
A Retrospective Medical Record Review of Adults with Non-Cancer Diagnoses Prescribed Medicinal Cannabis
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Setting, and Population
2.2. Characteristics Retrieved
2.3. Evaluation of Effectiveness
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Included Patients
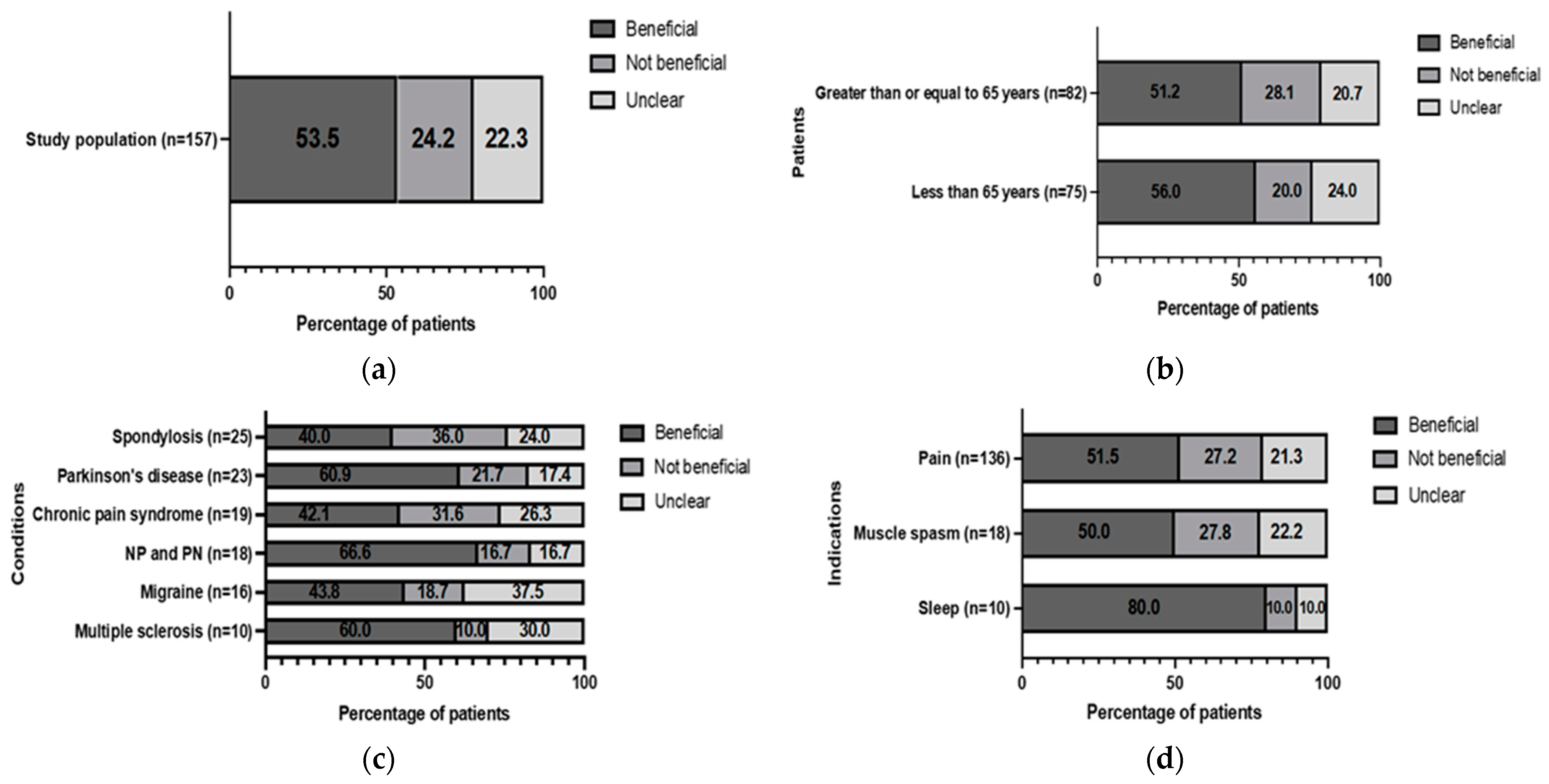
3.2. Effectiveness of Treatment—Patient-Perceived Benefit
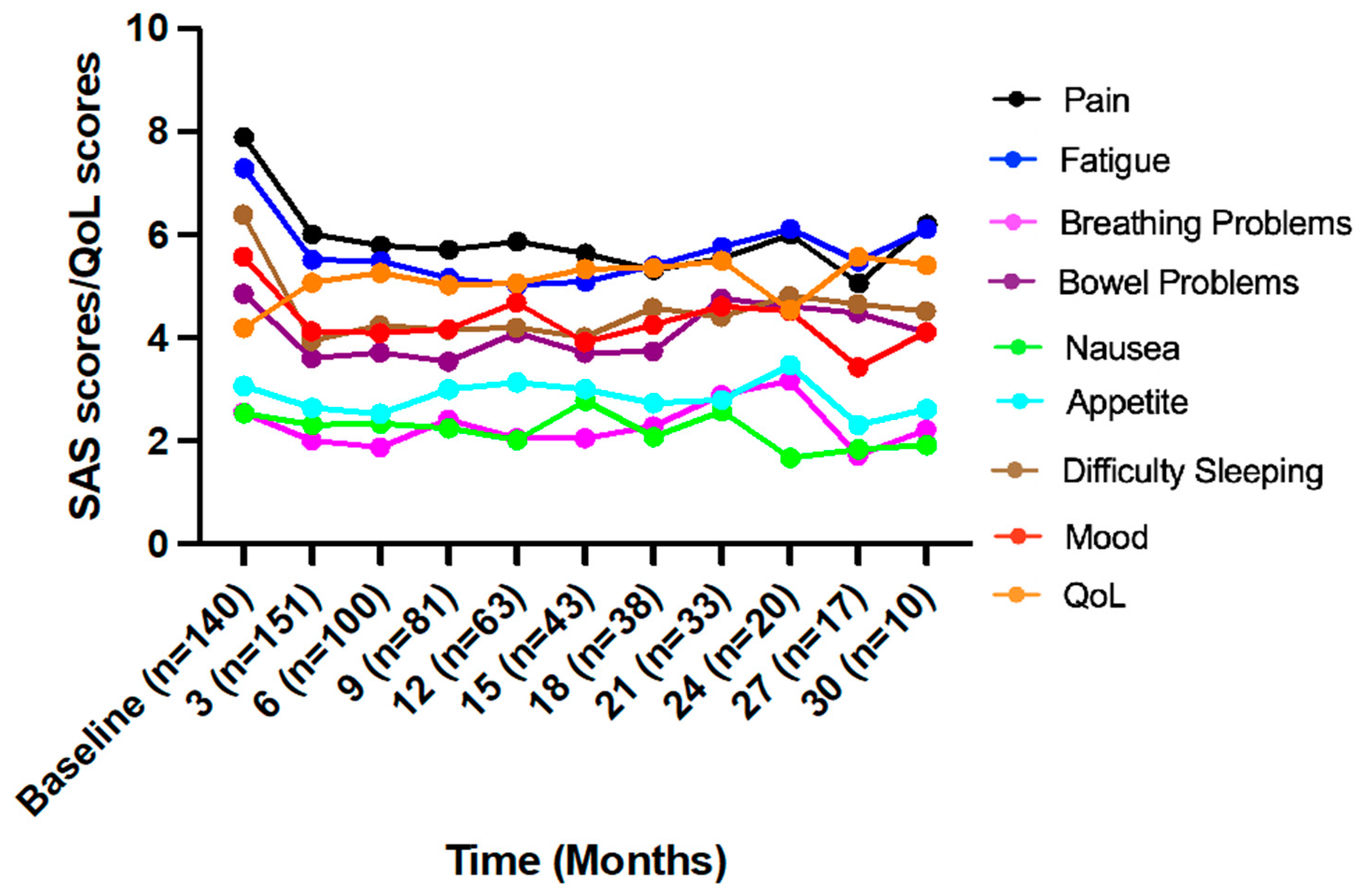
3.3. Effectiveness of Treatment—Overall Symptom Assessment Scale Scores
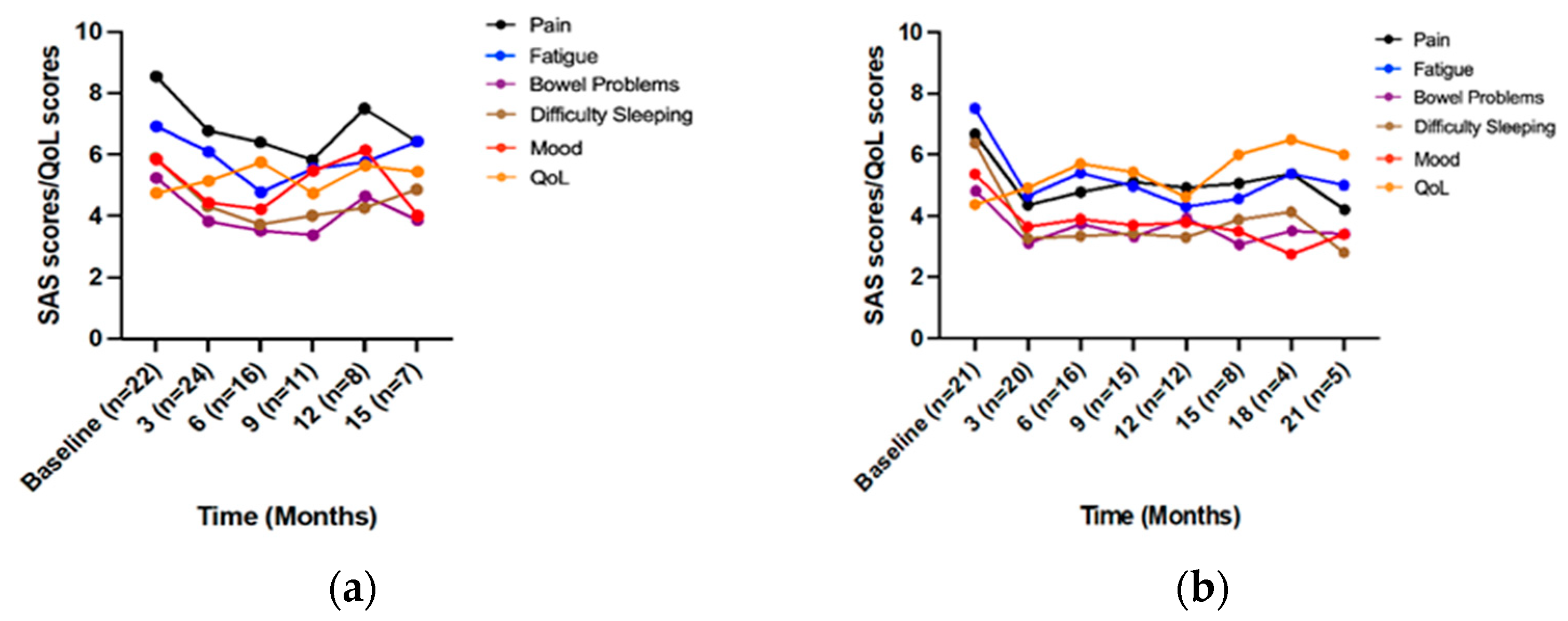
3.4. Conditions
3.4.1. Spondylosis
3.4.2. Parkinson’s Disease
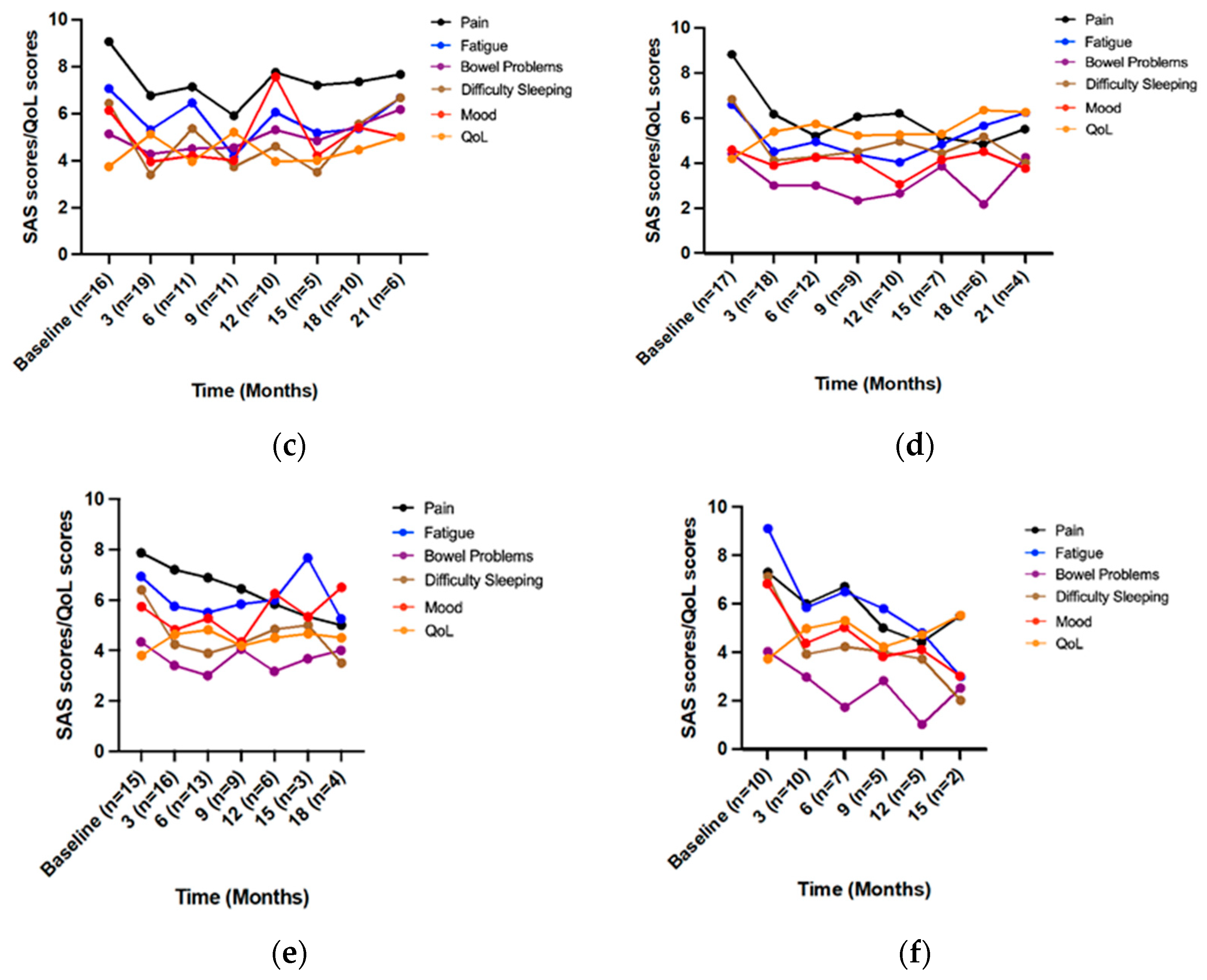
3.4.3. Chronic Pain Syndrome
3.4.4. Neuropathic Pain and Peripheral Neuropathy
3.4.5. Migraine
3.4.6. Multiple Sclerosis
3.5. Indications
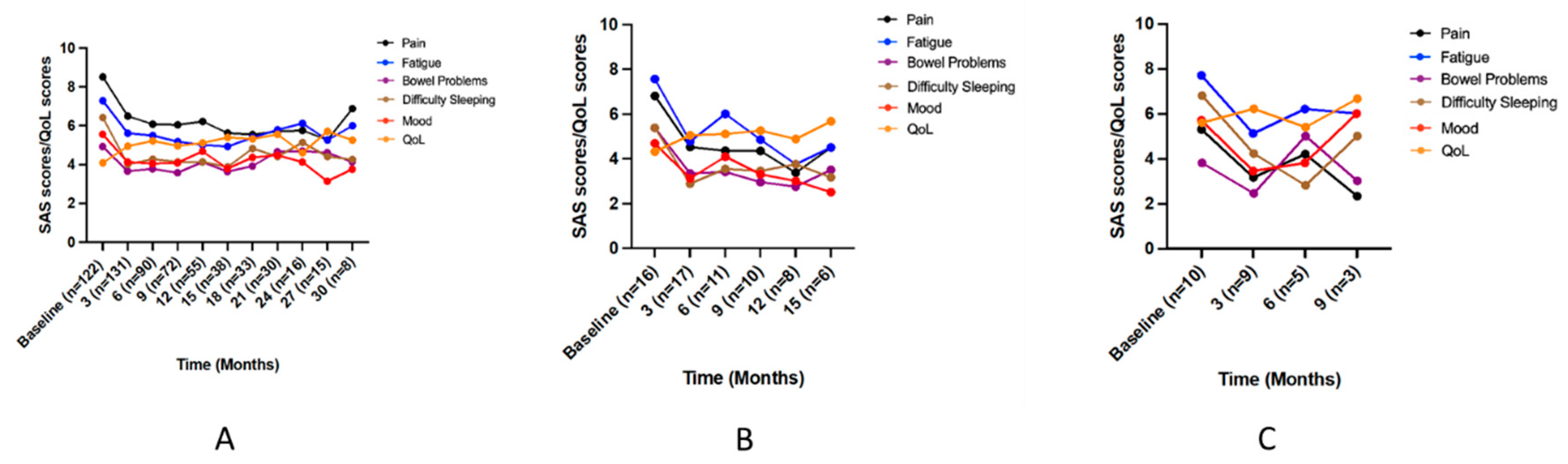
3.5.1. Pain
3.5.2. Muscle Spasm
3.5.3. Sleep
3.6. Safety and Treatment Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pisanti, S.; Bifulco, M. Medical Cannabis: A plurimillennial history of an evergreen. J. Cell Physiol. 2019, 234, 8342–8351. [Google Scholar] [CrossRef] [PubMed]
