
The Diagnostic Value of FibroTest and Hepascore as Non-Invasive Markers of Liver Fibrosis in Primary Sclerosing Cholangitis (PSC)
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Materials
2.3. Methods
2.3.1. Non-Invasive Laboratory Tests for Liver Fibrosis
2.3.2. Biochemical Measurements
2.3.3. Autoantibody Assays
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beuers, U.; Boberg, K.M.; Chapman, R.W.; Chazouilleres, O.; Invernizzi, P.; Jones, D.E.J.; Lammert, F.; Pares, A.; Trauner, M. EASL Clinical Practice Guidelines: Management of cholestatic liver diseases. J. Hepatol. 2009, 51, 237–267. [Google Scholar]
- Chapman, R.; Fevery, J.; Kalloo, A.; Nagorney, D.M.; Boberg, K.M.; Schneider, B.; Gores, G.J. Diagnosis and management of primary sclerosing cholangitis. Hepatology 2010, 51, 660–678. [Google Scholar] [CrossRef]
- Boonstra, K.; Beuers, U.; Ponsioen, C.Y. Epidemiology of primary sclerosing cholangitis and primary biliary cirrhosis: A systematic review. J. Hepatol. 2012, 56, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Appanna, G.; Kallis, Y. An update on the management of cholestatic liver diseases. Clin. Med. 2020, 20, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.; Stanca, C.; Clark, V.; Dixon, L.; Levy, C.; Odin, J.A.; Fiel, M.I.; Friedman, S.L.; Bach, N. Natural history of small duct primary sclerosing cholangitis: A case series with review of the literature. Hepatol. Int. 2011, 5, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Luth, S.; Kanzler, S.; Frenzel, C.; Kasper, H.U.; Dienes, H.P.; Schramm, C.; Galle, P.R.; Herkel, J.; Lohse, A.W. Characteristics and long-term prognosis of the autoimmune hepatitis/primary sclerosing cholangitis overlap syndrome. J. Clin. Gastroenterol. 2009, 43, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Corpechot, C.; Gaouar, F.; El Naggar, A.; Kemgang, A.; Wendum, D.; Poupon, R.; Carrat, F.; Chazouilleres, O. Baseline values and changes in liver stiffness measured by transient elastography are associated with severity of fibrosis and outcomes of patients with primary sclerosing cholangitis. Gastroenterology 2014, 146, 970–979. [Google Scholar] [CrossRef] [PubMed]
- Mjelle, A.B.; Fossdal, G.; Gilja, O.H.; Vesterhus, M. Liver elastography in primary sclerosing cholangitis patients using three different scanner systems. Ultrasound Med. Biol. 2020, 46, 1854–1864. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, T.H.; Folseraas, T.; Thorburn, D.; Vesterhus, M. Primary sclerosing cholangitis—A comprehensive review. J. Hepatol. 2017, 67, 1298–1323. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, G.; Bungău, S.; Ceobanu, G.; Ilie, M.; Bacalbaşa, N.; Bratu, O.G.; Vesa, C.M.; Găman, M.A.; Diaconu, C.C. The non-invasive assessment of hepatic fibrosis. J. Formos. Med. Assoc. 2021, 120, 794–803. [Google Scholar] [CrossRef]
- Lai, M.; Afdhal, N.H. Liver fibrosis determination. Gastroenterol. Clin. N. Am. 2019, 48, 281–289. [Google Scholar] [CrossRef]
- Hirschfield, G.M.; Chazouillères, O.; Drenth, J.P.; Thorburn, D.; Harrison, S.A.; Landis, C.S.; Mayo, M.J.; Muir, A.J.; Trotter, J.F.; Leeming, D.J.; et al. Effect of NGM282, and FGF19 analogue, in primary sclerosing cholangitis: A multicentre, randomized, double-blind, placebo-controlled phase II trial. J. Hepatol. 2019, 70, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, J.; Dickson, E.; McDonald, G. Staging of chronic nonsuppurative destructive cholangitis (syndrome of primary biliary cirrhosis). Virchows Arch. 1978, 22, 103–112. [Google Scholar] [CrossRef]
- Poynard, T.; Morra, R.; Halfon, P.; Castera, L.; Ratziu, V.; Imbert-Bismut, F.; Naveau, S.; Thabut, D.; Lebrec, D.; Zoulim, F.; et al. Meta-analyses of FibroTest diagnostic value in chronic liver disease. BMC Gastroenterol 2007, 7, 40. [Google Scholar] [CrossRef]
- Naveau, S.; Gaude, G.; Asnacios, A.; Agostini, H.; Abella, A.; Barri-Ova, N.; Dauvois, B.; Prevot, S.; Ngo, Y.; Munteanu, M.; et al. Diagnostic and prognostic values of noninvasive biomarkers of fibrosis in patients with alcoholic liver disease. Hepatology 2009, 49, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Gudowska, M.; Wojtowicz, E.; Cylwik, B.; Gruszewska, E.; Chrostek, L. The distribution of liver steatosis, fibrosis, steatohepatitis and inflammation activity in alcoholics according to FibroMax Test. Adv. Clin. Exp. Med. 2015, 24, 823–827. [Google Scholar] [CrossRef]
- Chrostek, L.; Przekop, D.; Gruszewska, E.; Gudowska-Sawczuk, M.; Cylwik, B. Noninvasive indirect markers of liver fibrosis in alcoholics. BioMed Res. Int. 2019, 2019, 3646975. [Google Scholar] [CrossRef] [PubMed]
- Przekop, D.; Klapczynski, J.; Grytczuk, A.; Gruszewska, E.; Gietka, A.; Panasiuk, A.; Golaszewski, S.; Cylwik, B.; Chrostek, L. Non-invasive indirect markers of liver fibrosis after interferon-free treatment for hepatitis C. J. Clin. Med. 2021, 10, 3951. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Angulo, P.; Lymp, J.; Li, D.; Satomura, S.; Lindor, K. Hyaluronic acid, an accurate serum marker for severe hepatic fibrosis in patients with non-alcoholic fatty liver disease. Liver Int. 2005, 25, 779–786. [Google Scholar] [CrossRef]
- Adams, L.A.; Bulsara, M.; Rossi, E.; DeBoer, B.; Speers, D.; George, J.; Kench, J.; Farrell, G.; McCaughan, G.W.; Jeffrey, G.P. Hepascore: An accurate validated predictor of liver fibrosis in chronic hepatitis C infection. Clin. Chem. 2005, 51, 1867–1873. [Google Scholar] [CrossRef]
