
Big Endothelin-1 as a Predictor of Reverse Remodeling and Prognosis in Dilated Cardiomyopathy

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Follow-Up
2.3. Laboratory Measurement
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Predictors for LVRR
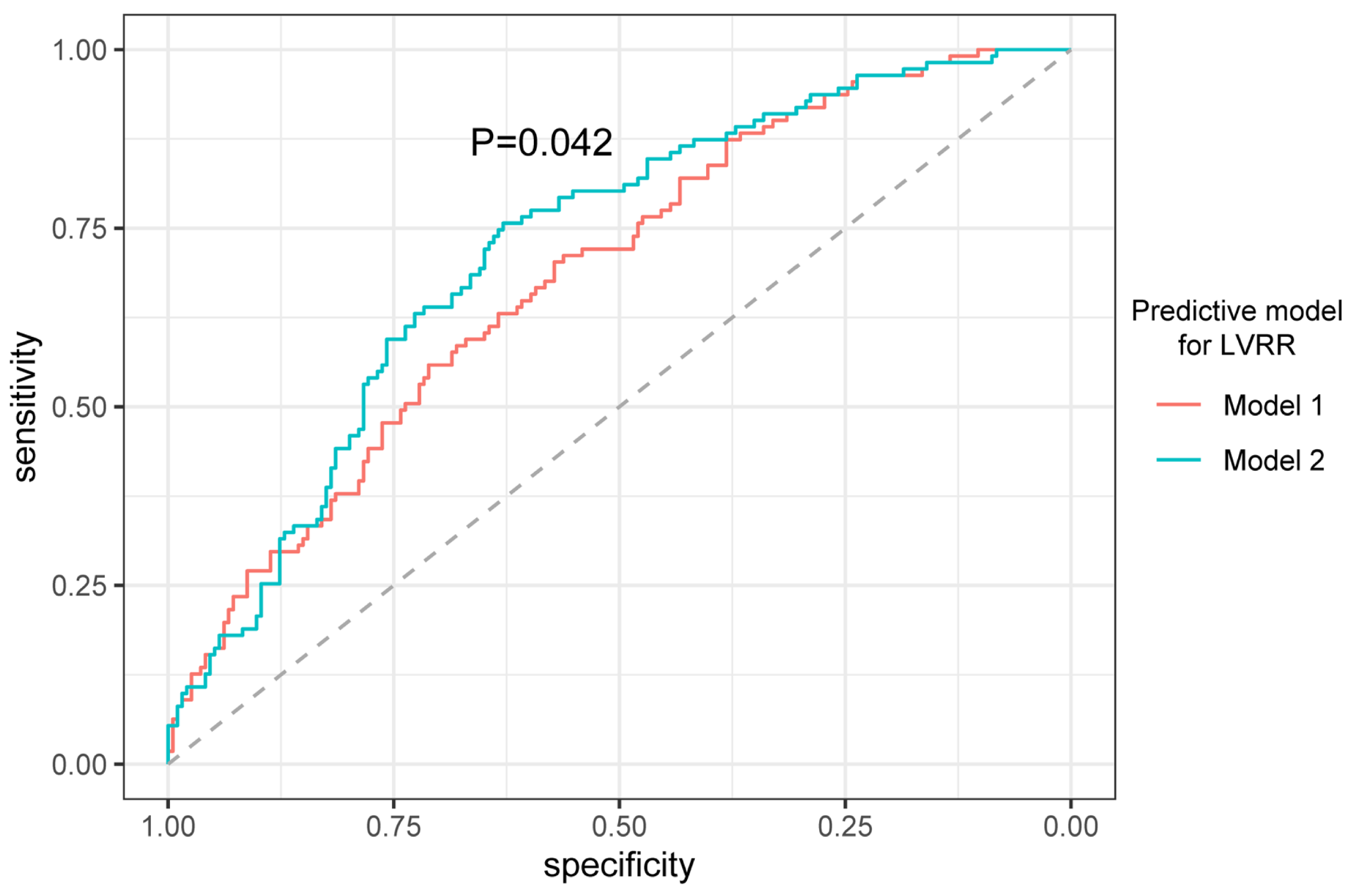
3.3. Predictive Value of Adding Big ET-1 to the Model for LVRR
3.4. The Outcome of Patients with LVRR and Prognostic Role of Big ET-1
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Richardson, P.; McKenna, W.; Bristow, M.; Maisch, B.; Mautner, B.; O’Connell, J.; Olsen, E.; Thiene, G.; Goodwin, J.; Gyarfas, I.; et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation 1996, 93, 841–842. [Google Scholar] [PubMed]
- Kober, L.; Thune, J.J.; Nielsen, J.C.; Haarbo, J.; Videbaek, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Steffensen, F.H.; Bruun, N.E.; et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N. Engl. J. Med. 2016, 375, 1221–1230. [Google Scholar] [CrossRef] [PubMed]
- Verdonschot, J.A.J.; Hazebroek, M.R.; Wang, P.; Sanders-van Wijk, S.; Merken, J.J.; Adriaansen, Y.A.; van den Wijngaard, A.; Krapels, I.P.C.; Brunner-La Rocca, H.-P.; Brunner, H.G.; et al. Clinical Phenotype and Genotype Associations with Improvement in Left Ventricular Function in Dilated Cardiomyopathy. Circ. Heart Fail. 2018, 11, e005220. [Google Scholar] [CrossRef] [PubMed]
- Merlo, M.; Gobbo, M.; Stolfo, D.; Losurdo, P.; Ramani, F.; Barbati, G.; Pivetta, A.; Di Lenarda, A.; Anzini, M.; Gigli, M.; et al. The Prognostic Impact of the Evolution of RV Function in Idiopathic DCM. JACC Cardiovasc. Imaging 2016, 9, 1034–1042. [Google Scholar] [CrossRef]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G.; et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N. Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef]
- Wilcox, J.E.; Fang, J.C.; Margulies, K.B.; Mann, D.L. Heart Failure with Recovered Left Ventricular Ejection Fraction: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2020, 76, 719–734. [Google Scholar] [CrossRef]
- Hemsén, A.; Ahlborg, G.; Ottosson-Seeberger, A.; Lundberg, J.M. Metabolism of Big endothelin-1 (1-38) and (22-38) in the human circulation in relation to production of endothelin-1 (1-21). Regul. Pept. 1995, 55, 287–297. [Google Scholar] [CrossRef]
- Leask, A. Getting to the heart of the matter: New insights into cardiac fibrosis. Circ. Res. 2015, 116, 1269–1276. [Google Scholar] [CrossRef]