- Bridgeman, M.B.; Abazia, D.T. Medicinal cannabis: History, pharmacology, and implications for the acute care setting. P T A Peer-Rev. J. Formul. Manag. 2017, 42, 180–188. [Google Scholar]
- Baron, E.P. Comprehensive review of medicinal marijuana, cannabinoids, and therapeutic implications in medicine and headache: What a long strange trip it’s been. Headache J. Head Face Pain 2015, 55, 885–916. [Google Scholar] [CrossRef]
- Arnold, J.C.; Nation, T.; McGregor, I.S. Prescribing medicinal cannabis. Aust. Prescr. 2020, 43, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Inglet, S.; Winter, B.; Yost, S.E.; Entringer, S.; Lian, A.; Biksacky, M.; Pitt, R.D.; Mortensen, W. Clinical data for the use of cannabis-based treatments: A comprehensive review of the literature. Ann. Pharmacother. 2020, 54, 1109–1143. [Google Scholar] [CrossRef] [PubMed]
- Savage, S.R.; Romero-Sandoval, A.; Schatman, M.; Wallace, M.; Fanciullo, G.; McCarberg, B.; Ware, M. Cannabis in pain treatment: Clinical and research considerations. J. Pain 2016, 17, 654–668. [Google Scholar] [CrossRef]
- Australian Government Department of Health and Aged Care, Therapeutics Goods Administration. Accessing Medicinal Cannabis for a Patient. 16 November 2021. Available online: https://www.tga.gov.au/accessing-medicinal-cannabis-patient (accessed on 26 January 2023).
- Australian Government Department of Health and Aged Care, Therapeutics Goods Administration. Medicinal Cannabis Special Access Scheme Category B Data. 19 August 2021. Available online: https://www.tga.gov.au/products/unapproved-therapeutic-goods/medicinal-cannabis-hub/medicinal-cannabis-access-pathways-and-patient-access-data/medicinal-cannabis-special-access-scheme-category-b-data (accessed on 26 January 2023).
- Australian Government Department of Health and Aged Care, Therapeutics Goods Administration. Medicinal Cannabis Authorised Prescriber Scheme Data. Available online: https://www.tga.gov.au/products/unapproved-therapeutic-goods/medicinal-cannabis-hub/medicinal-cannabis-access-pathways-and-patient-access-data/medicinal-cannabis-authorised-prescriber-scheme-data (accessed on 26 January 2023).
- Ministers, Australian Government Department of Health and Aged Care. $3 Million for Research into Medicinal Cannabis Benefits. Available online: https://www.health.gov.au/ministers/the-hon-greg-hunt-mp/media/3-million-for-research-into-medicinal-cannabis-benefits#:~:text=The%20Australian%20Government%20is%20investing,effect%20management%20for%20cancer%20patients (accessed on 26 January 2023).
