
Serum KL-6 as a Candidate Predictor of Outcome in Patients with SARS-CoV-2 Pneumonia

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Definition and Scoring of Disease Severity
2.3. Blood Sampling and Laboratory Assays
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Study Subjects
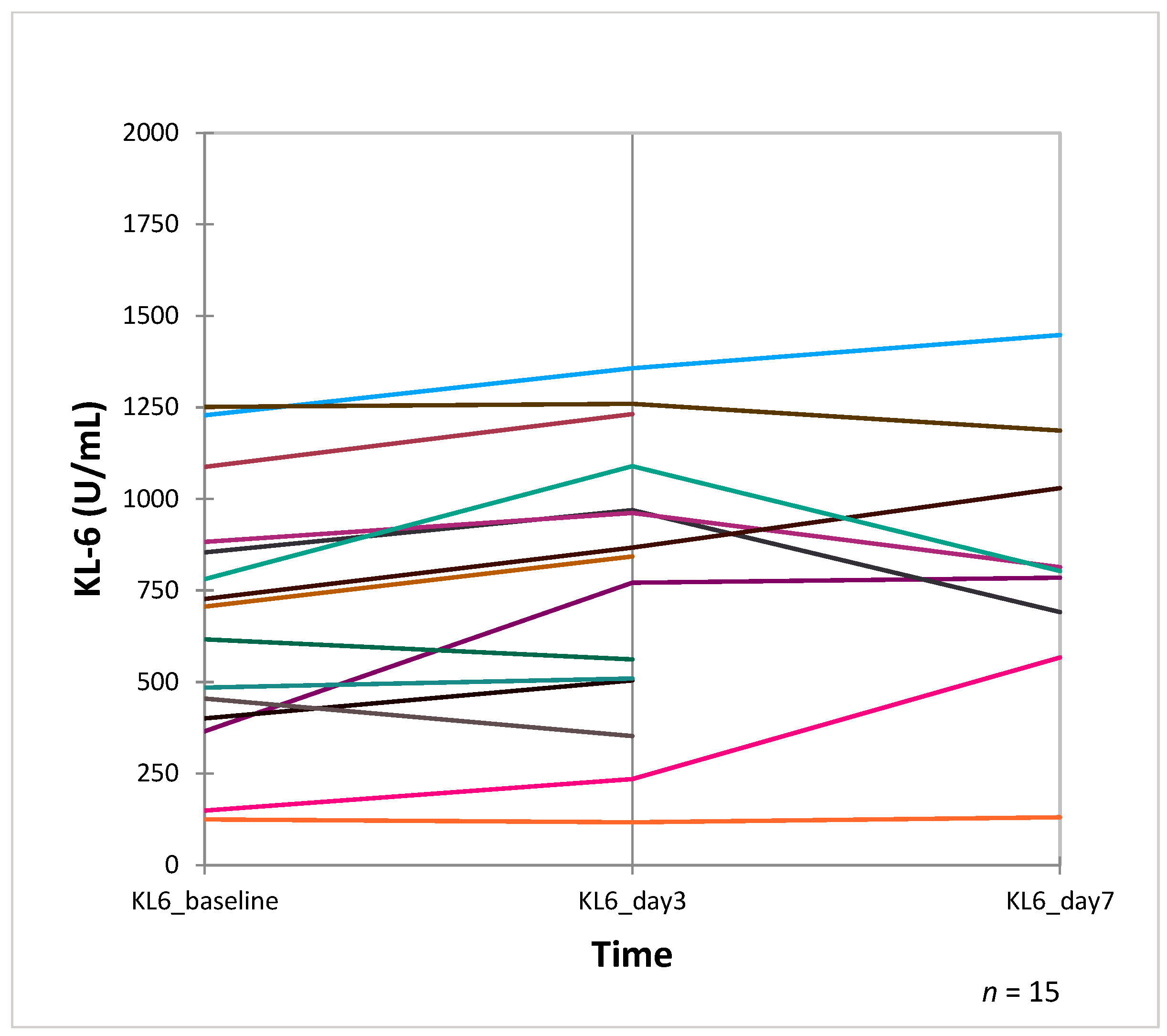
3.2. Serum KL-6 Levels
3.3. Predictive Value of Baseline Serum KL-6 and Other Biomarkers for SARS-CoV-2 Pneumonia Severity
3.4. Logistic Regression for Predictors of Disease Severity
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO COVID-19 Dashboard: WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 15 April 2023).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Delorey, T.M.; Ziegler, C.G.K.; Heimberg, G.; Normand, R.; Yang, Y.; Segerstolpe, Å.; Abbondanza, D.; Fleming, S.J.; Subramanian, A.; Montoro, D.T.; et al. COVID-19 tissue atlases reveal SARS-CoV-2 pathology and cellular targets. Nature 2021, 595, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Aggarwal, G.; Wong, J.; Benoit, S.; Vikse, J.; Plebani, M.; Lippi, G. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am. J. Emerg. Med. 2020, 38, 1722–1726. [Google Scholar] [CrossRef]
- Gao, M.; Piernas, C.; Astbury, N.M.; Hippisley-Cox, J.; O’Rahilly, S.; Aveyard, P.; Jebb, S.A. Associations between body-mass index and COVID-19 severity in 6·9 million people in England: A prospective, community-based, cohort study. Lancet Diabetes Endocrinol. 2021, 9, 350–359. [Google Scholar] [CrossRef]
- Sayah, W.; Berkane, I.; Guermache, I.; Sabri, M.; Lakhal, F.Z.; Yasmine Rahali, S.; Djidjeli, A.; Lamara Mahammed, L.; Merah, F.; Belaid, B.; et al. Interleukin-6, procalcitonin and neutrophil-to-lymphocyte ratio: Potential immune-inflammatory parameters to identify severe and fatal forms of COVID-19. Cytokine 2021, 141, 155428. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, N.; Hattori, N.; Yokoyama, A.; Kohno, N. Utility of KL-6/MUC1 in the clinical management of interstitial lung diseases. Respir. Investig. 