- Yanagisawa, M.; Kurihara, H.; Kimura, S.; Tomobe, Y.; Kobayashi, M.; Mitsui, Y.; Yazaki, Y.; Goto, K.; Masaki, T. A novel potent vasoconstrictor peptide produced by vascular endothelial cells. Nature 1988, 332, 411–415. [Google Scholar] [CrossRef]
- Zhang, C.L.; Xie, S.; Qiao, X.; An, Y.M.; Zhang, Y.; Li, L.; Guo, X.B.; Zhang, F.C.; Wu, L.L. Plasma endothelin-1-related peptides as the prognostic biomarkers for heart failure: A PRISMA-compliant meta-analysis. Medicine 2017, 96, e9342. [Google Scholar] [CrossRef]
- Wu, S.; Yang, Y.M.; Zhu, J.; Ren, J.M.; Wang, J.; Zhang, H.; Shao, X.H. The association between plasma big endothelin-1 levels at admission and long-term outcomes in patients with atrial fibrillation. Atherosclerosis 2018, 272, 1–7. [Google Scholar] [CrossRef]
- Fan, P.; Zhang, Y.; Lu, Y.T.; Yang, K.Q.; Lu, P.P.; Zhang, Q.Y.; Luo, F.; Lin, Y.H.; Zhou, X.L.; Tian, T. Prognostic value of plasma big endothelin-1 in left ventricular non-compaction cardiomyopathy. Heart 2021, 107, 836–841. [Google Scholar] [CrossRef]
- Wang, Y.; Tang, Y.; Zou, Y.; Wang, D.; Zhu, L.; Tian, T.; Wang, J.; Bao, J.; Hui, R.; Kang, L.; et al. Plasma level of big endothelin-1 predicts the prognosis in patients with hypertrophic cardiomyopathy. Int. J. Cardiol. 2017, 243, 283–289. [Google Scholar] [CrossRef]
- Kim, G.H.; Uriel, N.; Burkhoff, D. Reverse remodelling and myocardial recovery in heart failure. Nat. Rev. Cardiol. 2018, 15, 83–96. [Google Scholar] [CrossRef]
- Tseliou, E.; Lavine, K.J.; Wever-Pinzon, O.; Topkara, V.K.; Meyns, B.; Adachi, I.; Zimpfer, D.; Birks, E.J.; Burkhoff, D.; Drakos, S.G. Biology of myocardial recovery in advanced heart failure with long-term mechanical support. J. Heart Lung Transplant. 2022, 41, 1309–1323. [Google Scholar] [CrossRef]
- Aimo, A.; Gaggin, H.K.; Barison, A.; Emdin, M.; Januzzi, J.L., Jr. Imaging, Biomarker, and Clinical Predictors of Cardiac Remodeling in Heart Failure with Reduced Ejection Fraction. JACC Heart Fail. 2019, 7, 782–794. [Google Scholar] [CrossRef]
- Aimo, A.; Vergaro, G.; Gonzalez, A.; Barison, A.; Lupon, J.; Delgado, V.; Richards, A.M.; de Boer, R.A.; Thum, T.; Arfsten, H.; et al. Cardiac remodelling—Part 2: Clinical, imaging and laboratory findings. A review from the Study Group on Biomarkers of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2022, 24, 944–958. [Google Scholar] [CrossRef]
- Kramer, D.G.; Trikalinos, T.A.; Kent, D.M.; Antonopoulos, G.V.; Konstam, M.A.; Udelson, J.E. Quantitative evaluation of drug or device effects on ventricular remodeling as predictors of therapeutic effects on mortality in patients with heart failure and reduced ejection fraction: A meta-analytic approach. J. Am. Coll. Cardiol. 2010, 56, 392–406. [Google Scholar] [CrossRef]