- National Academies of Sciences EaM. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research; The National Academies Press: Washington, DC, USA, 2017. [Google Scholar]
- Daveson, B.A.; Allingham, S.F.; Clapham, S.; Johnson, C.E.; Currow, D.C.; Yates, P.; Eagar, K. The PCOC Symptom Assessment Scale (SAS): A valid measure for daily use at point of care and in palliative care programs. PLoS ONE 2021, 16, e0247250. [Google Scholar] [CrossRef]
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and how should multiple imputation be used for handling missing data in randomized clinical trials—A practical guide with flowcharts. BMC Med. Res. Methodol. 2017, 17, 162. [Google Scholar] [CrossRef]
- Safakish, R.; Ko, G.; Salimpour, V.; Hendin, B.; Sohanpal, I.; Loheswaran, G.; Yoon SY, R. Medical Cannabis for the Management of Pain and Quality of Life in Chronic Pain Patients: A Prospective Observational Study. Pain Med. 2020, 21, 3073–3086. [Google Scholar] [CrossRef]
- Aviram, J.; Pud, D.; Gershoni, T.; Schiff-Keren, B.; Ogintz, M.; Vulfsons, S.; Yashar, T.; Adahan, H.-M.; Brill, S.; Amital, H.; et al. Medical cannabis treatment for chronic pain: Outcomes and prediction of response. Eur. J. Pain 2021, 25, 359–374. [Google Scholar] [CrossRef]
- Meng, H.; Page, M.G.; Ajrawat, P.; Deshpande, A.; Samman, B.; Dominicis, M.; Ladha, K.S.; Fiorellino, J.; Huang, A.; Kotteeswaran, Y.; et al. Patient-reported outcomes in those consuming medical cannabis: A prospective longitudinal observational study in chronic pain patients. Can. J. Anesth. 2021, 68, 633–644. [Google Scholar] [CrossRef]
- Baron, E.P. Medicinal properties of cannabinoids, terpenes, and flavonoids in cannabis, and benefits in migraine, headache, and pain: An update on current evidence and cannabis science. Headache 2018, 58, 1139–1186. [Google Scholar] [CrossRef]
- Cahill, S.P.; Lunn, S.E.; Diaz, P.; Page, J.E. Evaluation of patient reported safety and efficacy of cannabis from a survey of medical cannabis patients in Canada. Front. Public Health 2021, 9, 626853. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Kaufmann, C.N.; Ko, R.; Li, Z.; Han, B.H. Patterns of medical cannabis use among cancer patients from a medical cannabis dispensary in New York State. J. Palliat. Med. 2019, 22, 1196–1201. [Google Scholar] [CrossRef]
- Poli, P.; Crestani, F.; Salvadori, C.; Valenti, I.; Sannino, C. Medical cannabis in patients with chronic pain: Effect on pain relief, pain disability, and psychological aspects. a prospective non randomized single arm clinical trial. Clin. Ter. 2018, 169, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Baron, E.P.; Lucas, P.; Eades, J.; Hogue, O. Patterns of medicinal cannabis use, strain analysis, and substitution effect among patients with migraine, headache, arthritis, and chronic pain in a medicinal cannabis cohort: Official Journal of the Italian Society for the Study of Headaches. J. Headache Pain 2018, 19, 1–28. [Google Scholar] [CrossRef]
- Australian Government: Australian Institute of Health and Welfare. Rural & Remote Health; AIHW: Canberra, Australia, 2019. [Google Scholar]
- Perkins, D.; Brophy, H.; McGregor, I.S.; O’Brien, P.; Quilter, J.; McNamara, L.; Sarris, J.; Stevenson, M.; Gleeson, P.; Sinclair, J.; et al. Medicinal cannabis and driving: The intersection of health and road safety policy. Int. J. Drug Policy 2021, 97, 103307. [Google Scholar] [CrossRef]
- Lintzeris, N.; Driels, J.; Elias, N.; Arnold, J.C.; McGregor, I.S.; Allsop, D.J. Medicinal cannabis in Australia, 2016: The cannabis as medicine survey (CAMS-16). Med. J. Aust. 2018, 209, 211–216. [Google Scholar] [CrossRef]
- Rhyne, D.N.; Anderson, S.L.; Gedde, M.; Borgelt, L.M. Effects of medical marijuana on migraine headache frequency in an adult population. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2016, 36, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Lucas, P.; Baron, E.P.; Jikomes, N. Medical cannabis patterns of use and substitution for opioids & other pharmaceutical drugs, alcohol, tobacco, and illicit substances; results from a cross-sectional survey of authorized patients. Harm Reduction J. 2019, 16, 1–11. [Google Scholar] [CrossRef]
- Tarolli, C.G.; Zimmerman, G.A.; Auinger, P.; McIntosh, S.; Horowitz, R.K.; Kluger, B.M.; Dorsey, E.R.; Holloway, R.G. Symptom burden among individuals with Parkinson disease: A national survey. Neurol. Clin. Pract. 2020, 10, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Green, R.; Cutter, G.; Friendly, M.; Kister, I. Which symptoms contribute the most to patients’ perception of health in multiple sclerosis? Mult. Scler. J. Exp. Transl. Clin. 2017, 3, 2055217317728301. [Google Scholar] [CrossRef] [PubMed]