2012, 50, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, A.; Kondo, K.; Nakajima, M.; Matsushima, T.; Takahashi, T.; Nishimura, M.; Bando, M.; Sugiyama, Y.; Totani, Y.; Ishizaki, T.; et al. Prognostic value of circulating KL-6 in idiopathic pulmonary fibrosis. Respirology 2006, 11, 164–168. [Google Scholar] [CrossRef]
- Ohshimo, S.; Ishikawa, N.; Horimasu, Y.; Hattori, N.; Hirohashi, N.; Tanigawa, K.; Kohno, N.; Bonella, F.; Guzman, J.; Costabel, U. Baseline KL-6 predicts increased risk for acute exacerbation of idiopathic pulmonary fibrosis. Respir. Med. 2014, 108, 1031–1039. [Google Scholar] [CrossRef]
- d’Alessandro, M.; Cameli, P.; Refini, R.M.; Bergantini, L.; Alonzi, V.; Lanzarone, N.; Bennett, D.; Rana, G.D.; Montagnani, F.; Scolletta, S.; et al. Serum KL-6 concentrations as a novel biomarker of severe COVID-19. J. Med. Virol. 2020, 92, 2216–2220. [Google Scholar] [CrossRef]
- Azekawa, S.; Chubachi, S.; Asakura, T.; Namkoong, H.; Sato, Y.; Edahiro, R.; Lee, H.; Tanaka, H.; Otake, S.; Nakagawara, K.; et al. Serum KL-6 levels predict clinical outcomes and are associated with MUC1 polymorphism in Japanese patients with COVID-19. BMJ Open Respir. Res. 2023, 10, e001625. [Google Scholar] [CrossRef]
- Bergantini, L.; Bargagli, E.; d’Alessandro, M.; Refini, R.M.; Cameli, P.; Galasso, L.; Scapellato, C.; Montagnani, F.; Scolletta, S.; Franchi, F.; et al. Prognostic bioindicators in severe COVID-19 patients. Cytokine 2021, 141, 155455. [Google Scholar] [CrossRef]
- Scotto, R.; Pinchera, B.; Perna, F.; Atripaldi, L.; Giaccone, A.; Sequino, D.; Zappulo, E.; Sardanelli, A.; Schiano Moriello, N.; Stanziola, A.; et al. Serum KL-6 Could Represent a Reliable Indicator of Unfavourable Outcome in Patients with COVID-19 Pneumonia. Int. J. Environ. Res. Public Health 2021, 18, 2078. [Google Scholar] [CrossRef]
