

Heart Failure Association-International Cardio-Oncology Society Risk Score Validation in HER2-Positive Breast Cancer
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
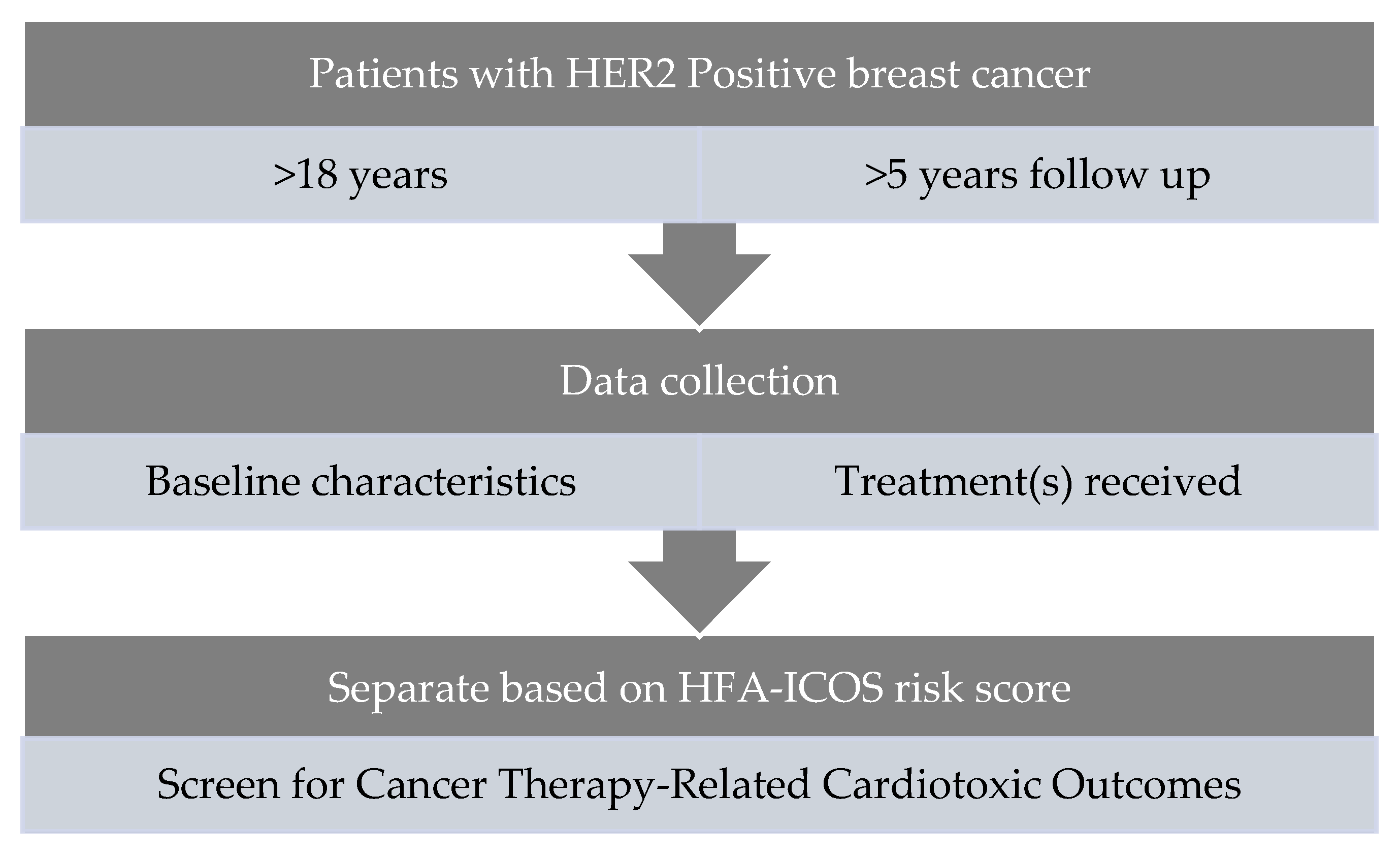
2.1. Participants
2.2. Data Collection
2.3. Risk Stratification
2.4. Study Outcomes and Definitions
2.5. Echocardiography
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment Characteristics
3.3. CTRCT and Cardioprotective Therapies
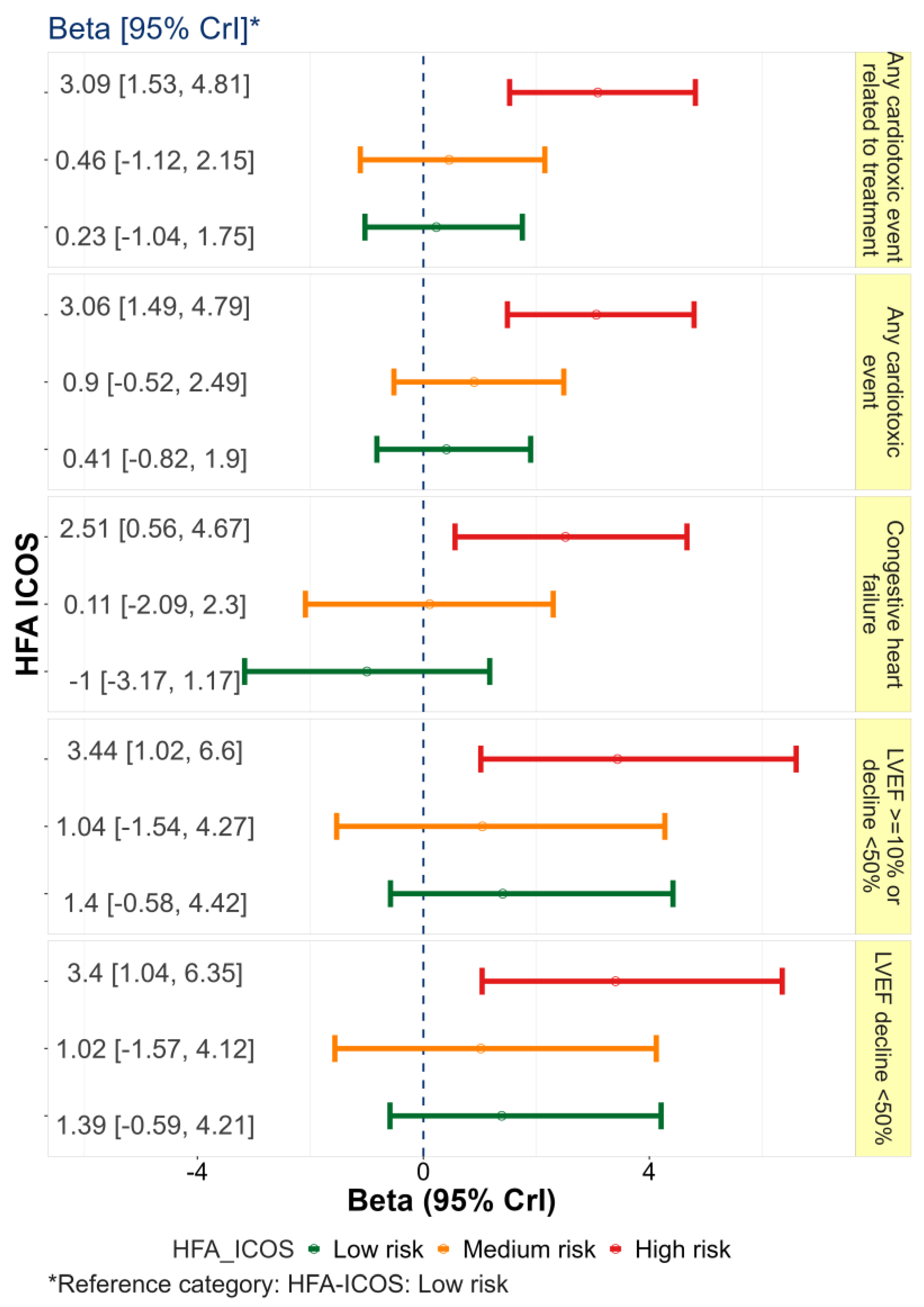
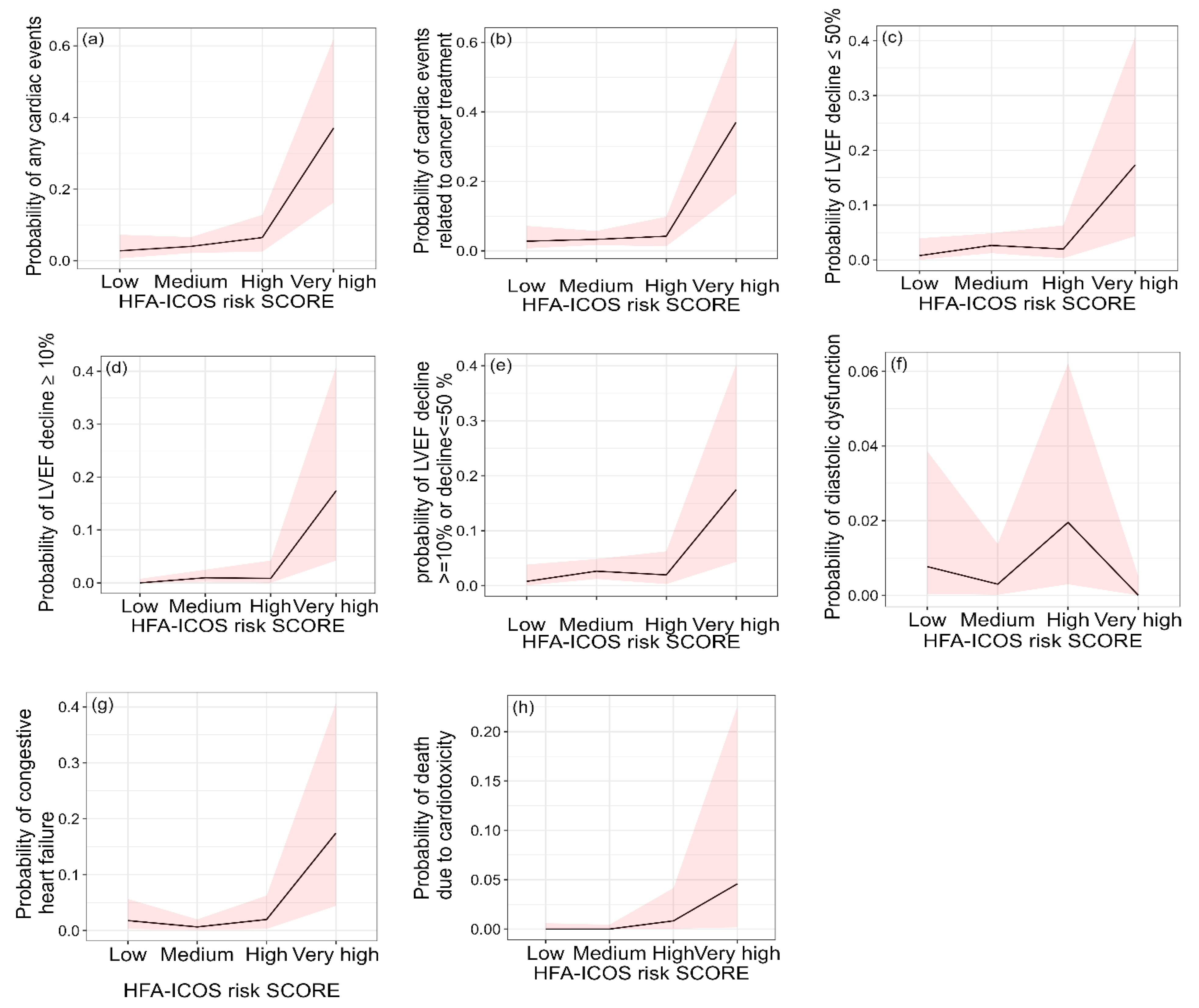
3.4. HFA-ICOS Risk Score Performance
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Prim. 2019, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Bouwer, N.I.; Jager, A.; Liesting, C.; Kofflard, M.J.; Brugts, J.J.; Kitzen, J.J.; Boersma, E.; Levin, M.-D. Cardiac monitoring in HER2-positive patients on trastuzumab treatment: A review and implications for clinical practice. Breast 2020, 52, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.L.; Lancellotti, P.; Muñoz, D.R.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Broberg, A.M.; Geisler, J.; Tuohinen, S.; Skytta, T.; Hrafnkelsdóttir, J.; Nielsen, K.M.; Hedayati, E.; Omland, T.; Offersen, B.V.; Lyon, A.R.; et al. Prevention, Detection, and Management of Heart Failure in Patients Treated for Breast Cancer. Curr. Heart Fail. Rep. 2020, 17, 397–408. [Google Scholar] [CrossRef]
- Jeyaprakash, P.; Sangha, S.; Ellenberger, K.; Sivapathan, S.; Pathan, F.; Negishi, K. Cardiotoxic Effect of Modern Anthracycline Dosing on Left Ventricular Ejection Fraction: A Systematic Review and Meta-Analysis of Placebo Arms from Randomized Controlled Trials. J. Am. Heart Assoc. 2021, 10, e018802. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: A position statement and new risk assessment tools from the C ardio- O ncology S tudy G roup of the H eart F ailure A ssociation of the E uropean S ociety of C ardiology in collaboration with the I nternational C ardio- O ncology S ociety. Eur. J. Heart Fail. 2020, 22, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Battisti, N.M.L.; Andres, M.S.; Lee, K.A.; Ramalingam, S.; Nash, T.; Mappouridou, S.; Senthivel, N.; Asavisanu, K.; Obeid, M.; Tripodaki, E.-S.; et al. Incidence of cardiotoxicity and validation of the Heart Failure Association-International Cardio-Oncology Society risk stratification tool in patients treated with trastuzumab for HER2-positive early breast cancer. Breast Cancer Res. Treat. 2021, 188, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef] [PubMed]
- Davey, M.G.; Kerin, E.; O'Flaherty, C.; Maher, E.; Richard, V.; McAnena, P.; McLaughlin, R.P.; Sweeney, K.J.; Barry, M.K.; Malone, C.M.; et al. Clinicopathological response to neoadjuvant therapies and pathological complete response as a biomarker of survival in human epidermal growth factor receptor-2 enriched breast cancer—A retrospective cohort study. Breast 2021, 59, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachssukampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.; Braybrooke, J.; Gray, R.; Hills, R.; Liu, Z.; Peto, R.; Davies, L.; Dodwell, D.; McGale, P.; Pan, H.; et al. Trastuzumab for early-stage, HER2-positive breast cancer: A meta-analysis of 13 864 women in seven randomised trials. Lancet Oncol. 2021, 22, 1139–1150. [Google Scholar] [CrossRef] [PubMed]