- Schleider, L.B.-L.; Mechoulam, R.; Lederman, V.; Lederman, V.; Hilou, M.; Lencovsky, O.; Betzalel, O.; Shbiro, L.; Novack, V. Prospective analysis of safety and efficacy of medical cannabis in large unselected population of patients with cancer. Eur. J. Intern. Med. 2018, 49, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Wolff, R.F.; Deshpande, S.; Di Nisio, M.; Duffy, S.; Hernandez, A.V.; Keurentjes, J.C.; Lang, S.; Misso, K.; Ryder, S.; et al. Cannabinoids for medical use: A systematic review and meta-analysis. JAMA 2015, 313, 2456–2473. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.; Mailis-Gagnon, A.; Zoheiry, N.; Lakha, S.F. Efficacy and adverse effects of medical marijuana for chronic noncancer pain: Systematic review of randomized controlled trials. Can. Fam. Physician 2015, 61, e372–e381. [Google Scholar]
- Harris, M.; Erridge, S.; Ergisi, M.; Nimalan, D.; Kawka, M.; Salazar, O.; Ali, R.; Loupasaki, K.; Holvey, C.; Coomber, R.; et al. UK Medical Cannabis registry: An analysis of clinical outcomes of medicinal cannabis therapy for chronic pain conditions. Expert Rev. Clin. Pharmacol. 2022, 15, 473–485. [Google Scholar] [CrossRef]
- Bruggink, L.; Hayes, C.; Lawrence, G.; Brain, K.; Holliday, S. Chronic pain: ‘Overlap and specificity in multimorbidity management’. Aust. J. Gen. Pract. 2019, 48, 689–692. [Google Scholar] [CrossRef]
- Urbi, B.; Corbett, J.; Hughes, I.; Owusu, M.A.; Thorning, S.; Broadley, S.A.; Sabet, A.; Heshmat, S. Effects of cannabis in Parkinson’s disease: A systematic review and meta-analysis. J. Park. Dis. 2022, 12, 495–508. [Google Scholar] [CrossRef]
- Cuttler, C.; Spradlin, A.; Cleveland, M.J.; Craft, R.M. Short-and long-term effects of cannabis on headache and migraine. J. Pain 2020, 21, 722–730. [Google Scholar] [CrossRef]
- Mechtler, L.; Bargnes, V.; Hart, P.; McVige, J.; Saikali, N. Medical Cannabis for Chronic Migraine: A Retrospective Review. Neurology 2019, 92 (Suppl. 15), 3.10-015. [Google Scholar]
- Lakin, L.; Davis, B.E.; Binns, C.C.; Currie, K.M.; Rensel, M.R. Comprehensive approach to management of multiple sclerosis: Addressing invisible symptoms—A narrative review. Neurol. Ther. 2021, 10, 75–98. [Google Scholar] [CrossRef]
- Haddad, F.; Dokmak, G.; Karaman, R. The efficacy of cannabis on multiple sclerosis-related symptoms. Life 2022, 12, 682. [Google Scholar] [CrossRef] [PubMed]
- Patti, F.; Messina, S.; Solaro, C.; Amato, M.P.; Bergamaschi, R.; Bonavita, S.; Bossio, R.B.; Morra, V.B.; Costantino, G.F.; Cavalla, P.; et al. Efficacy and safety of cannabinoid oromucosal spray for multiple sclerosis spasticity. J. Neurol. Neurosurg. Psychiatry 2016, 87, 944. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, C.M.; Devins, G.M.; Hussain, M.R. ABC of sleep disorders. Sleep problems in patients with medical illness. BMJ Br. Med. J. 1993, 306, 1532. [Google Scholar] [CrossRef]
- Kuhathasan, N.; Dufort, A.; MacKillop, J.; Gottschalk, R.; Minuzzi, L.; Frey, B.N. The use of cannabinoids for sleep: A critical review on clinical trials. Exp. Clin. Psychopharmacol. 2019, 27, 383. [Google Scholar] [CrossRef] [PubMed]
- Babson, K.A.; Sottile, J.; Morabito, D. Cannabis, cannabinoids, and sleep: A review of the literature. Curr. Psychiatry Rep. 2017, 19, 23. [Google Scholar] [CrossRef]
- Suraev, A.S.; Marshall, N.S.; Vandrey, R.; McCartney, D.; Benson, M.J.; McGregor, I.S.; Grunstein, R.R.; Hoyos, C.M. Cannabinoid therapies in the management of sleep disorders: A systematic review of preclinical and clinical studies. Sleep Med. Rev. 2020, 53, 101339. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J. A primer on medicinal cannabis safety and potential adverse effects. Aust. J. Gen. Pract. 2021, 50, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Pratt, M.; Stevens, A.; Thuku, M.; Butler, C.; Skidmore, B.; Wieland, L.S.; Clemons, M.; Kanji, S.; Hutton, B. Benefits and harms of medical cannabis: A scoping review of systematic reviews. Syst. Rev. 2019, 8, 320. [Google Scholar] [CrossRef]
- Bell, M.L.; Floden, L.; Rabe, B.A.; Hudgens, S.; Dhillon, H.M.; Bray, V.; Vardy, J.L. Analytical approaches and estimands to take account of missing patient-reported data in longitudinal studies. Patient Relat. Outcome Meas. 2019, 10, 129–140. [Google Scholar] [CrossRef]
- Little, R.J.; D’Agostino, R.; Cohen, M.L.; Dickersin, K.; Emerson, S.S.; Farrar, J.T.; Frangakis, C.; Hogan, J.W.; Molenberghs, G.; Murphy, S.A.; et al. The prevention and treatment of missing data in clinical trials. N. Engl. J. Med. 2012, 367, 1355–1360. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Patients (%) (n = 157) |
|---|---|
| Age (years) | |
| Mean ± standard deviation | 63.0 ± 16.0 |
