
Are YouTube Videos a Useful and Reliable Source of Information for Patients with Temporomandibular Joint Disorders?
 , , , ,
, , , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Health on the Net Foundation Code of Conduct Tool
2.2. Modified DISCERN
2.3. Global Quality Scale
2.4. Statistical Analysis
3. Results
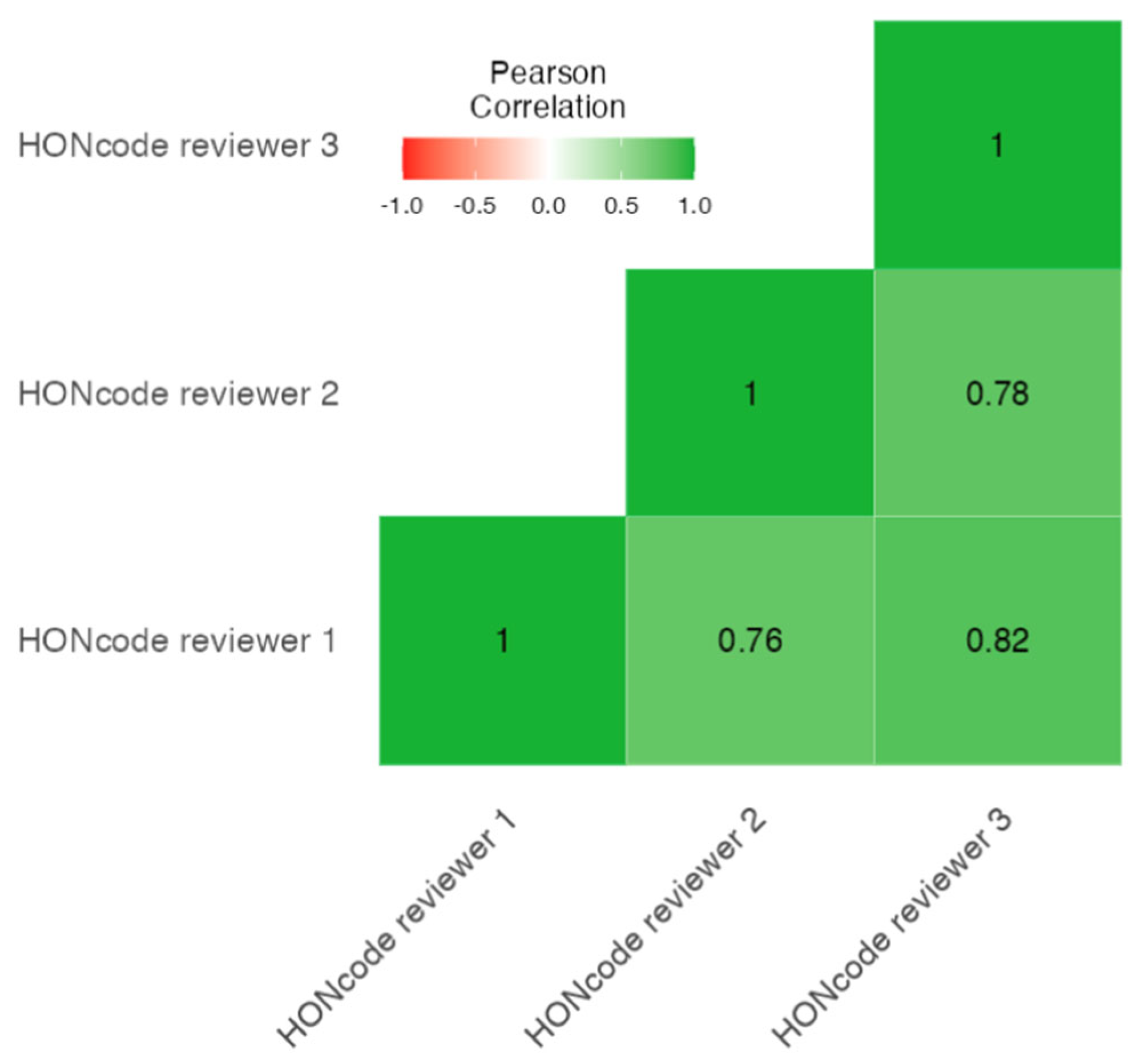
3.1. The HONcode Results
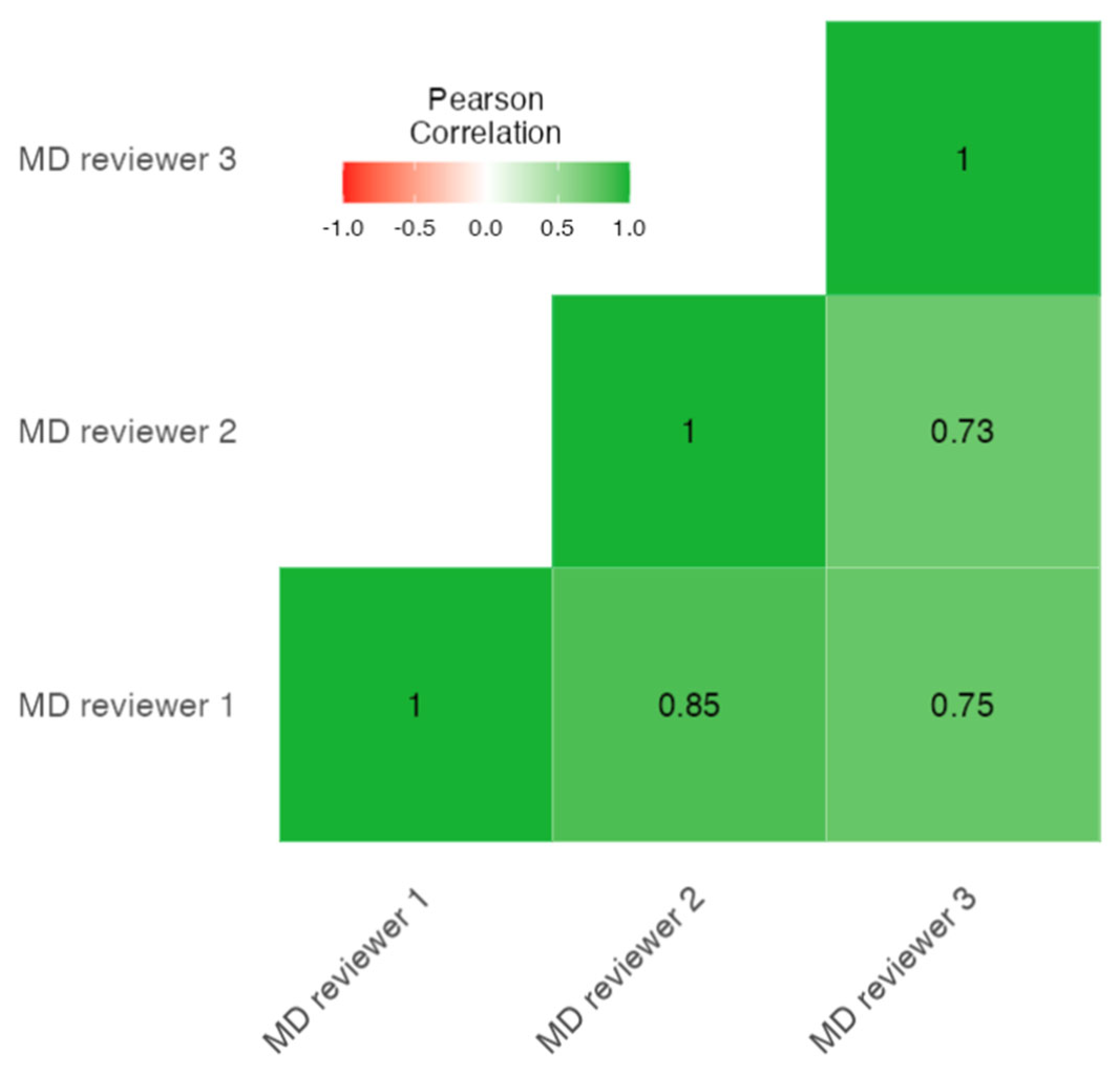
3.2. The Modified DISCERN Results
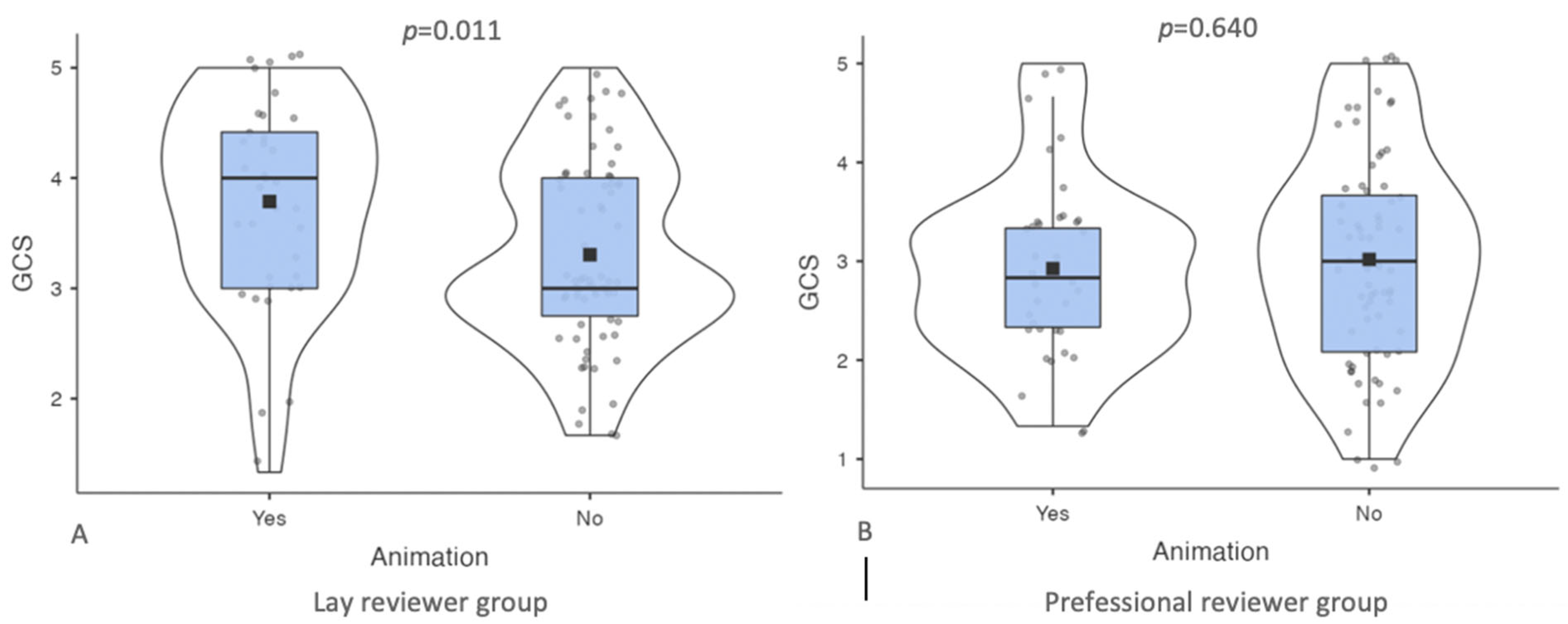
3.3. The Global Quality Scale Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, F.; Steinkeler, A. Epidemiology, diagnosis, and treatment of temporomandibular disorders. Dent. Clin. N. Am. 2013, 57, 465–479. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Yang, Y.; Dutra, E.H.; Robinson, J.L.; Wadhwa, S. Temporomandibular joint disorders in older adults. J. Am. Geriatr. Soc. 2018, 66, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Andre, A.; Kang, J.; Dym, H. Pharmacologic treatment for temporomandibular and temporomandibular joint disorders. Oral Maxillofac. Surg. North Am. 2022, 34, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Sousa, B.M.; Lopez-Valverde, N.; Lopez-Valverde, A.; Caramelo, F.; Fraile, J.F.; Payo, J.H.; Rodrigues, M.J. Different treatments in patients with temporomandibular joint disorders: A comparative randomized study. Medicina 2020, 56, 113. [Google Scholar] [CrossRef] [Green Version]
