
Biweekly Versus Monthly Hyperimmune Globulin Therapy for Primary Cytomegalovirus Infection in Pregnancy

 , , ,
, , ,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
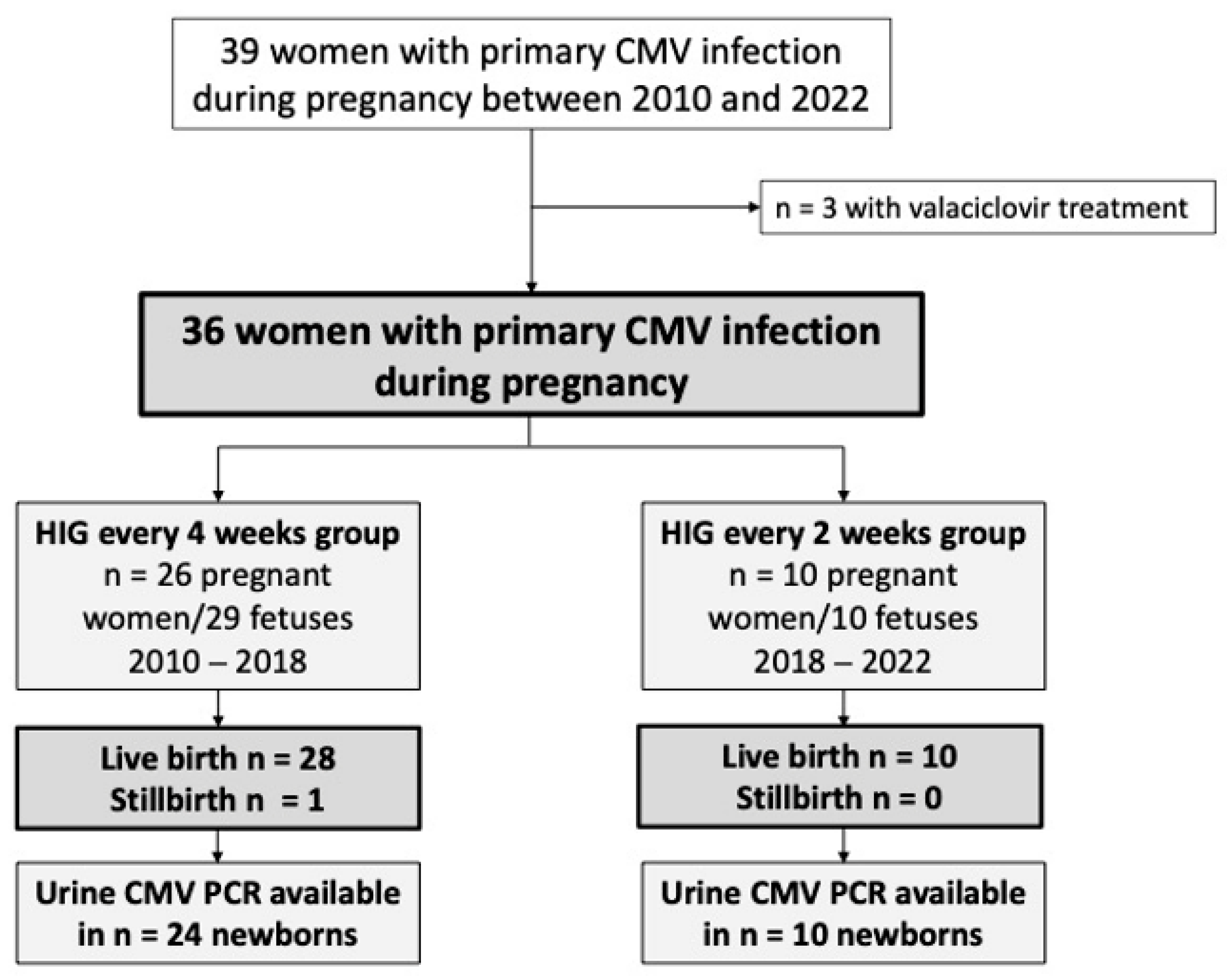
3.1. Study Population
3.2. HIG Administration
3.3. Virological Data of Pregnant Women with Primary CMV Infection
3.4. Maternal–Fetal Transmission Rate
3.5. Imaging Outcomes
3.6. Neonatal Characteristics and Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kenneson, A.; Cannon, M.J. Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Rev. Med. Virol. 2007, 17, 253–276. [Google Scholar] [CrossRef] [PubMed]
- Dollard, S.C.; Grosse, S.D.; Ross, D.S. New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection. Rev. Med. Virol. 2007, 17, 355–363. [Google Scholar] [CrossRef]
- Fowler, K.B.; Stagno, S.; Pass, R.F. Maternal age and congenital cytomegalovirus infection: Screening of two diverse newborn populations, 1980–1990. J. Infect. Dis. 1993, 168, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Stagno, S.; Reynolds, D.W.; Huang, E.S.; Thames, S.D.; Smith, R.J.; Alford, C.A. Congenital cytomegalovirus infection. N. Engl. J. Med. 1977, 296, 1254–1258. [Google Scholar] [CrossRef]
- Griffiths, P.D. Burden of disease associated with human cytomegalovirus and prospects for elimination by universal immunisation. Lancet Infect. Dis. 2012, 12, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Lancini, D.; Faddy, H.M.; Flower, R.; Hogan, C. Cytomegalovirus disease in immunocompetent adults. Med. J. Aust. 2014, 201, 578–580. [Google Scholar] [CrossRef]
- Rafailidis, P.I.; Mourtzoukou, E.G.; Varbobitis, I.C.; Falagas, M.E. Severe cytomegalovirus infection in apparently immunocompetent patients: A systematic review. Virol. J. 2008, 5, 47. [Google Scholar] [CrossRef]
- Bodéus, M.; Kabamba-Mukadi, B.; Zech, F.; Hubinont, C.; Bernard, P.; Goubau, P. Human cytomegalovirus in utero transmission: Follow-up of 524 maternal seroconversions. J. Clin. Virol. 2010, 47, 201–202. [Google Scholar] [CrossRef]