| Range | 18–100 |
| Over 40 years | 141 (89.8) |
| Under 65 years | 75 (47.8) |
| 65 years and over | 82 (52.2) |
| Gender a | |
| Male | 57 (36.3) |
| Female | 100 (63.7) |
| Place of residence | |
| Greater Sydney Region b | 136 (86.6) |
| Non-Sydney NSW | 17 (10.8) |
| Queensland | 1 (0.6) |
| Australian Capital Territory | 1 (0.6) |
| Tasmania | 1 (0.6) |
| Victoria | 1 (0.6) |
| Country of birth | |
| Australia | 105 (66.9) |
| Country other than Australia | 42 (26.7) |
| Unknown | 10 (6.4) |
| Indigenous status | |
| Aboriginal or Torres Strait Islander | 0 (0) |
| Not Indigenous | 153 (97.5) |
| Unknown | 4 (2.5) |
| Relationship status | |
| Single c | 49 (31.2) |
| Partnered d | 90 (57.3) |
| Unknown | 18 (11.5) |
| Previous cannabis use | |
| Yes | 28 (17.8) |
| No | 1 (0.6) |
| Not stated | 128 (81.5) |
| Condition class e and condition | |
| Musculoskeletal | 39 (24.8) f |
| Spondylosis | 25 (15.9) |
| Neurological | 91 (58.0) |
| Parkinson’s disease | 23 (14.6) |
| Migraine | 16 (10.2) |
| Multiple sclerosis | 10 (6.4) |
| Neuropathic pain | 9 (5.7) |
| Peripheral neuropathy | 9 (5.7) |
| Autoimmune | 14 (8.9) |
| Inflammatory | 10 (6.4) |
| Other | 23 (14.6) |
| Chronic pain syndrome | 19 (12.1) |
| Number of conditions treated | |
| One | 137 (87.3) |
| Two | 19 (12.1) |
| Three | 1 (0.6) |
| Indications | |
| Pain | 136 (86.6) |
| Muscle spasms | 18 (11.5) |
| Sleep | 10 (6.4) |
| Cannabis-based medicines used | |
| Number | |
| 1 | 112 (71.3) g |
| 2 | 31 (19.7) |
| ≥3 | 14 (8.9) |
| Type (route of administration) | |
| Oil (oral) | 156 (99.4) |
| Flower (inhalation) | 5 (3.2) |
| Oromucosal spray (sublingual) | 1 (0.6) |
| Cannabinoid ratios | |
| CBD only h | 22 (14.0) |
| CBD dominant i | 5 (3.2) |
| Low Δ-9-THC j | 12 (7.6) |
| Balanced k | 133 (84.7) |
| Δ-9-THC dominant/Δ-9-THC only l | 15 (9.6) |
| Cannabinoid highest dosage (mg/day) | Mean ± SD |
| CBD | 34.8 ± 48.04 * |
| Δ-9-THC | 16.9 ± 17.23 |
| Pain | Fatigue | Breathing Problems | Bowel Problems | Nausea | Appetite | Difficulty Sleeping | Mood | QoL | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p Value, F (DFn, DFd) | <0.0001, F (3.7, 342) = 36 | <0.0001, F (3.8, 357) = 28 | 0.0035, F (3.8, 351) = 4.1 | <0.0001, F (3.7, 340) = 8.3 | 0.1397, F (3.7, 340) = 1.8 | 0.0465, F (3.5, 327) = 2.5 | <0.0001, F (3.1, 292) = 40 | <0.0001, F (3.3, 303) = 14 | <0.0001, F (3.5, 313) = 7.5 | ||||||||||||||||||
| M | p-Value | 95% CI of Diff. | M | p-Value | 95% CI of Diff. | M | p-Value | 95% CI of Diff. | M | p-Value | 95% CI of Diff. | M | p-Value | 95% CI of Diff. | M | p-Value | 95% CI of Diff. | M | p-Value | 95% CI of Diff | M | p-Value | 95% CI of Diff | M | p-Value | 95% CI of Diff | |
| Baseline (n = 140) | 7.9 | 7.3 | 2.5 | 4.9 | 2.5 | 3.1 | 6.4 | 5.6 | 4.2 | ||||||||||||||||||
| 3 months (n = 151) | 6.0 | <0.0001 | 1.4 to 2.3 | 5.5 | <0.0001 | 1.2 to 2.3 | 2.0 | 0.0165 | 0.076 to 1.0 | 3.6 | <0.0001 | 0.58 to 1.9 | 2.3 | 0.7853 | −0.38 to 0.84 | 2.6 | 0.1852 | −0.13 to 0.98 | 3.9 | <0.0001 | 1.9 to 3.0 | 4.1 | <0.0001 | 0.93 to 2.0 | 5.1 | <0.0001 | −1.3 to −0.45 |
| 6 months (n = 100) | 5.8 | <0.0001 | 1.5 to 2.7 | 5.5 | <0.0001 | 1.3 to 2.4 | 1.9 | 0.0084 | 0.14 to 1.2 | 3.7 | 0.004 | 0.30 to 2.0 | 2.3 | 0.8621 | −0.43 to 0.83 | 2.5 | 0.2511 | −0.23 to 1.3 | 4.2 | <0.0001 | 1.6 to 2.7 | 4.1 | <0.0001 | 0.86 to 2.1 | 5.3 | 0.0001 | −1.7 to −0.47 |
| 9 months (n = 81) | 5.7 | <0.0001 | 1.6 to 2.8 | 5.1 | <0.0001 | 1.4 to 2.8 | 2.4 | 0.9486 | −0.45 to 0.72 | 3.5 | 0.0015 | 0.43 to 2.2 | 2.2 | 0.7263 | −0.43 to 1.0 | 3.0 | 0.9983 | −0.71 to 0.86 | 4.1 | <0.0001 | 1.5 to 2.9 | 4.2 | <0.0001 | 0.70 to 2.1 | 5.0 | 0.0039 | −1.4 to −0.22 |
| 12 months (n = 63) | 5.9 | <0.0001 | 1.4 to 2.7 | 5.0 | <0.0001 | 1.5 to 3.0 | 2.0 | 0.1381 | −0.11 to 1.1 | 4.1 | 0.0947 | −0.09 to 1.6 | 2.0 | 0.3074 | −0.27 to 1.3 | 3.1 | 0.9997 | −1.1 to 0.95 | 4.2 | <0.0001 | 1.2 to 3.1 | 4.7 | 0.0244 | 0.090 to 1.7 | 5.1 | 0.0221 | −1.7 to −0.1 |
| Spondylosis a | Pain | Fatigue | Bowel Problems | Difficulty Sleeping | Mood | Quality of Life | ||||||||||||
| p-Value, F (DFn, DFd) | 0.0001, F (2.3, 35) = 11 | 0.0039, F (2.0, 31) = 6.7 | 0.0260, F (1.8, 28) = 4.3 | 0.0037, F (1.7, 26) = 7.5 | 0.0192, F (2.0, 30) = 4.5 | 0.3216, F (2.9, 43) = 1.2 | ||||||||||||
| Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | |
| Baseline (n = 22) | 8.5 | 6.9 | 5.2 | 5.9 | 5.8 | 4.7 | ||||||||||||
| 3 months (n = 24) | 6.8 | 0.0001 | 0.92 to 2.6 | 6.1 | 0.1431 | −0.22 to 1.9 | 3.8 | 0.1635 | −0.44 to 3.2 | 4.3 | 0.0079 | 0.39 to 2.7 | 4.4 | 0.0292 | 0.13 to 2.7 | 5.1 | 0.7412 | −1.5 to 0.75 |
