambrin, J. Preoperative predictors of poor acute postoperative pain control: A systematic review and meta-analysis. BMJ Open 2019, 9, e025091. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Chen, D.; McNicol, E.; Sharma, L.; Varaday, G.; Sharma, A.; Wilson, E.; Wright-Yatsko, T.; Yaeger, L.; Gilron, I.; et al. Risk factors for persistent pain after breast and thoracic surgeries: A systematic literature review and meta-analysis. Pain 2022, 163, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Andreolotti, H.; Dereu, D.; Combescurre, C.; Rehberg, B. A systematic review and meta-analysis of three risk factors for chronic postsurgical pain: Age, sex and preoperative pain. Minerva Anestesiol. 2022, 88, 827–841. [Google Scholar] [CrossRef] [PubMed]
- Chesham, R.A.; Shanmugam, S. Does preoperative physiotherapy improve postoperative, patient-based outcomes in older adults who have undergone total knee arthroplasty? A systematic review. Physiother. Theory Pract. 2017, 33, 9–30. [Google Scholar] [CrossRef]
- Georgopoulos, V.; Akin-Akinyosoye, K.; Zhang, W.; McWilliams, D.F.; Hendrick, P.; Walsh, D.A. Quantitative sensory testing and predicting outcomes for musculoskeletal pain, disability, and negative affect: A systematic review and meta-analysis. Pain 2019, 160, 1920–1932. [Google Scholar] [CrossRef]
- O’Leary, H.; Smart, K.M.; Moloney, N.A.; Doody, C.M. Nervous System Sensitization as a Predictor of Outcome in the Treatment of Peripheral Musculoskeletal Conditions: A Systematic Review. Pain Pract. 2017, 17, 249–266. [Google Scholar] [CrossRef]
- Mcnicol, E.; Schumann, R.; Haratounian, S. A systematic review and meta-analysis of ketamine for the prevention of persistent post-surgical pain. Acta Anaesthesiol. Scand. 2014, 58, 1199–1213. [Google Scholar] [CrossRef]
- Meyer-Frießem, C.H.; Lipke, E.; Weibel, S.; Kranke, P.; Reichl, S.; Pogatzki-Zahn, E.M.; Zahn, P.K.; Schnabel, A. Perioperative ketamine for postoperative pain management in patients with preoperative opioid intake: A systematic review and meta-analysis. J. Clin. Anesth. 2022, 78, 110652. [Google Scholar] [CrossRef]
- Previtali, D.; Capone, G.; Marchettini, P.; Candrian, C.; Zaffagnini, S.; Filardo, G. High Prevalence of Pain Sensitization in Knee Osteoarthritis: A Meta-Analysis with Meta-Regression. Cartilage 2022, 13, 19476035221087698. [Google Scholar] [CrossRef]
- Lluch, E.; Nijs, J.; Courtney, C.A.; Rebbeck, T.; Wylde, V.; Baert, I.; Wideman, T.H.; Howells, N.; Skou, S.T. Clinical descriptors for the recognition of central sensitization pain in patients with knee osteoarthritis. Disabil. Rehabil. 2018, 40, 2836–2845. [Google Scholar] [CrossRef]
- Lluch, E.; Dueñas, L.; Falla, D.; Baert, I.; Meeus, M.; Sánchez-Frutos, J.; Nijs, J. Preoperative Pain Neuroscience Education Combined with Knee Joint Mobilization for Knee Osteoarthritis. Clin. J. Pain 2018, 34, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Yerneni, K.; Nichols, N.; Abecassis, Z.A.; Karras, C.L.; Tan, L.A. Preoperative Opioid Use and Clinical Outcomes in Spine Surgery. Neurosurgery 2020, 86, E490–E507. [Google Scholar] [CrossRef] [PubMed]
- Hannon, C.P.; Fillingham, Y.A.; Nam, D.; Courtney, P.M.; Curtin, B.M.; Vigdorchik, J.; Mullen, K.; Casambre, F.; Riley, C.; Hamilton, W.G.; et al. The Efficacy and Safety of Opioids in Total Joint Arthroplasty: Systematic Review and Direct Meta-Analysis. J. Arthroplast. 2020, 35, 2759–2771.e13. [Google Scholar] [CrossRef] [PubMed]