- Armijo-Olivo, S.; Pitance, L.; Singh, V.; Neto, F.; Thie, N.; Michelotti, A. Effectiveness of manual therapy and therapeutic exercise for temporomandibular disorders: Systematic review and meta-analysis. Phys. Ther. 2016, 96, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.H.; He, K.X.; Lin, C.J.; Liu, X.D.; Wu, L.; Chen, J.; Rausch-Fan, X. Efficacy of occlusal splints in the treatment of temporomandibular disorders: A systematic review of randomized controlled trials. Acta Odontol. Scand. 2020, 78, 580–589. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Farea, R.; Qasem, K.A.; Al-Wadeai, M.S.; Al-Sabahi, M.E.; Al-Iryani, G.M. Effectiveness of occlusal splint therapy in the management of temporomandibular disorders: Network meta-analysis of randomized controlled trials. Int. J. Oral. Maxillofac. Surg. 2020, 49, 1042–1056. [Google Scholar] [CrossRef]
- Vaira, L.A.; Raho, M.T.; Soma, D.; Salzano, G.; Dell’aversana Orabona, G.; Piombino, P.; De Riu, G. Complications and post-operative sequelae of temporomandibular joint arthrocentesis. Cranio 2018, 36, 264–267. [Google Scholar] [CrossRef]
- Vaira, L.A.; Soma, D.; Meloni, S.M.; Dell’aversana Orabona, G.; Piombino, P.; De Riu, G. Vertiginous crisis following temporomandibular joint arthrocentesis: A case report. Oral Maxillofac. Surg. 2017, 21, 79–81. [Google Scholar] [CrossRef]
- De Riu, G.; Vaira, L.A.; Carta, E.; Meloni, S.M.; Sembronio, S.; Robiony, M. Bone marrow nucleated cell concentrate autograft in temporomandibular joint degenerative disorders: 1-year results of a randomized clinical trial. J. Craniomaxillofac. Surg. 2019, 47, 1728–1738. [Google Scholar] [CrossRef]
- Rigon, M.; Pereira, L.M.; Bortoluzzi, M.C.; Loguercio, A.D.; Ramos, A.L.; Cardoso, J.R. Arthroscopy for temporomandibular disorders. Cochrane Database Syst. Rev. 2011, 5, CD006385. [Google Scholar]
