
Clinical Outcomes after Percutaneous Coronary Intervention for Cardiogenic Shock Secondary to Total Occlusive Unprotected Left Main Coronary Artery Lesion-Related Acute Myocardial Infarction
 , , and
, , and
Abstract
:1. Introduction
2. Methods
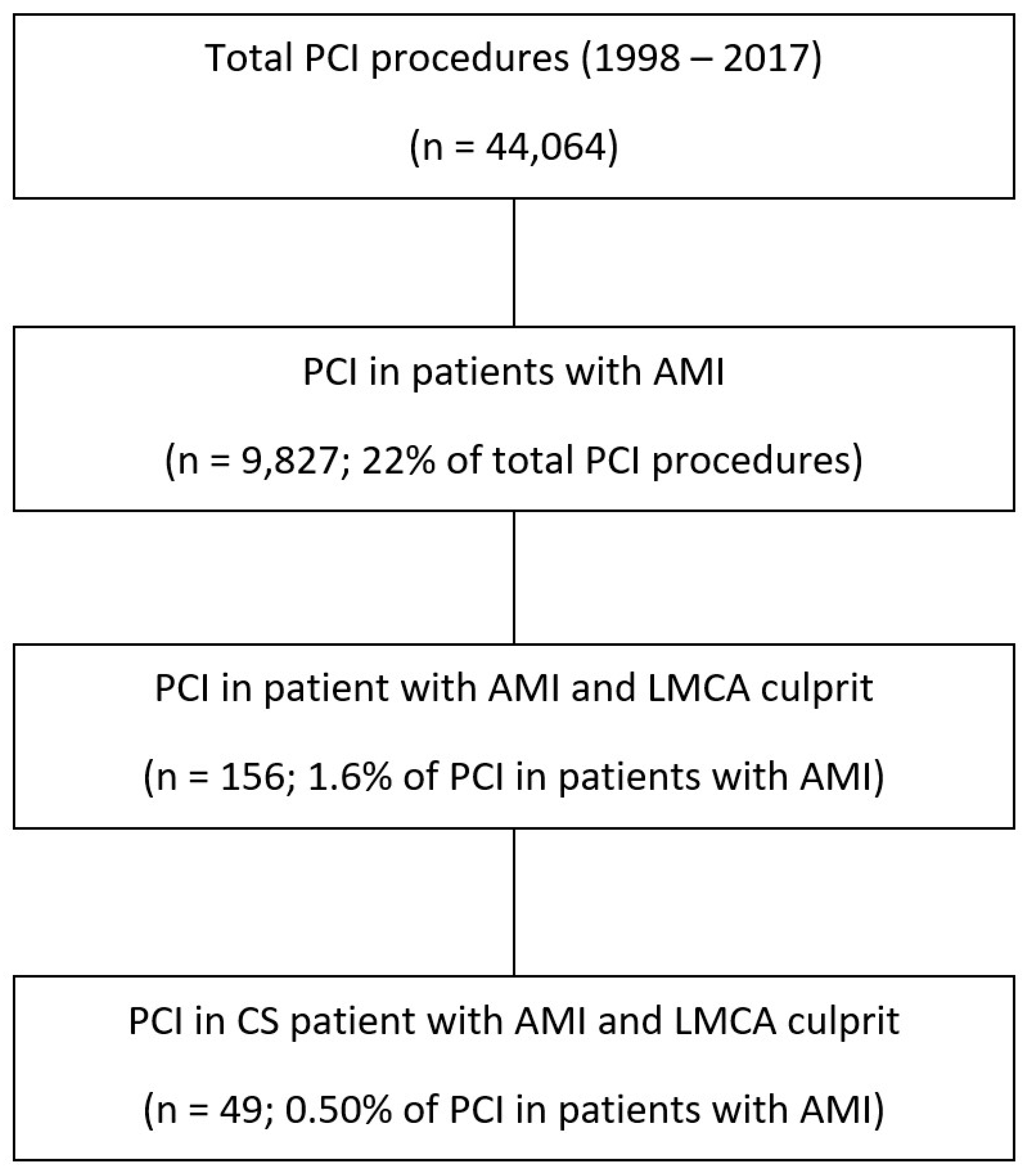
2.1. Study Design and Population
2.2. Data Collection and Definitions
2.3. Clinical Outcomes
2.4. Statistical Analysis
2.5. Ethics
3. Results
Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, N.; De Maria, G.L.; Kassimis, G.; Rahimi, K.; Bennett, D.; Ludman, P.; Banning, A.P. Outcomes after Emergency Percutaneous Coronary Intervention in Patients with Unprotected Left Main Stem Occlusion: The BCIS National Audit of Percutaneous Coronary Intervention 6-Year Experience. JACC Cardiovasc. Interv. 2014, 7, 969–980. [Google Scholar] [CrossRef]
- Pappalardo, A.; Mamas, M.A.; Imola, F.; Ramazzotti, V.; Manzoli, A.; Prati, F.; El-Omar, M. Percutaneous Coronary Intervention of Unprotected Left Main Coronary Artery Disease as Culprit Lesion in Patients with Acute Myocardial Infarction. JACC Cardiovasc. Interv. 2011, 4, 618–626. [Google Scholar] [CrossRef]
- De Luca, G.; Suryapranata, H.; Thomas, K.; van’t Hof, A.W.J.; de Boer, M.J.; Hoorntje, J.C.A.; Zijlstra, F. Outcome in Patients Treated with Primary Angioplasty for Acute Myocardial Infarction Due to Left Main Coronary Artery Occlusion. Am. J. Cardiol. 2003, 91, 235–238. [Google Scholar] [CrossRef]
- Prasad, S.B.; Whitbourn, R.; Malaiapan, Y.; Ahmar, W.; MacIsaac, A.; Meredith, I.T. Primary Percutaneous Coronary Intervention for Acute Myocardial Infarction Caused by Unprotected Left Main Stem Thrombosis. Catheter. Cardiovasc. Interv. 2009, 73, 301–307. [Google Scholar] [CrossRef]
- Tang, H.C.; Wong, A.; Wong, P.; Chua, T.S.J.; Koh, T.H.; Lim, S.T. Clinical Features and Outcome of Emergency Percutaneous Intervention of Left Main Coronary Artery Occlusion in Acute Myocardial Infarction. Singap. Med. J. 2007, 48, 1122–1124. [Google Scholar]
- Sakai, K.; Nakagawa, Y.; Kimura, T.; Ando, K.; Yokoi, H.; Iwabuchi, M.; Inoue, K.; Nosaka, H.; Nobuyoshi, M. Primary Angioplasty of Unprotected Left Main Coronary Artery for Acute Anterolateral Myocardial Infarction. J. Invasive Cardiol. 2004, 16, 621–625. [Google Scholar]
- Qin, Q.; Qian, J.; Fan, B.; Ge, L.; Ge, J. Clinical Outcomes After Percutaneous Coronary Intervention in Acute Myocardial Infarction Due to Unprotected Left Main Coronary Artery Disease. J. Invasive Cardiol. 2015, 27, E153–E157. [Google Scholar]
- Vis, M.M.; Beijk, M.A.; Grundeken, M.J.; Baan, J.; Koch, K.T.; Wykrzykowska, J.J.; Arkenbout, E.K.; Tijssen, J.G.P.; de Winter, R.J.; Piek, J.J.; et al. A Systematic Review and Meta-Analysis on Primary Percutaneous Coronary Intervention of an Unprotected Left Main Coronary Artery Culprit Lesion in the Setting of Acute Myocardial Infarction. JACC Cardiovasc. Interv. 2013, 6, 317–324. [Google Scholar] [CrossRef]
- Chia, P.-L.; Khoo, B.-C.-H.; Ng, C.-K.; Lim, J.-T.-W. Primary Percutaneous Coronary Intervention for Acute Myocardial Infarction Secondary to Acute Left Main Coronary Occlusion in an Institution without On-Site Cardiothoracic Surgical Support. EuroIntervention 2009, 4, 617–619. [Google Scholar] [CrossRef]
