
Effects of Extracorporeal Shock Wave Therapy in Patients with Mild-to-Moderate Carpal Tunnel Syndrome: An Updated Systematic Review with Meta-Analysis
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
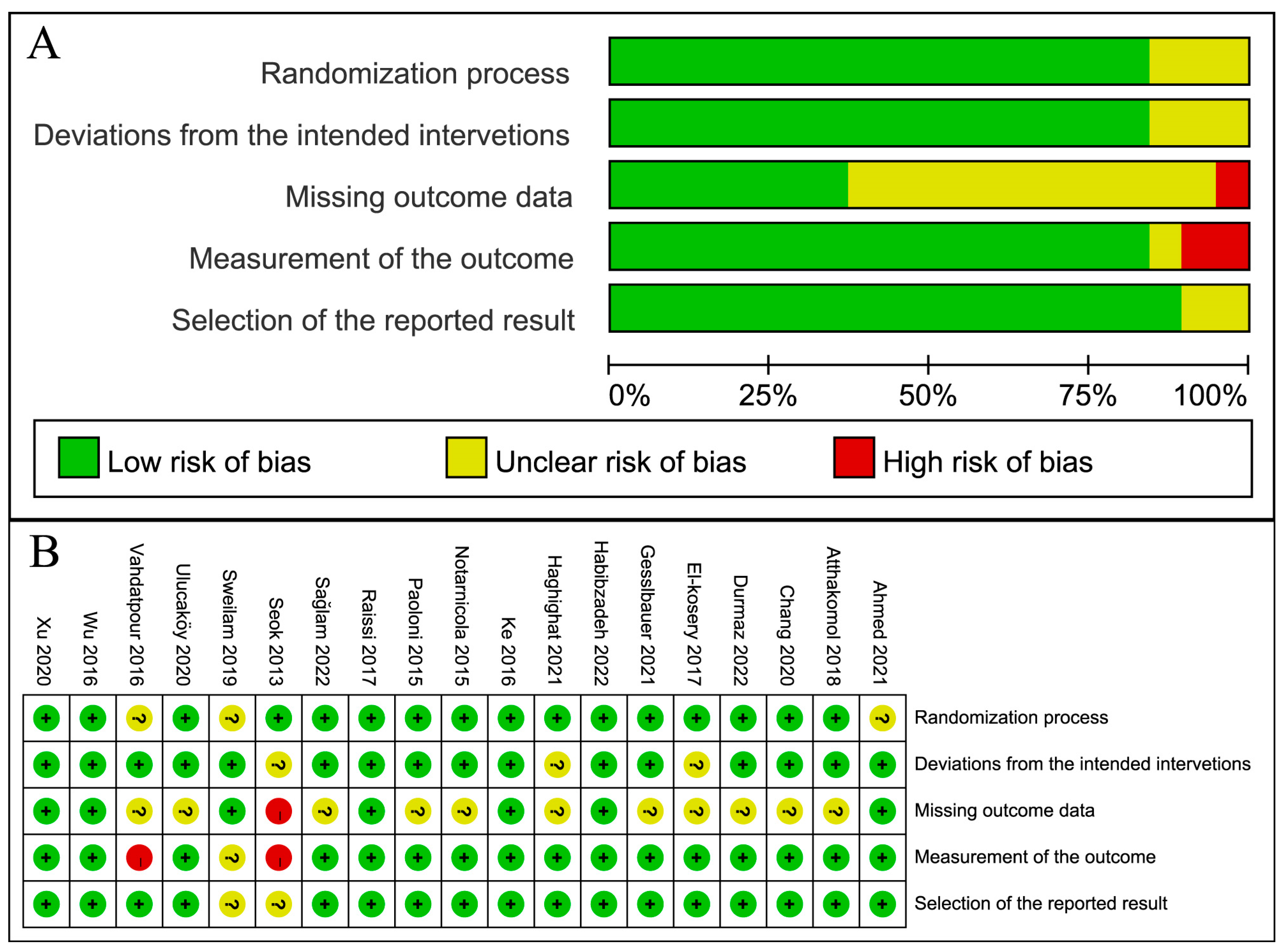
2.4. Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Search Results and Study Characteristics
3.2. Risk of Bias in Included Studies
3.3. ESWT versus Control
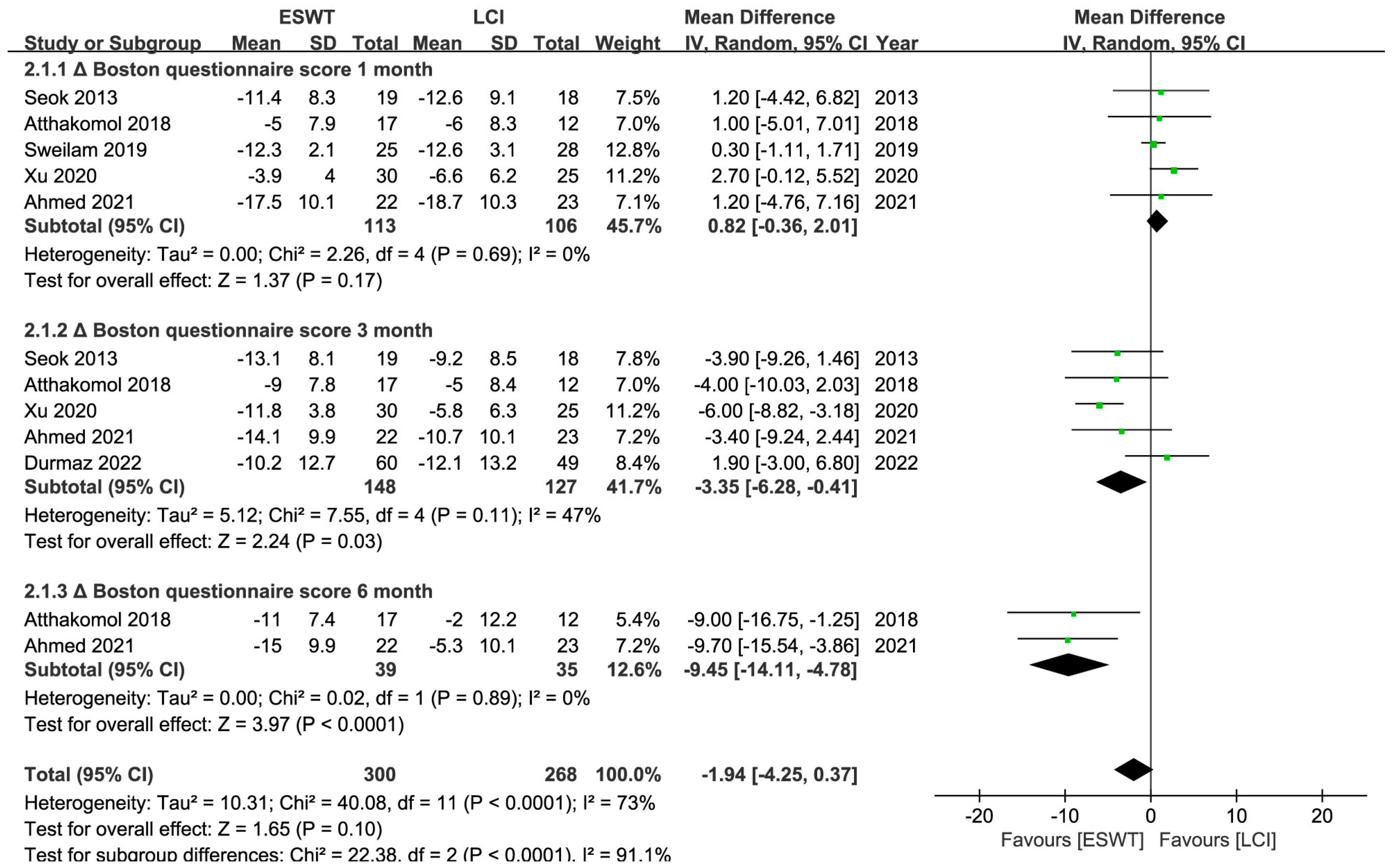
3.4. ESWT versus LCI
3.5. ESWT versus Other Interventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atroshi, I.; Gummesson, C.; Johnsson, R.; Ornstein, E.; Ranstam, J.; Rosén, I. Prevalence of carpal tunnel syndrome in a general population. JAMA 1999, 282, 153–158. [Google Scholar] [CrossRef]
- Padua, L.; Coraci, D.; Erra, C.; Pazzaglia, C.; Paolasso, I.; Loreti, C.; Caliandro, P.; Hobson-Webb, L.D. Carpal tunnel syndrome: Clinical features, diagnosis, and management. Lancet Neurol. 2016, 15, 1273–1284. [Google Scholar] [CrossRef]
- Werner, R.A.; Andary, M. Carpal tunnel syndrome: Pathophysiology and clinical neurophysiology. Clin. Neurophysiol. 2002, 113, 1373–1381. [Google Scholar] [CrossRef]
- Padua, L.; Di Pasquale, A.; Pazzaglia, C.; Liotta, G.A.; Librante, A.; Mondelli, M. Systematic review of pregnancy-related carpal tunnel syndrome. Muscle Nerve 2010, 42, 697–702. [Google Scholar] [CrossRef]
- Pourmemari, M.H.; Shiri, R. Diabetes as a risk factor for carpal tunnel syndrome: A systematic review and meta-analysis. Diabet. Med. A J. Br. Diabet. Assoc. 2016, 33, 10–16. [Google Scholar] [CrossRef]
- Shiri, R. Hypothyroidism and carpal tunnel syndrome: A meta-analysis. Muscle Nerve 2014, 50, 879–883. [Google Scholar] [CrossRef]
- Shiri, R.; Falah-Hassani, K. Computer use and carpal tunnel syndrome: A meta-analysis. J. Neurol. Sci. 2015, 349, 15–19. [Google Scholar] [CrossRef]
- Shiri, R.; Pourmemari, M.H.; Falah-Hassani, K.; Viikari-Juntura, E. The effect of excess body mass on the risk of carpal tunnel syndrome: A meta-analysis of 58 studies. Obes. Rev. 2015, 16, 1094–1104. [Google Scholar] [CrossRef]
- Kaile, E.; Bland, J.D.P. Safety of corticosteroid injection for carpal tunnel syndrome. J. Hand Surg. Eur. Vol. 2018, 43, 296–302. [Google Scholar] [CrossRef]
- Schroeder, A.N.; Tenforde, A.S.; Jelsing, E.J. Extracorporeal Shockwave Therapy in the Management of Sports Medicine Injuries. Curr. Sports Med. Rep. 2021, 20, 298–305. [Google Scholar] [CrossRef]
- Mariotto, S.; de Prati, A.C.; Cavalieri, E.; Amelio, E.; Marlinghaus, E.; Suzuki, H. Extracorporeal shock wave therapy in inflammatory diseases: Molecular mechanism that triggers anti-inflammatory action. Curr. Med. Chem. 2009, 16, 2366–2372. [Google Scholar] [CrossRef]
- Wang, C.J. Extracorporeal shockwave therapy in musculoskeletal disorders. J. Orthop. Surg. Res. 2012, 7, 11. [Google Scholar] [CrossRef]
- Wang, C.J.; Yang, Y.J.; Huang, C.C. The effects of shockwave on systemic concentrations of nitric oxide level, angiogenesis and osteogenesis factors in hip necrosis. Rheumatol. Int. 2011, 31, 871–877. [Google Scholar] [CrossRef]
- Kim, J.C.; Jung, S.H.; Lee, S.U.; Lee, S.Y. Effect of extracorporeal shockwave therapy on carpal tunnel syndrome: A systematic review and meta-analysis of randomized controlled trials. Medicine 2019, 98, e16870. [Google Scholar] [CrossRef]
