
Intraoperative Low-Dose S-Ketamine Reduces Depressive Symptoms in Patients with Crohn’s Disease Undergoing Bowel Resection: A Randomized Controlled Trial

Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Randomization and Masking
2.3. Procedures
2.4. Outcome Measures
2.5. Measurement of Biomarkers
2.6. Statistical Analysis
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sairenji, T.; Collins, K.L.; Evans, D.V. An Update on Inflammatory Bowel Disease. Prim. Care 2017, 44, 673–692. [Google Scholar] [CrossRef] [PubMed]
- Binder, V. Epidemiology of IBD during the twentieth century: An integrated view. Best Pract. Res. Clin. Gastroenterol. 2004, 18, 463–479. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, S.; Clark, D.C.; Gibbons, R.D. Diagnosing depression in the hospitalized medically ill. Psychosomatics 1983, 24, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.M.; Varma, M.G. Surgery for inflammatory bowel disease. World J. Gastroenterol. 2008, 14, 2678–2690. [Google Scholar] [CrossRef] [PubMed]
- Keefer, L. Behavioural medicine and gastrointestinal disorders: The promise of positive psychology. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 378–386. [Google Scholar] [CrossRef]
- Klem, F.; Wadhwa, A.; Prokop, L.J.; Sundt, W.J.; Farrugia, G.; Camilleri, M.; Singh, S.; Grover, M. Prevalence, Risk Factors, and Outcomes of Irritable Bowel Syndrome After Infectious Enteritis: A Systematic Review and Meta-analysis. Gastroenterology 2017, 152, 1042–1054.e1. [Google Scholar] [CrossRef]
- Sawynok, J. Topical and peripheral ketamine as an analgesic. Anesth. Analg. 2014, 119, 170–178. [Google Scholar] [CrossRef]
- Zuo, D.; Lin, L.; Liu, Y.; Wang, C.; Xu, J.; Sun, F.; Li, L.; Li, Z.; Wu, Y. Baicalin Attenuates Ketamine-Induced Neurotoxicity in the Developing Rats: Involvement of PI3K/Akt and CREB/BDNF/Bcl-2 Pathways. Neurotox. Res. 2016, 30, 159–172. [Google Scholar] [CrossRef]
- Perry, E.B., Jr.; Cramer, J.A.; Cho, H.S.; Petrakis, I.L.; Karper, L.P.; Genovese, A.; O’Donnell, E.; Krystal, J.H.; D’Souza, D.C.; Yale Ketamine Study Group. Psychiatric safety of ketamine in psychopharmacology research. Psychopharmacology 2007, 192, 253–260. [Google Scholar] [CrossRef]
- Wang, J.; Goffer, Y.; Xu, D.; Tukey, D.S.; Shamir, D.B.; Eberle, S.E.; Zou, A.H.; Blanck, T.J.; Ziff, E.B. A single subanesthetic dose of ketamine relieves depression-like behaviors induced by neuropathic pain in rats. Anesthesiology 2011, 115, 812–821. [Google Scholar] [CrossRef]
- Casoni, D.; Spadavecchia, C.; Adami, C. S-ketamine versus racemic ketamine in dogs: Their relative potency as induction agents. Vet. Anaesth. Analg. 2015, 42, 250–259. [Google Scholar] [CrossRef]