- Gaggin, H.K.; Szymonifka, J.; Bhardwaj, A.; Belcher, A.; De Berardinis, B.; Motiwala, S.; Wang, T.J.; Januzzi, J.L., Jr. Head-to-head comparison of serial soluble ST2, growth differentiation factor-15, and highly-sensitive troponin T measurements in patients with chronic heart failure. JACC Heart Fail. 2014, 2, 65–72. [Google Scholar] [CrossRef]
- Lupon, J.; Gaggin, H.K.; de Antonio, M.; Domingo, M.; Galan, A.; Zamora, E.; Vila, J.; Penafiel, J.; Urrutia, A.; Ferrer, E.; et al. Biomarker-assist score for reverse remodeling prediction in heart failure: The ST2-R2 score. Int. J. Cardiol. 2015, 184, 337–343. [Google Scholar] [CrossRef]
- Daubert, M.A.; Adams, K.; Yow, E.; Barnhart, H.X.; Douglas, P.S.; Rimmer, S.; Norris, C.; Cooper, L.; Leifer, E.; Desvigne-Nickens, P.; et al. NT-proBNP Goal Achievement Is Associated with Significant Reverse Remodeling and Improved Clinical Outcomes in HFrEF. JACC Heart Fail. 2019, 7, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Mayourian, J.; Ceholski, D.K.; Gonzalez, D.M.; Cashman, T.J.; Sahoo, S.; Hajjar, R.J.; Costa, K.D. Physiologic, Pathologic, and Therapeutic Paracrine Modulation of Cardiac Excitation-Contraction Coupling. Circ. Res. 2018, 122, 167–183. [Google Scholar] [CrossRef]
- Liu, J.; Zhuang, T.; Pi, J.; Chen, X.; Zhang, Q.; Li, Y.; Wang, H.; Shen, Y.; Tomlinson, B.; Chan, P.; et al. Endothelial Forkhead Box Transcription Factor P1 Regulates Pathological Cardiac Remodeling Through Transforming Growth Factor-beta1-Endothelin-1 Signal Pathway. Circulation 2019, 140, 665–680. [Google Scholar] [CrossRef] [PubMed]
- Van Beneden, R.; Gurne, O.; Selvais, P.L.; Ahn, S.A.; Robert, A.R.; Ketelslegers, J.M.; Pouleur, H.G.; Rousseau, M.F. Superiority of big endothelin-1 and endothelin-1 over natriuretic peptides in predicting survival in severe congestive heart failure: A 7-year follow-up study. J. Card. Fail. 2004, 10, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Masson, S.; Latini, R.; Anand, I.S.; Barlera, S.; Judd, D.; Salio, M.; Perticone, F.; Perini, G.; Tognoni, G.; Cohn, J.N.; et al. The prognostic value of big endothelin-1 in more than 2300 patients with heart failure enrolled in the Valsartan Heart Failure Trial (Val-HeFT). J. Card. Fail. 2006, 12, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Olivier, A.; Girerd, N.; Michel, J.B.; Ketelslegers, J.M.; Fay, R.; Vincent, J.; Bramlage, P.; Pitt, B.; Zannad, F.; Rossignol, P.; et al. Combined baseline and one-month changes in big endothelin-1 and brain natriuretic peptide plasma concentrations predict clinical outcomes in patients with left ventricular dysfunction after acute myocardial infarction: Insights from the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) study. Int. J. Cardiol. 