1. Introduction
Identifying the position of the mandibular foramen (MF) is essential for the successful administration of an inferior alveolar nerve block (IANB) and for avoiding damage to the inferior alveolar neurovascular bundle during ramus surgery. Located on the medial surface of the ramus, the MF is a bony orifice through which the inferior alveolar neurovascular bundle enters the mandible. The mandibular lingula (ML), located above the MF, is a key anatomical landmark for determining the position of the MF and for the orientation of the surgeon during ramus surgery. The ML is a bone plate structure that medially limits the MF and provides an attachment area for the sphenomandibular ligament [
1]. Determining the shape, position, and height of the ML is crucial for dentists and surgeons during IANBs and ramus surgeries [
2]. Understanding the position of the ML and the surrounding nerves and blood vessels is critical for a successful operation, thereby preventing excessive intraoperative blood loss and postoperative numbness in the lower lip [
3,
4].
In the past, determination of the morphometry of the lingula required using the dry mandible [
5,
6,
7,
8,
9,
10]. Recently, cone-beam computed tomography (CBCT) has provided high quality and accurate three-dimensional images to replace dry mandibles in morphometric study [
11,
12,
13,
14]. Studies [
15,
16,
17,
18,
19,
20,
21,
22] have employed CBCT images to determine the shape of the ML and measure the distances related to the ML. Although CBCT provides real-time measurements, the results obtained using the images may be affected by the resolution used for image processing and the applied image-recognition method. Furthermore, the ramus borders to ML distances are closely related to the horizontal and vertical reference planes set for CBCT scans and are considerably influenced by the consistency of the reference point. Therefore, this study reviewed articles on CBCT scans separately and explored the differences in the relative position of the ML on the ramus and its distance from other anatomical landmarks among patients of different sexes, ethnicities, and skeletal patterns. The present study included all reference planes used in the articles on CBCT.
2. Materials and Methods
2.1. Search Strategy
A literature search was conducted using the PubMed, Web of Science, and Embase databases. The search results were limited to studies published between 1970 and 2021. Results of participants aged <18 years were excluded from the review. The first search term used was “mandibular lingula location.” These results were further examined for the inclusion of CBCT.
2.2. Study Selection and Eligibility