- Enders, G.; Daiminger, A.; Bäder, U.; Exler, S.; Enders, M. Intrauterine transmission and clinical outcome of 248 pregnancies with primary cytomegalovirus infection in relation to gestational age. J. Clin. Virol. 2011, 52, 244–246. [Google Scholar] [CrossRef]
- Lipitz, S.; Yinon, Y.; Malinger, G.; Yagel, S.; Levit, L.; Hoffman, C.; Rantzer, R.; Weisz, B. Risk of cytomegalovirus-associated sequelae in relation to time of infection and findings on prenatal imaging. Ultrasound Obstet. Gynecol. 2013, 41, 508–514. [Google Scholar] [CrossRef]
- Picone, O.; Vauloup-Fellous, C.; Cordier, A.G.; Guitton, S.; Senat, M.V.; Fuchs, F.; Ayoubi, J.M.; Grangeot Keros, L.; Benachi, A. A series of 238 cytomegalovirus primary infections during pregnancy: Description and outcome. Prenat. Diagn. 2013, 33, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Chatzakis, C.; Ville, Y.; Makrydimas, G.; Dinas, K.; Zavlanos, A.; Sotiriadis, A. Timing of primary maternal cytomegalovirus infection and rates of vertical transmission and fetal consequences. Am. J. Obstet. Gynecol. 2020, 223, 870–883.e11. [Google Scholar] [CrossRef]
- Pass, R.F.; Fowler, K.B.; Boppana, S.B.; Britt, W.J.; Stagno, S. Congenital cytomegalovirus infection following first trimester maternal infection: Symptoms at birth and outcome. J. Clin. Virol. 2006, 35, 216–220. [Google Scholar] [CrossRef]
- Britt, W. Controversies in the natural history of congenital human cytomegalovirus infection: The paradox of infection and disease in offspring of women with immunity prior to pregnancy. Med. Microbiol. Immunol. 2015, 204, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Ornoy, A.; Diav-Citrin, O. Fetal effects of primary and secondary cytomegalovirus infection in pregnancy. Reprod. Toxicol. 2006, 21, 399–409. [Google Scholar] [CrossRef]
- Kagan, K.O.; Hamprecht, K. Cytomegalovirus infection in pregnancy. Arch. Gynecol. Obstet. 2017, 296, 15–26. [Google Scholar] [CrossRef]
- Leruez-Ville, M.; Foulon, I.; Pass, R.; Ville, Y. Cytomegalovirus infection during pregnancy: State of the science. Am. J. Obstet. Gynecol. 2020, 223, 330–349. [Google Scholar] [CrossRef]
- Khalil, A.; Sotiriadis, A.; Chaoui, R.; da Silva Costa, F.; D’Antonio, F.; Heath, P.T.; Jones, C.; Malinger, G.; Odibo, A.; Prefumo, F.; et al. ISUOG Practice Guidelines: Role of ultrasound in congenital infection. Ultrasound Obstet. Gynecol. 2020, 56, 128–151. [Google Scholar] [CrossRef] [PubMed]