- Ezaz, G.; Long, J.B.; Gross, C.P.; Chen, J. Risk Prediction Model for Heart Failure and Cardiomyopathy After Adjuvant Trastuzumab Therapy for Breast Cancer. J. Am. Heart Assoc. 2014, 3, e000472. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant Trastuzumab in HER2-Positive Breast Cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [PubMed]
- Linssen, P.B.C.; Veugen, M.G.J.; Henry, R.M.A.; Van Der Kallen, C.J.H.; Kroon, A.A.; Schram, M.T.; Rocca, H.-P.B.-L.; Stehouwer, C.D.A. Associations of (pre)diabetes with right ventricular and atrial structure and function: The Maastricht Study. Cardiovasc. Diabetol. 2020, 19, 88. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, N.; Singh, A.; Zhou, W.; Gupta, A.; Fujikura, K.; Byrne, C.; Harms, H.J.; Osborne, M.T.; Bravo, P.; Andrikopoulou, E.; et al. Coronary Microvascular Dysfunction, Left Ventricular Remodeling, and Clinical Outcomes in Patients with Chronic Kidney Impairment. Circulation 2020, 141, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Serrano, C.; Cortés, J.; De Mattos-Arruda, L.; Bellet, M.; Gómez, P.; Saura, C.; Pérez, J.; Vidal, M.; Muñoz-Couselo, E.; Carreras, M.J.; et al. Trastuzumab-related cardiotoxicity in the elderly: A role for cardiovascular risk factors. Ann. Oncol. 2012, 23, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Kirova, Y.M.; Cao, L.; Arsene-Henry, A.; Chen, J. Cardiotoxicity associated with radiotherapy in breast cancer: A question-based review with current literatures. Cancer Treat. Rev. 2018, 68, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Bhagat, A.; Kleinerman, E.S. Anthracycline-Induced Cardiotoxicity: Causes, Mechanisms, and Prevention. Adv. Exp. Med. Bio. 2020, 1257, 181–192. [Google Scholar] [CrossRef]