- Xie, Y.; Zhang, C.; Liang, B.; Wang, J.; Wang, L.; Wan, T.; Xu, F.; Lei, L. Effects of shock wave therapy in patients with carpal tunnel syndrome: A systematic review and meta-analysis. Disabil. Rehabil. 2022, 44, 177–188. [Google Scholar] [CrossRef]
- Chen, K.T.; Chen, Y.P.; Kuo, Y.J.; Chiang, M.H. Extracorporeal Shock Wave Therapy Provides Limited Therapeutic Effects on Carpal Tunnel Syndrome: A Systematic Review and Meta-Analysis. Medicina 2022, 58, 677. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Padua, L.; LoMonaco, M.; Gregori, B.; Valente, E.M.; Padua, R.; Tonali, P. Neurophysiological classification and sensitivity in 500 carpal tunnel syndrome hands. Acta Neurol. Scand. 1997, 96, 211–217. [Google Scholar] [CrossRef]
- Leite, J.C.; Jerosch-Herold, C.; Song, F. A systematic review of the psychometric properties of the Boston Carpal Tunnel Questionnaire. BMC Musculoskelet. Disord. 2006, 7, 78. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. S11), S240–S252. [Google Scholar] [CrossRef]
- Werner, R.A.; Andary, M. Electrodiagnostic evaluation of carpal tunnel syndrome. Muscle Nerve 2011, 44, 597–607. [Google Scholar] [CrossRef]
- Burton, C.L.; Chesterton, L.S.; Chen, Y.; van der Windt, D.A. Clinical Course and Prognostic Factors in Conservatively Managed Carpal Tunnel Syndrome: A Systematic Review. Arch. Phys. Med. Rehabil. 2016, 97, 836–852. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Measures of interrater agreement. J. Thorac. Oncol. 2011, 6, 6–7. [Google Scholar] [CrossRef]
- Ahmed, L.S.; Ismaiel, A.H.; Taha, N.H.J.J.o.M.i.S.R. Comparison between the effect of single-dose radial extracorporeal shock wave and local corticosteroid injection in treatment of patients with carpal tunnel syndrome. J. Med. Sci. Res. 2021, 4, 202. [Google Scholar] [CrossRef]
- Atthakomol, P.; Manosroi, W.; Phanphaisarn, A.; Phrompaet, S.; Iammatavee, S.; Tongprasert, S. Comparison of single-dose radial extracorporeal shock wave and local corticosteroid injection for treatment of carpal tunnel syndrome including mid-term efficacy: A prospective randomized controlled trial. BMC Musculoskelet. Disord. 2018, 19, 32. [Google Scholar] [CrossRef]
- Chang, C.Y.; Chen, L.C.; Chou, Y.C.; Li, T.Y.; Ho, T.Y.; Wu, Y.T. The Effectiveness of Platelet-Rich Plasma and Radial Extracorporeal Shock Wave Compared with Platelet-Rich Plasma in the Treatment of Moderate Carpal Tunnel Syndrome. Pain Med. 2020, 21, 1668–1675. [Google Scholar] [CrossRef]
- EL-KOSERY, S.M.; EL-REFAYE, G.E.; EL-KHOLY, A.-E.G.; EL-AHWAL, A.M. Extracorpeal Shock Wave Therapy Versus Ultrasound for Carpal Tunnel Syndrome in Post Menopausal Women. Med. J. Cairo Univ. 2017, 85, 2895–2901. Available online: www.medicaljournalofcairouniversity.net (accessed on 8 December 2017).
- Gesslbauer, C.; Mickel, M.; Schuhfried, O.; Huber, D.; Keilani, M.; Crevenna, R. Effectiveness of focused extracorporeal shock wave therapy in the treatment of carpal tunnel syndrome: A randomized, placebo-controlled pilot study. Wien. Klin. Wochenschr. 2021, 133, 568–577. [Google Scholar] [CrossRef]
- Habibzadeh, A.; Mousavi-Khatir, R.; Saadat, P.; Javadian, Y. The effect of radial shockwave on the median nerve pathway in patients with mild-to-moderate carpal tunnel syndrome: A randomized clinical trial. J. Orthop. Surg. Res. 2022, 17, 46. [Google Scholar] [CrossRef]