- Awano, N.; Inomata, M.; Kuse, N.; Tone, M.; Takada, K.; Muto, Y.; Fujimoto, K.; Akagi, Y.; Mawatari, M.; Ueda, A.; et al. Serum KL-6 level is a useful biomarker for evaluating the severity of coronavirus disease 2019. Respir. Investig. 2020, 58, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Castellví, I.; Castillo, D.; Corominas, H.; Mariscal, A.; Orozco, S.; Benito, N.; Pomar, V.; Baucells, A.; Mur, I.; de La Rosa-Carrillo, D.; et al. Krebs von den Lungen-6 glycoprotein circulating levels are not useful as prognostic marker in COVID-19 pneumonia: A large prospective cohort study. Front. Med. 2022, 9, 973918. [Google Scholar] [CrossRef]
- Fukui, S.; Ikeda, K.; Kobayashi, M.; Nishida, K.; Yamada, K.; Horie, S.; Shimada, Y.; Miki, H.; Goto, H.; Hayashi, K.; et al. Predictive prognostic biomarkers in patients with COVID-19 infection. Mol. Med. Rep. 2023, 27, 15. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Callister, M.E.J.; Mumby, S.; Quinlan, G.J.; Welsh, K.I.; duBois, R.M.; Evans, T.W. KL-6 levels are elevated in plasma from patients with acute respiratory distress syndrome. Eur. Respir. J. 2004, 23, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Schälte, G.; Spinner, C.D.; Malin, J.J.; Gastmeier, P.; Langer, F.; Bracht, H.; et al. S3-Empfehlungen zur Stationaeren Therapie von Patienten mit COVID-19; AWMF-Register-Nr. 113/001: Berlin, Germany, 2021. [Google Scholar]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Schälte, G.; Salzberger, B.; Gastmeier, P.; Langer, F.; Wepler, M.; Westhoff, M.; et al. German recommendations for treatment of critically ill patients with COVID-19-version 3: S1-guideline. Anaesthesist 2020, 69, 653–664. [Google Scholar] [CrossRef]
- Fachgruppe COVRIIN am Robert-Koch-Institut. Medikamentöse Therapie bei COVID-19 mit Bewertung durch die Fachgruppe COVRIIN am Robert-Koch-Institut; Robert Koch-Institut: Berlin, Germany, 2021. [Google Scholar] [CrossRef]
- World Health Organization. Therapeutics and COVID-19: Living Guideline. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2023.1 (accessed on 19 September 2023).