- Lunardi, M.; Al-Habbaa, A.; Abdelshafy, M.; Davey, M.G.; Elkoumy, A.; Ganly, S.; Elzomor, H.; Cawley, C.; Sharif, F.; Crowley, J.; et al. Genetic and RNA-related molecular markers of trastuzumab-chemotherapy-associated cardiotoxicity in HER2 positive breast cancer: A systematic review. BMC Cancer 2022, 22, 396. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| With Cardiotoxicity N (%) | Without Cardiotoxicity N (%) | Posterior Beta | 95% Credible Interval for Beta | |
|---|---|---|---|---|
| Characteristics | ||||
| Age (>65 year/<65 year) | 5/18 (21.7) | 128/356 (26.4) | −0.319 | (−1.42, 0.63) |
| Diabetes | 1/22 (4.3) | 22/440 (4.8) | −0.624 | (−3.8, 1.38) |
| Hypertension | 10/13 (43.5) | 96/366 (20.8) | 1.055 | (0.171, 1.9) |
| Kidney disease | 3/20 (13) | 28/434 (6.1) | 0.69 | (−0.83, 1.92) |
| Congestive cardiac failure | 5 (1.3) | 12 (9) | ||
| Smoking | 5/16 (23.8) | 101/331 (23.4) | −0.04 | (−1.19, 0.94) |
| Death | 17/6 (73.9) | 253/230 (52.4) | 0.991 | (0.05, 2.01) |
| Tumour Features | ||||
| Grade 0 or 1 | 0 (5.3) | 31 (8.3) | - | - |
| Grade 2 | 7 (36.9) | 176 (33.8) | 51.87 | (1.55, 215.14) |
| Grade 3 | 16 (57.8) | 277 (57.9) | 52.28 | (1.99, 215.6) |
| Previous trastuzumab | 22/1 (95.7) | 353/131 (72.9) | 2.5 | (0.62, 5.44) |
| ER status (positive/negative) | 14/9 (59.4) | 288/193 (60.2) | −0.06 | (−0.94, 0.79) |
| PgR status (positive/negative) | 11/12 (47.8) | 229/251 (47.7) | 0.003 | (−0.84, 0.85) |
| Histology | ||||
| Ductal | 313 (83.7) | 108 (81.2) | 0.45 | (−0.73, 1.94) |
| Lobular | 1/22 (4.3) | 23/461 (4.8) | −0.62 | (−3.7, 1.36) |
| Mixed | 0/23 (0) | 4/480 (0.8) | - | - |
| Other | 2/21 (8.7) | 56/428 (11.6) | −0.541 | (−2.46, 0.85) |
| Cardiac Therapy | ||||
| Aspirin | 0 | 3/49 (0.6) | - | - |
| Beta blockers | 0/23 (0) | 53/431 (0.8) | - | - |
| Statins | 37 (9.9) | 48 (36.1) | 0.001 | |