- Haghighat, S.; Khosravi, M.; Rezaei, M. The Effect of Shock Wave and Phonophoresis in the Improvement of the Clinical Symptoms and Function of Patients with Mild to Moderate Carpal Tunnel Syndrome: A Clinical Trial. Med. J. Islam. Repub. Iran 2021, 35, 179. [Google Scholar] [CrossRef]
- Ke, M.J.; Chen, L.C.; Chou, Y.C.; Li, T.Y.; Chu, H.Y.; Tsai, C.K.; Wu, Y.T. The dose-dependent efficiency of radial shock wave therapy for patients with carpal tunnel syndrome: A prospective, randomized, single-blind, placebo-controlled trial. Sci. Rep. 2016, 6, 38344. [Google Scholar] [CrossRef]
- Koçak Ulucaköy, R.; Yurdakul, F.G.; Bodur, H. Extracorporeal shock wave therapy as a conservative treatment option for carpal tunnel syndrome: A double-blind, prospective, randomized, placebo-controlled study. Turk. J. Phys. Med. Rehabil. 2020, 66, 388–397. [Google Scholar] [CrossRef]
- Notarnicola, A.; Maccagnano, G.; Tafuri, S.; Fiore, A.; Pesce, V.; Moretti, B. Comparison of shock wave therapy and nutraceutical composed of Echinacea angustifolia, alpha lipoic acid, conjugated linoleic acid and quercetin (perinerv) in patients with carpal tunnel syndrome. Int. J. Immunopathol. Pharmacol. 2015, 28, 256–262. [Google Scholar] [CrossRef]
- Öztürk Durmaz, H.; Tuncay, F.; Durmaz, H.; Erdem, H.R. Comparison of Radial Extracorporeal Shock Wave Therapy and Local Corticosteroid Injection Effectiveness in Patients With Carpal Tunnel Syndrome: A Randomized Controlled Study. Am. J. Phys. Med. Rehabil. 2022, 101, 685–692. [Google Scholar] [CrossRef]
- Paoloni, M.; Tavernese, E.; Cacchio, A.; D’Orazi, V.; Ioppolo, F.; Fini, M.; Santilli, V.; Mangone, M. Extracorporeal shock wave therapy and ultrasound therapy improve pain and function in patients with carpal tunnel syndrome. A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2015, 51, 521–528. [Google Scholar] [PubMed]
- Raissi, G.R.; Ghazaei, F.; Forogh, B.; Madani, S.P.; Daghaghzadeh, A.; Ahadi, T. The Effectiveness of Radial Extracorporeal Shock Waves for Treatment of Carpal Tunnel Syndrome: A Randomized Clinical Trial. Ultrasound Med. Biol. 2017, 43, 453–460. [Google Scholar] [CrossRef]
- Sağlam, G.; Çetinkaya Alişar, D.; Özen, S. Physical therapy versus radial extracorporeal shock wave therapy in the treatment of carpal tunnel syndrome: A randomized-controlled study. Turk. J. Phys. Med. Rehabil. 2022, 68, 126–135. [Google Scholar] [CrossRef]
- Seok, H.; Kim, S.H. The effectiveness of extracorporeal shock wave therapy vs. local steroid injection for management of carpal tunnel syndrome: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2013, 92, 327–334. [Google Scholar] [CrossRef]
- Sweilam, G.; Elshahaly, M.; Hefny, M.J.B.J. Extracorporeal shock wave therapy (ESWT) versus local steroids injection in the management of carpal tunnel syndrome. Biomed. J. Sci. Tech. Res. 2019, 1, 4. [Google Scholar] [CrossRef]
- Vahdatpour, B.; Kiyani, A.; Dehghan, F. Effect of extracorporeal shock wave therapy on the treatment of patients with carpal tunnel syndrome. Adv. Biomed. Res. 2016, 5, 120. [Google Scholar] [CrossRef]
- Wu, Y.T.; Ke, M.J.; Chou, Y.C.; Chang, C.Y.; Lin, C.Y.; Li, T.Y.; Shih, F.M.; Chen, L.C. Effect of radial shock wave therapy for carpal tunnel syndrome: A prospective randomized, double-blind, placebo-controlled trial. J. Orthop. Res. 2016, 34, 977–984. [Google Scholar] [CrossRef]