- Nigro, G.; Adler, S.P.; La Torre, R.; Best, A.M. Passive immunization during pregnancy for congenital cytomegalovirus infection. N. Engl. J. Med. 2005, 353, 1350–1362. [Google Scholar] [CrossRef]
- Nigro, G. Hyperimmune globulin in pregnancy for the prevention of congenital cytomegalovirus disease. Expert Rev. Anti-Infect. Ther. 2017, 15, 977–986. [Google Scholar] [CrossRef]
- Nigro, G.; Adler, S.P.; Parruti, G.; Anceschi, M.M.; Coclite, E.; Pezone, I.; Di Renzo, G.C. Immunoglobulin therapy of fetal cytomegalovirus infection occurring in the first half of pregnancy--a case-control study of the outcome in children. J. Infect. Dis. 2012, 205, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Buxmann, H.; Stackelberg, O.M.; Schlößer, R.L.; Enders, G.; Gonser, M.; Meyer-Wittkopf, M.; Hamprecht, K.; Enders, M. Use of cytomegalovirus hyperimmunoglobulin for prevention of congenital cytomegalovirus disease: A retrospective analysis. J. Perinat. Med. 2012, 40, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Blázquez-Gamero, D.; Galindo Izquierdo, A.; Del Rosal, T.; Baquero-Artigao, F.; Izquierdo Méndez, N.; Soriano-Ramos, M.; Rojo Conejo, P.; González-Tomé, M.I.; García-Burguillo, A.; Pérez Pérez, N.; et al. Prevention and treatment of fetal cytomegalovirus infection with cytomegalovirus hyperimmune globulin: A multicenter study in Madrid. J. Matern. Fetal Neonatal Med. 2019, 32, 617–625. [Google Scholar] [CrossRef]
- Revello, M.G.; Lazzarotto, T.; Guerra, B.; Spinillo, A.; Ferrazzi, E.; Kustermann, A.; Guaschino, S.; Vergani, P.; Todros, T.; Frusca, T.; et al. A randomized trial of hyperimmune globulin to prevent congenital cytomegalovirus. N. Engl. J. Med. 2014, 370, 1316–1326. [Google Scholar] [CrossRef]
- Hughes, B.L.; Clifton, R.G.; Rouse, D.J.; Saade, G.R.; Dinsmoor, M.J.; Reddy, U.M.; Pass, R.; Allard, D.; Mallett, G.; Fette, L.M.; et al. A Trial of Hyperimmune Globulin to Prevent Congenital Cytomegalovirus Infection. N. Engl. J. Med. 2021, 385, 436–444. [Google Scholar] [CrossRef]