- Kim, J.; Farchione, T.; Potter, A.; Chen, Q.; Temple, R. Esketamine for Treatment-Resistant Depression-First FDA-Approved Antidepressant in a New Class. N. Engl. J. Med. 2019, 381, 1–4. [Google Scholar] [CrossRef]
- Krystal, J.H.; Charney, D.S.; Duman, R.S. A New Rapid-Acting Antidepressant. Cell 2020, 181, 7. [Google Scholar] [CrossRef]
- Liu, P.; Li, P.; Li, Q.; Yan, H.; Shi, X.; Liu, C.; Zhang, Y.; Peng, S. Effect of Pretreatment of S-Ketamine on Postoperative Depression for Breast Cancer Patients. J. Investig. Surg. 2021, 34, 883–888. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Y.; Xu, X.; Peng, S.; Xu, F.; Liu, P. Use of Various Doses of S-Ketamine in Treatment of Depression and Pain in Cervical Carcinoma Patients with Mild/Moderate Depression After Laparoscopic Total Hysterectomy. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e922028. [Google Scholar] [CrossRef]
- Garcia, L.S.; Comim, C.M.; Valvassori, S.S.; Réus, G.Z.; Barbosa, L.M.; Andreazza, A.C.; Stertz, L.; Fries, G.R.; Gavioli, E.C.; Kapczinski, F.; et al. Acute administration of ketamine induces antidepressant-like effects in the forced swimming test and increases BDNF levels in the rat hippocampus. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2008, 32, 140–144. [Google Scholar] [CrossRef]
- Martin-Subero, M.; Anderson, G.; Kanchanatawan, B.; Berk, M.; Maes, M. Comorbidity between depression and inflammatory bowel disease explained by immune-inflammatory, oxidative, and nitrosative stress; tryptophan catabolite; and gut-brain pathways. CNS Spectr. 2016, 21, 184–198. [Google Scholar] [CrossRef]
- Abautret-Daly, Á.; Dempsey, E.; Riestra, S.; de Francisco-García, R.; Parra-Blanco, A.; Rodrigo, L.; Medina, C.; Connor, T.J.; Harkin, A. Association between psychological measures with inflammatory anddisease-related markers of inflammatory bowel disease. Int. J. Psychiatry Clin. Pract. 2017, 21, 221–230. [Google Scholar] [CrossRef]
- Hsuchou, H.; Kastin, A.J.; Mishra, P.K.; Pan, W. C-reactive protein increases BBB permeability: Implications for obesity and neuroinflammation. Cell. Physiol. Biochem. 2012, 30, 1109–1119. [Google Scholar] [CrossRef]
- Pasco, J.A.; Nicholson, G.C.; Williams, L.J.; Jacka, F.N.; Henry, M.J.; Kotowicz, M.A.; Schneider, H.G.; Leonard, B.E.; Berk, M. Association of high-sensitivity C-reactive protein with de novo major depression. Br. J. Psychiatry 2010, 197, 372–377. [Google Scholar] [CrossRef]
- Szałach, Ł.P.; Lisowska, K.A.; Słupski, J.; Włodarczyk, A.; Górska, N.; Szarmach, J.; Jakuszkowiak-Wojten, K.; Gałuszko-Węgielnik, M.; Wiglusz, M.S.; Wilkowska, A.; et al. The immunomodulatory effect of ketamine in depression. Psychiatr. Danub. 2019, 31 (Suppl. 3), 252–257. [Google Scholar]