- Xu, D.; Ma, W.; Jiang, W.; Hu, X.; Jiang, F.; Mao, C.; Wang, Y.; Fang, L.; Luo, N.; Li, H.; et al. A randomized controlled trial: Comparing extracorporeal shock wave therapy versus local corticosteroid injection for the treatment of carpal tunnel syndrome. Int. Orthop. 2020, 44, 141–146. [Google Scholar] [CrossRef]
- Ciampa, A.R.; de Prati, A.C.; Amelio, E.; Cavalieri, E.; Persichini, T.; Colasanti, M.; Musci, G.; Marlinghaus, E.; Suzuki, H.; Mariotto, S. Nitric oxide mediates anti-inflammatory action of extracorporeal shock waves. FEBS Lett. 2005, 579, 6839–6845. [Google Scholar] [CrossRef]
- Mense, S.; Hoheisel, U. Shock wave treatment improves nerve regeneration in the rat. Muscle Nerve 2013, 47, 702–710. [Google Scholar] [CrossRef]
- Li, W.; Dong, C.; Wei, H.; Xiong, Z.; Zhang, L.; Zhou, J.; Wang, Y.; Song, J.; Tan, M. Extracorporeal shock wave therapy versus local corticosteroid injection for the treatment of carpal tunnel syndrome: A meta-analysis. J. Orthop. Surg. Res. 2020, 15, 556. [Google Scholar] [CrossRef]
- Graham, B.; Peljovich, A.E.; Afra, R.; Cho, M.S.; Gray, R.; Stephenson, J.; Gurman, A.; MacDermid, J.; Mlady, G.; Patel, A.T.; et al. The American Academy of Orthopaedic Surgeons Evidence-Based Clinical Practice Guideline on: Management of Carpal Tunnel Syndrome. J. Bone Jt. Surg. Am. Vol. 2016, 98, 1750–1754. [Google Scholar] [CrossRef]
- Brinks, A.; Koes, B.W.; Volkers, A.C.; Verhaar, J.A.; Bierma-Zeinstra, S.M. Adverse effects of extra-articular corticosteroid injections: A systematic review. BMC Musculoskelet. Disord. 2010, 11, 206. [Google Scholar] [CrossRef]
- Guo, J.; Hai, H.; Ma, Y. Application of extracorporeal shock wave therapy in nervous system diseases: A review. Front. Neurol. 2022, 13, 963849. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Wrists (Patients), n | Age, Years Mean ± SD | Sex (M/F) | Symptom Duration, Weeks Mean ± SD | Follow-up, Weeks | ESWT Protocol | Non-ESWT Protocol | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ESWT | Non-ESWT | ESWT | Non-ESWT | ESWT | Non-ESWT | ESWT | Non-ESWT | Intervention | Frequency (Hz) | Intensity | Total Shocks | Sessions (Time Period) | |||||
| ESWT versus Control | |||||||||||||||||
| Ke, M.J., et al. [32] | 2016 | China | 30 (23) | 30 (23) | 56.33 ± 1.48 | 58.13 ± 1.13 | 24/6 | 25/5 | 34.27 ± 5.85 | 35.34 ± 7.45 | 4, 10, 14 | rESWT + night splint | 5 | 4 bar | 2000 | 3 (3 weeks) | Sham rESWT + night splint |
| Vahdatpour, B., et al. [41] | 2016 | Iran | NA (28) | NA (27) | 51.5 ± 8.5 | 49 ± 7.3 | NA | NA | 14 ± 1.39 | 17.86 ± 2.14 | 12, 24 | fESWT + night splint + drugs | 3 | 0.05, 0.07, 0.1, 0.15 mJ/mm2 | 800, 900, 1000, 1100 | 4 (4 weeks) | Sham fESWT + night splint + drugs |
| Wu, Y.T., et al. [42] | 2016 | China | 20 (17) | 20 (17) | 54.7 ± 7.96 | 57.8 ± 6.51 | 18/2 | 17/3 | 34.1 ± 33.11 | 36.1 ± 30.8 | 1, 4, 8, 12 | rESWT + night splint | 5 | 4 bar | 2000 | 3 (3 weeks) | Sham rESWT + night splint |
| Raissi, G.R., et al. [37] | 2017 | Iran | NA (20) | NA (20) | 46.1 ± 1.95 | 46.65 ± 2.23 | 18/2 | 19/1 | NA | NA | 3, 8, 12 | rESWT + night splint | 6 | 1.5 bar | 1000 | 3 (3 weeks) | Night splint |
| Chang, C.Y., et al. [27] | 2020 | China | 32 (20) | 32 (20) | 56.47 ± 1.41 | 58.63 ± 1.72 | 29/3 | 30/2 | 63.5 ± 7.55 | 61.34 ± 15.48 | 4, 12, 24 | rESWT + PRP | 5 | 4 bar | 2000 | 1 | Sham rESWT + PRP |