| 6 months (n = 16) | 6.4 | 0.0005 | 1.1 to 3.2 | 4.8 | 0.0039 | 0.72 to 3.5 | 3.5 | 0.2181 | −0.80 to 4.2 | 3.7 | 0.0016 | 0.88 to 3.4 | 4.2 | 0.0295 | 0.16 to 3.1 | 5.7 | 0.3092 | −2.7 to 0.68 |
| 9 months (n = 11) | 5.8 | 0.0044 | 1.1 to 4.4 | 5.5 | 0.1269 | −0.38 to 3.1 | 3.4 | 0.2046 | −0.91 to 4.6 | 4 | 0.0075 | 0.59 to 3.1 | 5.5 | 0.9243 | −1.7 to 2.5 | 4.7 | >0.9999 | −1.8 to 1.8 |
| Parkinson’s disease b | Pain | Fatigue | Bowel problems | Difficulty sleeping | Mood | Quality of life | ||||||||||||
| p-Value, F (DFn, DFd) | 0.0068, F (3.4, 49) = 4.3 | 0.0005, F (2.9, 40) = 7.4 | 0.2521, F (2.1, 30) = 1.4 | 0.0002, F (1.6, 22) = 15 | 0.1228, F (2.3, 32) = 2.2 | 0.2160, F (2.5, 34) = 1.6 | ||||||||||||
| Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | |
| Baseline (n = 21) | 6.7 | 7.5 | 4.8 | 6.4 | 5.4 | 4.4 | ||||||||||||
| 3 months (n = 20) | 4.4 | 0.0039 | 0.71 to 3.9 | 4.7 | 0.0002 | 1.4 to 4.4 | 3.1 | 0.0615 | −0.068 to 3.5 | 3.3 | <0.0001 | 1.8 to 4.4 | 3.7 | 0.0214 | 0.23 to 3.2 | 4.9 | 0.5842 | −1.7 to 0.65 |
| 6 months (n = 16) | 4.8 | 0.0793 | −0.19 to 4.0 | 5.4 | 0.0161 | 0.38 to 3.9 | 3.7 | 0.6584 | −1.6 to 3.8 | 3.3 | 0.0001 | 1.7 to 4.4 | 3.9 | 0.0707 | −0.11 to 3.1 | 5.7 | 0.1724 | −3.1 to 0.46 |
| 9 months (n = 15) | 5.1 | 0.0917 | −0.22 to 3.4 | 5 | 0.0067 | 0.73 to 4.4 | 3.3 | 0.1953 | −0.59 to 3.6 | 3.4 | 0.0007 | 1.4 to 4.5 | 3.7 | 0.0791 | −0.17 to 3.5 | 5.4 | 0.3543 | −2.9 to 0.78 |
| 12 months (n = 12) | 4.9 | 0.1614 | −0.58 to 4.1 | 4.3 | 0.0092 | 0.85 to 5.6 | 3.9 | 0.5466 | −1.1 to 2.9 | 3.3 | 0.0235 | 0.42 to 5.8 | 3.8 | 0.1499 | −0.48 to 3.7 | 4.6 | 0.9954 | −2.7 to 2.2 |
| Chronic pain syndrome c | Pain | Fatigue | Bowel problems | Difficulty sleeping | Mood | Quality of life | ||||||||||||
| p-Value, F (DFn, DFd) | 0.0012, F (2.1, 23) = 8.8 | 0.0362, F (1.7, 19) = 4.2 | 0.7399, F (2.4, 26) = 0.36 | 0.0128, F (2.6, 29) = 4.6 | 0.0013, F (2.5, 27) = 7.5 | 0.1453, F (2.2, 22) = 2.1 | ||||||||||||
| Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | |
| Baseline (n = 16) | 9.1 | 7.1 | 5.1 | 6.4 | 6.1 | 3.7 | ||||||||||||
| 3 months (n = 19) | 6.8 | 0.0052 | 0.67 to 3.9 | 5.3 | 0.2321 | −0.80 to 4.3 | 4.3 | 0.8853 | −2.4 to 4.1 | 3.4 | 0.0015 | 1.2 to 4.9 | 3.9 | 0.01 | 0.50 to 3.9 | 5.1 | 0.0293 | −2.6 to −0.13 |
| 6 months (n = 11) | 7.1 | 0.043 | 0.063 to 3.8 | 6.5 | 0.6122 | −0.94 to 2.2 | 4.5 | 0.94 | −2.6 to 3.9 | 5.4 | 0.582 | −1.5 to 3.7 | 4.2 | 0.1026 | −0.39 to 4.2 | 4 | 0.9957 | −2.7 to 2.2 |
| 9 months (n = 11) | 5.9 | 0.0031 | 1.3 to 5.0 | 4.2 | 0.0147 | 0.67 to 5.1 | 4.5 | 0.9323 | −2.4 to 3.6 | 3.7 | 0.1257 | −0.74 to 6.2 | 4 | 0.1444 | −0.70 to 4.9 | 5.2 | 0.2037 | −3.8 to 0.83 |
| 12 months (n = 10) | 7.8 | 0.0348 | 0.11 to 2.5 | 6.1 | 0.6067 | −1.7 to 3.7 | 5.3 | 0.9998 | −4.3 to 4.0 | 4.6 | 0.5133 | −2.5 to 6.2 | 7.6 | 0.4838 | −4.7 to 1.8 | 4 | 0.9806 | −2.1 to 1.6 |
| Neuropathic pain/peripheral neuropathy d | Pain | Fatigue | Bowel problems | Difficulty sleeping | Mood | Quality of life | ||||||||||||
| p-Value, F (DFn, DFd) | <0.0001, F (2.5, 27) = 14 | 0.0326, F (2.5, 26) = 3.6 | 0.0563, F (2.6, 29) = 2.9 | 0.0046, F (2.2, 24) = 6.4 | 0.5335, F (2.0, 22) = 0.65 | 0.0771, F (2.7, 29) = 2.6 | ||||||||||||
| Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | |
| Baseline (n = 17) | 8.8 | 6.6 | 4.4 | 6.8 | 4.6 | 4.2 | ||||||||||||
| 3 months (n = 18) | 6.2 | <0.0001 | 1.5 to 3.8 | 4.5 | 0.1047 | −0.35 to 4.5 | 3 | 0.0273 | 0.14 to 2.7 | 4.1 | 0.0014 | 1.1 to 4.4 | 3.9 | 0.7809 | −1.4 to 2.8 | 5.4 | 0.0353 | −2.4 to −0.073 |
| 6 months (n = 12) | 5.2 | <0.0001 | 2.2 to 5.1 | 5 | 0.153 | −0.53 to 3.8 | 3 | 0.422 | −1.3 to 4.1 | 4.3 | 0.0073 | 0.74 to 4.4 | 4.2 | 0.9828 | −2.1 to 2.8 | 5.7 | 0.096 | −3.4 to 0.25 |
| 9 months (n = 9) | 6.1 | 0.0038 | 1.1 to 4.4 | 4.4 | 0.209 | −1.3 to 5.7 | 2.3 | 0.3018 | −1.5 to 5.7 | 4.5 | 0.0616 | −0.12 to 4.8 | 4.2 | 0.943 | −1.9 to 2.7 | 5.2 | 0.3717 | −3.0 to 0.94 |
| 12 months (n = 10) | 6.2 | 0.008 | 0.79 to 4.5 | 4.1 | 0.0949 | −0.48 to 5.6 | 2.7 | 0.2241 | −0.90 to 4.4 | 5 | 0.1147 | −0.43 to 4.2 | 3.1 | 0.1474 | −0.49 to 3.6 | 5.3 | 0.4064 | −3.2 to 1.0 |
| Migraine e | Pain | Fatigue | Bowel problems | Difficulty sleeping | Mood | Quality of life | ||||||||||||
| p-Value, F (DFn, DFd) | 0.2182, F (1.7, 19) = 1.7 | 0.0144, F (2.0, 23) = 5.1 | 0.1243, F (2.3, 27) = 2.2 | 0.0171, F (2.4, 27) = 4.4 | 0.2191, F (1.7, 18) = 1.7 | 0.1138, F (2.0, 20) = 2.4 | ||||||||||||
| Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | |
| Baseline (n = 17) | 7.9 | 6.9 | 4.3 | 6.4 | 5.7 | 3.8 | ||||||||||||
| 3 months (n = 18) | 7.2 | 0.7377 | −1.4 to 2.7 | 5.8 | 0.0287 | 0.12 to 2.2 | 3.4 | 0.4631 | −0.97 to 2.8 | 4.2 | 0.0536 | −0.030 to 4.4 | 4.8 | 0.2354 | −0.46 to 2.3 | 4.6 | 0.3831 | −2.4 to 0.72 |