Two authors of this study selected the articles using a data retrieval system. After reading the titles and abstracts, the authors independently assessed the selected articles based on eligibility criteria. The inclusion criteria were as follows: (1) Randomized controlled trials and observational studies; (2) Research participants aged ≥18 years. The exclusion criteria were as follows: (1) Non-English articles; (2) Non-human studies; (3) Duplicate articles. The authors read the full text of any article for which they could not reach a consensus regarding eligibility. Regarding the inter-rater reliability, the kappa coefficient was 0.890 (p < 0.05), demonstrating a high level of consistency between the two authors’ discretionary eligibility selections.
2.3. Data Extraction and Analysis of ML Location
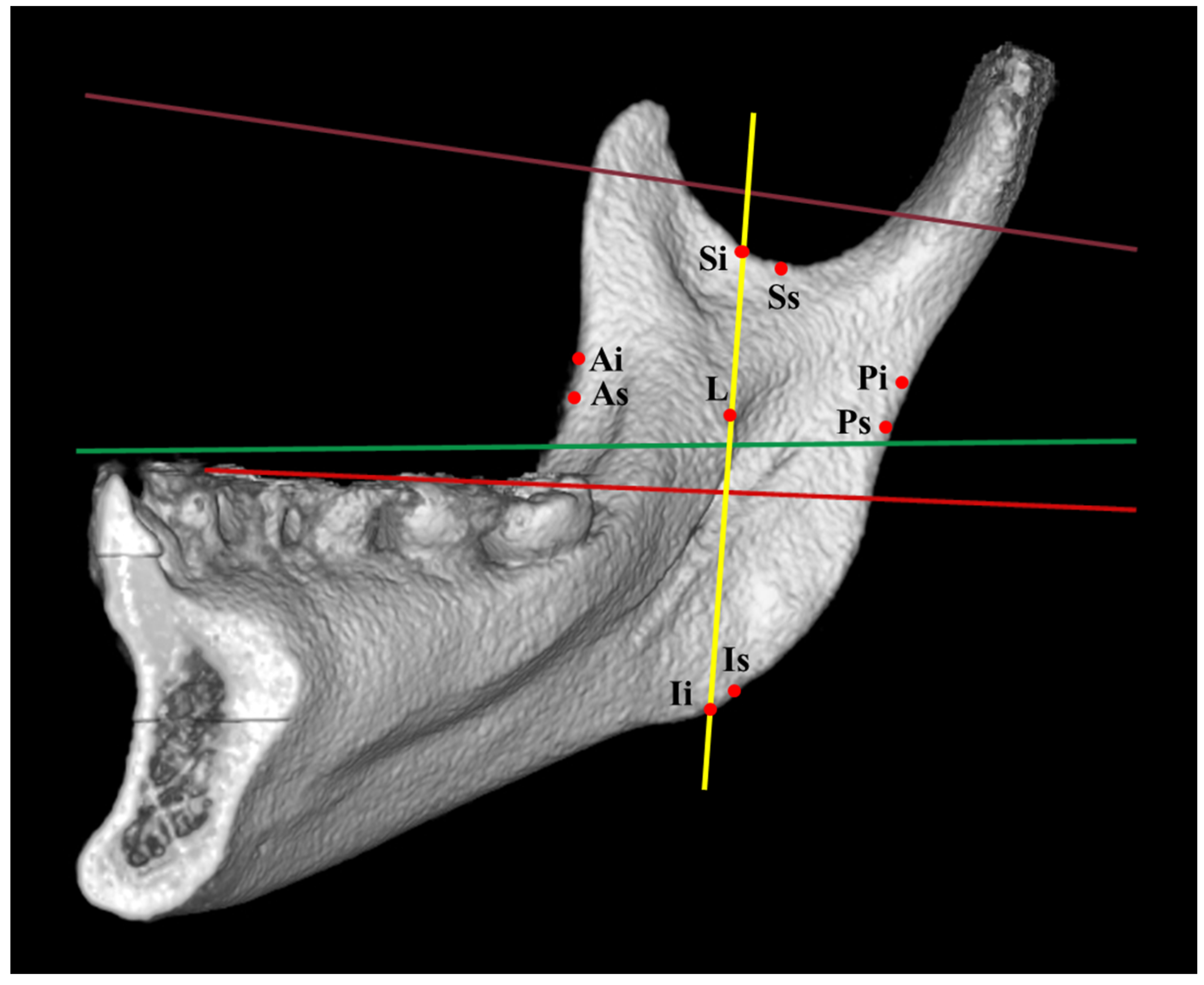
The data were examined independently by the two authors according to the research methodology. ML was identified as a reference landmark, and its related distances were obtained. If the results extracted by the two authors from the same article were inconsistent, the authors discussed the article with other authors to reach a consensus. The ML location was determined based on relevant reference planes (
Figure 1). The ML-related distances (
Figure 2) were measured using the following landmarks: lingula tip to anterior ramus border (As: landmark (shortest distance) at the anterior border of ramus; Ai: intersection landmark parallel to horizontal plane at the anterior border of ramus), posterior ramus border (Ps: landmark (shortest distance) at the posterior border of ramus; Pi: intersection landmark parallel to the horizontal plane at the posterior border of ramus), sigmoid notch (Ss: lowest location (shortest distance) of the sigmoid notch; Si: intersection landmark parallel to vertical plane and through lingula at the sigmoid notch), inferior ramus border (Is: landmark (shortest distance) at the inferior border of ramus; Ii: intersection landmark parallel to vertical plane and through lingula at the inferior border of ramus), and occlusal plane.
3. Results
3.1. Study Selection and Eligibility
Using the term “mandibular lingula location” (
Figure 3), 121 articles were identified from electronic databases (PubMed,
n = 53; Web of Science,
n = 36; Embase,
n = 32). Regarding the mandibular lingual location and CBCT, 29 articles were identified from electronic databases (PubMed,
n = 12; Web of Science,
n = 11; Embase,
n = 6). After verifying the eligibility of the selected articles, eight remained for inclusion in the study and full-text review by the authors.
3.2. Data Extraction and Analysis
3.2.1. ML Height
The sample size of the CBCT group ranged from 60 to 412 participants (
Table 1); the youngest participant was 18 years old and the oldest participant was 71 years old. The occlusal plane was used as the coordinate axis for measurements in five studies [
16,
18,
19,
20,
22]. The mean ML height ranged from 7 to 9.08 mm [
16,
17,
21].