| Koçak Ulucaköy, R., et al. [33] | 2020 | Turkey | 66 (47) | 75 (50) | 48.4 ± 10.1 | 48.5 ± 9.8 | 39/8 | 47/3 | 33.7 ± 38.1 | 24.8 ± 31.5 | 4, 12 | rESWT + night splint | 5 | 0.05 mJ/mm2 | 1000 | 3 (3 weeks) | Sham rESWT + night splint |
| Gesslbauer, C., et al. [29] | 2021 | Austria | NA (10) | NA (10) | 55.8 ± 4.66 | 54 ± 17.4 | 8/2 | 6/4 | 29 ± 32.89 | 33.6 ± 44.26 | 3, 12 | fESWT + night splint | 4 | 0.05 mJ/mm2 | 500 | 3 (3 weeks) | Sham fESWT + night splint |
| Haghighat, S., et al. [31] | 2021 | Iran | NA (20) | NA (20) | 50.1 ± 8.14 | 51.13 ± 9.06 | 18/2 | 14/6 | NA | NA | 4, 8 | fESWT + night splint + drugs | 3 | 0.05, 0.07, 0.1, 0.15 mJ/mm2 | 800, 900, 1000, 1100 | 4 (4 weeks) | Night splint + drugs |
| Habibzadeh, A., et al. [30] | 2022 | Iran | NA (20) | NA (20) | 45.54 ± 11.90 | 51 ± 7.77 | 18/2 | 15/5 | NA | NA | 1, 4 | rESWT + physiotherapy + night splint + drugs | 6 | 1.5 bar | 1500 | 4 (10 weeks) | Physiotherapy + night splint + drugs |
| Sağlam, G., et al. [38] | 2022 | Turkey | 42 (32) | 41 (32) | 53.8 ± 11.8 | 53.4 ± 10.9 | 34/8 | 29/12 | 11.4 ± 11.1 | 10.6 ± 6.7 | 3, 12 | rESWT + night splint + exercise | 5 | 4 bar | 2000 | 3 (3 weeks) | Night splint + exercise |
| ESWT versus LCI | |||||||||||||||||
| Seok, H., et al. [39] | 2013 | Korea | 19 (15) | 18 (16) | 54.03 ± 19.47 | 49.67 ± 18.83 | 12/3 | 14/2 | 9.76 ± 3.57 | 10.15 ± 2.3 | 4, 12 | fESWT | 6 | 0.09–0.29 mJ/mm2 | 1000 | 1 | 1 mL lidocaine + 1 mL triamcinolone acetonide (40 mg) |
| Atthakomol, P., et al. [26] | 2018 | Thailand | 17 (13) | 12 (12) | 46 ± 9 | 53 ± 12 | 8/5 | 11/1 | 25.1 ± 19.3 | 26.4 ± 17.9 | 1, 4, 12, 24 | rESWT | 15 | 4 bar | 5000 | 1 | 1 mL lidocaine + 1 mL triamcinolone (10 mg) |
| Sweilam, G., et al. [40] | 2019 | Egypt | NA (25) | NA (28) | 37.6 ± 8.5 | 36.8 ± 8.8 | 21/4 | 23/5 | 25.1 ± 19.3 | 26.4 ± 17.9 | 2, 4 | fESWT | 10 | 2 bar | 2500 | 2 (2 weeks) | 1 mL triamcinolone acetonide (40 mg) |
| Xu, D., et al. [43] | 2020 | China | NA (30) | NA (25) | 47.2 ± 1.86 | 46.9 ± 1.76 | 25/5 | 21/4 | 2.9 ± 0.8 | 2.8 ± 0.7 | 3, 9, 12 | rESWT | 6 | 1.5 bar | 1000 | 3 (3 weeks) | 1 mL lidocaine + 1 mL betamethasone (40 mg) |
| Ahmed, L., et al. [25] | 2021 | Egypt | 22 (20) | 23 (20) | 51 ± 6 | 49 ± 8 | 16/4 | 15/5 | NA | NA | 4, 12, 24 | rESWT | 15 | 4 bar | 5000 | 1 | 1 mL lidocaine + 1 mL triamcinolone (10 mg) |
| Öztürk Durmaz, H., et al. [35] | 2022 | Turkey | 60 (33) | 49 (28) | 51.1 ± 7.1 | 54.1 ± 9.6 | 23/10 | 20/8 | 19.2 ± 24.1 | 17.4 ± 20.3 | 1, 12 | rESWT | 5 | 4 bar | 2000 | 3 (3 weeks) | 1 mL methylprednisolone (40 mg) |
| ESWT versus US | |||||||||||||||||
| Paoloni, M., et al. [36] | 2015 | Italy | 12 (8) | 13 (8) | 59.1 ± 12.5 | 56.5 ± 9.4 | 11/1 | 12/1 | 5.3 ± 3.1 | 5.1 ± 4.3 | 4, 12 | fESWT | NA | 0.05 mJ/mm2 | 2500 | 4 (3 weeks) | 15 sessions of US |
| El-Kosery, S.M., et al. [28] | 2017 | Egypt | NA (20) | NA (20) | 54.55 ± 2.3 | 54.5 ± 2.23 | 20/0 | 20/0 | NA | NA | 4 | fESWT + night splint | NA | 4 bar | 2000 | 3 (4 weeks) | 12 sessions of US + night splint |
| ESWT versus nutraceutical | |||||||||||||||||
| Notarnicola, A., et al. [34] | 2015 | Italy | NA (34) | NA (26) | 57.1 ± 9.5 | 60.2 ± 6.6 | NA | NA | 12.05 ± 1.43 | 11.92 ± 1.83 | 4, 8, 16, 24 | fESWT | 4 | 0.03 mJ/mm2 | 1600 | 3 (3 weeks) | A diet supplementary composed mainly of ALA, GLA, and echinacea |
| No. of Studies (No. of Wrists) | WMD | 95% CI | I2 | p Value | Comparison | |