- Marshall, J.C.; Murthy, S.; Diaz, J.; Adhikari, N.K.; Angus, D.C.; Arabi, Y.M.; Baillie, K.; Bauer, M.; Berry, S.; Blackwood, B.; et al. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- d’Alessandro, M.; Bergantini, L.; Cameli, P.; Lanzarone, N.; Antonietta Mazzei, M.; Alonzi, V.; Sestini, P.; Bargagli, E. Serum KL-6 levels in pulmonary Langerhans’ cell histiocytosis. Eur. J. Clin. Investig. 2020, 50, e13242. [Google Scholar] [CrossRef]
- d’Alessandro, M.; Carleo, A.; Cameli, P.; Bergantini, L.; Perrone, A.; Vietri, L.; Lanzarone, N.; Vagaggini, C.; Sestini, P.; Bargagli, E. BAL biomarkers’ panel for differential diagnosis of interstitial lung diseases. Clin. Exp. Med. 2020, 20, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Bonella, F.; Costabel, U. Biomarkers in connective tissue disease-associated interstitial lung disease. Semin. Respir. Crit. Care Med. 2014, 35, 181–200. [Google Scholar] [CrossRef]
- Bonella, F.; Long, X.; Ohshimo, S.; Horimasu, Y.; Griese, M.; Guzman, J.; Kohno, N.; Costabel, U. MUC1 gene polymorphisms are associated with serum KL-6 levels and pulmonary dysfunction in pulmonary alveolar proteinosis. Orphanet J. Rare Dis. 2016, 11, 48. [Google Scholar] [CrossRef]
- Bonella, F.; Ohshimo, S.; Miaotian, C.; Griese, M.; Guzman, J.; Costabel, U. Serum KL-6 is a predictor of outcome in pulmonary alveolar proteinosis. Orphanet J. Rare Dis. 2013, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Deng, K.; Fan, Q.; Yang, Y.; Deng, X.; He, R.; Tan, Y.; Lan, Y.; Deng, X.; Pan, Y.; Wang, Y.; et al. Prognostic roles of KL-6 in disease severity and lung injury in COVID-19 patients: A longitudinal retrospective analysis. J. Med. Virol. 2021, 93, 2505–2512. [Google Scholar] [CrossRef] [PubMed]
- d’Alessandro, M.; Bergantini, L.; Cameli, P.; Curatola, G.; Remediani, L.; Bennett, D.; Bianchi, F.; Perillo, F.; Volterrani, L.; Mazzei, M.A.; et al. Serial KL-6 measurements in COVID-19 patients. Intern. Emerg. Med. 2021, 16, 1541–1545. [Google Scholar] [CrossRef] [PubMed]
- Xue, M.; Zheng, P.; Bian, X.; Huang, Z.; Huang, H.; Zeng, Y.; Hu, H.; Liu, X.; Zhou, L.; Sun, B.; et al. Exploration and correlation analysis of changes in Krebs von den Lungen-6 levels in COVID-19 patients with different types in China. Biosci. Trends 2020, 14, 290–296. [Google Scholar] [CrossRef]
- Chen, H.; Qin, R.; Huang, Z.; Luo, W.; Zheng, P.; Huang, H.; Hu, H.; Wang, H.; Sun, B. Clinical relevance of serum Krebs von den Lungen-6 levels in patients with coronavirus disease 2019. Cytokine 2021, 148, 155513. [Google Scholar] [CrossRef]
- Karadeniz, H.; Avanoğlu Güler, A.; Özger, H.S.; Yıldız, P.A.; Erbaş, G.; Bozdayı, G.; Deveci Bulut, T.; Gülbahar, Ö.; Yapar, D.; Küçük, H.; et al. The Prognostic Value of Lung Injury and Fibrosis Markers, KL-6, TGF-β1, FGF-2 in COVID-19 Patients. Biomark. Insights 2022, 17, 11772719221135443. [Google Scholar] [CrossRef]
- Suryananda, T.D.; Yudhawati, R. Association of serum KL-6 levels on COVID-19 severity: A cross-sectional study design with purposive sampling. Ann. Med. Surg. 2021, 69, 102673. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 157) | RLK (n = 66) | KAI (n = 91) | p-Value |
|---|---|---|---|---|
| Age, yrs. | 61 [49–73.5] | 59.5 [48.5–70.3] | 62 [49–76] | 0.287 |
| Gender, M/F | 96/61 | 40/26 | 56/35 | 0.906 |
| BMI kg/m2 | 26 ± 1 | 30 ± 1 | 25 ± 1 | 0.01 * |
| SARS-CoV-2 severity/outcome | ||||
| WHO score (mean) | 6 | 5 | 6 | 0.38 + |
| Oxygen (yes/no) | 135/22 (86%/14%) | 54/12 (82%/18%) | 81/10 (89%/11%) | 0.25 + |
| ICU admission (yes/no) | 68/89 (43%/57%) | 26/40 (39%/61%) | 42/49 (46%/54%) | 0.4 + |
| IV (yes/no) | 20/137 (13%/87%) | 4/62 (6%/94%) | 16/75 (18%/82%) | 0.05 + |
| Death (yes/no) | 15/142 (10%/90%) | 3/63 (5%/95%) | 12/79 (13%/87%) | 0.07 + |
| Blood cell count | ||||
| Leucocyte, ×103/µL | 7 [5.2–9.95] | 7.2 [5.6–10.2] | 6.8 [4.8–9.6] | 0.252 |
| Lymphocyte, ×103/µL | 1.2 [0.7–1.7] | 1.5 [1.2–2] | 1 [0.6–1.5] | 0.002 |
| Neutrophil, ×103/µL | 5 ± 0 | 5 ± 0 | 5 ± 0 | 0.34 * |
| Thrombocyte, ×103/µL | 226 [169.3–326] | 321 [238.8–421] | 186 [126.5–240.5] | 0.000 |
| Serum biomarkers | ||||
| KL-6, U/mL at baseline | 407 [260.1–627] | 501.5 [291.3–742.5] | 381 [250–544] | 0.038 |
| KL-6, U/mL day 3 | 843 [505–1090] (n = 15) | 855 [467–1125] (n = 14) | n.a. (n = 1) | n.a. |
| KL-6, U/mL day 7 | 553.5 [370.8–789.5] (n = 50) | 653 [429.8–868] (n = 14) | 522.5 [366.3–773.5] (n = 36) | 0.336 |
| Delta KL-6, U/mL baseline to day 7 | 123 [29.5–270.3] (n = 50) | 57 [20.3–177] (n = 14) | 147 [30–348] (n = 36) | 0.120 |
| LDH, U/L | 337 ± 15 (n = 138) | 312 ± 13 (n = 52) | 352 ± 22 (n = 86) | 0.13 * |
| IL-6, pg/mL | 22.4 [8.1–69.5] (n = 87) | 7.8 [5.1–31.4] (n = 27) | 33.4 [12.4–86.3] (n = 60) | 0.000 |
| PCT, ng/mL | 0.11 [0.03–0.4] (n = 115) | .04 [0–4.8] (n = 31) | 0.13 [0.1–0.9] (n = 84) | 0.000 |
| CRP, mg/dL | 46 ± 11 (n = 143) | 5 ± 1 (n = 56) | 71 ± 16 (n = 87) | 0.01 * |
| NLR | 3 [2–6] (n = 127) | 3 [2–5] (n = 42) | 6 [3–8] (n = 85) | 0.889 |
| P/F | 112 [64–167.3] (n = 44) | (n = 0) | 112 [64–167.3] (n = 44) | n.a. |