| Anticoagulant | 23/0 (100) | 432/48 (89.3) | 28.4 | (1.78, 118.88) |
| ACE inhibitor | 0 | 4/48 (12) | - | - |
| (A) | |||||
|---|---|---|---|---|---|
| Treatment Characteristic | Category | With Cardiotoxicity N (%) | Without Cardiotoxicity N (%) | Posterior Beta | 95% Credible Interval for Beta |
| Concurrent chemotherapy | Paclitaxel; (yes/no) | 6/15 (28.6%) | 92/318 (22.4%) | 0.273 | (−0.8, 1.22) |
| Docetaxel; (yes/no) | 14/7 (66.7%) | 226/168 (57.4%) | 0.41 | (−0.5, 1.35) | |
| Anthracycline (Doxorubicin); (yes/no) | 0/23 (17.2%) | 39/445 (8.1%) | 0.86 | (−0.05, 1.73) | |
| Carboplatin; (yes/no) | 7/14 (33.3%) | 160/233 (40.7%) | −0.432 | (−3.6, 1.6) | |
| Epirubicin | - | 2 (0.5%) | 0 (0 %) | - | - |
| Pertuzumab (yes/no) | - | 1/22 (4.1%) | 20/464 (4.3%) | −0.08 | (−0.98, 1.99) |
| Radiotherapy (yes/no) | - | 15/6 (65.2%) | 313/104 (64.7%) | −0.12 | (−1.08, 0.95) |
| Endocrine therapy | Tamoxifen (yes/no) | 8/15 (34.8%) | 127/357 (26.2%) | 0.376 | (−0.51, 1.25) |
| Letrozole (yes/no) | 10/13 (43.5%) | 132/352 (27.3%) | 0.704 | (−0.16, 1.55) | |
| Other Aromatase inhibitors (yes/no) | 1/22 (4.3%) | 40/444 (8.3%) | −1.2 | (−4.23, 0.73) | |
| (B) | |||||
| Treatment Characteristic | Category | Low Risk (N = 100) | Medium Risk (N = 301) | High Risk (N = 90) | Very High Risk (N = 16) |
| Concurrent chemotherapy | Paclitaxel; (yes/no) | 13 (13%) | 59 (19.6%) | 20 (22.2%) | 6 (37.5%) |
| Docetaxel; (yes/no) | 55 (55%) | 146 (48.5%) | 34 (37.8%) | 5 (31.3%) | |
| Anthracycline (Doxorubicin); (yes/no) | 12 (13%) | 51 (17%) | 19 (21.1%) | 5 (31.3%) | |
| Carboplatin; (yes/no) | 36 (36%) | 108 (35.9%) | 18 (20%) | 5 (31.3%) | |
| Epirubicin use | Yes | 2 (2%) | 0 (0%) | 0 (0%) | 0 (0%) |