|---|---|---|---|---|---|---|
| ESWT versus Control | ||||||
| Short-term follow-up (<1 month) | ||||||
| BCTQ | ||||||
| Overall | 8 (488) | −9.97 | −11.15, −8.79 | 25% | <0.01 | ESWT > control |
| rESWT | 6 (428) | −10.26 | −11.48, −9.04 | 13% | <0.01 | rESWT > control |
| fESWT | 2 (60) | −5.84 | −10.45, −1.22 | 0% | 0.01 | fESWT > control |
| VAS | ||||||
| Overall | 7 (404) | −2.07 | −2.30, −1.85 | 36% | <0.01 | ESWT > control |
| rESWT | 5 (344) | −2.12 | −2.35, −1.89 | 34% | <0.01 | rESWT > control |
| fESWT | 2 (60) | −1.41 | −2.29, −0.52 | 0% | <0.01 | fESWT > control |
| SNCV | ||||||
| Overall | 4 (247) | 0.92 | 0.55, 1.29 | 0% | <0.01 | rESWT > control |
| rESWT | 4 (247) | 0.92 | 0.55, 1.29 | 0% | <0.01 | |
| CSA | ||||||
| Overall | 3 (164) | −0.55 | −0.64, −0.47 | 33% | <0.01 | rESWT > control |
| rESWT | 3 (164) | −0.55 | −0.64, −0.47 | 33% | <0.01 | |
| Medium-term follow-up (1–6 month) | ||||||
| BCTQ | ||||||
| Overall | 7 (464) | −9.38 | −10.91, −7.84 | 45% | <0.01 | ESWT > control |
| rESWT | 5 (389) | −9.16 | −10.81, −7.50 | 20% | <0.01 | rESWT > control |
| fESWT | 2 (75) | −6.75 | −20.28, 6.78 | 83% | 0.33 | fESWT = control |
| VAS | ||||||
| Overall | 6 (379) | −1.26 | −1.56, −0.97 | 31% | <0.01 | ESWT > control |
| rESWT | 4 (304) | −1.30 | −1.78, −0.81 | 53% | <0.01 | rESWT > control |
| fESWT | 2 (75) | −0.93 | −1.69, −0.16 | 0% | 0.02 | fESWT > control |
| SNCV | ||||||
| Overall | 5 (267) | 1.08 | 0.69, 1.47 | 46% | <0.01 | ESWT > control |
| rESWT | 4 (247) | 1.12 | 0.48, 1.75 | 58% | <0.01 | rESWT > control |
| fESWT | 1 (20) | 1.60 | −0.11, 3.31 | NA | 0.07 | fESWT = control |
| MDL | ||||||
| Overall | 4 (179) | −0.29 | −0.34, −0.24 | 20% | <0.01 | ESWT > control |
| rESWT | 2 (104) | −0.23 | −0.42, −0.04 | 67% | 0.02 | rESWT > control |
| fESWT | 2 (75) | −0.26 | −0.47, −0.04 | 0% | 0.02 | fESWT > control |
| CSA | ||||||
| Overall | 3 (164) | −0.85 | −0.95, −0.76 | 31% | <0.01 | rESWT > control |
| rESWT | 3 (164) | −0.85 | −0.95, −0.76 | 31% | <0.01 | |
| Long-term follow-up (>6 month) | ||||||
| BCTQ | ||||||
| Overall | 2 (119) | −15.47 | −18.09, −12.85 | 21% | <0.01 | ESWT > control |
| rESWT | 1 (64) | −14.30 | −17.62, −10.98 | NA | <0.01 | rESWT > control |
| fESWT | 1 (55) | −17.40 | −21.67, −13.13 | NA | <0.01 | fESWT > control |
| ESWT versus LCI | ||||||
| Short-term follow-up (<1 month) | ||||||
| BCTQ | ||||||
| Overall | 5 (219) | 0.82 | −0.36, 2.01 | 0% | 0.17 | ESWT = LCI |
| rESWT | 3 (129) | 2.21 | −0.14, 4.56 | 0% | 0.07 | rESWT = LCI |
| fESWT | 2 (90) | 0.35 | −1.02, 1.72 | 0% | 0.61 | fESWT = LCI |
| VAS | ||||||
| Overall | 5 (219) | −0.02 | −0.32, 0.29 | 0% | 0.91 | ESWT = LCI |
| rESWT | 3 (129) | 0.08 | −0.28, 0.45 | 0% | 0.66 | rESWT = LCI |
| fESWT | 2 (90) | 0.35 | −1.02, 1.72 | 0% | 0.37 | fESWT = LCI |
| SNAP | ||||||
| Overall | 2 (92) | −0.13 | −0.90, 0.65 | 0% | 0.75 | ESWT = LCI |
| rESWT | 1 (55) | −0.10 | −1.13, 0.93 | NA | 0.85 | rESWT = LCI |
| fESWT | 1 (37) | −4.80 | −13.93, 4.33 | NA | 0.30 | fESWT = LCI |
| CMAP | ||||||
| Overall | 3 (145) | 0.01 | −0.16, 0.18 | 0% | 0.92 | ESWT = LCI |
| rESWT | 1 (55) | 0.00 | −0.17, 0.17 | NA | 1.00 | rESWT = LCI |
| fESWT | 2 (90) | 0.47 | −0.82, 1.75 | 0% | 0.48 | fESWT = LCI |
| MDL | ||||||
| Overall | 3 (145) | 0.04 | −0.11, 0.20 | 0% | 0.41 | ESWT = LCI |