- Poynard, T.; Imbert-Bismut, F.; Munteanu, M.; Messous, D.; Myers, R.P.; Thabut, D.; Ratziu, V.; Mercadier, A.; Benhamou, Y.; Hainque, B. Overview of the diagnostic value of biochemical markers of liver fibrosis (FibroTest, HCV FibroSure) and necrosis (ActiTest) in patients with chronic hepatitis C. Comp. Hepatol. 2004, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Poynard, T.; Halfon, P.; Castera, L.; Munteanu, M.; Imbert-Bismut, F.; Ratziu, V.; Benhamou, Y.; Bourlière, M.; de Ledinghen, V.; FibroPaca Group. Standardization of ROC curve areas for diagnostic evaluation of liver fibrosis markers based on prevalences of fibrosis stages. Clin. Chem. 2007, 9, 1615–1622. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PSC (n = 74) | Healthy Subjects (n = 38) | p-Value | |
|---|---|---|---|
| Age (years) (median/range) | 36 (26–75) | 25 (21–54) | - |
| Sex (Female/Male) | 27/47 | 27/11 | - |
| ALP (IU/L) | 190 91.0–331.0 | 59.0 53.0–70.0 | p < 0.001 * |
| GGT (IU/L) | 255.7 111.5–532.2 | 23.5 18.5–28.0 | p < 0.001 * |
| AST (IU/L) | 24.9 14.4–48.7 | 23.0 19.0–26.0 | p = 0.541 |
| ALT (IU/L) | 34.4 21.8–67.0 | 17.5 11.5–19.5 | p < 0.001 * |
| Bilirubin (µmol/L) | 7.69 6.16–15.05 | 13.42 7.27–17.1 | p = 0.222 |
| α2-macroglobulin (g/L) | 2.33 1.80–2.82 | 1.84 1.47–2.18 | p < 0.001 * |
| Haptoglobin (g/L) | 0.99 0.61–1.48 | 0.98 0.77–1.21 | p = 0.684 |
| ApoA1 (g/L) | 1.60 1.28–1.91 | 1.52 1.39–1.72 | p = 0.455 |
| FibroTest | 0.32 0.17–0.51 | 0.10 0.07–0.15 | p < 0.001 |
| Hepascore | 0.39 0.14–0.82 | 0.27 0.21–0.27 | p < 0.047 |
| Hyaluronic acid (ng/mL) | 40.8 18.5–95.0 | 35.0 25.0–40.5 | p = 0.259 |
| Anti-PR3-ANCA (+/−) (%) | 25/49 (34.3) | ND | - |
| Anti-sp100 (+/−) (%) | 2/72 (2.94) | ND | - |
| Anti-gp210 (+/−) (%) | 4/70 (4.90) | ND | - |
| Marker | F0 | F1 | F2 | F3 | F4 |
|---|---|---|---|---|---|
| FibroTest | 0.14 0.09–0.19 (n = 28) | 0.33 0.31–0.41 (n = 24) | 0.51 0.50–0.51 (n = 6) | 0.63 0.60–0.68 (n = 7) | 0.89 0.84–0.93 (n = 9) |
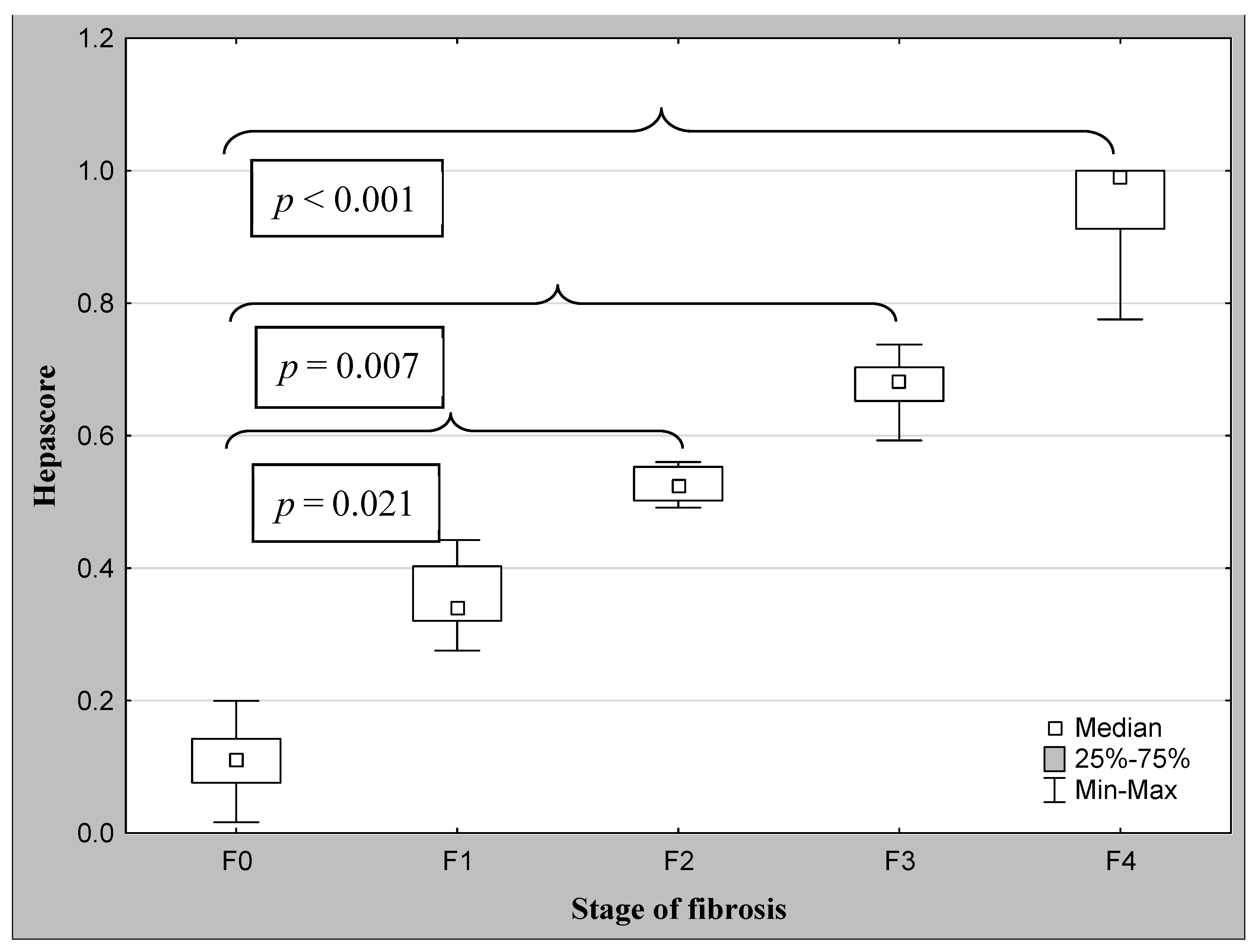
| Hepascore | 0.11 0.08–0.14 (n = 27) | 0.34 0.32–0.40 (n = 13) | 0.52 0.50–0.55 (n = 6) | 0.68 0.65–0.70 (n = 5) | 0.99 0.91–1.00 (n = 22) |
| Marker | No Significant Fibrosis (F1) | Significant Fibrosis (F ≥ 2) | Without Cirrhosis (F1–F3) | Cirrhosis (F4) |
|---|---|---|---|---|
| Hepascore | 0.14 0.10–0.30 n = 40 | 0.91 0.68–1.00 n = 33 | 0.18 0.11–0.42 n = 51 | 0.99 0.87–1.00 n = 23 |
| p < 0.001 * | p < 0.001 # | |||
| FibroTest | 0.26 0.12–0.33 n = 52 | 0.68 0.55–0.88 n = 22 | 0.30 0.15–0.44 n = 64 | 0.89 0.78–0.93 n = 10 |
| p < 0.001 * | p < 0.001 # |
| Marker | F0 | F1 | F2 | F3 | F4 |
|---|---|---|---|---|---|
| HA | 24.7 7.65–40.0 (n = 28) | 35.0 21.1–88.9 (n = 24) | 33.8 17.9–145 (n = 6) | 95.0 43.4–142 (n = 7) | 178.5 96.4–224 (n = 9) |