- Pedrazzini, G.B.; Radovanovic, D.; Vassalli, G.; Sürder, D.; Moccetti, T.; Eberli, F.; Urban, P.; Windecker, S.; Rickli, H.; Erne, P.; et al. Primary Percutaneous Coronary Intervention for Unprotected Left Main Disease in Patients with Acute ST-Segment Elevation Myocardial Infarction the AMIS (Acute Myocardial Infarction in Switzerland) plus Registry Experience. JACC Cardiovasc. Interv. 2011, 4, 627–633. [Google Scholar] [CrossRef]
- Yip, H.K.; Wu, C.J.; Chen, M.C.; Chang, H.W.; Hsieh, K.Y.; Hang, C.L.; Fu, M. Effect of Primary Angioplasty on Total or Subtotal Left Main Occlusion: Analysis of Incidence, Clinical Features, Outcomes, and Prognostic Determinants. Chest 2001, 120, 1212–1217. [Google Scholar] [CrossRef]
- Valeur, N.; Gaster, A.L.; Saunamäki, K. Percutaneous Revascularization in Acute Myocardial Infarction Due to Left Main Stem Occlusion. Scand Cardiovasc. J. 2005, 39, 24–29. [Google Scholar] [CrossRef]
- Izumikawa, T.; Sakamoto, S.; Takeshita, S.; Takahashi, A.; Saito, S. Outcomes of Primary Percutaneous Coronary Intervention for Acute Myocardial Infarction with Unprotected Left Main Coronary Artery Occlusion. Catheter. Cardiovasc. Interv. 2012, 79, 1111–1116. [Google Scholar] [CrossRef]
- Zeymer, U.; Bueno, H.; Granger, C.B.; Hochman, J.; Huber, K.; Lettino, M.; Price, S.; Schiele, F.; Tubaro, M.; Vranckx, P.; et al. Acute Cardiovascular Care Association Position Statement for the Diagnosis and Treatment of Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock: A Document of the Acute Cardiovascular Care Association of the European Society of Cardiology. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 183–197. [Google Scholar] [CrossRef]
- Steg, P.G.; James, S.K.; Atar, D.; Badano, L.P.; Lundqvist, C.B.; Borger, M.A.; Di Mario, C.; Dickstein, K.; Ducrocq, G.; Fernandez-Aviles, F.; et al. ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation: The Task Force on the Management of ST-Segment Elevation Acute Myocardial Infarction of the European Society of Cardiology (ESC). Eur. Heart J. 2012, 33, 2569–2619. [Google Scholar] [CrossRef]
- Van de Werf, F.; Bax, J.; Betriu, A.; Blomstrom-Lundqvist, C.; Crea, F.; Falk, V.; Filippatos, G.; Fox, K.; Huber, K.; Kastrati, A.; et al. Management of Acute Myocardial Infarction in Patients Presenting with Persistent ST-Segment Elevation: The Task Force on the Management of ST-Segment Elevation Acute Myocardial Infarction of the European Society of Cardiology. Eur. Heart J. 2008, 29, 2909–2945. [Google Scholar] [CrossRef]
- Van de Werf, F.; Ardissino, D.; Betriu, A.; Cokkinos, D.V.; Falk, E.; Fox, K.A.A.; Julian, D.; Lengyel, M.; Neumann, F.-J.; Ruzyllo, W.; et al. Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Eur. Heart J. 2003, 24, 28–66. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Lee, M.S.; Bokhoor, P.; Park, S.-J.; Kim, Y.-H.; Stone, G.W.; Sheiban, I.; Biondi-Zoccai, G.; Sillano, D.; Tobis, J.; Kandzari, D.E. Unprotected Left Main Coronary Disease and ST-Segment Elevation Myocardial Infarction: A Contemporary Review and Argument for Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2010, 3, 791–795. [Google Scholar] [CrossRef]
- Gutiérrez-Barrios, A.; Gheorghe, L.; Camacho-Freire, S.; Valencia-Serrano, F.; Cañadas-Pruaño, D.; Calle-Pérez, G.; Alarcón de la Lastra, I.; Silva, E.; García-Molinero, D.; Agarrado-Luna, A.; et al. Primary Angioplasty in a Catastrophic Presentation: Acute Left Main Coronary Total Occlusion-The ATOLMA Registry. J. Interv. Cardiol. 2020, 2020, 5246504. [Google Scholar] [CrossRef]