3.2.2. Distances from Lingual Tip to Anterior Ramus Border and Posterior Ramus Border
The mean distance of the ML to the anterior ramus border ranged from 15.57 to 20 mm [
15,
16,
17,
18,
19,
20,
21,
22]. The mean distance of the ML to the posterior ramus border ranged from 12 to 18.2 mm [
15,
16,
17,
18,
19,
20,
21,
22].
3.2.3. Distances from Lingual Tip to Sigmoid Notch and Inferior Ramus Border
The mean distance of the ML to the sigmoid notch ranged from 13.34 to 20.72 mm [
15,
16,
17,
18,
19,
20,
21,
22]. The mean distance of the ML to the inferior ramus border ranged from 30.4 to 39.1 mm [
15,
16,
17,
18,
19,
20,
21,
22].
3.2.4. Distances from Lingual Tip to Occlusal Plane
Most ML locations were above the occlusal plane. Five articles reported that the ML was above the occlusal plane, with a distance range of 3.57 to 11.77 mm [
16,
18,
19,
20,
22].
4. Discussion
Mandibular growth is fully developed at approximately 18 years of age. Therefore, studies were excluded from our review if the included patients were younger than 18. The outcomes of the eligible studies for different sexes, races, and skeletal patterns are discussed below.
4.1. ML Height
Sekerci and Sisman [
16] observed that the ML height on the right side of the mandible was greater in men than in women. Hsu et al. [
21] reported that the ML height was significantly greater in men than in women and that there were no significant differences in the ML height between the left and right sides of the mandible. They also noted no significant differences in ML height among patients with Class I, Class II, or Class III malocclusion. ML height had similar dimensions in different races and skeletal patterns.
4.2. Anterior Ramus Border to Mandibular Lingula Distance (ARL Distance)
The reported distance of the ML from the anterior ramus border differed considerably between studies. Findik et al. [
15] reported a mean distance of 15–16 mm, whereas Hsu et al. [
21] reported a distance of 18–20 mm. These inconsistencies arose because each study used different reference points and planes (horizontal and vertical). Findik et al. [
15] directly measured the ML distance from the anterior ramus border using the axial plane as the reference plane, thereby obtaining the lowest measurement results. Other studies [
16,
18,
20] that used the occlusal plane as the reference plane obtained measurement results larger than those of Findik et al. [
15] but smaller than those of Hsu et al. [
21], who measured the distance using the Frankfort horizontal plane as the reference plane.
Several studies [
17,
18,
21,
22] reported no significant differences between the sexes or between the left and right sides of the mandible. However, Findik et al. [
15] reported that the distance between the ML and the anterior ramus border on the left side of the mandible was significantly greater than that on the right side. Hsu et al. [
21] reported that the distance of the ML from the anterior ramus border was significantly greater in men than in women but observed no significant differences in the distance of the ML from the anterior ramus border in patients with different skeletal patterns. However, Zhou et al. [
18] reported that the ML distance from the anterior ramus border was significantly greater in men with a low gonial angle (LGA) than that in men with a high gonial angle (HGA). Among the distances to the lingual, the anterior ramus border to the lingula distance is more important than the posterior border to the lingual distance.
For clinical application, we recommend using the occlusal plane as a reference plane. The measured landmark is a plane running parallel to the occlusal plane, which runs through the ML and intercepts the anterior ramus border. This method should result in more accurate administration of IANB and avoid damage to the inferior alveolar neurovascular bundle during ramus surgery.
4.3. Posterior Ramus Border to Lingula Distance
Some studies [
16,
18,
19,
20,
21] stated that the distance between the ML and the posterior ramus border was significantly greater in men than in women, except for Lupi et al. [
22], who observed no significant differences between the sexes. Sekerci and Sisman [
16] proposed that the distance between the ML and the posterior ramus border is significantly greater on the left side of the mandible in men than that on the left side of the mandible in women. Seneal et al. [
17] and Hsu et al. [
21] noted no significant differences in the distance between the ML and the posterior ramus border on the left and right sides of the mandible. Hsu et al. [
21] also observed no significant differences between participants with different classes of malocclusions. However, Zhou et al. [
20] reported that the distance between the ML and the posterior ramus border was significantly greater in men with LGA than that in men with HGA, in women with LGA than that in women with HGA, in men with LGA than that in women with LGA, and in men with HGA than that in women with HGA.