| α2-M | 1.77 1.54–2.36 (n = 28) | 2.54 2.03–3.01 (n = 24) | 2.43 2.01–2.95 (n = 6) | 2.47 2.22–2.80 (n = 7) | 2.70 2.33–3.22 (n = 9) |
| GGT | 165 53.4–353 (n = 14) | 257.5 111.5–557 (n = 9) | 545 545–545 (n = 1) | 298 263–557 (n = 4) | 429 242–462 (n = 4) |
| Bilirubin | 6.16 4.45–6.16 (n = 28) | 8.55 6.33–11.2 (n = 24) | 14.9 7.69–15.9 (n = 6) | 22.4 11.6–25.8 (n = 7) | 46.2 40.5–60.7 (n = 9) |
| Hp | 0.99 0.67–1.67 (n = 28) | 0.81 0.52–1.12 (n = 24) | 0.62 0.45–1.24 (n = 6) | 0.91 0.21–1.24 (n = 7) | 1.11 0.26–1.74 (n = 9) |
| ApoA1 | 1.70 1.44–2.01 (n = 28) | 1.73 1.52–1.91 (n = 24) | 1.69 1.42–1.84 (n = 6) | 1.70 1.30–2.20 (n = 7) | 0.58 0.31–1.16 (n = 9) |
| Marker | No Significant Fibrosis (F1) (n = 52) | Significant Fibrosis (F ≥ 2) (n = 22) | Without Cirrhosis (F1–F3) (n = 64) | Cirrhosis (F4) (n = 10) |
|---|---|---|---|---|
| Hyaluronic acid | 28.9 15.6–52.1 | 95.8 28.1–219 | 34.0 16.9–66.5 | 167 69.2–224 |
| p < 0.001 * | p < 0.001 # |
| Marker | Cut-Off | Sensitivity (%) | Specificity (%) | ACC (%) | PPV (%) | NPV (%) | AUC ± SE |
|---|---|---|---|---|---|---|---|
| Hepascore | |||||||
| -for fibrosis | 0.52 * | 96.8 | 100 | 98.0 | 100 | 94.7 | 1.000 ± 0.00 |
| -for cirrhosis | 0.80 # | 95.2 | 100 | 98.0 | 100 | 96.6 | 1.000 ± 0.00 |
| FibroTest | |||||||
| -for fibrosis | 0.51 * | 58.6 | 90.0 | 71.4 | 89.5 | 60.0 | 0.769 ± 0.07 |
| -for cirrhosis | 0.73 # | 42.9 | 100 | 61.3 | 100 | 45.5 | 0.767 ± 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cylwik, B.; Bauer, A.; Gruszewska, E.; Gan, K.; Kazberuk, M.; Chrostek, L. The Diagnostic Value of FibroTest and Hepascore as Non-Invasive Markers of Liver Fibrosis in Primary Sclerosing Cholangitis (PSC). J. Clin. Med. 2023, 12, 7552. https://doi.org/10.3390/jcm12247552
Cylwik B, Bauer A, Gruszewska E, Gan K, Kazberuk M, Chrostek L. The Diagnostic Value of FibroTest and Hepascore as Non-Invasive Markers of Liver Fibrosis in Primary Sclerosing Cholangitis (PSC). Journal of Clinical Medicine. 2023; 12(24):7552. https://doi.org/10.3390/jcm12247552
Chicago/Turabian StyleCylwik, Bogdan, Alicja Bauer, Ewa Gruszewska, Kacper Gan, Marcin Kazberuk, and Lech Chrostek. 2023. "The Diagnostic Value of FibroTest and Hepascore as Non-Invasive Markers of Liver Fibrosis in Primary Sclerosing Cholangitis (PSC)" Journal of Clinical Medicine 12, no. 24: 7552. https://doi.org/10.3390/jcm12247552
APA StyleCylwik, B., Bauer, A., Gruszewska, E., Gan, K., Kazberuk, M., & Chrostek, L. (2023). The Diagnostic Value of FibroTest and Hepascore as Non-Invasive Markers of Liver Fibrosis in Primary Sclerosing Cholangitis (PSC). Journal of Clinical Medicine, 12(24), 7552. https://doi.org/10.3390/jcm12247552