| Variables | Moderate Disease WHO Score 4–5 (n = 89) | Severe Disease WHO Score 6–10 (n = 68) | p-Value |
|---|---|---|---|
| Age, yrs | 61 [48–73] | 62.5 [50–74] | 0.403 |
| Gender, M/F | 47/42 | 49/19 | 0.02 |
| BMI kg/m2 | 25 ± 1 | 28 ± 1 | 0.006 * |
| SARS-CoV-2 severity/outcome | |||
| Oxygen (yes/no) | 67/22 (75%/25%) | 68/0 (100%/0%) | <0.001 + |
| ICU admission (yes/no) | 0/89 (0%/100%) | 68/0 (100%/0%) | n.a. |
| IV (yes/no) | 0/89 (0%/100%) | 20/48 (30%/70%) | <0.001 + |
| Death (yes/no) | 0/89 (0%/100%) | 15/53 (23%/77%) | <0.001 + |
| Blood cell count | |||
| Leucocyte, ×103/µL | 6.3 [4.5–8.8] | 8 [6–10.6] | 0.014 |
| Lymphocyte, ×103/µL | 1.3 [0.8–1.8] | 0.9 [0.6–1.5] | 0.010 |
| Neutrophil, ×103/µL | 4 ± 0 | 5 ± 0 | 0.019 * |
| Thrombocyte, ×103/µL | 239 [170.8–327] | 214.5 [136–313.3] | 0.196 |
| Serum biomarkers | |||
| KL-6, U/mL at baseline | 364 [245–511.5] | 542.5 [350–838.3] | <0.001 |
| KL-6, U/mL day 3 | 826 [467–1263.3] (n = 6) | 843 [372.5–966] (n = 9) | 0.556 |
| KL-6, U/mL day 7 | 457.5 [328–657.5] (n = 22) | 631.5 [460.8–1018] (n = 28) | 0.013 |
| Delta KL-6, U/mL baseline to day 7 | 67.5 [24.3–150.8] (n = 22) | 179 [47.8–434] (n = 28) | 0.018 |
| LDH, U/L | 309 ± 12 (n = 81) | 377 ± 30 (n = 57) | 0.04 * |
| IL-6, pg/mL | 19.4 [8.2–38.8] (n = 48) | 49.3 [8.1–97] (n = 39) | 0.013 |
| PCT, ng/mL | 0.05 [0–0.25] (n = 60) | 0.2 [0.1–2] (n = 55) | <0.001 |
| CRP, mg/dL | 21 ± 9 (n = 79) | 77 ± 20 (n = 64) | 0.012 * |
| NLR | 3 [2–4] (n = 72) | 5 [1–8] (n = 55) | 0.016 |
| P/F | 146 [43.8–191.3] (n = 8) | 109.5 [64–155.5] (n = 36) | 0.447 |
| n | Correlation Coefficient (r) | p | |
|---|---|---|---|
| Age years | 157 | −0.052 | 0.52 |
| BMI kg/m2 | 124 | 0.164 | 0.068 |
| Blood cell count | |||
| Leucocyte, ×103/µL | 155 | 0.087 | 0.281 |
| Lymphocyte, ×103/µL | 131 | 0.151 | 0.086 |
| Neutrophil, ×103/µL | 128 | 0.199 | 0.024 |
| Thrombocyte, ×103/µL | 152 | 0.134 | 0.099 |
| Serum biomarkers | |||
| LDH, U/L | 138 | 0.244 | 0.004 |
| IL-6, pg/mL | 87 | 0.114 | 0.114 |
| PCT, ng/mL | 115 | 0.039 | 0.680 |
| CRP, mg/dL | 143 | 0.036 | 0.671 |
| NLR | 127 | 0.069 | 0.441 |
| P/F | 44 | 0.272 | 0.074 |
| Variables | Cut-Off | AUC | S.E. | Se | Sp | p Value |
|---|---|---|---|---|---|---|
| KL-6, U/mL baseline | 335 | 0.70 | 0.052 | 0.80 | 0.57 | 0.001 |
| LDH, U/L | 308 | 0.63 | 0.057 | 0.65 | 0.54 | 0.028 |
| NLR, ratio | 3.5 | 0.64 | 0.058 | 0.67 | 0.63 | 0.018 |
| PCT, ng/mL | 0.075 | 0.71 | 0.051 | 0.80 | 0.59 | 0.000 |
| CRP, mg/dL | 5.2 | 0.73 | 0.051 | 0.80 | 0.52 | 0.000 |
| Thrombocyte, ×103/µL | n.a. | 0.44 | 0.058 | n.a. | n.a. | 0.298 |