- Brueren, B.R.G.; Ernst, J.M.P.G.; Suttorp, M.J.; ten Berg, J.M.; Rensing, B.J.W.M.; Mast, E.G.; Bal, E.T.; Six, A.J.; Plokker, H.W.M. Emergency Percutaneous Coronary Interventions for Unprotected Left Main Stenoses: Immediate and Long Term Follow Up. Heart 2004, 90, 1067–1068. [Google Scholar] [CrossRef]
- Marso, S.P.; Steg, G.; Plokker, T.; Holmes, D.; Park, S.J.; Kosuga, K.; Tamai, H.; Macaya, C.; Moses, J.; White, H.; et al. Catheter-Based Reperfusion of Unprotected Left Main Stenosis during an Acute Myocardial Infarction (the ULTIMA Experience). Unprotected Left Main Trunk Intervention Multi-Center Assessment. Am. J. Cardiol. 1999, 83, 1513–1517. [Google Scholar] [CrossRef] [PubMed]
- Grundeken, M.J.; Vis, M.M.; Beijk, M.A.M.; Kikkert, W.J.; Damman, P.; Kloek, J.J.; Baan, J.; Koch, K.T.; Wykrzykowska, J.J.; Tijssen, J.G.P.; et al. Clinical Outcomes after Percutaneous or Surgical Revascularisation of Unprotected Left Main Coronary Artery-Related Acute Myocardial Infarction: A Single-Centre Experience. Heart 2013, 99, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Puricel, S.; Adorjan, P.; Oberhänsli, M.; Stauffer, J.-C.; Moschovitis, A.; Vogel, R.; Goy, J.-J.; Müller, O.; Eeckhout, E.; Togni, M.; et al. Clinical Outcomes after PCI for Acute Coronary Syndrome in Unprotected Left Main Coronary Artery Disease: Insights from the Swiss Acute Left Main Coronary Vessel Percutaneous Management (SALVage) Study. EuroIntervention 2011, 7, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Hurtado, J.; Pinar Bermúdez, E.; Redondo, B.; Lacunza Ruiz, J.; Gimeno Blanes, J.R.; García de Lara, J.; Valdesuso Aguilar, R.; Teruel, F.; Valdés Chavarri, M. Emergency Percutaneous Coronary Intervention in Unprotected Left Main Coronary Arteries. Predictors of Mortality and Impact of Cardiogenic Shock. Rev. Esp. Cardiol. 2009, 62, 1118–1124. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Sun, H.; Wang, L.-F.; Yang, X.-C.; Li, K.-B.; Zhang, D.-P.; Wang, H.-S.; Li, W.-M. Long-Term Prognosis of Patients with Acute Myocardial Infarction Due to Unprotected Left Main Coronary Artery Disease: A Single-Centre Experience over 14 Years. Singap. Med. J. 2016, 57, 396–400. [Google Scholar] [CrossRef]
- Parma, A.; Fiorilli, R.; DE Felice, F.; Chini, F.; Giorgi Rossi, P.; Borgia, P.; Nazzaro, M.S.; Musto, C.; Guasticchi, G.; Violini, R. Early and Mid-Term Clinical Outcome of Emergency PCI in Patients with STEMI Due to Unprotected Left Main Coronary Artery Disease. J. Interv. Cardiol. 2012, 25, 215–222. [Google Scholar] [CrossRef]
- Liu, H.-W.; Han, Y.-L.; Jin, Q.-M.; Wang, X.-Z.; Ma, Y.-Y.; Wang, G.; Wang, B.; Xu, K.; Li, Y.; Chen, S.-L. One-Year Outcomes in Patients with ST-Segment Elevation Myocardial Infarction Caused by Unprotected Left Main Coronary Artery Occlusion Treated by Primary Percutaneous Coronary Intervention. Chin. Med. J. 2018, 131, 1412–1419. [Google Scholar] [CrossRef]
- Gharacholou, S.M.; Ijioma, N.N.; Lennon, R.J.; Rihal, C.S.; Bell, M.R.; Brenes-Salazar, J.A.; Sandhu, G.S.; Gulati, R.; Pellikka, P.A.; Pollak, P.M.; et al. Characteristics and Long Term Outcomes of Patients with Acute Coronary Syndromes Due to Culprit Left Main Coronary Artery Disease Treated with Percutaneous Coronary Intervention. Am. Heart J. 2018, 199, 156–162. [Google Scholar] [CrossRef]
- Sadowski, M.; Gutkowski, W.; Raczyński, G.; Janion-Sadowska, A.; Gierlotka, M.; Poloński, L. Acute Myocardial Infarction Due to Left Main Coronary Artery Disease in Men and Women: Does ST-Segment Elevation Matter? Arch. Med. Sci. 2015, 11, 1197–1204. [Google Scholar] [CrossRef]