- Kagan, K.O.; Enders, M.; Schampera, M.S.; Baeumel, E.; Hoopmann, M.; Geipel, A.; Berg, C.; Goelz, R.; De Catte, L.; Wallwiener, D.; et al. Prevention of maternal-fetal transmission of cytomegalovirus after primary maternal infection in the first trimester by biweekly hyperimmunoglobulin administration. Ultrasound Obs. Gynecol. 2019, 53, 383–389. [Google Scholar] [CrossRef]
- Nigro, G.; Adler, S.P. Cytomegalovirus infections during pregnancy. Curr. Opin. Obs. Gynecol. 2011, 23, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Yinon, Y.; Farine, D.; Yudin, M.H. Screening, diagnosis, and management of cytomegalovirus infection in pregnancy. Obs. Gynecol. Surv. 2010, 65, 736–743. [Google Scholar] [CrossRef]
- Sebghati, M.; Khalil, A. New evidence on prognostic features, prevention and treatment of congenital Cytomegalovirus infection. Curr. Opin. Obs. Gynecol. 2020, 32, 342–350. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | All Patients (n = 36) | HIG Every 4 Weeks (n = 26) | HIG Every 2 Weeks (n = 10) | p-Value |
|---|---|---|---|---|
| Maternal age, years | 30.5 (27.4–34.8) | 31.9 (26.9–35.6) | 31.5 (28.3–34.3) | 0.710 |
| Maternal body mass index, kg/m2 | 21.9 (20.2–26.3) | 22.5 (21.3–27.6) | 21.1 (19.0–22.2) | 0.236 |
| Nullipara, n (%) | 19 (52.8%) | 14 (53.8%) | 5 (50.0%) | 0.836 |
| Mode of conception, n (%) | 0.739 | |||
| Spontaneous | 33 (91.6%) | 23 (88.6%) | 10 (100.0%) | |
| In vitro fertilization | 1 (2.8%) | 1 (3.8%) | 0 (0.0%) | |
| Intracytoplasmic sperm injection | 1 (2.8%) | 1 (3.8%) | 0 (0.0%) | |
| Stimulation | 1 (2.8%) | 1 (3.8%) | 0 (0.0%) | |
| Median gestational age at first diagnosis, days (IQR) | 11.6 (8.6–14.0) | 11.8 (7.6–17.8) | 11.1 (8.6–12.7) | 0.471 |
| Median gestational age at first HIG administration, days (IQR) | 13.1 (11.9–17.0) | 13.5 (12.4–19.8) | 11.6 (9.4–13.4) | 0.063 |
| Median time between first diagnosis and administration, days | 5.0 (3.0–13.0) | 6.5 (4.0–39.2) | 3.5 (1.8–7.0) | 0.362 |
| All Patients n = 12 | HIG Every 4 Weeks n = 2 | HIG Every 2 Weeks n = 10 | p-Value | |
|---|---|---|---|---|
| Gestational age at amniocentesis, weeks (IQR) | 21.4 (20.6–21.8) | 23.9 (n.a.) | 21.4 (20.7–21.5) | 0.203 |