| Variables | KL-6 < 335 U/mL (n = 56) | KL-6 ≥ 335 U/mL (n = 101) | p-Value |
|---|---|---|---|
| Age, yrs | 64 [50.3–76.8] | 59 [48–72] | 0.248 |
| Gender, M/F | 30/26 | 66/35 | 0.148 |
| BMI kg/m2 | 25 ± 1 | 27 ± 1 | 0.124 * |
| SARS-CoV-2 severity/outcome | |||
| WHO score (mean) | 5 | 6 | 0.002 + |
| Oxygen (yes/no) | 46/10 (82%/18%) | 89/12 (88%/12%) | 0.301 + |
| ICU admission (yes/no) | 15/41 (27%/73%) | 53/48 (52%/48%) | 0.002 + |
| IV (yes/no) | 3/53 (5%/95%) | 17/84 (17%/83%) | 0.046 + |
| Death (yes/no) | 2/54 (4%/96%) | 13/88 (13%/87%) | 0.087 + |
| Blood cell count | |||
| Leucocyte, ×103/µL | 6.8 [4.8–9.3] | 7.3 [5.3–10.2] | 0.402 |
| Lymphocyte, ×103/µL | 1.2 [0.8–1.6] | 1.2 [0.6–1.9] | 0.888 |
| Neutrophil, ×103/µL | 4 ± 0 | 5 ± 0 | 0.348 * |
| Thrombocyte, ×103/µL | 199.5 [166–303.2] | 244 [170–353.5] | 0.137 |
| Serum biomarkers | |||
| KL-6, U/mL at baseline | 235.5 [180.3–262.8] | 553 [432.5–767] | <0.001 |
| KL-6, U/mL day 3 | n.a. (n = 2) | 867 [536–1161] (n = 13) | 0.027 |
| KL-6, U/mL day 7 | 279 [229.3–477.3] (n = 16) | 672.5 [508.5–954.3] (n = 34) | <0.001 |
| Delta KL-6, U/mL baseline to day 7 | 73.5 [17.5–235.5] (n = 16) | 161 [34–281.3] (n = 34) | 0.14 |
| LDH, U/L | 315 ± 16 (n = 52) | 355 ± 21 (n = 86) | 0.137 * |
| IL-6, pg/mL | 27.9 [8–64.2] (n = 36) | 21.7 [8.3–84.1] (n = 51) | 0.695 |
| PCT, ng/mL | 0.01 [0.02–0.3] (n = 47) | 0.13 [0.04–0.5] (n = 68) | 0.042 |
| CRP, mg/dL | 23 ± 11 (n = 52) | 60 ± 15 (n = 91) | 0.053 * |
| NLR | 3 [2–5] (n = 50) | 3 [2–6] (n = 77) | 0.613 |
| P/F | 126.5 [90.8–173.5] (n = 12) | 108.3 [62–161.3] (n = 32) | 0.392 |
| Variables | B | S.E. | Wald | p Value | Odds Ratio | 95% C.I. for OR | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Univariate | |||||||
| Age, yrs. | 0.009 | 0.018 | 0.248 | 0.618 | 1.009 | 0.974 | 1.046 |
| Gender (Male) | −0.836 | 0.622 | 1.805 | 0.179 | 0.433 | 0.128 | 1.467 |
| BMI, kg/m2 | 0.093 | 0.060 | 2.456 | 0.117 | 1.098 | 0.977 | 1.234 |
| KL-6, U/mL, baseline | 0.001 | 0.001 | 1.959 | 0.162 | 1.001 | 0.999 | 1.003 |
| LDH, U/L | 0.007 | 0.003 | 6.634 | 0.010 | 1.007 | 1.002 | 1.013 |
| NLR | 0.175 | 0.070 | 6.331 | 0.012 | 1.192 | 1.040 | 1.366 |
| PCT, ng/mL | 0.019 | 0.016 | 1.367 | 0.242 | 1.019 | 0.987 | 1.052 |
| CRP, mg/dL | 0.001 | 0.008 | 0.007 | 0.931 | 1.001 | 0.985 | 1.017 |
| Multivariate * | |||||||
| BMI, kg/m2 | 0.130 | 0.052 | 6.226 | 0.013 | 1.139 | 1.028 | 1.261 |
| NLR | 0.172 | 0.066 | 6.787 | 0.009 | 1.187 | 1.043 | 1.351 |
| PCT, ng/mL | 0.021 | 0.006 | 12.944 | 0.001 | 1.021 | 1.009 | 1.032 |