- Yap, J.; Singh, G.D.; Kim, J.-S.; Soni, K.; Chua, K.; Neo, A.; Koh, C.H.; Armstrong, E.J.; Waldo, S.W.; Shunk, K.A.; et al. Outcomes of Primary Percutaneous Coronary Intervention in Acute Myocardial Infarction Due to Unprotected Left Main Thrombosis: The Asia-Pacific Left Main ST-Elevation Registry (ASTER). J. Interv. Cardiol. 2018, 31, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Gagnor, A.; Tomassini, F.; Romagnoli, E.; Montali, N.; Giolitto, S.; Tizzani, E.; Infantino, V.; Varbella, F. Primary Angioplasty in ST-Elevation Myocardial Infarction Due to Unprotected Left-Main Coronary Disease in a High-Volume Catheterization Center without on-Site Surgery Facilities: Immediate and Medium-Term Outcome: The STEMI-Placet Registry. J. Invasive. Cardiol. 2012, 24, 645–649. [Google Scholar]
- Jensen, L.O.; Thayssen, P.; Maeng, M.; Ravkilde, J.; Krusell, L.R.; Raungaard, B.; Junker, A.; Terkelsen, C.J.; Veien, K.T.; Villadsen, A.B.; et al. Randomized Comparison of a Biodegradable Polymer Ultrathin Strut Sirolimus-Eluting Stent With a Biodegradable Polymer Biolimus-Eluting Stent in Patients Treated With Percutaneous Coronary Intervention: The SORT OUT VII Trial. Circ. Cardiovasc. Interv. 2016, 9, e003610. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.Y.; Seo, S.M.; Park, H.-J.; Kim, P.J.; Park, M.W.; Koh, Y.S.; Chang, K.Y.; Jeong, M.H.; Park, S.J.; Seung, K.-B. Clinical Outcomes and Predictors of Unprotected Left Main Stem Culprit Lesions in Patients with Acute ST Segment Elevation Myocardial Infarction. Catheter Cardiovasc. Interv. 2014, 83, E243–E250. [Google Scholar] [CrossRef]
- Almudarra, S.S.; Gale, C.P.; Baxter, P.D.; Fleming, S.J.; Brogan, R.A.; Ludman, P.F.; de Belder, M.A.; Curzen, N.P. National Institute for Cardiovascular Outcomes Research (NICOR) Comparative Outcomes after Unprotected Left Main Stem Percutaneous Coronary Intervention: A National Linked Cohort Study of 5,065 Acute and Elective Cases from the BCIS Registry (British Cardiovascular Intervention Society). JACC Cardiovasc. Interv. 2014, 7, 717–730. [Google Scholar] [CrossRef]
- Ielasi, A.; Silvestro, A.; Personeni, D.; Saino, A.; Angeletti, C.; Costalunga, A.; Tespili, M. Outcomes Following Primary Percutaneous Coronary Intervention for Unprotected Left Main-Related ST-Segment Elevation Myocardial Infarction. J. Cardiovasc. Med. 2015, 16, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Shibata, N.; Umemoto, N.; Tanaka, A.; Takagi, K.; Iwama, M.; Uemura, Y.; Inoue, Y.; Negishi, Y.; Ohashi, T.; Tanaka, M.; et al. Clinical Outcomes Following Emergent Percutaneous Coronary Intervention for Acute Total/Subtotal Occlusion of the Left Main Coronary Artery. Circ. J. 2021, 85, 1789–1796. [Google Scholar] [CrossRef]
- Homorodean, C.; Iancu, A.C.; Leucuţa, D.; Bãlãnescu, Ş.; Dregoesc, I.M.; Spînu, M.; Ober, M.; Tãtaru, D.; Olinic, M.; Bindea, D.; et al. New Predictors of Early and Late Outcomes after Primary Percutaneous Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction and Unprotected Left Main Coronary Artery Culprit Lesion. J. Interv. Cardiol. 2019, 2019, 8238972. [Google Scholar] [CrossRef]
- Yeoh, J.; Andrianopoulos, N.; Reid, C.M.; Yudi, M.B.; Hamilton, G.; Freeman, M.; Noaman, S.; Oqueli, E.; Picardo, S.; Brennan, A.; et al. Long-Term Outcomes Following Percutaneous Coronary Intervention to an Unprotected Left Main Coronary Artery in Cardiogenic Shock. Int. J. Cardiol. 2020, 308, 20–25. [Google Scholar] [CrossRef]