- Al-Moraissi, E.A. Open versus arthroscopic surgery for the management of internal derangement of the temporomandibular joint: A meta-analysis of the literature. Int. J. Oral Maxillofac. Surg. 2015, 44, 763–770. [Google Scholar] [CrossRef] [PubMed]
- De Barros Pascoal, A.L.; Falcao Carvalho Porto de Freitas, R.; Granceiro da Silva, L.F.; Roncalli Costa Oliveira, A.G.; Dos Santos Calderon, P. Effectiveness of counseling on chronic pain management in patients with temporomandibular disorders. J. Oral Facial Pain Headache 2020, 34, 77–82. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, R.F.; Ferreira, M.A.; Barbosa, G.A.; Calderon, P.S. Counselling and self-management therapies for temporomandibular disorders: A systematic review. J. Oral Rehabil. 2013, 40, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues Conti, P.C.; da Mota Correa, A.S.; Pereira Lauris, J.R.; Stuginski-Barbosa, J. Management of painful temporomandibular joint clicking with different intraoral devices and counseling: A controlled study. J. Appl. Oral Sci. 2015, 23, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Albuquerque Melo, R.; Bastos Machado de Resende, C.M.; de Figueiredo Rego, C.S.; de Sousa Leite Bispo, A.; Seabra Barbosa, G.A.; Oliveira de Almeida, E. Conservative therapies to treat pain and anxiety associated with temporomandibular disorders: A randomized clinical trial. Int. Dent. J. 2020, 70, 245–253. [Google Scholar] [CrossRef]
- De Laat, A.; Stappaerts, K.; Papy, S. Counseling and physical therapy as treatment for myofascial pain of the masticatory system. J. Orofac. Pain 2003, 17, 42–49. [Google Scholar]
- Rickards, L.D. The effectiveness of non-invasive treatments for active myofascial trigger point pain: A systematic review of the litetrature. Int. J. Osteopath Med. 2006, 9, 120–136. [Google Scholar] [CrossRef]
- Mozhodeh, M.; Caroccia, F.; Moscagiuri, F.; Festa, F.; D’attilio, M. Evaluation of knowledge among dentists on symptoms and treatments of temporomandibular disorders in Italy. Int. J. Environ. Res. Public Health 2020, 17, 8760. [Google Scholar] [CrossRef]
- Gnauck, M.; Magnusson, T.; Ekberg, E. Knowledge and competence in temporomandibular disorders among Swedish general dental practitioners and dental hygienists. Acta Odontol Scand 2017, 75, 429–436. [Google Scholar] [CrossRef]
- Al Ghamdi, K.M.; Moussa, N.A. Internet use by the public to search for health-related information. Int. J. Med. Inform. 2012, 81, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Gholami-Kordkheili, F.; Wild, V.; Strech, D. The impact of social media on medical professionalism: A systematic qualitative review of challenges and opportunities. J. Med. Internet Res. 2013, 15, e184. [Google Scholar] [CrossRef] [PubMed]
- Madathil, K.C.; Rivera-Rodriguez, A.J.; Greenstein, J.S.; Gramopadhye, A.K. Healthcare information on YouTube: A systematic review. Health Inform. J. 2015, 21, 173–194. [Google Scholar] [CrossRef] [PubMed]
- Tonsaker, T.; Bartlett, G.; Trpkov, C. Health information on the internet: Gold mine or minefield? Can. Fam. Physician 2014, 60, 407–408. [Google Scholar]
- Zhao, Y.; Zhang, J. Consumer health information seeking social media: A literature review. Health Inf. Libr. J. 2017, 34, 268–283. [Google Scholar] [CrossRef] [Green Version]
- McMullan, M. Patients using the internet to obtain health information: How this affects the patient-health professional relationship. Patient Educ. Couns. 2006, 63, 24–28. [Google Scholar] [CrossRef]
- Kidy, S.; McGoldrick, D.M.; Stockton, P. YouTube™ as a source of information on extraction of third molars. Oral Maxillofac. Surg. 2021, 25, 519–524. [Google Scholar] [CrossRef]
- Bayazit, S.; Ege, B.; Koparal, M. Is the youtube™ a useful resource of information about orthognathic surgery?: A cross-sectional study. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e981–e987. [Google Scholar]
- Kurian, N.; Varghese, K.G.; Daniel, S.; Varghese, V.S.; Kaur, T.; Verma, R. Are YouTube videos on complete arch fixed implant-supported prostheses useful for patient education? J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef]
- Ward, B.; Ward, M.; Nicheporuck, A.; Alaeddin, I.; Paskhover, B. Assessment of YouTube as an informative resource on facial plastic surgery procedures. JAMA Facial Plast. Surg. 2019, 21, 75–76. [Google Scholar] [CrossRef]
- Hassona, Y.; Taimeh, D.; Marahleh, A.; Scully, C. YouTube as a source of information on mouth (oral) cancer. Oral Dis. 2016, 22, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Jansen, B.; Spink, A. An Analysis of Web Documents Retrieved and Viewed. In Proceedings of the 9th International Conference on Internet Computing, Las Vegas, NV, USA, 23–26 June 2003; Available online: https://faculty.ist.psu.edu/jjansen/academic/pubs/pages_viewed.pdf (accessed on 19 June 2022).
- Drozd, B.; Couvillon, E.; Suarez, A. Medical YouTube videos and methods of evaluation: Literature review. JMIR Med. Educ. 2018, 4, e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkens, F.M.; Ganter, C.; Kriegsmann, K.; Wilkens, H.; Kahn, N.; Goobie, G.C.; Ryerson, C.J.; Kreuter, M. YouTube-videos for patient education in lymphangioleiomyomatosis? Respir. Res. 2022, 23, 103. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Rodriguez, A.M.; Blanco-Diaz, M.; de la Fuente-Costa, M.; Hernandez-Sanchez, S.; Escobio-Prieto, I.; Casana, J. Review of the quality of YouTube videos recommending exercises for the COVID-19 lockdown. Int. J. Environ. Res. Public Health 2022, 19, 8016. [Google Scholar] [CrossRef]
- Rodriguez-Rodriguez, A.M.; Blanco-Diaz, M.; Lopez-Diaz, P.; de la Fuente Costa, M.; Duenas, L.; Escobio Prieto, I.; Calatayud, J.; Casana, J. Quality analysis of YouTube videos presenting shoulder exercises after breast cancer surgery. Breast Care 2022, 17, 188–198. [Google Scholar] [CrossRef]
- Bernard, A.; Langille, M.; Huges, S.; Rose, C.; Leddin, D.; Van Zanten, S.V. A systematic review of patient inflammatory bowel disease information resources on the World Wide Web. Am. J. Gastroenterol. 2007, 102, 2070–2077. [Google Scholar] [CrossRef]
- Toksoz, A.; Duran, M.B. Analysis of videos about vesicoureteral reflux on YouTube. J. Pediatr. Urol. 2021, 17, 858.e1–858.e6. [Google Scholar] [CrossRef]
- Cassidy, J.T.; Fitzgerald, E.; Cassidy, E.S.; Cleary, M.; Byrne, D.P.; Devitt, B.M.; Baker, J.F. YouTube provides poor information regarding anterior cruciate ligament injury and reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 840–845. [Google Scholar] [CrossRef]
- The Jamovi Project. Jamovi. (Version 2.3) [Computer Software]. 2022. Available online: https://www.jamovi.org (accessed on 20 November 2022).
- Simsek, H.; Buyuk, S.K.; Cetinkaya, E.; Tural, M.; Koseoglu, S. “How I whiten my teeth”: YouTube™ as a patient information resource for teeth whitening. BMC Oral Health 2020, 20, 183. [Google Scholar] [CrossRef]
- Osman, W.; Mohamed, F.; Elhassan, M.; Shoufan, A. Is YouTube a reliable source of health-related information? A systematic review. BMC Med. Educ. 2022, 22, 382. [Google Scholar] [CrossRef]
- Patel, R.; Chang, T.; Greysen, S.R.; Chopra, V. Social media use in chronic disease: A systematic review and novel taxonomy. Am. J. Med. 2015, 128, 1335–1350. [Google Scholar] [CrossRef] [PubMed]
- Zheng, K.; George, M.; Roehlkepartain, E.; Santelli, J.; Bruzzese, J.M.; Smaldone, A. Developmental assets of adolescents and young adults with chronic illness and comorbid depression: Qualitative study using YouTube. JMIR Ment. Health 2021, 8, e23960. [Google Scholar] [CrossRef] [PubMed]
- Braczynski, A.K.; Ganse, B.; Ridwan, S.; Schlenstedt, C.; Schulz, J.B.; Hoog Antink, c. YouTube videos on Parkinson’s disease are a relevant source of patient information. J. Park. Dis. 2021, 11, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Verkamp, J. Patient loyalty and the social media effect. J. Med. Pract. Manag. 2013, 29, 96–98. [Google Scholar]
- Langford, A.; Loeb, S. Perceived patient-provider communication quality and sociodemographic factors associated with watching health-related videos on YouTube: A cross-sectional analysis. J. Med. Internet Res. 2019, 21, e13512. [Google Scholar] [CrossRef]
- Portillo, I.A.; Johnson, C.V.; Johnson, S.Y. Quality evaluation of consumer health information websites found on Google, using DISCERN, CRAAP, and HONcode. Med. Ref. Serv. Q 2021, 40, 396–407. [Google Scholar] [CrossRef]
- Cacciatore, M.A. Misinformation and public opinion of science and health: Approaches, findings, and future directions. Proc. Natl. Acad. Sci. USA 2021, 118, e1912437117. [Google Scholar] [CrossRef]