| No | 78 (78%) | 260 (86.4%) | 78 (86.7%) | 14 (87.5%) | |
| Pertuzumab use | Yes | 3 (3%) | 17 (5.6%) | 1 (1.1%) | 0 (0%) |
| No | 97 (97%) | 284 (94.4%) | 89 (98.9%) | 16 (100%) | |
| Radiotherapy use | Yes | 60 (60%) | 199 (66.1%) | 57 (63.3%) | 12 (75%) |
| No | 22 (22%) | 64 (21.3%) | 22 (24.4%) | 2 (12.5%) | |
| Unknown | 18 (18%) | 38 (12.6%) | 11 (12.2%) | 2 (12.5%) | |
| Endocrine use | None | 25 (25%) | 113 (37.5%) | 42 (46.7%) | 5 (31.3%) |
| Tamoxifen | 31 (31%) | 80 (26.6%) | 22 (24.4%) | 2 (12.5%) | |
| Letrozole | 30 (30%) | 83 (27.6%) | 23 (25.6%) | 6 (37.5%) | |
| Other aromatase inhibitors | 9 (9%) | 21 (7%) | 9 (10%) | 2 (12.5%) | |
| Cardiac Events | Overall (N = 507) | Age < 65 Years (N = 374) | Age ≥ 65 Years (N = 133) | Beta (95% CrI) | Low Risk (N = 100) | Medium Risk (N = 301) | High Risk (N = 90) | Very High Risk (N = 16) |
|---|---|---|---|---|---|---|---|---|
| Overall: N (%) | 27 (5.3%) | 19 (3.7%) | 8 (1.6%) | −0.13 (−0.97, 0.78) | 3 (3%) | 12 (3.98%) | 6 (4.5%) | 6 (37.5%) |
| Not related to cancer treatment: N (%) | 4 (0.8%) | 1 (0.2%) | 3 (0.6%) | - | 0 | 2 (0.7%) | 2 (0.7%) | 0 |
| Related to cancer treatment: N (%) | 23 (4.5%) | 18 (3.6%) | 5 (1%) | 0.33 (−0.63, 1.47) | 3 (3%) | 10 (3.3%) | 4 (4.4%) | 6 (37.5%) |
| LVEF decline ≥10%: N (%) | 7 (1.4%) | 6 (1.2%) | 1 (0.2%) | 1.16 (−0.87, 4.11) | 0 | 3 (1%) | 1 (1.1%) | 3 (18.8%) |
| LVEF decline below 50%: N (%) | 14 (2.8%) | 13 (2.6%) | 1 (0.2%) | 1.97 (0.08, 4.85) | 1 (1%) | 8 (2.7%) | 2 (2.2%) | 3 (18.8%) |
| LVEF decline ≥10%/below 50%: N (%) | 14 (2.8%) | 13 (2.6%) | 1 (0.2%) | 1.94 (0.03, 4.89) | 1 (1%) | 8 (2.7%) | 2 (2.2%) | 3 (18.8%) |
| Congestive heart failure: N (%) | 9 (1.8%) | 5 (1%) | 4 (0.8%) | −0.77 (−2.12, 0.64) | 2 (2%) | 2 (0.7%) | 2 (2.2%) | 3 (18.8%) |