- Galván-Román, F.; Fernández-Herrero, I.; Ariza-Solé, A.; Sánchez-Salado, J.C.; Puerto, E.; Lorente, V.; Gómez-Lara, J.; Martín-Asenjo, R.; Gómez-Hospital, J.A.; Comín-Colet, J. Prognosis of Cardiogenic Shock Secondary to Culprit Left Main Coronary Artery Lesion-Related Myocardial Infarction. ESC Heart Fail 2022, 10, 111–120. [Google Scholar] [CrossRef]
- Tan, C.-H.; Hong, M.-K.; Lee, C.-W.; Kim, Y.-H.; Lee, C.-H.; Park, S.-W.; Park, S.-J. Percutaneous Coronary Intervention with Stenting of Left Main Coronary Artery with Drug-Eluting Stent in the Setting of Acute ST Elevation Myocardial Infarction. Int. J. Cardiol. 2008, 126, 224–228. [Google Scholar] [CrossRef]
- Sjauw, K.D.; Engström, A.E.; Vis, M.M.; van der Schaaf, R.J.; Baan, J.; Koch, K.T.; de Winter, R.J.; Piek, J.J.; Tijssen, J.G.P.; Henriques, J.P.S. A Systematic Review and Meta-Analysis of Intra-Aortic Balloon Pump Therapy in ST-Elevation Myocardial Infarction: Should We Change the Guidelines? Eur. Heart J. 2009, 30, 459–468. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Neumann, F.-J.; Ferenc, M.; Olbrich, H.-G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef]
- Ouweneel, D.M.; Eriksen, E.; Sjauw, K.D.; van Dongen, I.M.; Hirsch, A.; Packer, E.J.S.; Vis, M.M.; Wykrzykowska, J.J.; Koch, K.T.; Baan, J.; et al. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump in Cardiogenic Shock After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2017, 69, 278–287. [Google Scholar] [CrossRef]
- Meraj, P.M.; Doshi, R.; Schreiber, T.; Maini, B.; O’Neill, W.W. Impella 2.5 Initiated Prior to Unprotected Left Main PCI in Acute Myocardial Infarction Complicated by Cardiogenic Shock Improves Early Survival. J. Interv. Cardiol. 2017, 30, 256–263. [Google Scholar] [CrossRef]
- Barone-Rochette, G.; Vanzetto, G.; Fluttaz, A.; Marlière, S.; Bouvaist, H.; Durand, M.; Chavanon, O.; Blin, D.; Machecourt, J. Cardiogenic Shock Due to Unprotected Left Main Coronary Artery Thrombosis in the Era of Mechanical Circulatory Support. Int. J. Cardiol. 2011, 148, 394–396. [Google Scholar] [CrossRef]
- Abu-Assi, E.; Castiñeira-Busto, M.; González-Salvado, V.; Raposeiras-Roubin, S.; Riziq-Yousef Abumuaileq, R.; Peña-Gil, C.; Rigueiro-Veloso, P.; Ocaranza, R.; García-Acuña, J.M.; González-Juanatey, J.R. Coronary Artery Dominance and Long-Term Prognosis in Patients With ST-Segment Elevation Myocardial Infarction Treated With Primary Angioplasty. Rev. Esp. Cardiol. 2016, 69, 19–27. [Google Scholar] [CrossRef]
- Kim, M.C.; Ahn, Y.; Park, K.H.; Sim, D.S.; Yoon, N.S.; Yoon, H.J.; Kim, K.H.; Hong, Y.J.; Park, H.W.; Kim, J.H.; et al. Clinical Outcomes of Low-Dose Aspirin Administration in Patients with Variant Angina Pectoris. Int. J. Cardiol. 2013, 167, 2333–2334. [Google Scholar] [CrossRef]
- Meier, P.; Lansky, A.J.; Fahy, M.; Xu, K.; White, H.D.; Bertrand, M.E.; Mehran, R.; Stone, G.W. The Impact of the Coronary Collateral Circulation on Outcomes in Patients with Acute Coronary Syndromes: Results from the ACUITY Trial. Heart 2014, 100, 647–651. [Google Scholar] [CrossRef]
- Guedeney, P.; Thiele, H.; Kerneis, M.; Barthélémy, O.; Baumann, S.; Sandri, M.; de Waha-Thiele, S.; Fuernau, G.; Rouanet, S.; Piek, J.J.; et al. Radial versus Femoral Artery Access for Percutaneous Coronary Artery Intervention in Patients with Acute Myocardial Infarction and Multivessel Disease Complicated by Cardiogenic Shock: Subanalysis from the CULPRIT-SHOCK Trial. Am. Heart J. 2020, 225, 60–68. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| (n = 49) | |