| 6 months (n = 12) | 6.9 | 0.1592 | −0.33 to 2.3 | 5.5 | 0.0424 | 0.049 to 2.8 | 3 | 0.418 | −1.3 to 4.0 | 3.9 | 0.0606 | −0.11 to 5.1 | 5.3 | 0.909 | −1.9 to 2.8 | 4.8 | 0.2834 | −2.7 to 0.68 |
| 9 months (n = 9) | 6.4 | 0.2864 | −1.0 to 3.9 | 5.8 | 0.3116 | −0.85 to 3.1 | 4.1 | 0.9874 | −2.8 to 3.3 | 4.3 | 0.1356 | −0.64 to 4.9 | 4.3 | 0.546 | −2.0 to 4.8 | 4.2 | 0.9356 | −2.8 to 2.0 |
| Multiple sclerosis f | Pain | Fatigue | Bowel problems | Difficulty sleeping | Mood | Quality of life | ||||||||||||
| Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | |
| Baseline (n = 10) | 9 | 9.5 | 3 | 7.5 | 7 | 3.5 | ||||||||||||
| 3 months (n = 10) | 6.3 | 0.0859 | −3.0 to 0.0 | 6 | 0.0039 | −6.0 to −1.0 | 2.5 | 0.4609 | −5.0 to 1.0 | 4.3 | 0.0039 | −5.5 to −1.0 | 5 | 0.0195 | −5.0 to 0.50 | 5 | 0.0508 | 0.0 to 3.0 |
| Pain a | Pain | Fatigue | Bowel Problems | Difficulty Sleeping | Mood | Quality of Life | ||||||||||||
| p-Value, F (DFn, DFd) | <0.0001, F (5.0, 308) = 26 | <0.0001, F (5.6, 342) = 15 | <0.0001, F (5.2, 316) = 5.3 | <0.0001, F (4.8, 296) = 21 | <0.0001, F (5.0, 305) = 6.9 | 0.0004, F (4.7, 279) = 4.8 | ||||||||||||
| Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | Mean | p-Value | 95% CI of Diff. | |
| Baseline (n = 122) | 8.5 | 7.3 | 4.9 | 6.4 | 5.6 | 4.1 | ||||||||||||
| 3 months (n = 131) | 6.5 | <0.0001 | 1.5 to 2.5 | 5.6 | <0.0001 | 1.0 to 2.3 | 3.7 | 0.0001 | 0.50 to 2.0 | 4 | <0.0001 | 1.8 to 3.0 | 4.1 | <0.0001 | 0.83 to 2.0 | 4.9 | <0.0001 | −1.3 to −0.40 |
| 6 months (n = 90) | 6.1 | <0.0001 | 1.9 to 3.0 | 5.5 | <0.0001 | 1.2 to 2.4 | 3.8 | 0.0121 | 0.18 to 2.1 | 4.3 | <0.0001 | 1.5 to 2.8 | 4 | <0.0001 | 0.78 to 2.2 | 5.2 | 0.0003 | −1.8 to −0.42 |
| 9 months (n = 72) | 6 | <0.0001 | 1.8 to 3.1 | 5.2 | <0.0001 | 1.3 to 2.9 | 3.6 | 0.0049 | 0.31 to 2.4 | 4.1 | <0.0001 | 1.5 to 3.1 | 4.1 | <0.0001 | 0.63 to 2.3 | 5 | 0.0137 | −1.6 to −0.13 |
| 12 months (n = 55) | 6.2 | <0.0001 | 1.6 to 3.0 | 5 | <0.0001 | 1.4 to 3.1 | 4.1 | 0.1599 | −0.18 to 1.8 | 4.1 | <0.0001 | 1.2 to 3.4 | 4.7 | 0.092 | −0.088 to 1.8 | 5.1 | 0.029 | −2.0 to −0.074 |
| Muscle spasm a | Pain | Fatigue | Bowel problems | Difficulty sleeping | Mood | Quality of life | ||||||||||||
| p-Value, F (DFn, DFd) | 0.0490, F (2.8, 28) = 3.1 | 0.0043, F (1.9, 19) = 7.6 | 0.1481, F (2.6, 26) = 2.0 | 0.0555, F (1.4, 14) = 3.9 | 0.1790, F (2.0, 20) = 1.9 | 0.4053, F (2.2, 21) = 0.96 | ||||||||||||
| Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | Mean | p-Value | 95% CI of diff. | |
| Baseline (n = 16) | 6.8 | 7.6 | 5.4 | 5.4 | 4.7 | 4.3 | ||||||||||||
| 3 months (n = 17) | 4.5 | 0.0201 | 0.33 to 4.2 | 4.8 | 0.0003 | 1.4 to 4.2 | 3.3 | 0.0978 | −0.31 to 4.4 | 2.9 | 0.0028 | 0.89 to 4.1 | 3.1 | 0.1239 | −0.34 to 3.5 | 5 | 0.3463 | −2.0 to 0.51 |
| 6 months (n = 11) | 4.4 | 0.1706 | −0.90 to 5.8 | 6 | 0.1522 | −0.50 to 3.6 | 3.4 | 0.1528 | −0.63 to 4.6 | 3.5 | 0.0174 | 0.34 to 3.3 | 4.1 | 0.8001 | −1.4 to 2.6 | 5.1 | 0.7777 | −3.3 to 1.8 |
| 9 months (n = 10) | 4.4 | 0.1326 | −0.69 to 5.6 | 4.9 | 0.0266 | 0.34 to 5.1 | 3 | 0.1514 | −0.80 to 5.7 | 3.5 | 0.094 | −0.32 to 4.2 | 3.3 | 0.3255 | −1.0 to 3.8 | 5.3 | 0.5827 | −3.2 to 1.3 |
| 12 months (n = 8) | 3.4 | 0.1348 | −1.2 to 8.1 | 3.8 | 0.0072 | 1.5 to 6.2 | 2.8 | 0.1428 | −0.99 to 6.2 | 3.8 | 0.6223 | −3.1 to 6.3 | 3 | 0.2172 | −1.0 to 4.4 | 4.9 | 0.9376 | −3.9 to 2.8 |
| Sleep b | Pain | Fatigue | Bowel problems | Difficulty sleeping | Mood | Quality of life | ||||||||||||
| Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | Median | p-Value | 95% CI of diff. | |
| Baseline (n = 9) | 7 | 8 | 3 | 7.5 | 7 | 5 | ||||||||||||
| 3 months (n = 9) | 2 | 0.1406 | −5.0 to 0.50 | 5.5 | 0.0391 | −6.0 to 0.0 | 2 | 0.5625 | −3.0 to 2.5 | 4 | 0.0117 | −4.0 to −1.5 | 4 | 0.0156 | −4.5 to 0.50 | 6 | 0.3281 | −1.0 to 3.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morris, M.; Chye, R.; Liu, Z.; Agar, M.; Razmovski-Naumovski, V. A Retrospective Medical Record Review of Adults with Non-Cancer Diagnoses Prescribed Medicinal Cannabis. J. Clin. Med. 2023, 12, 1483. https://doi.org/10.3390/jcm12041483
Morris M, Chye R, Liu Z, Agar M, Razmovski-Naumovski V. A Retrospective Medical Record Review of Adults with Non-Cancer Diagnoses Prescribed Medicinal Cannabis. Journal of Clinical Medicine. 2023; 12(4):1483. https://doi.org/10.3390/jcm12041483
Chicago/Turabian StyleMorris, Michael, Richard Chye, Zhixin Liu, Meera Agar, and Valentina Razmovski-Naumovski. 2023. "A Retrospective Medical Record Review of Adults with Non-Cancer Diagnoses Prescribed Medicinal Cannabis" Journal of Clinical Medicine 12, no. 4: 1483. https://doi.org/10.3390/jcm12041483