- Kiraly, D.D.; Horn, S.R.; Van Dam, N.T.; Costi, S.; Schwartz, J.; Kim-Schulze, S.; Patel, M.; Hodes, G.E.; Russo, S.J.; Merad, M.; et al. Altered peripheral immune profiles in treatment-resistant depression: Response to ketamine and prediction of treatment outcome. Transl. Psychiatry 2017, 7, e1065. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Li, C.T.; Lin, W.C.; Hong, C.J.; Tu, P.C.; Bai, Y.M.; Cheng, C.M.; Su, T.P. Rapid inflammation modulation and antidepressant efficacy of a low-dose ketamine infusion in treatment-resistant depression: A randomized, double-blind control study. Psychiatry Res. 2018, 269, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Weng, H.; Zhou, H.; Yang, Z.; Tian, Z.; Xi, B.; Li, Y. Esketamine alleviates postoperative depression-like behavior through anti-inflammatory actions in mouse prefrontal cortex. J. Affect. Disord. 2022, 307, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Elia, N.; Tramèr, M.R. Ketamine and postoperative pain--a quantitative systematic review of randomised trials. Pain 2005, 113, 61–70. [Google Scholar] [CrossRef]
- Kohrs, R.; Durieux, M.E. Ketamine: Teaching an old drug new tricks. Anesth. Analg. 1998, 87, 1186–1193. [Google Scholar] [CrossRef]
- Schmid, R.L.; Sandler, A.N.; Katz, J. Use and efficacy of low-dose ketamine in the management of acute postoperative pain: A review of current techniques and outcomes. Pain 1999, 82, 111–125. [Google Scholar] [CrossRef]
- Nitta, R.; Goyagi, T.; Nishikawa, T. Combination of oral clonidine and intravenous low-dose ketamine reduces the consumption of postoperative patient-controlled analgesia morphine after spine surgery. Acta Anaesthesiol. Taiwanica 2013, 51, 14–17. [Google Scholar] [CrossRef]
- Kudoh, A.; Takahira, Y.; Katagai, H.; Takazawa, T. Small-dose ketamine improves the postoperative state of depressed patients. Anesth. Analg. 2002, 95, 114–118. [Google Scholar] [CrossRef]
- Targownik, L.E.; Nugent, Z.; Singh, H.; Bugden, S.; Bernstein, C.N. The prevalence and predictors of opioid use in inflammatory bowel disease: A population-based analysis. Am. J. Gastroenterol. 2014, 109, 1613–1620. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Feagan, B.G.; Cohen, R.D.; Salzberg, B.A.; Diamond, R.H.; Price, S.; Langholff, W.; Londhe, A.; Sandborn, W.J. Serious infection and mortality in patients with Crohn’s disease: More than 5 years of follow-up in the TREAT registry. Am. J. Gastroenterol. 2012, 107, 1409–1422. [Google Scholar] [CrossRef]
- Burr, N.E.; Smith, C.; West, R.; Hull, M.A.; Subramanian, V. Increasing Prescription of Opiates and Mortality in Patients With Inflammatory Bowel Diseases in England. Clin. Gastroenterol. Hepatol. 2018, 16, 534–541.e6. [Google Scholar] [CrossRef]
- Sheehan, J.L.; Jacob, J.; Berinstein, E.M.; Greene-Higgs, L.; Steiner, C.A.; Berry, S.K.; Shannon, C.; Cohen-Mekelburg, S.A.; Higgins, P.; Berinstein, J.A. The Relationship Between Opioid Use and Healthcare Utilization in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Inflamm. Bowel Dis. 2022, 28, 1904–1914. [Google Scholar] [CrossRef]
- Sanacora, G.; Frye, M.A.; McDonald, W.; Mathew, S.J.; Turner, M.S.; Schatzberg, A.F.; Summergrad, P.; Nemeroff, C.B.; American Psychiatric Association (APA) Council of Research Task Force on Novel Biomarkers and Treatments. A Consensus Statement on the Use of Ketamine in the Treatment of Mood Disorders. JAMA Psychiatry 2017, 74, 399–405. [Google Scholar] [CrossRef]
- Lepack, A.E.; Fuchikami, M.; Dwyer, J.M.; Banasr, M.; Duman, R.S. BDNF release is required for the behavioral actions of ketamine. Int. J. Neuropsychopharmacol. 2014, 18, pyu033. [Google Scholar] [CrossRef]
- Laje, G.; Lally, N.; Mathews, D.; Brutsche, N.; Chemerinski, A.; Akula, N.; Kelmendi, B.; Simen, A.; McMahon, F.J.; Sanacora, G.; et al. Brain-derived neurotrophic factor Val66Met polymorphism and antidepressant efficacy of ketamine in depressed patients. Biol. Psychiatry 2012, 72, e27–e28. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Placebo, n = 60 | S-Ketamine, n = 60 | p-Value |
|---|---|---|---|
| Age, y | 35.2 ± 10.9 | 35.7 ± 9.3 | 0.774 |
| Sex, male | 45 (70%) | 40 (66.7%) | 0.315 |
| Weight, kg | 52.6 ± 8.4 | 51.0 ± 8.0 | 0.270 |
| Height, cm | 169.8 ± 8.4 | 168.3 ± 8.7 | 0.361 |
| Body mass index, kg/m2 | 18.2 ± 2.3 | 18.0 ± 2.3 | 0.566 |
| Education, senior middle school or above | 57 (95%) | 55 (91.7%) | 0.359 |
| Marriage status, married | 38 (63.3%) | 41 (68.3%) | 0.564 |
| Smoking history | 10 (16.7%) | 6 (10%) | 0.283 |
| Hypertension | 1 (1.7%) | 1 (1.7%) | 1.000 |
| Heart disorders | 1 (1.7%) | 0 (0) | 0.500 |
| Disease course, y | 7.1 ± 4.9 | 8.2 ± 5.0 | 0.226 |
| ASA (I/II) | 13/47 | 7/53 | 0.315 |
| PHQ-9 | 15.2 ± 2.45 | 15.6 ± 2.65 | 0.454 |
| HAMD-17 score | 19.5 ± 3.73 | 19.0 ± 3.59 | 0.475 |
| Time Point | Absolute Score | Change from Baseline | Treatment Difference | ||||
|---|---|---|---|---|---|---|---|
| Placebo | S-Ketamine | Placebo | S-Ketamine | ||||
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SE) | 95%CI | p-Value | |
| HAMD-17 | |||||||
| Baseline | 19.5 (3.73) | 19.0 (3.59) | |||||
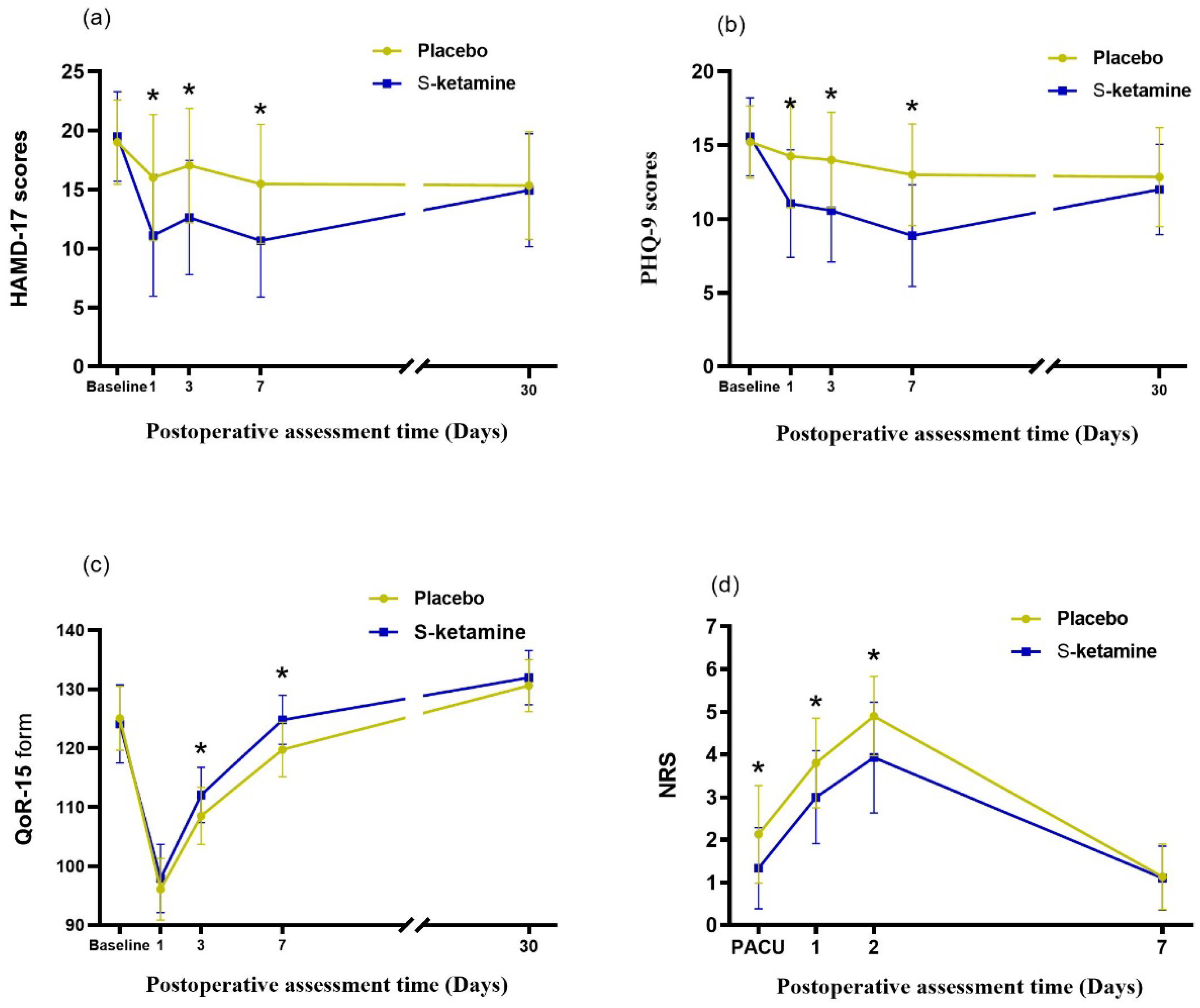