Participants of different races, ages, and sexes were recruited in each of the aforementioned studies [
15,
16,
17,
18,
19,
20,
21,
22]. The use of different reference planes, including the occlusal plane, Frankfort horizontal plane, and axial plane, resulted in considerable differences in the measured distances. Regarding the various landmarks at the posterior ramus border, we suggest that the occlusal plane is a better reference plane to set both landmarks of anterior and posterior ramus borders.
4.4. Sigmoid Notch to Lingual Distance
Regarding the distance from the ML to the sigmoid notch, Lupi et al. [
22] reported that the lowest mean distance was 13.34 mm in women. However, the measurements were not performed using the lowest point of the sigmoid notch. Instead, the authors measured the distance vertical to the occlusal plane from the lingula tip to the sigmoid notch, thereby obtaining a lower value. Lupi et al. [
22] and Hsu et al. [
21] reported no significant differences between sexes. Seneal et al. [
17] and Hsu et al. [
21] observed no significant difference between the left and right sides of the mandible. Hsu et al. [
21] reported no significant differences in the distance between the ML and sigmoid notches in patients with different skeletal patterns. However, Akcay et al. [
19] noted that the distance between the ML and the sigmoid notch was significantly greater in men with Class III malocclusion than that in women with Class III malocclusion. However, there were no significant differences in the distance of the ML from the sigmoid notch in men and women with Class I malocclusion. Zhou et al. [
18] observed that the distance between the ML and the sigmoid notch was significantly greater in men with LGA than in those with HGA. Moreover, the number of men with LGA and HGA was greater than the number of women with LGA and HGA. For consistency, we recommend that the measured landmark be the lowest point of the sigmoid notch.
4.5. Inferior Ramus Border to Lingula Distance
Among all studies, Senel et al. [
17] reported the greatest distance (38.3 mm) of the ML from the inferior ramus border. This result can be attributed to the reference plane used by Senel et al. [
17]. Several articles [
16,
18,
20,
21] reported that the distance between the ML and the inferior ramus border was significantly greater in men than in women. However, Lupi et al. [
22] reported no significant differences in the distance between the ML and the inferior ramus border between the sexes. Seneal et al. [
17] and Hsu et al. [
21] noted no significant differences in the ML distance from the inferior ramus border between the left and right sides of the mandible. Hsu et al. [
21] observed no significant differences in the distance between the ML and the inferior ramus border in patients with different classes of malocclusion. However, Zhou et al. [
18] reported that the distance between the ML and the inferior ramus border was significantly greater in men with LGA than that in men with HGA, and in women with LGA than that in women with HGA. Moreover, the number of men with LGA and HGA was greater than the number of women with LGA and HGA. In each of the aforementioned studies, participants of different ethnicities, ages, and sexes were recruited. Different reference planes, sigmoid notch landmarks, and inferior border landmarks were used, resulting in considerable differences in the measured distances. Tracing an obvious notch at the inferior border of the mandible is not always possible. Therefore, we recommend identifying two landmarks: (1) Setting a plane through the ML vertically to the occlusal plane and intercepting the inferior border; (2) Setting a plane from the lowest point of the sigmoid notch through to the inferior border.
4.6. Lingula to Occlusal Plane Distance
Akcay et al. [
19] reported the distance of the ML from the occlusal plane as 8–10 mm, whereas Lupi et al. [
22] reported this distance as 10–12 mm. There were no significant differences in the distance of the ML from the occlusal plane between the sexes or between the left and right sides of the mandible. Akcay et al. [
19] reported that the distance between the ML and the occlusal plane was significantly greater in patients with Class III malocclusion than that in those with Class I malocclusion. Zhou et al. [
18] reported that this distance was higher in men with LGA than that in women with LGA, and in men with HGA than that in women with HGA. Lingula-to-occlusal plane distance is more important than other distances in terms of administering an IANB and performing ramus surgery. CBCT is a useful tool for identifying ML morphology, location, and relation to the occlusal plane to avoid damage to the neurovascular bundle.
4.7. Clinical Relevance and Limitations of the Study
Numerous studies [
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
26] have been conducted on the position of the ML and have presented different results. CBCT images were affected by the resolution used for image processing. Moreover, the varied settings for different reference planes and points may have influenced the results of the study. Regarding clinical relevance, the occlusal plane is the preferred reference plane to identify the ML and MF to prevent injury to the inferior alveolar neurovascular bundle.