| Diastolic dysfunction: N (%) | 4 (0.8%) | 2 (0.4%) | 2 (0.4%) | 0.44 (−1.83, 3.45) | 1 (1%) | 1 (0.7%) | 2 (2.2%) | 0 |
| Death due to cardiotoxicity: N (%) | 2 (0.4%) | 2 (0.4%) | 0 (0%) | −0.77 (−3.82, 2.43) | 0 | 0 | 1 (1.1%) | 1 (6.3%) |
| Treatment Characteristic Category | Overall (N = 507) | Age < 65 Years (N = 374) | Age ≥ 65 Years (N = 133) | p-Value | Low Risk (N = 100) | Medium Risk (N = 301) | High Risk (N = 90) | Very High Risk (N = 16) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| (ACEi/ARB) | 4 (0.8%) | 1 (0.3%) | 3 (2.3%) | 0.002 | 0 (0%) | 4 (1.3%) | 0 (0%) | 0 (0%) | 0.12 |
| Alpha blocker | 2 (0.4%) | 1 (0.3%) | 1 (0.8%) | 0.070 | 0 (0%) | 2 (0.7%) | 0 (0%) | 0 (0%) | 0.13 |
| Beta blocker | 4 (0.8%) | 3 (0.8%) | 1 (0.8%) | 0.19 | 2 (2%) | 2 (0.7%) | 0 (0%) | 0 (0%) | 0.078 |
| Statins | 5 (1%) | 1 (0.3%) | 4 (3%) | 0.001 | 0 (0%) | 5 (1.7%) | 0 (0%) | 0 (0%) | 0.13 |
| CCB | 2 (0.4%) | 1 (0.3%) | 1 (0.8%) | 0.085 | 0 (0%) | 2 (0.7%) | 0 (0%) | 0 (0%) | 0.32 |
| Aspirin | 3 (0.6%) | 1 (0.3%) | 2 (1.5%) | 0.001 | 0 (0%) | 2 (0.7%) | 1 (1.1%) | 0 (0%) | 0.20 |
| Diuretic | 2 (0.4%) | 0 (0%) | 2 (1.5%) | 0.007 | 0 (0%) | 1 (0.3%) | 1 (1.1%) | 0 (0%) | 0.079 |
| Cardiac Events | Sensitivity | Specificity | AUC, 95% CI | PPV | NPV | Accuracy |
|---|---|---|---|---|---|---|
| Overall | 0.26 | 0.97 | 0.652 (0.53, 0.76) | 0.113 | 0.963 | 0.785 |
| Related to cancer treatment | 0.26 | 0.98 | 0.643 (0.51, 0.76) | 0.375 | 0.965 | 0.947 |
| LVEF decline ≥10% | 0.42 | 0.974 | 0.762 (0.55, 0.97) | 0.188 | 0.992 | 0.966 |
| LVEF decline below 50% | 0.214 | 0.973 | 0.629 (0.47, 0.78) | 0.188 | 0.978 | 0.953 |