- Pate, J.W.; Heathcote, L.C.; Simons, L.E.; Leake, H.; Moseley, G.L. Creating online animated videos to reach and engage youth: Lessons learned from pain science education and a call to action. Pediatr. Neonatol. Pain 2020, 2, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Huang, X.; Liu, Z. The effect of preoperative health education, delivered as animation videos, on postoperative anxiety and pain in femoral fractures. Front. Psychol. 2022, 13, 881799. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Principle | Definition |
|---|---|
| Authoritativeness | Indicates the qualifications of the authors |
| Complementarity | The information supports, rather than replaces, the doctor–patient relationship |
| Privacy | Respects the privacy and confidentiality of any personal data submitted to the site by the visitor |
| Attribution | Cites the sources of the published information, data, and medical and health pages |
| Justifiability | Supports with evidence any claims relating to benefits and performance |
| Transparency | Presents accessible and accurate email contacts |
| Financial disclosure | Identifies funding sources |
| Advertising policy | Clearly distinguishes advertising from editorial content |
| Video Characteristics |
|---|
| 1. Are the aims clear and achieved? |
| 2. Is reliable information used (i.e., are publications cited? Is the speaker a board certified practitioner?)? |
| 3. Is the information presented balanced and unbiased? |
| 4. Are additional sources of information listed for patient reference? |
| 5. Are areas of uncertainty mentioned? |
| Score | Definition |
|---|---|
| 1 | Poor quality, poor flow of the video, most important information missing, not useful for the patient |
| 2 | Generally poor quality and poor flow of the video, some significant information included but many important topics missing, of very limited use to the patient |
| 3 | Moderate quality, suboptimal flow, some important information is adequately presented but other topics are poorly discussed, somewhat useful for the patient |
| 4 | Good quality and generally good flow, most of the relevant information is included but some topics are not covered, useful for the patient |
| 5 | Excellent quality and flow, very useful for the patient |
| GQS Score Lay Reviewer 1 | GQS Score Lay Reviewer 2 | GQS Score Lay Reviewer 3 | GQS Score Professional Reviewer 1 | GQS Score Professional Reviewer 2 | GQS Score Professional Reviewer 3 | ||
|---|---|---|---|---|---|---|---|
| GQS score lay reviewer 1 | Pearson’s r | - | |||||
| p-value | - | ||||||
| GQS score lay reviewer 2 | Pearson’s r | 0.697 | - | ||||
| p-value | <0.001 | - | |||||
| GQS score lay reviewer 3 | Pearson’s r | 0.743 | 0.871 | - | |||
| p-value | <0.001 | <0.001 | - | ||||
| GQS score professional reviewer 1 | Pearson’s r | 0.016 | −0.015 | −0.094 | - | ||
| p-value | 0.868 | 0.881 | 0.335 | - | |||
| GQS score professional reviewer 2 | Pearson’s r | 0.112 | 0.092 | −0.008 | 0.774 | - | |
| p-value | 0.252 | 0.349 | 0.937 | <0.001 | - | ||
| GQS score professional reviewer 3 | Pearson’s r | 0.157 | 0.167 | 0.086 | 0.685 | 0.783 | - |
| p-value | 0.108 | 0.087 | 0.381 | <0.001 | <0.001 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaira, L.A.; Sergnese, S.; Salzano, G.; Maglitto, F.; Arena, A.; Carraturo, E.; Abbate, V.; Committeri, U.; Vellone, V.; Biglio, A.; et al. Are YouTube Videos a Useful and Reliable Source of Information for Patients with Temporomandibular Joint Disorders? J. Clin. Med. 2023, 12, 817. https://doi.org/10.3390/jcm12030817
Vaira LA, Sergnese S, Salzano G, Maglitto F, Arena A, Carraturo E, Abbate V, Committeri U, Vellone V, Biglio A, et al. Are YouTube Videos a Useful and Reliable Source of Information for Patients with Temporomandibular Joint Disorders? Journal of Clinical Medicine. 2023; 12(3):817. https://doi.org/10.3390/jcm12030817
Chicago/Turabian StyleVaira, Luigi Angelo, Silvia Sergnese, Giovanni Salzano, Fabio Maglitto, Antonio Arena, Emanuele Carraturo, Vincenzo Abbate, Umberto Committeri, Valentino Vellone, Andrea Biglio, and et al. 2023. "Are YouTube Videos a Useful and Reliable Source of Information for Patients with Temporomandibular Joint Disorders?" Journal of Clinical Medicine 12, no. 3: 817. https://doi.org/10.3390/jcm12030817