
Safety and Efficacy of Dexmedetomidine for Bronchoscopy: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Literature Screen
2.4. Data Collection
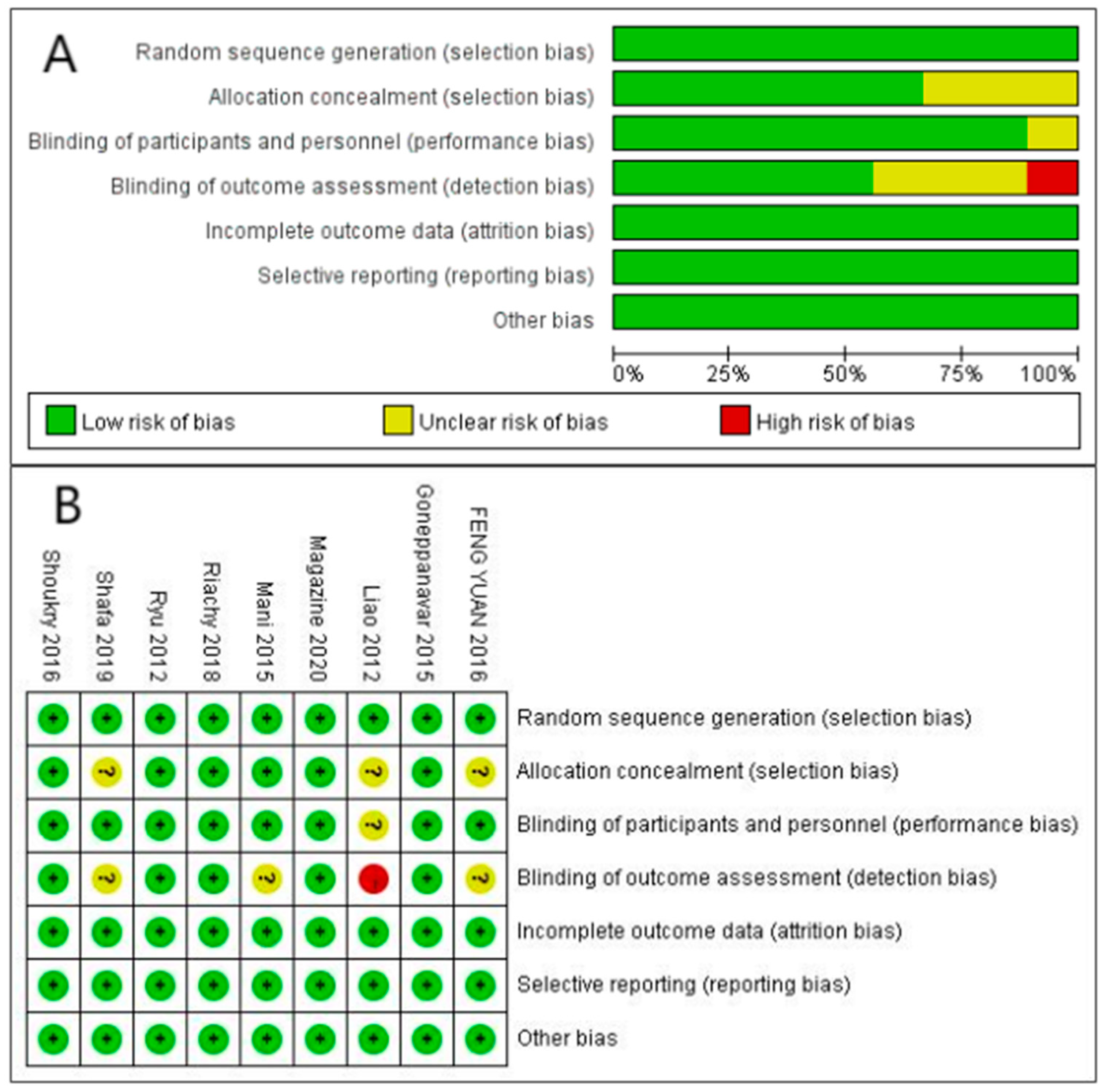
2.5. Bias Assessment
2.6. Meta-Analysis
3. Results
3.1. Literature Search and Basic Characteristics of the Literature
3.2. Quality Evaluation
3.3. Results of the Meta-Analysis
3.3.1. Hypoxemia
3.3.2. Hypertension
3.3.3. Hypotension
3.3.4. Tachycardia
3.3.5. Bradycardia
3.3.6. Patient Satisfaction Level
3.3.7. Arrhythmia
3.3.8. Cough
3.3.9. Laryngospasm
3.3.10. Bronchospasm
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- José, R.J.; Shaefi, S.; Navani, N. Sedation for flexible bronchoscopy: Current and emerging evidence. Eur. Respir. Rev. 2013, 22, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Poi, P.J.; Chuah, S.Y.; Srinivas, P.; Liam, C.K. Common fears of patients undergoing bronchoscopy. Eur. Respir. J. 1998, 11, 1147–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xavier Scheuermeyer, F.; Andolfatto, G.; Qian, H.; Grafstein, E. Does the sedation regimen affect adverse events during procedural sedation and analgesia in injection drug users? CJEM 2013, 15, 279–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Rand, I.A.; Blaikley, J.; Booton, R.; Chaudhuri, N.; Gupta, V.; Khalid, S.; Mandal, S.; Martin, J.; Mills, J.; Navani, N. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: Accredited by NICE. Thorax 2013, 68 (Suppl. 1), i1–i44. [Google Scholar] [CrossRef] [Green Version]
- Schlatter, L.; Pflimlin, E.; Fehrke, B.; Meyer, A.; Tamm, M.; Stolz, D. Propofol versus propofol plus hydrocodone for flexible bronchoscopy: A randomised study. Eur. Respir. J. 2011, 38, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Ost, D.E.; Ernst, A.; Grosu, H.B.; Lei, X.; Diaz-Mendoza, J.; Slade, M.; Gildea, T.R.; Machuzak, M.S.; Jimenez, C.A.; Toth, J. Therapeutic bronchoscopy for malignant central airway obstruction: Success rates and impact on dyspnea and quality of life. Chest 2015, 147, 1282–1298. [Google Scholar] [CrossRef] [Green Version]
- Piro, R.; Casalini, E.; Fontana, M.; Galeone, C.; Ruggiero, P.; Taddei, S.; Ghidoni, G.; Patricelli, G.; Facciolongo, N. Efficacy and safety of EBUS-TBNA under conscious sedation with meperidine and midazolam. Thorac. