
Artificial Intelligence-Assisted Detection of Osteoporotic Vertebral Fractures on Lateral Chest Radiographs in Post-Menopausal Women

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
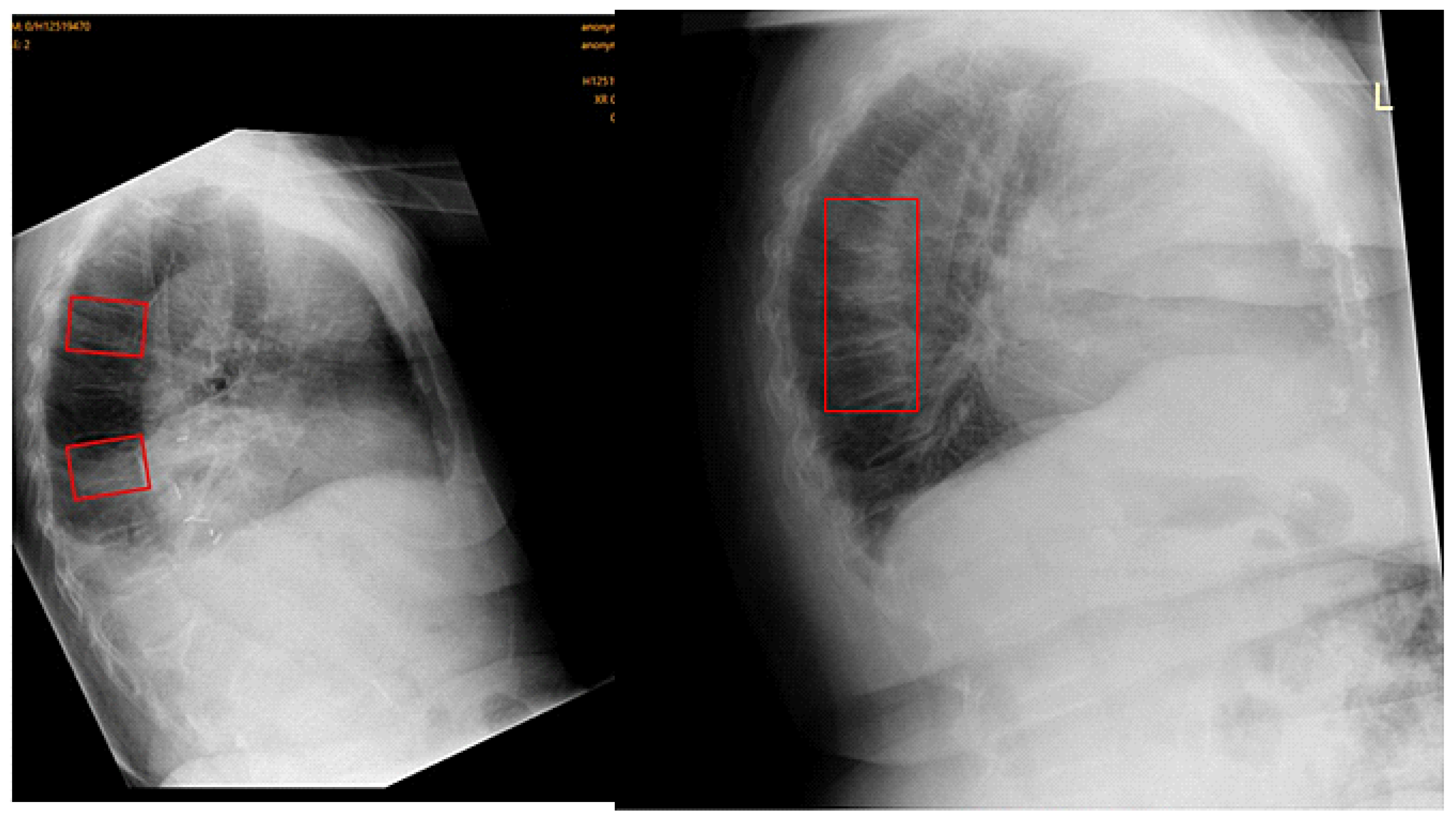
2.2. Image Analysis Using Ofeye 1.0 for Automatic Detection of OVFs
2.3. Image Assessment by Human Observers
- A reduction of at least 20% in the anterior or middle vertebral height compared with the posterior height.
- A reduction of at least 20% in any of the anterior, middle, or posterior vertebral heights, relative to the vertebra immediately above or below it.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, S.; Zhu, X.; Xiao, D.; Zhuang, J.; Liang, G.; Liang, C.; Zheng, X.; Ke, Y.; Chang, Y. Therapeutic effect of percutaneous kyphoplasty combined with anti-osteoporosis drug on postmenopausal women with osteoporotic vertebral compression fracture and analysis of postoperative bone cement leakage risk factors: A retrospective cohort study. J. Orthop. Surg. Res. 2019, 14, 452. [Google Scholar] [CrossRef] [PubMed]
- Wáng, Y.X.J.; Deng, M.; He, L.C.; Che-Nordin, N.; Santiago, F.R. Osteoporotic vertebral endplate and cortex fractures: A pictorial review. J. Orthop. Translat. 2018, 15, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Griffith, J.F. Identifying osteoporotic vertebral fracture. Quant. Imaging Med. Surg. 2015, 5, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Wáng, Y.X.J. An update of our understanding of radiographic diagnostics for prevalent osteoporotic vertebral fracture in elderly women. Quant. Imaging Med. Surg. 2022, 12, 3495–3514. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.; Rong, Y.; Wang, J.; Yu, S.; Yin, G.; Fan, J.; Tang, P.; Jiang, D.; Liu, W.; Gong, F.; et al. Risk factors for refracture following primary osteoporotic vertebral compression fractures. Pain. Physician 2021, 24, E335–E340. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Liu, J.; Ebraheim, N.A. Managements of osteoporotic vertebral compression fractures: A narrative review. World. J. Orthop. 2022, 13, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Lenchik, L.; Rogers, L.F.; Delmas, P.D.; Genant, H.K. Diagnosis of Osteoporotic Vertebral Fractures: Importance of Recognition and Description by Radiologists. AJR Am. J. Roentgenol. 2004, 183, 949–958. [Google Scholar] [CrossRef]
- Howe, T.E.; Shea, B.; Dawson, L.J.; Downie, F.; Murray, A.; Ross, C.; Harbour, R.T.; Caldwell, L.M.; Creed, G. Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane. Database. Syst. Rev. 2011, 7, CD000333. [Google Scholar] [CrossRef]
- Wáng, Y.X.J.; Lu, Z.H.; Leung, J.C.; Fang, Z.Y.; Kwok, T.C. Osteoporotic-like vertebral fracture with less than 20% height loss is associated with increased further vertebral fracture risk in older women: The MrOS and MsOS (Hong Kong) year-18 follow-up radiograph results. Quant. Imaging Med. Surg. 2023, 13, 1115–1125. [Google Scholar] [CrossRef]
- Xiao, B.H.; Zhu, M.S.; Du, E.Z.; Liu, W.H.; Ma, J.B.; Huang, H.; Gong, J.S.; Diacinti, D.; Zhang, K.; Gao, B.; et al. A software program for automated compressive vertebral fracture detection on elderly women’s lateral chest radiograph: Ofeye 1.0. Quant. Imaging Med. Surg. 2022, 12, 4259–4271. [Google Scholar] [CrossRef]
- Gündel, S.; Grbic, S.; Georgescu, B.; Liu, S.; Maier, A.; Comaniciu, D. Learning to recognize abnormalities in chest X-Rays with location-aware dense networks. In Progress in Pattern Recognition, Image Analysis, Computer Vision, and Applications; Vera-Rodriguez, R., Fierrez, J., Morales, A., Eds.; Springer: Cham, Switzerland, 2019; Volume 11401, pp. 757–765. [Google Scholar] [CrossRef]
- Du, M.M.; Che-Nordin, N.; Ye, P.P.; Qiu, S.W.; Yan, Z.H.; Wang, Y.X.J. Underreporting characteristics of osteoporotic vertebral fracture in back pain clinic patients of a tertiary hospital in China. J. Orthop. Translat. 2020, 23, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.S.; Judge, C.; Bollard, S.M.; Clifford, S.M.; Healy, G.M.; Aziz, A.; Mathur, P.; Islam, S.; Yeom, K.W.; Lawlor, A.; et al. Radiology artificial intelligence: A systematic review and evaluation of methods (RAISE). Eur. Radiol. 2022, 32, 7998–8007. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Thakur, G.S.M. Advanced applications of neural networks and artificial intelligence: A review. I.J. Inform. Technol. Comput. Sci. 2012, 4, 57. [Google Scholar] [CrossRef]
- Nazar, M.; Alam, M.M.; Yafi, E.; Su’ud, M.M. A Systematic Review of Human–Computer Interaction and Explainable Artificial Intelligence in Healthcare with Artificial Intelligence Techniques. IEEE Access 2021, 9, 153316–153348. [Google Scholar] [CrossRef]
- Xu, F.; Xiong, Y.; Ye, G.; Liang, Y.; Guo, W.; Deng, Q.; Wu, L.; Jia, W.; Wu, D.; Chen, S.; et al. Deep learning-based artificial intelligence model for classification of vertebral compression fractures: A multicenter diagnostic study. Front. Endocrinol. 2023, 14, 1025749. [Google Scholar] [CrossRef]
- Chen, W.; Liu, X.; Li, K.; Luo, Y.; Bai, S.; Wu, J.; Chen, W.; Dong, M.; Guo, D. A deep-learning model for identifying fresh vertebral compression fractures on digital radiography. Eur. Radiol. 2022, 32, 1496–1505. [Google Scholar] [CrossRef]
- Hong, N.; Cho, S.W.; Shin, S.; Lee, S.; Jang, S.A.; Roh, S.; Lee, Y.H.; Rhee, Y.; Cummings, S.R.; Kim, H.; et al. Deep-Learning-Based Detection of Vertebral Fracture and Osteoporosis Using Lateral Spine X-Ray Radiography. J. Bone. Miner Res. 2023, 38, 887–895. [Google Scholar] [CrossRef]
- Du, E.Z.; Wáng, Y.X.J. CT detects more osteoporotic endplate depressions than radiograph: A descriptive comparison of 76 vertebrae. Osteoporosis. Int. 2022, 33, 1569–1577. [Google Scholar] [CrossRef]
- Li, Y.C.; Chen, H.H.; Horng-Shing Lu, H.; Hondar Wu, H.T.; Chang, M.C.; Chou, P.H. Can a Deep-learning Model for the Automated Detection of Vertebral Fractures Approach the Performance Level of Human Subspecialists? Clin. Orthop. Relat. Res. 2021, 479, 1598–1612. [Google Scholar] [CrossRef]
- Wáng, Y.X.J. The definition of spine bone mineral density (BMD)-classified osteoporosis and the much inflated prevalence of spine osteoporosis in older Chinese women when using the conventional cutpoint T-score of-2.5. Ann. Transl. Med. 2022, 10, 1421. [Google Scholar] [CrossRef]
- Matsumoto, M.; Okada, E.; Kaneko, Y.; Ichihara, D.; Watanabe, K.; Chiba, K.; Toyama, Y.; Fujiwara, H.; Momoshima, S.; Nishiwaki, Y.; et al. Wedging of vertebral bodies at the thoracolumbar junction in asymptomatic healthy subjects on magnetic resonance imaging. Surg. Radiol. Anat. 2011, 33, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Crawford, M.B.; Toms, A.P.; Shepstone, L. Defining Normal Vertebral Angulation at the Thoracolumbar Junction. AJR Am. J. Roentgenol. 2009, 193, W33–W37. [Google Scholar] [CrossRef]
- Ranschaert, E. Artificial Intelligence in Radiology: Hype or Hope? J. Belg. Sco. Radiol. 2018, 102, 20. [Google Scholar] [CrossRef]
- Kim, D.H.; Jeong, J.G.; Kim, Y.J.; Kim, K.G.; Jeon, J.Y. Automated Vertebral Segmentation and Measurement of Vertebral Compression Ratio Based on Deep Learning in X-ray Images. J. Digit. Imaging 2021, 34, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.D.; Sebro, R. Computer-Aided Detection of Incidental Lumbar Spine Fractures from Routine Dual-Energy X-ray Absorptiometry (DEXA) Studies Using a Support Vector Machine (SVM) Classifier. J. Digit. Imaging 2020, 33, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.E.; Yao, J.; Summers, R.M. Vertebral body compression fractures and bone density: Automated detection and and classification in CT. Radiology 2017, 284, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.C.; Cho, H.C.; Jang, T.J.; Choi, J.M.; Seo, J.K. Automatic detection and segmentation of lumbar vertebrae from X-ray images for compression fracture evaluation. Comput. Methods. Programs. Biomed. 2021, 200, 105833. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Hsu, B.W.Y.; Yin, Y.K.; Lin, F.H.; Yang, T.H.; Yang, R.S.; Lee, C.K.; Tseng, V.S. Application of deep learning algorithm to detect and visualize vertebral fractures on plain frontal radiographs. PLoS ONE 2021, 16, e0245992. [Google Scholar] [CrossRef]
- Shen, L.; Gao, C.; Hu, S.; Kang, D.; Zhang, Z.; Xia, D.; Xu, Y.; Xiang, S.; Zhu, Q.; Xu, G.; et al. Using Artificial Intelligence to Diagnose Osteoporotic Vertebral Fractures on Plain Radiographs. J. Bone. Miner Res. 2023, 38, 1278–1287. [Google Scholar] [CrossRef]
- Lampignano, J.P.; Kendrick, L.E. Bontrager’s Textbook of Radiographic Positioning and Related Anatomy, 10th ed.; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Delrue, L.; Gosselin, R.; Ilsen, B.; Van Landeghem, A.; de Mey, J.; Duyck, P. Difficulties in the Interpretation of Chest Radiography; Springer: Berlin/Heidelberg, Germany, 2011; pp. 27–49. [Google Scholar] [CrossRef]
- Shin, H.J.; Han, K.; Ryu, L.; Kim, E.K. The impact of artificial intelligence on the reading times of radiologists for chest radiographs. NPJ Digit. Med. 2023, 6, 82. [Google Scholar] [CrossRef]
- Lentle, B.; Koromani, F.; Brown, J.P.; Oei, L.; Ward, L.; Goltzman, D.; Rivadeneira, F.; Leslie, W.D.; Probyn, L.; Prior, J.; et al. The Radiology of osteoporotic vertebral fractures revisited. J. Bone. Miner Res. 2019, 34, 409–418. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Total No. of Cases | Original Radiologist Reports/AI Analysis | Original Radiologist Reports/AI Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| TP | FP | TN | FN | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | Accuracy (95% CI) | ||
| A | 106 | 7/11 | 2/4 | 72/69 | 25/22 | 21.9 (9.3, 40)/ 33.3 (18, 51.8) | 97.3 (90.6, 99.7)/ 94.5 (86.6, 98.5) | 77.8 (43.5, 94.1)/ 73.3(48.6, 88.9) | 74.2 (70.5, 77.6)/ 75.8 (71, 80.1) | 74.5 (65.1, 82.5)/ 75.5 (66.1, 83.3) |
| B | 269 | 17/51 | 11/14 | 172/167 | 69/37 | 19.8 (12, 29.8)/ 58 (47, 68.4) | 94 (89.5,97)/ 92.3 (87.4, 95.7) | 60.7 (43.1, 75.9)/ 78.5(68.1, 86.1) | 71.4 (69, 73.6)/ 81.9 (77.9, 85.3) | 70.3 (64.4, 75.7)/ 81.0 (75.8, 85.5) |
| C | 135 | 6/11 | 4/8 | 105/99 | 20/17 | 23 (9, 43.6)/ 39.3 (21.5, 59.4) | 96.3 (90.9, 99)/ 92.5 (85.8, 96.7) | 60 (31.3, 83.1)/ 57.9 (38, 75.6) | 84 (80.9, 86.7)/ 85.3 (81.4, 88.7) | 82.2 (74.7, 88.3)/ 81.5 (73.9, 87.6) |
| All sites | 510 | 30/73 | 17/26 | 349/335 | 114/76 | 20.8 (14.5, 28.4)/ 49 (40.7, 57.3) | 95.4 (92.7,97.3)/ 92.8 (89.6, 95.2) | 63.8 (50.1, 75.6)/ 73.7 (65.2, 80.8) | 75.4 (73.7, 77)/ 81.5 (79, 83.8) | 74.3 (70.3, 78.1)/ 80.3 (76.3, 83.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silberstein, J.; Wee, C.; Gupta, A.; Seymour, H.; Ghotra, S.S.; Sá dos Reis, C.; Zhang, G.; Sun, Z. Artificial Intelligence-Assisted Detection of Osteoporotic Vertebral Fractures on Lateral Chest Radiographs in Post-Menopausal Women. J. Clin. Med. 2023, 12, 7730. https://doi.org/10.3390/jcm12247730
Silberstein J, Wee C, Gupta A, Seymour H, Ghotra SS, Sá dos Reis C, Zhang G, Sun Z. Artificial Intelligence-Assisted Detection of Osteoporotic Vertebral Fractures on Lateral Chest Radiographs in Post-Menopausal Women. Journal of Clinical Medicine. 2023; 12(24):7730. https://doi.org/10.3390/jcm12247730
Chicago/Turabian StyleSilberstein, Jenna, Cleo Wee, Ashu Gupta, Hannah Seymour, Switinder Singh Ghotra, Cláudia Sá dos Reis, Guicheng Zhang, and Zhonghua Sun. 2023. "Artificial Intelligence-Assisted Detection of Osteoporotic Vertebral Fractures on Lateral Chest Radiographs in Post-Menopausal Women" Journal of Clinical Medicine 12, no. 24: 7730. https://doi.org/10.3390/jcm12247730
APA StyleSilberstein, J., Wee, C., Gupta, A., Seymour, H., Ghotra, S. S., Sá dos Reis, C., Zhang, G., & Sun, Z. (2023). Artificial Intelligence-Assisted Detection of Osteoporotic Vertebral Fractures on Lateral Chest Radiographs in Post-Menopausal Women. Journal of Clinical Medicine, 12(24), 7730. https://doi.org/10.3390/jcm12247730