| Time interval between first presentation and amniocentesis, weeks (IQR) | 11.0 (8.0–12.0) | 11.5 (n.a.) | 9.0 (7.5–12.0) | 0.999 |
| Materno-fetal transmission rate at time of amniocentesis, n (%) | 4 (33.3%) | 1 (50.0%) | 3 (30.0%) | 0.584 |
| Parameters | All Patients (n = 36) | HIG Every 4 Weeks (n = 26) | HIG Every 2 Weeks (n = 10) | p-Value |
|---|---|---|---|---|
| CMV DNA qPCR | ||||
| Not detectable at first presentation, n (%) | 7 (19.4%) | 5 (19.2%) | 2 (20.0%) | 0.958 |
| Detectable at first presentation, n (%) | 29 (80.6%) | 21 (80.8%) | 8 (80.0%) | |
| CMV viral load in cases with detectable CMV DNA qPCR, co/mL | 788.0 (218.0–1700.0) | 1305.0 (424.5–3725.0) | 174.0 (116.0–259.0) | 0.006 |
| CMV -IgM at first presentation, n (%) | ||||
| CMV IgM negative | 1 (2.8%) | 0 (0.0%) | 1 (10.0%) | 0.222 |
| CMV IgM positive | 34 (94.4%) | 25 (96.2%) | 9 (90.0%) | |
| CMV IgM borderline | 1 (2.8%) | 1 (3.8%) | 0 (0.0%) | |
| CMV IgG at first presentation, n (%) | ||||
| CMV IgG negative | 0 (0%) | 0 (0%) | 0 (0%) | 0.491 |
| CMV IgG positive | 36 (100%) | 26 (100%) | 10 (100%) | |
| CMV IgG avidity at first presentation, n (%) | ||||
| Low avidity | 30 (83.3%) | 22 (84.6%) | 8 (80.0%) | 0.679 |
| Borderline avidity | 5 (13.9%) | 3 (11.6%) | 2 (20.0%) | |
| Seroconversion | 1 (2.8%) | 1 (3.8%) | 0 (0.0%) |
| Case | GA 1 at Diagnosis in Weeks | Fetal Ultrasound Abnormalities | Fetal MRI 2 Abnormalities | HIG Interval | Findings at Birth | Hearing Test, Eye Examination, Neurological Outcome Two Years after Birth |
|---|---|---|---|---|---|---|
| 1 | 17.1 | - | Small temporal cysts | Every 4 weeks | Intracerebral cystic lesions at neonatal ultrasound | No abnormalities |
| 2 | 12.9 | Oligohydramnios | - | Every 4 weeks | pPROM 3 at 34 + 2 weeks, preterm delivery in 34 + 4 weeks | No abnormalities |
| 3 | 11.0 | Fetal growth retardation (<3. percentile) | Splenomegaly, subependymal cysts, leucencephalopathy, placental edema | Every 4 weeks | Stillbirth at 40.0 weeks, MRI 2: profound intracerebral lesions Histology: large infarcts in the placenta | - |