- Giusti, E.M.; Lacerenza, M.; Manzoni, G.M.; Castelnuovo, G. Psychological and psychosocial predictors of chronic postsurgical pain: A systematic review and meta-analysis. Pain 2021, 162, 10–30. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Rodrigues, D.; Rodrigues, A.; Martins, T.; Pinto, J.; Amorim, D.; Almeida, A.; Pinto-Ribeiro, F. Correlation between pain severity and levels of anxiety and depression in osteoarthritis patients: A systematic review and meta-analysis. Rheumatology 2021, 61, 53–75. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Cortés, R.; Cruz-Montecinos, C.; Torres-Castro, R.; Tapia, C.; Püschel, T.A.; Pérez-Alenda, S. Effects of Cognitive and Mental Health Factors on the Outcomes Following Carpal Tunnel Release: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2022, 103, 1615–1627. [Google Scholar] [CrossRef]
- Moloney, N.A.; Pocovi, N.C.; Dylke, E.S.; Graham, P.L.; de Groef, A. Psychological Factors Are Associated with Pain at All Time Frames after Breast Cancer Surgery: A Systematic Review with Meta-Analyses. Pain Med. 2021, 22, 915–947. [Google Scholar] [CrossRef]
- Tseli, E.; Boersma, K.; Stålnacke, B.-M.; Enthoven, P.; Gerdle, B.; Äng, B.O.; Grooten, W.J. Prognostic Factors for Physical Functioning after Multidisciplinary Rehabilitation in Patients with Chronic Musculoskeletal Pain. Clin. J. Pain 2019, 35, 148–173. [Google Scholar] [CrossRef]
- Ioannidis, J.P. Integration of evidence from multiple meta-analyses: A primer on umbrella reviews, treatment networks and multiple treatments meta-analyses. Can. Med. Assoc. J. 2009, 181, 488–493. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Author | Type of Study | Characteristics of the Sample | Studies Included | Prognostic Factors Analyzed |
|---|---|---|---|---|
| Santaguida et al. [45] | Systematic review | JKR or JHR | 64 studies (6 prospective studies, 58 retrospective studies) | Age; sex; BMI or weight |
| Vissers et al. [46] | Systematic review | TKA and THA | 35 prospective studies | Mental health; pain catastrophizing; depression; anxiety; coping; personality; perceived stress; emotionality; fear of movement; sense of coherence; fatigue |
| Khatib et al. [47] | Systematic review | KJR | 17 prospective cohort studies and 2 cross-sectional surveys | Mental health; anxiety; depression; pain catastrophizing; self-efficacy; quality of life |
| Burns et al. [44] | Systematic review | TKA | 6 studies (2 prospective cohort studies, 3 case-control studies, and 1 cohort and case-control study) | Pain catastrophizing |
| Hernández et al. [42] | Systematic review | Total hip and knee arthroplasty | 37 studies (4 systematic reviews, 1 randomized clinical trial, and 32 observational studies) | Age; sex; level of education; socioeconomic status; social support; preoperative educational interventions; race; body mass index; comorbidities; preoperative pain; preoperative functional capacity; self-efficacy; patient expectations; pain catastrophizing; depression; anxiety; personality; mental health; other psychological factors |
| Lewis et al. [43] | Systematic review and meta-analysis | TKA | 32 studies (28 studies included in meta-analyses, 23 prospective studies) | Age; weight; social support; anxiety; pain catastrophizing; comorbidities; depression; education; gender; mental health; other pain sites; preoperative pain |
| Lungu et al. [41] | Systematic review | THA | 22 studies included | Age; sex; BMI; lower educational; surgery expectations; preoperative pain; preoperative functional capacity; mental health; physical health; physical status; comorbidities; knee extensor strength; radiographic OA severity; waiting time for surgery; widespread pain sensitivity |