|---|---|
| Age (years) | 62 ± 11 |
| Male | 42 (86%) |
| BMI (kg/m2) * | 27 ± 4 |
| Risk factors | |
| Diabetes | 6 (12%) |
| Requiring oral medication | 3 (6.1%) |
| Requiring insulin | 1 (2.0%) |
| Unknown | 2 (4.1%) |
| Hypertension | 5 (10%) |
| Hypercholesterolemia | 4 (8.2%) |
| Family history of CAD | 9 (18%) |
| Ever smoker | 13 (27%) |
| History of | |
| Myocardial infarction | 9 (18%) |
| Percutaneous coronary intervention | 3 (6.1%) |
| Presentation | |
| Cardiac arrest prior of during PCI | 26 (53%) |
| Time from symptom-onset to PCI (hours) ** | 2.2 (1.50–3.74) |
| (n = 49) | ||
|---|---|---|
| Femoral access | 46 | (94%) |
| Angiographic characteristics | ||
| Coronary artery dominance | ||
| RCA | 41 | (84%) |
| LCA | 1 | (2.0%) |
| Balanced | 3 | (6.1%) |
| Unknown (RCA not visualized) | 4 | (8.2%) |
| Collaterals arising from the RCA | 4 | (8.2%) |
| Procedural characteristics | ||
| Mechanical support device | 38 | (78%) |
| IABP | 28 | (57%) |
| LVAD (Impella®) | 10 | (20%) |
| Upgrade IABP to LVAD (Impella®) | 8 | (16%) |
| Timing of mechanical support (n = 39) | ||
| Immediately before PCI | 21 | (55%) |
| Directly after PCI | 17 | (45%) |
| Thrombus aspiration performed | 9 | (18%) |
| Concomitant medication | ||
| GP IIb/IIIa inhibitors | 16 | (33%) |
| Inotropics | 46 | (94%) |
| PCI type | ||
| Balloon angioplasty only | 10 | (20%) |
| Stent placement | 39 | (80%) |
| Stent type (n = 39) | ||
| Drug-eluting stent | 16 | (41%) |
| Bare metal stent | 22 | (56%) |
| EPC capturing stent | 1 | (2.3%) |
| Mean stent length (mm) | 17.7 ± 5.6 | |
| Mean stent diameter (mm) | 3.6 ± 0.4 | |
| No. of stents: (n = 39) | ||
| No. of patients treated with one stent | 34 | (87%) |
| No. of patients treated with two stents | 5 | (13%) |
| TIMI flow after intervention | ||
| TIMI 0 | 9 | (18%) |
| TIMI 1 | 1 | (2.0%) |
| TIMI 2 | 13 | (27%) |
| TIMI 3 | 26 | (53%) |
| (n = 49) | ||
|---|---|---|
| Primary outcome | ||
| All-cause mortality at 30 days | 38 | (78%) |
| Secondary endpoints at 30 days | ||
| MACCE | 40 | (82%) |
| AMI | 0 | (0%) |
| Revascularization | ||
| Staged PCI | 1 | (2.0%) |
| Staged CABG | 1 | (2.0%) |
| TLR | 2 | (4.1%) |
| Stroke | 1 | (2.0%) |
| Secondary outcomes at long-term follow-up | ||
| All-cause mortality | 42 | (86%) |
| MACCE | 46 | (94%) |
| AMI | 3 | (6.1%) |
| Revascularization | ||
| Any PCI | 2 | (4.1%) |
| Any CABG | 1 | (2.0%) |
| TLR | 2 | (4.1%) |
| Stroke | 2 | (4.1%) |
| Survivors | ||||
|---|---|---|---|---|
| At 30 Days | p-Value | Long-Term * | p-Value | |
| (n = 11, 22%) | (n = 7, 16%) | |||
| Clinical variables | ||||
| Gender (male vs. female) | 9/42 vs. 2/7 | 0.41 | 5/42 vs. 2/7 | 0.25 |
| Age (years, alive vs. dead) | 56.0 vs. 63.5 | 0.026 | 57.9 vs. 62.5 | 0.16 |
| BMI (kg/m2, alive vs. dead) ** | 27.6 vs. 26.5 | 0.24 | 28.2 vs. 26.5 | 0.17 |
| Smoking | 5/13 vs. 6/36 | 0.084 | 3/13 vs. 4/36 | 0.13 |
| Diabetes mellitus | 1/6 vs. 10/43 | 0.37 | 0/6 vs. 7/43 | 0.14 |
| Hypertension | 1/5 vs. 10/44 | 0.85 | 0/5 vs. 7/44 | 0.44 |
| Dyslipidemia | 1/4 vs. 10/45 | 0.97 | 0/4 vs. 7/45 | 0.55 |
| Family history of CAD | 2/9 vs. 9/40 | 0.91 | 1/9 vs. 6/40 | 0.86 |
| Previous AMI | 2/9 vs. 9/40 | 0.99 | 1/9 vs. 6/40 | 0.77 |
| Cardiac arrest prior or during PCI | 2/26 vs. 9/23 | 0.004 | 1/26 vs. 6/23 | 0.003 |
| Time to puncture *** (hours, alive vs. dead) | 4.4 vs. 3.0 | 0.16 | 4.3 vs. 3.1 | 0.24 |
| Procedural characteristics | ||||
| Vascular access (femoral vs. radial/brachial) | 10/46 vs. 1/3 | 0.56 | 6/46 vs. 1/3 | 0.45 |
| Presence of collaterals arising from the RCA **** | 3/4 vs. 8/41 | 0.059 | 3/4 vs. 4/41 | 0.017 |
| Successful reperfusion | 9/26 vs. 2/23 | 0.026 | 6/26 vs. 1/23 | 0.031 |
| Mechanical assist device used | 10/38 vs. 1/11 | 0.041 | 6/38 vs. 1/11 | 0.073 |
| Thrombus aspiration performed | 3/9 vs. 8/40 | 0.29 | 1/9 vs. 6/40 | 0.58 |
| Balloon only angioplasty | 0/10 vs. 11/39 | 0.027 | 0/10 vs. 7/39 | 0.027 |
| Stent type (BMS vs. DES) | 6/22 vs. 5/16 | 0.89 | 4/22 vs. 3/16 | 0.83 |
| First Author (Ref.#) | Study Period | Sample Size | Study Setting | Follow-Up Period (Mean) | Symptom-Onset to PCI | Treatment | Presenting with Shock | Mechanical Support | 30-Day Mortality | Long Term Mortality |
|---|---|---|---|---|---|---|---|---|---|---|
| Izumikawa et al. [13] | 1988–2009 | 72 | Two centers (TIMI flow 0–3) | 1.7 ± 2.9 years | 2.6 ± 0.7 h | 15% BA, 69% BMS, 15% DES | 46% | 89% IABP, 32% ECLS | 44% (in-hospital) | >50% |
| Sakai et al. [6] | 1990–2001 | 38 | Single center (TIMI flow 0–2) | 1 year | NA | 74% BMS | 74% | 100% IABP | 55% | 58% |
| Brueren et al. [21] | 1990–2001 | 35 | Single center (TIMI flow NA) | 2 (0–5.1) years | 1.7 ± 2.1 h | 71% stenting | NA | 57% IABP | NA | 41% |
| Marso et al. [22] | 1994–1996 | 40 | Multicenter, international registry (TIMI flow 0–3) | 1 year | 1 h (0.5–4.5) | 58% BA, 42% BMS | 92% | 87% IABP | 55% (in-hospital) | 65% |
| Grundeken et al. [23] | 1998–2008 | 84 | Single center (TIMI flow 0–3) | 1 year | 2.2 h (1.5–3.7) | 51% stenting, 35% CABG, 14% BA/suction | 55% | 84% IABP, 16% Impella | 50% | 54% |
| Puricel et al. [24] | 1995–2007 | 65 | Single center (TIMI flow 0–3) | 1 year | NA | 35% BA, 42% BMS, 23% DES | NA | 38% IABP, 11% TandemHeart or Impella | 33% (in-hospital) | ±50% |
| Hurtado et al. [25] | 1999–2007 | 71 | Single center (TIMI flow 0–3) | 2.7 (0.1–7.3) years | NA | 85% stenting, 47% DES | 59% | 54% IABP | 47% (in-hospital) | 75% |
| Xu et al. [26] | 1999–2013 | 55 | Single center (TIMI flow 0–3) | 44.6 ± 31.3 months | 1.8 h ± 0.6 | 11, BA, 82% stenting, 7% no intervention | 55% | 95% IABP | 40% (in-hospital | 69% |
| Parma et al. [27] | 2000–2010 | 58 | Single center (TIMI flow 0–3) | 3 years | 43% within 3 h | 7% BA, 27 BMS, 74% DES | 52% | 52% IABP | 40% | 60% |
| Liu et al. [28] | 2000–2014 | 372 | Two centers (TIMI flow 0–3) | 1 year | 40% < 6 h | 26% thrombolytic therapy, 1% BA, 12 BMS | 8% Cardiac arrest | 21% IABP | 6.2% | 8.1% |
| Gharacholou et al. [29] | 2000–2014 | 40 | Three centers (TIMI flow 0–3) | 5 years | NA | 45% BMS, 55% DES | 43% | 48% IABP, 10% TandemHeart | 33% | 34% |
| Sadowski et al. [30] | 2003–2006 | 643 | Nationwide (Poland) (TIMI flow 0–3) | 1 year | NA | 57% stenting, 32% no intervention, 7% CABG | 16% | 12% IABP | 23% | 31% |
| Yap et al. [31] | 2003–2012 | 67 | Multicenter, international registry (TIMI flow 0–3) | In-hospital | NA | 12% BA, 31% BMS, 55% DES | 66% | 81% IABP, 22% ECMO | 48% (in-hospital) | NA |
| Gagnor et al. [32] | 2004–2009 | 38 | Single center (TIMI flow 0–3) | 504 ± 653 days | 1.3 h ± 0.9 | 3% BA, 37% BMS, 60% DES | 74% | 95% IABP | 42% (in-hospital) | 44% |
| Jensen et al. [33] | 2005–2007 | 71 | Multicenter (Denmark) (TIMI flow 0–3) | 1.5 years | NA | 89% DES | 41% | 13% IABP | 31% | 38% |