| 4 | 11.6 | Intraventricular adhesion | - | Every 2 weeks | Asymptomatic, normal BERA 4, eye exam, neurological exam, and neurological development | No abnormalities |
| 5 | 11.6 | - | Placental anomalies in correlation with fetal inflammatory response syndrome | Every 4 weeks | Asymptomatic, normal BERA 4, eye exam, neurological exam, and neurological development | No abnormalities |
| 6 | 22.7 | - | Second MRI†: Bilateral small cysts in the medial temporal lobe | Every 4 weeks | Asymptomatic, normal BERA 4, eye exam, neurological exam, and neurological development | No abnormalities |
| 7 | 7.3 | - | Every 4 weeks | Asymptomatic, normal BERA 4, eye exam, neurological exam, and neurological development | No abnormalities | |
| 8 | 13 | - | Every 4 weeks | Asymptomatic, normal BERA 4, eye exam, neurological exam, and neurological development | No abnormalities | |
| 9 | 8.6 | - | Every 2 weeks | Asymptomatic, normal BERA 4, eye exam, neurological exam, and neurological development | No abnormalities | |
| 10 | 9.9 | - | Every 2 weeks | Asymptomatic, normal BERA 4, eye exam, neurological exam, and neurological development | No abnormalities | |
| 11 | 23.6 | - | Every 4 weeks | Asymptomatic, normal BERA 4, eye exam, neurological exam, and neurological development | No abnormalities |
| Parameters | All Patients (n = 39) | HIG Every 4 Weeks (n = 29) | HIG Every 2 Weeks (n = 10) | p-Value |
|---|---|---|---|---|
| Sex, n (%) | 0.313 | |||
| Male | 17 (34.6%) | 11 (37.9%) | 6 (60.0%) | |
| Female | 18 (46.1%) | 14 (48.3%) | 4 (40.0%) | |
| Unknown | 4 (10.3%) | 4 (13.8%) | 0 (0.0%) | |
| Singleton pregnancy, n (%) | 33 (84.6%) | 23 (79.3%) | 10 (100.0%) | 0.118 |
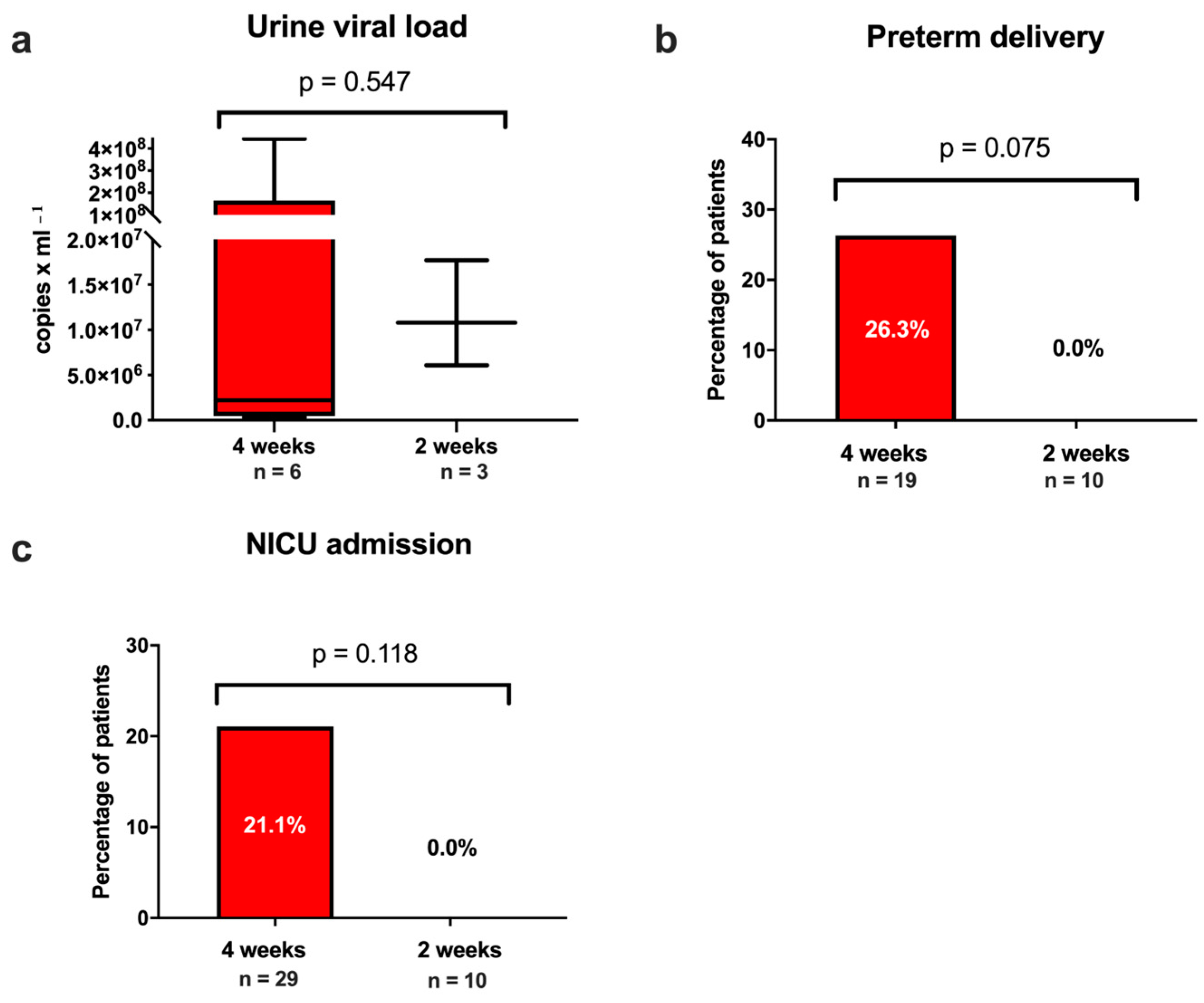
| Preterm birth < 37 weeks, n (%) | 5/29 (17.2%) | 5/19 (26.3%) | 0/10 (0.0%) | 0.075 |
| Gestational age at delivery, weeks | 38.9 (36.6–40.0) | 38.6 (36.3–40.0) | 39.4 (38.2–40.3) | 0.734 |
| Birthweight, grams | 3440.0 (2955.0–3655.0) | 3460.0 (2710.0–3760.0) | 3365.0 (3067.5–3507.5) | 0.191 |
| Mode of birth, n (%) | 0.470 | |||
| Vaginal delivery | 16/30 (53.3%) | 11/20 (55.0%) | 5/10 (50.0%) | |
| ventouse | 1/30 (3.3%) | 0/20 (0.0%) | 1/10 (10.0%) | |