The limitations of this literature review were as follows: (1) Varied reference planes; (2) Rare reports of edentulous people; (3) Imbalance in the age distribution of the population; (4) Racial distribution disequilibrium of the population. For clinical applications, we recommend using the occlusal plane as the reference plane in future studies. However, there should be modifications to the occlusal plane if the patient is edentulous. Furthermore, future studies should include a sample distribution that considers the age and race of the study population.
5. Conclusions
Differences in age, race, and sex of participants, and in reference planes and points may have generated different measurement results. Significant differences were observed in the ML height between patients of different sexes and races and of those with different skeletal patterns. In most studies, the ML was located above the occlusal plane. In addition, most studies reported no significant differences in the distance of the ML to the anterior ramus border, posterior ramus border, sigmoid notch, or inferior ramus border among patients of different sexes and races and among those with different skeletal patterns. Additionally, the distances of the ML to the anterior ramus border, posterior ramus border, sigmoid notch, and inferior ramus border were significantly greater in patients with LGA than those in patients with HGA.
Author Contributions
Conceptualization, K.-J.H., C.-M.C. and H.-N.L.; methodology, Y.-T.C.; writing—original draft preparation, K.-J.H.; writing—review and editing, C.-M.C. and H.-N.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable for studies not involving humans or animals.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Richard, L.; Drake, A.; Vogl, W.; Adam, W.; Mitchell, M. Head and Neck: Gray’s Anatomy for Students, 2nd ed.; Churchill Livingstone: London, UK, 2010; 922p. [Google Scholar]
- Yeh, A.Y.E.; Finn, B.P.; Jones, R.H.B.; Goss, A.N. The variable position of the inferior alveolar nerve (IAN) in the mandibular ramus: A computed tomography (CT) study. Surg. Radiol. Anat. 2018, 40, 653–665. [Google Scholar] [CrossRef]
- Park, J.H.; Jung, H.D.; Kim, H.J.; Jung, Y.S. Anatomical study of the location of the antilingula, lingula, and mandibular foramen for vertical ramus osteotomy. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 15. [Google Scholar] [CrossRef]
- Lima, F.J.; Oliveira Neto, O.B.; Barbosa, F.T.; Sousa-Rodrigues, C.F. Location, shape and anatomic relations of the mandibular foramen and the mandibular lingula: A contribution to surgical procedures in the ramus of the mandible. Oral Maxillofac. Surg. 2016, 20, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Tuli, A.; Choudhry, R.; Choudhry, S.; Raheja, S.; Agarwal, S. Variation in shape of the lingula in the adult human mandible. J. Anat. 2000, 197, 313–317. [Google Scholar] [CrossRef]
- Kositbowornchai, S.; Siritapetawee, M.; Damrongrungruang, T.; Khongkankong, W.; Chatrchaiwiwatana, S.; Khamanarong, K.; Chanthaooplee, T. Shape of the lingula and its localization by panoramic radiograph versus dry mandibular measurement. Surg. Radiol. Anat. 2007, 29, 689–694. [Google Scholar] [CrossRef]
- Murlimanju, B.V.; Prabhu, L.V.; Pai, M.M.; Paul, M.T.; Saralaya, V.V.; Kumar, C.G. Morphological study of lingula of the mandibles in South Indian population. Morphologie 2012, 96, 16–20. [Google Scholar] [CrossRef]
- Jung, Y.H.; Cho, B.H.; Hwang, J.J. Location and shape of the mandibular lingula: Comparison of skeletal class I and class III patients using panoramic radiography and cone-beam computed tomography. Imaging Sci. Dent. 2018, 48, 185–190. [Google Scholar] [CrossRef]
- Hayward, J.; Richardson, E.R.; Malhotra, S.K. The mandibular foramen: Its anteroposterior position. Oral Surg. Oral Med. Oral Pathol. 1977, 44, 837–843. [Google Scholar] [CrossRef]
- Jansisyanont, P.; Apinhasmit, W.; Chompoopong, S. Shape, height, and location of the lingula for sagittal ramus osteotomy in Thais. Clin. Anat. 2009, 22, 787–793. [Google Scholar] [CrossRef]