| Baert et al. [48] | Systematic review | TKA | 16 studies included (cohort studies) | Depressive symptoms; anxiety, pain catastrophizing; fear of movement; coping strategy; preoperative pain; widespread pain sensitivity |
| Harmenlink et al. [40] | Systematic review | TKA from OA with a follow-up > 1 yr | 18 studies (13 prospective studies, 5 retrospective studies) | Age; sex; BMI; anxiety; depression; social support; education; income; employment; preoperative pain; physical function; preoperative quadriceps muscle force; preoperative flexion contracture; preoperative ROM; quality of life; comorbidities; walking distance; painful other joints; radiographic severity; overall health status |
| Wylde et al. [38] | Systematic review | TKR and follow-up less than 6 months | 14 studies (11 cohort, 2 RCT, 2 retrospective, and 1 case-control) | Pain catastrophizing; depression; anxiety; social support; coping strategies; fear of movement |
| Haynes et al. [39] | Systematic review | THA | 17 cohort studies | BMI |
| Goplen et al. [32] | Systematic review and metanalysis | Total joint arthroplasty | 6 retrospective studies | Preoperative opioid use |
| Wluka et al. [34] | Systematic review and metanalysis | TKR | 5 manuscripts with 6 cohorts (4 studies, 1 pre-pint) | Neuropathic-like pain symptoms |
| Podmore et al. [36] | Systematic review and metanalysis | TKR and THR | 70 observational studies | Depression, comorbidities |
| Murphy et al. [37] | Systematic review | TKA and THA | 32 studies included | Age |
| Pozzobon et al. [31] | Systematic review and metanalysis | TKA and THA | 62 studies included in the qualitative analysis. 31 in the meta-analyses | BMI |
| Migliorini et al. [33] | Systematic review and metanalysis | Minimal invasive THA | 76 studies (33 randomized clinical trials, 29 prospective studies, and 17 retrospective studies) | Sex; age; BMI; preoperative pain, preoperative function |
| Kim et al. [35] | Systematic review and meta-analysis | TKA | 8 studies in the systematic review (5 prospective studies, 1 randomized clinical trial, and 2 retrospective studies). 5 studies in the meta-analyses | Central sensitization (CSI) |
| Prognostic Factor | Reviews Investigating a Particular Prognostic Factor | Overall Risk of Bias (ROBIS) | Summary of Findings from Reviews | Confidence in Conclusions Based on All Review Findings | ||||
|---|---|---|---|---|---|---|---|---|
| Low | Unclear | High | Consistent (High, Moderate, Low, or Very Low): Association | Consistent (Moderate/Strong Evidence): NO Association | Conflicting/Inconsistent or Weak/Limited Evidence | High/Moderate/Low/Very Low | ||
| Race | One review (Hernández et al. [42]) | 1/1 (Hernández et al. [42]) | 1 (Hernández et al. [42]) | High confidence: worse postoperative pain (1 low RoB) | ||||
| Comorbidities | One review (Podmore et al. [36]) | 1/1 (Podmore et al. [36]) | 1/1 (Podmore et al. [36]) | High confidence: no association (1 low RoB) | ||||
| Other pain sites | Two reviews (Harmelink et al. [40], Lewis et al. [43]) | 2/2 (Harmelink et al. [40], Lewis et al. [43]) | 1 (Lewis et al. [43]) | 1 (Harmelink et al. [40]) | Moderate confidence: worse postoperative pain—1 review (1 low RoB) and 1 very low evidence for association (1 low RoB) | |||
| Opioid use | One review (Goplen et al. [32]) | 1/1 (Goplen et al. [32]) | 1 (Goplen et al. [32]) | High confidence: worse postoperative pain (1 low RoB) | ||||