| Pappalardo et al. [2] | 2005–2008 | 48 | Two centers (TIMI flow 0–3) | 1 year | NA | 61% DES, 39% BMS | 45% | 54% IABP | 21% (in-hospital) | 29% |
| Baek et al. [34] | 2005–2009 | 61 | Multicenter (Korean registry) (TIMI flow 0–3) | 1 year | 4.6 h ± 9.1 | 95% DES, 5% BMS | 23% | 44% IABP | 21.3% | 23% |
| Almudarra et al. [35] | 2005–2010 | 784 | British Cardiovascular Intervention Society (BCIS) registry (TIMI flow 0–3) | 1 year | NA | 36% BMS, 60% DES | 41% | 39% IABP | 28% | 38% |
| Pedrazzini et al. [10] | 2005–2010 | 348 | 76 centers (TIMI flow NA) | NA | 4.3 h (1.9–10.6) | 78% DES | 12% | 14% | 11% (in-hospital) | NA |
| Qin et al. [7] | 2005–2016 | 30 | Single center (TIMI flow 0–3) | 3 ± 2.2 years | 6.4 ± 5.5 h | 80% DES, 13% BMS, 7% no PTCA | 27% | 30% IABP | 20% (in-hospital) | 20% |
| Ielasi et al. [36] | 2006–2012 | 34 | Single center (TIMI flow 0–3) | 8.5 ± 6.2 months | 1.5 h ± 0.5 | 28% BMS, 18% DES | 65% | 62% IABP | 24% | 24% |
| Shibata et al. [37] | 2006–2017 | 134 | Multicenter registry (TIMI flow 0–2) | In-hospital | NA | 13% BA, 31% BMS, 56% DES | 69% | 96% IABP, 47% VA-ECMO | 55% (in-hospital) | NA |
| Patel et al. [1] | 2007–2012 | 568 | 117 centers (TIMI flow 0–1) | 3 years | 3.3 h (2.2–5.6) | Stenting in almost all patients, 2/3 DES use * | 58% | 53% IABP, 6.1% CPS | 42% (in-hospital) | 74% |
| Homorodean et al. [38] | 2010–2017 | 81 | Two centers (TIMI flow 0–3) | 3 years | 6 h | 59% BMS, 41 DES | 49% | 7% IABP | 36% | 53% |
| Studies with inclusion of either only TIMI flow 0 or 100% cardiogenic shock | ||||||||||
| Current study | 1998–2017 | 49 | Single center (TIMI flow 0) | 9.9 ± 6.2 years | 2.2 h (1.5–3.7) | 20% BA, 45% BMS, 33% DES | 100% | 57% IABP, 20% Impella | 78% | 84% |
| Gutiérrez-Barrios et al. [20] | 2005–2011 | 46 | Two centers (TIMI flow 0) | 1 year | 1.9 h ± 0.9 | 30% BA, 22% BMS, 48% DES | 89% | 44% IABP, 7% VA-ECMO | 59% | 61% |
| Yeoh et al. [39] | 2005–2013 | 45 | Multicenter (TIMI flow NA) | 1 year/up to 9 years | NA | 13% BA, 58% BMS, 29% DES | 100% | 8% IABP | 67% | 73%/80% |
| Galván-Román et al. [40] | 2012–2022 | 70 | Two centers (TIMI flow 0–3) | In-hospital | 3.4 h ± 5.52 | 14% BA, 8% BMS, 77 DES | 100% | 69% IABP, 21% Impella, 27% VA-ECMO | 54% (in-hospital) | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beijk, M.A.M.; Palacios-Rubio, J.; Grundeken, M.J.D.; Kalkman, D.N.; De Winter, R.J. Clinical Outcomes after Percutaneous Coronary Intervention for Cardiogenic Shock Secondary to Total Occlusive Unprotected Left Main Coronary Artery Lesion-Related Acute Myocardial Infarction. J. Clin. Med. 2023, 12, 1311. https://doi.org/10.3390/jcm12041311
Beijk MAM, Palacios-Rubio J, Grundeken MJD, Kalkman DN, De Winter RJ. Clinical Outcomes after Percutaneous Coronary Intervention for Cardiogenic Shock Secondary to Total Occlusive Unprotected Left Main Coronary Artery Lesion-Related Acute Myocardial Infarction. Journal of Clinical Medicine. 2023; 12(4):1311. https://doi.org/10.3390/jcm12041311
Chicago/Turabian StyleBeijk, Marcel A. M., Julián Palacios-Rubio, Maik J. D. Grundeken, Debbie N. Kalkman, and Robbert J. De Winter. 2023. "Clinical Outcomes after Percutaneous Coronary Intervention for Cardiogenic Shock Secondary to Total Occlusive Unprotected Left Main Coronary Artery Lesion-Related Acute Myocardial Infarction" Journal of Clinical Medicine 12, no. 4: 1311. https://doi.org/10.3390/jcm12041311