| Elective cesarean section | 12/30 (40.0%) | 8/20 (40.0%) | 4/10 (40.0%) | |
| Emergency cesarean section | 1/30 (3.3%) | 0/20 (0.0%) | 1/10 (10.0%) | |
| Neonatal unit admission, n (%) | 4/29 (13.8%) | 4/19 (21.1%) | 0/10 (0.0%) | 0.118 |
| Stillbirth, n (%) | 1/39 (2.6%) | 1/29 (3.4%) | 0/10 (0.0%) | 0.552 |
| Congenital CMV infection, n (%) | 11/34 (32.4%) | 8/24 (33.3%) | 3/10 (30.0%) | 0.850 |
| Urine CMV viral load in cases with detectable CMVDNA qPCR | 6.1 × 106 (9.5 × 105–4.4 × 107) | 2.2 × 106 (4.9 × 105–1.6 × 108) | 1.1 × 107 (6.1 × 106–1.7 × 107) | 0.547 |
| Antibodies in cord blood, n (%) | 8/14 (57.1%) | 6/11 (54.5%) | 2/3 (66.7%) | 0.707 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schirwani-Hartl, N.; Palmrich, P.; Haberl, C.; Perkmann-Nagele, N.; Kiss, H.; Berger, A.; Rittenschober-Böhm, J.; Kasprian, G.; Kienast, P.; Khalil, A.; et al. Biweekly Versus Monthly Hyperimmune Globulin Therapy for Primary Cytomegalovirus Infection in Pregnancy. J. Clin. Med. 2023, 12, 6776. https://doi.org/10.3390/jcm12216776
Schirwani-Hartl N, Palmrich P, Haberl C, Perkmann-Nagele N, Kiss H, Berger A, Rittenschober-Böhm J, Kasprian G, Kienast P, Khalil A, et al. Biweekly Versus Monthly Hyperimmune Globulin Therapy for Primary Cytomegalovirus Infection in Pregnancy. Journal of Clinical Medicine. 2023; 12(21):6776. https://doi.org/10.3390/jcm12216776
Chicago/Turabian StyleSchirwani-Hartl, Nawa, Pilar Palmrich, Christina Haberl, Nicole Perkmann-Nagele, Herbert Kiss, Angelika Berger, Judith Rittenschober-Böhm, Gregor Kasprian, Patric Kienast, Asma Khalil, and et al. 2023. "Biweekly Versus Monthly Hyperimmune Globulin Therapy for Primary Cytomegalovirus Infection in Pregnancy" Journal of Clinical Medicine 12, no. 21: 6776. https://doi.org/10.3390/jcm12216776
APA StyleSchirwani-Hartl, N., Palmrich, P., Haberl, C., Perkmann-Nagele, N., Kiss, H., Berger, A., Rittenschober-Böhm, J., Kasprian, G., Kienast, P., Khalil, A., & Binder, J. (2023). Biweekly Versus Monthly Hyperimmune Globulin Therapy for Primary Cytomegalovirus Infection in Pregnancy. Journal of Clinical Medicine, 12(21), 6776. https://doi.org/10.3390/jcm12216776