| Social support | Four reviews (Harmelink et al. [40], Hernández et al. [42], Lewis et al. [43], Wylde et al. [38]) | 4/4 (Harmelink et al. [40], Hernández et al. [42], Lewis et al. [43], Wylde et al. [38]) | 2/4 (Lewis et al. [43], Wylde et al. [38]) | 2/4 (Harmelink et al. [40], Hernández et al. [42]) | Moderate confidence: worse postoperative pain—2 reviews (2 low RoB), 1 reported conflicting evidence (low RoB), and 1 reported very low evidence of association (low RoB) | |||
| Preoperative function | Three reviews (Hernández et al. [42], Lewis et al. [43], Lungu et al. [41]) | 2/3 (Hernández et al. [42], Lewis et al. [43]) | 1/3 (Lungu et al. [41]) | 3 (Hernández et al. [42], Lewis et al. [43], Lungu et al. [41]) | High confidence: worse postoperative pain—3 reviews (2 low RoB and 1 high RoB) | |||
| Preoperative pain | Six reviews (Baert et al. [48], Harmelink et al. [40], Hernández et al. [42], Lewis et al. [43], Lungu et al. [41], Migliorini et al. [33]) | 4/6 (Harmelink et al. [40], Hernández et al. [42], Lewis et al. [43]) | 2/6 (Lungu et al. [41], Migliorini et al. [33]) | 4 (Hernández et al. [42], Lewis et al. [43], Lungu et al. [41], Migliorini et al. [33]) | 2 (Baert et al. [48], Harmelink et al. [40]) | Moderate confidence: worse postoperative pain—4 reviews (2 low RoB) and 2 reported very low evidence for association (low RoB) | ||
| Central sensitization | Three reviews (Baert et al. [48], Kim et al. [35], Lungu et al. [41]) | 1/3 (Baert et al. [48]) | 1/3 (Kim et al. [35]) | 1/3 (Lungu et al. [41]) | 3 (Kim et al. [35], Baert et al. [48], Lungu et al. [41]) | High confidence: worse postoperative pain—3 reviews (1 low RoB, 1 unclear RoB, and 1 high RoB) | ||
| Neuropathic pain | Two reviews (Wluka et al. [34], Wylde et al. [38]) | 2/2 (Wluka et al. [34], Wylde et al. [38]) | 2 (Wluka et al. [34], Wylde et al. [38]) | High confidence: worse postoperative pain—2 reviews (2 low RoB) | ||||
| Mental health | Five reviews (Hernández et al. [42], Khatib et al. [47], Lewis et al. [43], Lungu et al. [41], Vissers et al. [46]) | 2/5 (Hernández et al. [42]. Lewis et al. [43]) | 3/5 (Khatib et al. [47], Lungu et al. [41], Vissers et al. [46]) | 4 (Hernández et al. [42], Lewis et al. [43], Lungu et al. [41], Vissers et al. [46]) | 1 (Khatib et al. [47]) | Moderate confidence: 4 reviews reporting association (2 low RoB) and 1 reporting for no association (high RoB) | ||
| Pain catastrophizing | Seven reviews (Baert et al. [48], Burns et al. [44], Hernández et al. [42], Khatib et al. [47], Lewis et al. [43], Vissers et al. [46], Wylde et al. [38]) | 4/7 (Baert et al. [48], Hernández et al. [42], Lewis et al. [43], Wylde et al. [38]) | 3/7 (Burns et al. [44], Khatib et al. [47], Vissers et al. [46]) | 7 (Baert et al. [48], Burns et al. [44], Hernández et al. [42], Khatib et al. [47], Lewis et al. [43], Vissers et al. [46], Wylde et al. [38]) | High confidence: worse postoperative pain—7 reviews reporting association (4 low RoB and 3 high RoB) | |||
| Depression | Eight reviews (Baert et al. [48], Harmelink et al. [40], Hernández et al. [42], Khatib et al. [47], Lewis et al. [43], Podmore et al. [36], Vissers et al. [46], Wylde et al. [38]) | 6/8 (Baert et al. [48], Harmelink et al. [40], Hernández et al. [42], Lewis et al. [43], Podmore et al. [36], Wylde et al. [38]) | 2/8 (Khatib et al. [47], Vissers et al. [46]) | 5 (Hernández et al. [42], Khatib et al. [47], Lewis et al. [43], Vissers et al. [46], Wylde et al. [38]) | 1 (Podmore et al. [36]) | 2 (Baert et al. [48], Harmelink et al. [40]) | Moderate confidence: 5 reviews reporting association (3 low RoB), 1 reporting no association (1 low RoB) and 2 reported very low evidence for association (2 low RoB) | |