| Day 7 | 15.5 (5.04) | 10.7 (4.80) | −3.5 (2.17) | −8.8 (3.27) | −5.3 (0.50) | −6.3 to −4.3 | <0.001 |
| PHQ-9 | |||||||
| Baseline | 15.2 (2.45) | 15.6 (2.65) | |||||
| Day 7 | 13.0 (3.44) | 8.9 (3.45) | −2.2 (1.49) | −6.7 (2.53) | −4.5 (0.38) | −5.2 to −3.7 | <0.001 |
| Variables | Placebo, n = 60 | S-Ketamine, n = 60 | p-Value |
|---|---|---|---|
| Laparoscopic surgery | 18 (30%) | 12 (20%) | 0.206 |
| Blood loss, mL | 152.5 ± 89.5 | 174.2 ± 91.8 | 0.193 |
| Anesthesia duration, min | 140.0 (125.0–177.5) | 150.0 (121.3–180.0) | 0.721 |
| Sufentanil, μg | 31.8 (30.5–33.1) | 30.4 (29.2.0–31.6) | 0.110 |
| Remifentanil, μg | 623.5 (569.6–677.4) | 610.3 (552.7–667.9) | 0.739 |
| Propofol, mg | 945.9 (870.3–1021.5) | 941.0 (853.5–1028.5) | 0.993 |
| Postoperative opioid used, mg | 23.9 ± 8.4 | 16.4 ± 5.9 | <0.050 |
| Time to extubation, min | 31.0 (20.5–58.0) | 39.5 (22.0–50.8) | 0.854 |
| PPOI | 7 (11.7%) | 10 (16.7%) | 0.432 |
| Complication, n (%) | |||
| Nausea | 6 (10%) | 3 (5%) | 0.245 |
| Dizzy | 3 (5%) | 5 (8.3%) | 0.359 |
| Dysphoria | 1 (1.7%) | 4 (6.7) | 0.182 |
| Length of stay, days | 21 (17–25) | 20 (16–22) | 0.185 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Zhang, W.-H.; Lu, Y.-X.; Lu, B.-X.; Wang, Y.-B.; Cui, L.-Y.; Cheng, H.; Yuan, Z.-Y.; Zhang, J.; Gao, D.-P.; et al. Intraoperative Low-Dose S-Ketamine Reduces Depressive Symptoms in Patients with Crohn’s Disease Undergoing Bowel Resection: A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 1152. https://doi.org/10.3390/jcm12031152
Zhang Z, Zhang W-H, Lu Y-X, Lu B-X, Wang Y-B, Cui L-Y, Cheng H, Yuan Z-Y, Zhang J, Gao D-P, et al. Intraoperative Low-Dose S-Ketamine Reduces Depressive Symptoms in Patients with Crohn’s Disease Undergoing Bowel Resection: A Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(3):1152. https://doi.org/10.3390/jcm12031152
Chicago/Turabian StyleZhang, Zhen, Wen-Hao Zhang, Yin-Xiao Lu, Bo-Xuan Lu, Yi-Bo Wang, Li-Ying Cui, Hao Cheng, Zhen-Yu Yuan, Jie Zhang, Da-Peng Gao, and et al. 2023. "Intraoperative Low-Dose S-Ketamine Reduces Depressive Symptoms in Patients with Crohn’s Disease Undergoing Bowel Resection: A Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 3: 1152. https://doi.org/10.3390/jcm12031152
APA StyleZhang, Z., Zhang, W.-H., Lu, Y.-X., Lu, B.-X., Wang, Y.-B., Cui, L.-Y., Cheng, H., Yuan, Z.-Y., Zhang, J., Gao, D.-P., Gong, J.-F., & Ji, Q. (2023). Intraoperative Low-Dose S-Ketamine Reduces Depressive Symptoms in Patients with Crohn’s Disease Undergoing Bowel Resection: A Randomized Controlled Trial. Journal of Clinical Medicine, 12(3), 1152. https://doi.org/10.3390/jcm12031152