| rESWT | 1 (55) | 0.00 | −0.17, 0.17 | NA | 1.00 | rESWT = LCI |
| fESWT | 2 (90) | 0.25 | −0.12, 0.62 | 0% | 0.19 | fESWT = LCI |
| Medium-term follow-up (1–6 month) | ||||||
| BCTQ | ||||||
| Overall | 5 (275) | −3.94 | −5.90, −1.98 | 47% | <0.01 | ESWT > LCI |
| rESWT | 4 (238) | −3.11 | −6.85, −0.63 | 60% | <0.01 | rESWT > LCI |
| fESWT | 1 (37) | −3.90 | −9.26, 1.46 | NA | 0.15 | fESWT = LCI |
| VAS | ||||||
| Overall | 5 (275) | −0.79 | −1.12, −0.47 | 67% | <0.01 | ESWT > LCI |
| rESWT | 4 (211) | −0.78 | −1.13, −0.43 | 75% | <0.01 | rESWT > LCI |
| fESWT | 1 (37) | −0.90 | −1.87, 0.07 | NA | 0.07 | fESWT = LCI |
| SNAP | ||||||
| Overall | 5 (275) | −0.23 | −1.14, 0.69 | 0% | 0.63 | ESWT = LCI |
| rESWT | 4 (238) | −0.19 | −1.11, 0.73 | 11% | 0.68 | rESWT = LCI |
| fESWT | 1 (37) | −3.60 | −12.77, 5.57 | NA | 0.44 | fESWT = LCI |
| CMAP | ||||||
| Overall | 5 (275) | −0.03 | −0.20, 0.13 | 0% | 0.69 | ESWT = LCI |
| rESWT | 4 (238) | −0.03 | −0.20, 0.13 | 0% | 0.68 | rESWT = LCI |
| fESWT | 1 (37) | 0.10 | −1.99, 2.19 | NA | 0.93 | fESWT = LCI |
| SDL | ||||||
| Overall | 4 (166) | −0.30 | −0.35, −0.24 | 46% | <0.01 | ESWT > LCI |
| rESWT | 3 (129) | −0.30 | −0.35, −0.25 | 0% | <0.01 | rESWT > LCI |
| fESWT | 1 (37) | 0.50 | −0.16, 1.16 | NA | 0.14 | fESWT = LCI |
| MDL | ||||||
| Overall | 5 (275) | 0.09 | 0.03, 0.21 | 0% | 0.14 | ESWT = LCI |
| rESWT | 4 (238 | 0.09 | −0.03, 0.21 | 0% | 0.16 | rESWT = LCI |
| fESWT | 1 (37) | 0.30 | −0.57, 1.17 | NA | 0.50 | fESWT = LCI |
| Long-term follow-up (>6 month) | ||||||
| BCTQ | ||||||
| Overall | 2 (74) | −9.45 | −14.11, −4.78 | 0% | <0.01 | rESWT > LCI |
| rESWT | 2 (74) | −9.45 | −14.11, −4.78 | 0% | <0.01 | |
| VAS | ||||||
| Overall | 2 (74) | −1.65 | −2.17, −1.12 | 0% | <0.01 | rESWT > LCI |
| rESWT | 2 (74) | −1.65 | −2.17, −1.12 | 0% | <0.01 | |
| ESWT for Mild to Moderate CTS | ||||
| Patient or population: Patients with mild-to-moderate CTS Intervention: ESWT Comparison: Other conservative interventions | ||||
| Outcomes | Weighted mean difference (95% CI) | No of Wrists (studies) | Quality of the evidence (GRADE) | Comments |
| ESWT versus Control | ||||
| ΔVAS score 1 month | The mean ΔVAS score 1 month in the intervention groups was 2.07 lower (2.30 lower to 1.85 lower) | 404 (7 studies) | ⊕⊕⊝⊝ low | |
| ΔVAS score 3 month | The mean ΔVAS score 3 month in the intervention groups was 1.26 lower (1.56 lower to 0.97 lower) | 379 (6 studies) | ⊕⊕⊝⊝ low | |
| ΔBCTQ score 1 month | The mean ΔBCTQ score 1 month in the intervention groups was 9.29 lower (11.57 lower to 7.02 lower) | 488 (8 studies) | ⊕⊕⊝⊝ low | |
| ΔBCTQ score 3 month | The mean ΔBCTQ score 3 month in the intervention groups was 9.47 lower (7.91 lower to 11.02 lower) | 464 (7 studies) | ⊕⊕⊝⊝ low | |
| ΔBCTQ score 6 month | The mean ΔBCTQ score 6 month in the intervention groups was 15.55 lower (18.53 lower to 12.57 lower) | 119 (2 studies) | ⊕⊝⊝⊝ very low | |
| ΔSNCV 1 month | The mean ΔSNCV 1 month in the intervention groups was 0.92 higher (0.55 higher to 1.29 higher) | 247 (4 studies) | ⊕⊕⊝⊝ low | |
| ΔSNCV 3 month | The mean ΔSNCV 3 month in the intervention groups was 1.15 higher (0.59 higher to 1.72 higher) | 267 (5 studies) | ⊕⊕⊝⊝ low | |
| ΔMDL 3 month | The mean ΔMDL 3 month in the intervention groups was 0.26 lower (0.35 lower to 0.17 lower) | 179 (4 studies) | ⊕⊕⊝⊝ low | |