| Anxiety | Seven reviews (Baert et al. [48], Harmelink et al. [40], Hernández et al. [42], Khatib et al. [47], Lewis et al. [43], Vissers et al. [46], Wylde et al. [38]) | 5/7 (Baert et al. [48], Harmelink et al. [40], Hernández et al. [42], Lewis et al. [43], Wylde et al. [38]) | 2/7 (Khatib et al. [47], Vissers et al. [46]) | 6 (Harmelink et al. [40], Hernández et al. [42], Khatib et al. [47], Lewis et al. [43], Vissers et al. [46], Wylde et al. [38]) | 1 (Baert et al. [48]) | High confidence: 7 reviews reporting association (4 low RoB and 2 high RoB), and 1 reported conflicting evidence (1 low RoB) | ||
| Fear of movement | Three reviews (Baert et al. [48], Vissers et al. [46], Wylde et al. [38]) | 2/3 (Baert et al. [48], Wylde et al. [38]) | 1/3 (Vissers et al. [46]) | 2 (Vissers et al. [46], Wylde et al. [38]) | 1 (Baert et al. [48]) | Moderate confidence: 2 review reporting association (1 low RoB and 1 high RoB), and 1 reported no association (1 low RoB) | ||
| Coping strategy | Three reviews (Baert et al. [48], Vissers et al. [46], Wylde et al. [38]) | 2/3 (Baert et al. [48], Wylde et al. [38]) | 0 | 1/3 (Visser et al. [46]) | 2 (Baert et al. [48], Vissers et al. [46]) | 1 (Wylde et al. [38]) | Moderate confidence: 2 reported association (1 high RoB and 1 low RoB) and 1 review reporting no association (1 low RoB). | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-de-las-Peñas, C.; Florencio, L.L.; de-la-Llave-Rincón, A.I.; Ortega-Santiago, R.; Cigarán-Méndez, M.; Fuensalida-Novo, S.; Plaza-Manzano, G.; Arendt-Nielsen, L.; Valera-Calero, J.A.; Navarro-Santana, M.J. Prognostic Factors for Postoperative Chronic Pain after Knee or Hip Replacement in Patients with Knee or Hip Osteoarthritis: An Umbrella Review. J. Clin. Med. 2023, 12, 6624. https://doi.org/10.3390/jcm12206624
Fernández-de-las-Peñas C, Florencio LL, de-la-Llave-Rincón AI, Ortega-Santiago R, Cigarán-Méndez M, Fuensalida-Novo S, Plaza-Manzano G, Arendt-Nielsen L, Valera-Calero JA, Navarro-Santana MJ. Prognostic Factors for Postoperative Chronic Pain after Knee or Hip Replacement in Patients with Knee or Hip Osteoarthritis: An Umbrella Review. Journal of Clinical Medicine. 2023; 12(20):6624. https://doi.org/10.3390/jcm12206624
Chicago/Turabian StyleFernández-de-las-Peñas, César, Lidiane L. Florencio, Ana I. de-la-Llave-Rincón, Ricardo Ortega-Santiago, Margarita Cigarán-Méndez, Stella Fuensalida-Novo, Gustavo Plaza-Manzano, Lars Arendt-Nielsen, Juan A. Valera-Calero, and Marcos J. Navarro-Santana. 2023. "Prognostic Factors for Postoperative Chronic Pain after Knee or Hip Replacement in Patients with Knee or Hip Osteoarthritis: An Umbrella Review" Journal of Clinical Medicine 12, no. 20: 6624. https://doi.org/10.3390/jcm12206624
APA StyleFernández-de-las-Peñas, C., Florencio, L. L., de-la-Llave-Rincón, A. I., Ortega-Santiago, R., Cigarán-Méndez, M., Fuensalida-Novo, S., Plaza-Manzano, G., Arendt-Nielsen, L., Valera-Calero, J. A., & Navarro-Santana, M. J. (2023). Prognostic Factors for Postoperative Chronic Pain after Knee or Hip Replacement in Patients with Knee or Hip Osteoarthritis: An Umbrella Review. Journal of Clinical Medicine, 12(20), 6624. https://doi.org/10.3390/jcm12206624