- Sekerci, A.E.; Cantekin, K.; Aydinbelge, M. Cone beam computed tomographic analysis of the shape, height, and location of the mandibular lingula in a population of children. BioMed Res. Int. 2013, 2013, 825453. [Google Scholar] [CrossRef]
- Freire-Maia, B.; Machado, V.D.; Valerio, C.S.; Custódio, A.L.; Manzi, F.R.; Junqueira, J.L. Evaluation of the accuracy of linear measurements on multi-slice and cone beam computed tomography scans to detect the mandibular canal during bilateral sagittal split osteotomy of the mandible. Int. J. Oral. Maxillofac. Surg. 2017, 46, 296–302. [Google Scholar] [CrossRef]
- Tengku Shaeran, T.A.; Shaari, R.; Abdul Rahman, S.; Alam, M.K.; Muhamad Husin, A. Morphometric analysis of prognathic and non-prognathic mandibles in relation to BSSO sites using CBCT. J. Oral Biol. Craniofac. Res. 2017, 7, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Ahn, B.S.; Oh, S.H.; Heo, C.K.; Kim, G.T.; Choi, Y.S.; Hwang, E.H. Cone-beam computed tomography of mandibular foramen and lingula for mandibular anesthesia. Imaging Sci. Dent. 2020, 50, 125–132. [Google Scholar] [CrossRef]
- Findik, Y.; Yildirim, D.; Baykul, T. Three-dimensional anatomic analysis of the lingula and mandibular foramen: A cone beam computed tomography study. J. Craniofac. Surg. 2014, 25, 607–610. [Google Scholar] [CrossRef]
- Sekerci, A.E.; Sisman, Y. Cone-beam computed tomography analysis of the shape, height, and location of the mandibular lingula. Surg. Radiol. Anat. 2014, 36, 155–162. [Google Scholar] [CrossRef]
- Senel, B.; Ozkan, A.; Altug, H.A. Morphological evaluation of the mandibular lingula using cone-beam computed tomography. Folia Morphol. 2015, 74, 497–502. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.; Jeon, T.H.; Jun, S.H.; Kwon, J.J. Evaluation of mandibular lingula and foramen location using 3-dimensional mandible models reconstructed by cone-beam computed tomography. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 30. [Google Scholar] [CrossRef] [Green Version]
- Akcay, H.; Kalabalık, F.; Tatar, B.; Ulu, M. Location of the mandibular lingula: Comparison of skeletal Class I and Class III patients in relation to ramus osteotomy using cone-beam computed tomography. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 504–508. [Google Scholar] [CrossRef]
- Zhao, K.; Zhang, B.; Hou, Y.; Miao, L.; Wang, R.; Yuan, H. Imaging study on relationship between the location of lingula and the Gonial angle in a Chinese population. Surg. Radiol. Anat. 2019, 41, 455–460. [Google Scholar] [CrossRef]
- Hsu, K.J.; Tseng, Y.C.; Liang, S.W.; Hsiao, S.Y.; Chen, C.M. Dimension and Location of the Mandibular Lingula: Comparisons of Gender and Skeletal Patterns Using Cone-Beam Computed Tomography. BioMed Res. Int. 2020, 2020, 2571534. [Google Scholar] [CrossRef] [Green Version]
- Lupi, S.M.; Landini, J.; Olivieri, G.; Todaro, C.; Scribante, A.; Rodriguez YBaena, R. Correlation between the Mandibular Lingula Position and Some Anatomical Landmarks in Cone Beam CT. Healthcare 2021, 9, 1747. [Google Scholar] [CrossRef]
- Apinhasmit, W.; Chompoopong, S.; Jansisyanont, P.; Supachutikul, K.; Rattanathamsakul, N.; Ruangves, S.; Sangvichien, S. The study of position of antilingula, midwaist of mandibular ramus and midpoint between coronoid process and gonion in relation to lingula of 92 Thai dried mandibles as potential surgical landmarks for vertical ramus osteotomy. Surg. Radiol. Anat. 2011, 33, 337–343. [Google Scholar] [CrossRef]
- Monnazzi, M.S.; Passeri, L.A.; Gabrielli, M.F.; Bolini, P.D.; de Carvalho, W.R.; da Costa Machado, H. Anatomic study of the mandibular foramen, lingula and antilingula in dry mandibles, and its statistical relationship between the true lingula and the antilingula. Int. J. Oral Maxillofac. Surg. 2012, 41, 74–78. [Google Scholar] [CrossRef]
- Jang, H.Y.; Han, S.J. Measurement of mandibular lingula location using cone-beam computed tomography and internal oblique ridge-guided inferior alveolar nerve block. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, D.Y.; Hur, M.S. Anatomical review of the mandibular lingula for inferior alveolar nerve block. Folia Morphol. 2021, 80, 786–791. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).






{kind=link}
{kind=link}
{kind=link}