| ΔCSA 1 month | The mean ΔCSA 1 month in the intervention groups was 0.55 lower (0.64 lower to 0.47 lower) | 164 (3 studies) | ⊕⊝⊝⊝ very low | |
| ΔCSA 3 month | The mean ΔCSA 3 month in the intervention groups was 0.85 lower (0.95 lower to 0.76 lower) | 164 (3 studies) | ⊕⊝⊝⊝ very low | |
| ESWT versus LCI | ||||
| ΔVAS score 1 month | The mean ΔVAS score 1 month in the intervention groups was 0.02 lower (0.32 lower to 0.29 higher) | 219 (5 studies) | ⊕⊕⊝⊝ low | |
| ΔVAS score 3 month | The mean ΔVAS score 3 month in the intervention groups was 0.79 lower (1.12 lower to 0.47 lower) | 275 (5 studies) | ⊕⊕⊝⊝ low | |
| ΔVAS score 6 month | The mean ΔVAS score 6 month in the intervention groups was 1.65 lower (2.17 lower to 1.12 lower) | 74 (2 studies) | ⊕⊝⊝⊝ very low | |
| ΔBCTQ score 1 month | The mean ΔBCTQ score 1 month in the intervention groups was 0.82 higher (0.36 lower to 2.01 higher) | 219 (5 studies) | ⊕⊕⊝⊝ low | |
| ΔBCTQ score 3 month | The mean ΔBCTQ score 3 month in the intervention groups was 3.35 lower (6.28 lower to 0.41 lower) | 275 (5 studies) | ⊕⊕⊝⊝ low | |
| ΔBCTQ score 6 month | The mean ΔBCTQ score 6 month in the intervention groups was 9.45 lower (14.11 lower to 4.78 lower) | 74 (2 studies) | ⊕⊝⊝⊝ very low | |
| ΔSNAP amplitude 1 month | The mean ΔSNAP amplitude 1 month in the intervention groups was 0.16 lower (1.19 lower to 0.87 higher) | 92 (2 studies) | ⊕⊝⊝⊝ very low | |
| ΔSNAP amplitude 3 month | The mean ΔSNAP amplitude 3 month in the intervention groups was 0.23 lower (1.14 lower to 0.69 higher) | 275 (5 studies) | ⊕⊕⊝⊝ low | |
| ΔCMAP amplitude 1 month | The mean ΔCMAP amplitude 1 month in the intervention groups was 0.01 higher (0.16 lower to 0.18 higher) | 145 (3 studies) | ⊕⊝⊝⊝ very low | |
| ΔCMAP amplitude 3 month | The mean ΔCMAP amplitude 3 month in the intervention groups was 0.03 lower (0.20 lower to 0.13 higher) | 275 (5 studies) | ⊕⊕⊝⊝ low | |
| ΔSDL 3 month | The mean ΔSDL 3 month in the intervention groups was 0.30 lower (0.35 lower to 0.24 lower) | 166 (4 studies) | ⊕⊕⊝⊝ low | |
| ΔMDL 1 month | The mean ΔMDL 1 month in the intervention groups was 0.04 higher (0.11 lower to 0.20 higher) | 145 (3 studies) | ⊕⊝⊝⊝ very low | |
| ΔMDL 3 month | The mean ΔMDL 3 month in the intervention groups was 0.09 higher (0.03 lower to 0.21 higher) | 275 (5 studies) | ⊕⊕⊝⊝ low | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Yang, T.; Pang, L.; Li, Y.; Li, T.; Zhang, C.; Yao, L.; Li, R.; Tang, X. Effects of Extracorporeal Shock Wave Therapy in Patients with Mild-to-Moderate Carpal Tunnel Syndrome: An Updated Systematic Review with Meta-Analysis. J. Clin. Med. 2023, 12, 7363. https://doi.org/10.3390/jcm12237363
Zhang L, Yang T, Pang L, Li Y, Li T, Zhang C, Yao L, Li R, Tang X. Effects of Extracorporeal Shock Wave Therapy in Patients with Mild-to-Moderate Carpal Tunnel Syndrome: An Updated Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2023; 12(23):7363. https://doi.org/10.3390/jcm12237363
Chicago/Turabian StyleZhang, Lei, Ting Yang, Long Pang, Yinghao Li, Tao Li, Chunsen Zhang, Lei Yao, Ran Li, and Xin Tang. 2023. "Effects of Extracorporeal Shock Wave Therapy in Patients with Mild-to-Moderate Carpal Tunnel Syndrome: An Updated Systematic Review with Meta-Analysis" Journal of Clinical Medicine 12, no. 23: 7363. https://doi.org/10.3390/jcm12237363