2017, 241, 344–350. [Google Scholar] [CrossRef]
- Leary, P.J.; Jenny, N.S.; Bluemke, D.A.; Kawut, S.M.; Kronmal, R.A.; Lima, J.A.; Maron, B.A.; Ralph, D.D.; Rayner, S.G.; Ryan, J.J.; et al. Endothelin-1, cardiac morphology, and heart failure: The MESA angiogenesis study. J. Heart Lung Transplant. 2020, 39, 45–52. [Google Scholar] [CrossRef]
- Hathaway, C.K.; Grant, R.; Hagaman, J.R.; Hiller, S.; Li, F.; Xu, L.; Chang, A.S.; Madden, V.J.; Bagnell, C.R.; Rojas, M.; et al. Endothelin-1 critically influences cardiac function via superoxide-MMP9 cascade. Proc. Natl. Acad. Sci. USA 2015, 112, 5141–5146. [Google Scholar] [CrossRef]
- Shen, M.T.; Li, Y.; Guo, Y.K.; Jiang, L.; Gao, Y.; Shi, R.; Yang, Z.G. Impact of type 2 diabetes mellitus on left ventricular deformation in non-ischemic dilated cardiomyopathy patients assessed by cardiac magnetic resonance imaging. Cardiovasc. Diabetol. 2022, 21, 94. [Google Scholar] [CrossRef]
- Zhang, N.; Wang, Y.; Tse, G.; Korantzopoulos, P.; Letsas, K.P.; Zhang, Q.; Li, G.; Lip, G.Y.H.; Liu, T. Effect of sodium-glucose cotransporter-2 inhibitors on cardiac remodelling: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2021, 28, 1961–1973. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Overall | LVRR Absent | LVRR Present | p-Value | |
|---|---|---|---|---|
| N | 375 | 240 | 135 | |
| Clinical characteristics | ||||
| Age(years) | 47 [34, 57] | 48 [35, 58] | 44 [32, 55] | 0.073 |
| Female (%) | 79 (21.1) | 52 (21.7) | 27 (20.0) | 0.804 |
| Heart rate (b.p.m) | 84 [72, 96] | 82 [70, 94] | 85 [77, 98] | 0.023 |
| SBP (mmHg) | 113 [102, 124] | 110 [100, 121] | 116 [105, 130] | 0.001 |
| DBP (mmHg) | 72 [66, 80] | 70 [65, 80] | 76 [70, 85] | <0.001 |
| BMI (kg/m2) | 24.8 [22.1, 28.1] | 24.5 [21.7, 27.3] | 26.0 [23.2, 29.2] | 0.002 |
| T2DM (%) | 66 (17.6) | 51 (21.2) | 15 (11.1) | 0.020 |
| Hypertension (%) | 124 (33.1) | 64 (26.7) | 60 (44.4) | 0.001 |
| NYHA Class III/IV (%) | 297 (79.2) | 196 (81.7) | 101 (74.8) | 0.151 |
| Smoking (%) | 123 (49.4) | 81 (51.6) | 42 (45.7) | 0.439 |
| Length of stay (days) | 10 [8, 13] | 11 [8, 14] | 10 [8, 13] | 0.153 |
| Electrocardiography | ||||
| QRS duration (ms) | 107 [95, 126] | 110 [98, 128] | 101 [92, 115.2] | 0.001 |
| PR interval (ms) | 174 [160, 192] | 174 [158, 192] | 176 [161, 190] | 0.913 |
| QTc interval (ms) | 457 [430, 486] | 457 [431, 486] | 456 [427, 478] | 0.298 |
| AF (%) | 87 (23.2) | 60 (25.0) | 27 (20.0) | 0.330 |
| LBBB (%) | 36 (9.6) | 26 (10.8) | 10 (7.4) | 0.369 |
| NSVT (%) | 88 (23.5) | 66 (27.5) | 22 (16.3) | 0.020 |
| Laboratory Test | ||||
| Hemoglobin (g/L) | 150.0 [137.2, 162.0] | 148.0 [137.0, 159.0] | 153.0 [139.5, 167.0] | 0.010 |
| WBC (109/L) | 7.4 [6.2, 8.9] | 7.2 [6.2, 8.9] | 7.6 [6.3, 9.1] | 0.330 |
| K (mmol/L) | 4.0 [3.7, 4.2] | 4.0 [3.7, 4.2] | 4.0 [3.7, 4.2] | 0.996 |
| Na (mmol/L) | 138.0 [135.4, 140.0] | 137.3 [134.9, 139.9] | 139.0 [136.4, 140.9] | 0.001 |
| FBG (mmol/L) | 5.1 [4.6, 5.7] | 5.1 [4.6, 5.8] | 5.0 [4.6, 5.5] | 0.299 |
| Hemoglobin A1C (%) | 6.1 [5.6, 6.7] | 6.2 [5.7, 6.9] | 6.0 [5.6, 6.5] | 0.039 |
| LDL-C (mmol/L) | 2.7 [2.1, 3.4] | 2.6 [2.0, 3.3] | 2.9 [2.2, 3.4] | 0.028 |
| Scr (umol/L) | 89.4 [75.5, 106.2] | 89.4 [75.6, 103.8] | 89.4 [75.5, 108.0] | 0.974 |
| Big ET-1 (pmol/L) | 0.72 [0.41, 1.02] | 0.77 [0.52, 1.08] | 0.61 [0.30, 0.94] | <0.001 |
| NT-Pro BNP (pg/mL) | 1922.9 [897.4, 4021.5] | 2041.9 [1078.5, 4297.5] | 1570.0 [745.3, 3265.0] | 0.009 |
| Echocardiography | ||||
| LAD (mm) | 45 [41, 50] | 46 [41, 51] | 44 [40, 48] | 0.002 |
| LVEDD (mm) | 68 [63, 74] | 69 [63, 75] | 66 [62, 72] | 0.021 |
| LVEF (%) | 29 [24, 35] | 28 [24, 35] | 30 [25, 34] | 0.236 |
| RVD (mm) | 25 [22, 28] | 25 [22, 29] | 24 [22, 28] | 0.199 |
| Therapy | ||||
| Digoxin (%) | 324 (86.4) | 208 (86.7) | 116 (85.9) | 0.965 |
| ACEI/ARB (%) | 305 (81.3) | 184 (76.7) | 121 (89.6) | 0.003 |
| β-blocker (%) | 366 (97.6) | 232 (96.7) | 134 (99.3) | 0.221 |
| MRA (%) | 364 (97.1) | 231 (96.2) | 133 (98.5) | 0.352 |
| Diuretics (%) | 307 (81.9) | 197 (82.1) | 110 (81.5) | 0.996 |
| Univariable Logistic Regression | Multivariable Logistic Regression | |||
|---|---|---|---|---|
| Characteristics | Crude OR (95%CI) | p-Value | Adjusted OR (95%CI) | p-Value |
| Age | 0.99 (0.97–1.01) | 0.098 | ||
| Gender | 0.9 (0.54–1.52) | 0.704 | ||
| BMI | 1.07 (1.03–1.12) | 0.003 | 1.07 (1.01–1.14) | 0.026 |
| NYHA III/IV | 0.67 (0.4–1.11) | 0.118 | ||
| SBP | 1.03 (1.01–1.04) | <0.001 | 1.02 (1.01–1.04) | 0.035 |
| T2DM | 0.46 (0.25–0.86) | 0.015 | 0.30 (0.14–0.65) | 0.002 |
| AF | 0.75 (0.45–1.25) | 0.272 | ||
| QRS duration | 0.90 (0.82–0.98) | 0.015 | 0.92 (0.84–1.02) | 0.124 |
| LBBB | 0.66 (0.31–1.41) | 0.282 | ||
| LVEF | 1.01 (0.99–1.04) | 0.325 | ||
| LVEDD | 0.97 (0.95–1.01) | 0.024 | 0.98 (0.95–1.01) | 0.167 |
| RVD | 0.97 (0.93–1.01) | 0.147 | ||
| Hemoglobin | 1.02 (1.01–1.03) | 0.009 | ||
| log Big ET-1 | 0.67 (0.55–0.83) | <0.001 | 0.70 (0.55–0.89) | 0.003 |
| log NT-Pro-BNP | 0.84 (0.74–0.96) | 0.012 | ||
| log Scr | 0.76 (0.45–1.29) | 0.304 | ||
| ACEI/ARB | 2.63 (1.40–4.93) | 0.003 | 2.30 (1.02–5.21) | 0.045 |
| β-blocker | 4.62 (0.57–37.35) | 0.151 | ||
| MRA | 2.59 (0.55–12.17) | 0.228 | ||
| Model 1 (Basic Model) | Model 2 (Basic Model + Big ET-1) | p-Value | |
|---|---|---|---|
| AUC | 0.684 (0.624–0.744) | 0.721 (0.663–0.779) | 0.042 |
| IDI | reference | 0.033 (0.012,0.054) | 0.002 |
| cNRI | reference | 0.354 (0.1253–0.583) | 0.002 |
| Crude HR (95%CI) | Crude p Value | Adjusted HR (95% CI) | Adjusted p Value | |
|---|---|---|---|---|
| Age | 1.01 (1.00,1.03) | 0.066 | 1.03 (1.01,1.04) | <0.001 |
| SBP | 0.96 (0.95,0.98) | <0.001 | 0.97 (0.95,0.99) | <0.001 |
| LVEDD | 1.06 (1.04,1.09) | <0.001 | 1.06 (1.03,1.09) | <0.001 |
| log Big ET-1 | 1.49 (1.20,1.85) | <0.001 | 1.45 (1.13,1.85) | 0.003 |
| log NT-Pro-BNP | 1.55 (1.33,1.80) | <0.001 | 1.29 (1.08,1.54) | 0.005 |
| Use of ACEI/ARB | 0.40 (0.25,0.64) | <0.001 | 0.52 (0.32,0.86) | 0.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, J.; Liang, L.; Chen, Y.; Tian, P.; Zhao, X.; Huang, B.; Wu, Y.; Wang, J.; Guan, J.; Huang, L.; et al. Big Endothelin-1 as a Predictor of Reverse Remodeling and Prognosis in Dilated Cardiomyopathy. J. Clin. Med. 2023, 12, 1363. https://doi.org/10.3390/jcm12041363
Feng J, Liang L, Chen Y, Tian P, Zhao X, Huang B, Wu Y, Wang J, Guan J, Huang L, et al. Big Endothelin-1 as a Predictor of Reverse Remodeling and Prognosis in Dilated Cardiomyopathy. Journal of Clinical Medicine. 2023; 12(4):1363. https://doi.org/10.3390/jcm12041363
Chicago/Turabian StyleFeng, Jiayu, Lin Liang, Yuyi Chen, Pengchao Tian, Xuemei Zhao, Boping Huang, Yihang Wu, Jing Wang, Jingyuan Guan, Liyan Huang, and et al. 2023. "Big Endothelin-1 as a Predictor of Reverse Remodeling and Prognosis in Dilated Cardiomyopathy" Journal of Clinical Medicine 12, no. 4: 1363. https://doi.org/10.3390/jcm12041363
APA StyleFeng, J., Liang, L., Chen, Y., Tian, P., Zhao, X., Huang, B., Wu, Y., Wang, J., Guan, J., Huang, L., Li, X., Zhang, Y., & Zhang, J. (2023). Big Endothelin-1 as a Predictor of Reverse Remodeling and Prognosis in Dilated Cardiomyopathy. Journal of Clinical Medicine, 12(4), 1363. https://doi.org/10.3390/jcm12041363