| LVEF decline ≥10%/below 50% | 0.214 | 0.974 | 0.629 (0.47, 0.78) | 0.188 | 0.978 | 0.953 |
| CHF | 0.55 | 0.79 | 0.658 (0.46, 0.85) | 0.047 | 0.99 | 0.793 |
| Diastolic dysfunction | 0.50 | 0.79 | 0.588 (0.29, 0.88) | 0.019 | 0.995 | 0.791 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cronin, M.; Crowley, A.; Davey, M.G.; Ryan, P.; Abdelshafy, M.; Elkoumy, A.; Elzomor, H.; Arsang-Jang, S.; Ganly, S.; Nash, P.; et al. Heart Failure Association-International Cardio-Oncology Society Risk Score Validation in HER2-Positive Breast Cancer. J. Clin. Med. 2023, 12, 1278. https://doi.org/10.3390/jcm12041278
Cronin M, Crowley A, Davey MG, Ryan P, Abdelshafy M, Elkoumy A, Elzomor H, Arsang-Jang S, Ganly S, Nash P, et al. Heart Failure Association-International Cardio-Oncology Society Risk Score Validation in HER2-Positive Breast Cancer. Journal of Clinical Medicine. 2023; 12(4):1278. https://doi.org/10.3390/jcm12041278
Chicago/Turabian StyleCronin, Michael, Aileen Crowley, Matthew G. Davey, Peter Ryan, Mahmoud Abdelshafy, Ahmed Elkoumy, Hesham Elzomor, Shahram Arsang-Jang, Sandra Ganly, Patrick Nash, and et al. 2023. "Heart Failure Association-International Cardio-Oncology Society Risk Score Validation in HER2-Positive Breast Cancer" Journal of Clinical Medicine 12, no. 4: 1278. https://doi.org/10.3390/jcm12041278
APA StyleCronin, M., Crowley, A., Davey, M. G., Ryan, P., Abdelshafy, M., Elkoumy, A., Elzomor, H., Arsang-Jang, S., Ganly, S., Nash, P., Crowley, J., Sharif, F., Simpkin, A., Lowery, A., Wijns, W., Kerin, M., & Soliman, O. (2023). Heart Failure Association-International Cardio-Oncology Society Risk Score Validation in HER2-Positive Breast Cancer. Journal of Clinical Medicine, 12(4), 1278. https://doi.org/10.3390/jcm12041278