| LDH, U/L | 0.009 | 0.003 | 9.770 | 0.002 | 1.009 | 1.003 | 1.014 |
| Variables | B | S.E. | Wald | p Value | Odds Ratio | 95% C.I. for OR | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Univariate | |||||||
| Age, yrs. | 0.020 | 0.018 | 1.256 | 0.262 | 1.021 | 0.985 | 1.058 |
| Gender (Male) | −0.646 | 0.595 | 1.188 | 0.276 | 0.523 | 0.163 | 1.679 |
| BMI, kg/m2 | 0.143 | 0.058 | 5.993 | 0.014 | 1.153 | 1.029 | 1.293 |
| KL-6 cut-off 335 U/mL, baseline | 1.569 | 0.620 | 6.412 | 0.011 | 4.800 | 1.425 | 16.166 |
| LDH cut-off 308 U/L | 0.352 | 0.715 | 0.243 | 0.622 | 1.422 | 0.350 | 5.777 |
| NLR cut-off 3.5 | 0.692 | 0.635 | 1.188 | 0.276 | 1.997 | 0.576 | 6.929 |
| PCT cut-off 0.075 ng/mL | 1.399 | 0.634 | 4.867 | 0.027 | 4.050 | 1.169 | 14.033 |
| CRP cut-off 5.2 mg/dL | 1.276 | 0.718 | 3.162 | 0.075 | 3.583 | 0.878 | 14.629 |
| Multivariate * | |||||||
| BMI, kg/m2 | 0.135 | 0.051 | 6.899 | 0.009 | 1.144 | 1.035 | 1.266 |
| KL-6 cut-off 335 U/mL, baseline | 1.535 | 0.591 | 6.787 | 0.009 | 4.642 | 1.457 | 14.786 |
| NLR cut-off 3.5 | 0.953 | 0.578 | 2.719 | 0.099 | 2.594 | 0.835 | 8.058 |
| PCT cut-off 0.075 ng/mL | 1.374 | 0.611 | 5.057 | 0.025 | 3.952 | 1.193 | 13.092 |
| CRP cut-off 5.2 mg/dL | 1.398 | 0.661 | 4.473 | 0.034 | 4.047 | 1.108 | 14.784 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kattner, S.; Sutharsan, S.; Berger, M.M.; Limmer, A.; Jehn, L.-B.; Herbstreit, F.; Brenner, T.; Taube, C.; Bonella, F. Serum KL-6 as a Candidate Predictor of Outcome in Patients with SARS-CoV-2 Pneumonia. J. Clin. Med. 2023, 12, 6772. https://doi.org/10.3390/jcm12216772
Kattner S, Sutharsan S, Berger MM, Limmer A, Jehn L-B, Herbstreit F, Brenner T, Taube C, Bonella F. Serum KL-6 as a Candidate Predictor of Outcome in Patients with SARS-CoV-2 Pneumonia. Journal of Clinical Medicine. 2023; 12(21):6772. https://doi.org/10.3390/jcm12216772
Chicago/Turabian StyleKattner, Simone, Sivagurunathan Sutharsan, Marc Moritz Berger, Andreas Limmer, Lutz-Bernhard Jehn, Frank Herbstreit, Thorsten Brenner, Christian Taube, and Francesco Bonella. 2023. "Serum KL-6 as a Candidate Predictor of Outcome in Patients with SARS-CoV-2 Pneumonia" Journal of Clinical Medicine 12, no. 21: 6772. https://doi.org/10.3390/jcm12216772
APA StyleKattner, S., Sutharsan, S., Berger, M. M., Limmer, A., Jehn, L.-B., Herbstreit, F., Brenner, T., Taube, C., & Bonella, F. (2023). Serum KL-6 as a Candidate Predictor of Outcome in Patients with SARS-CoV-2 Pneumonia. Journal of Clinical Medicine, 12(21), 6772. https://doi.org/10.3390/jcm12216772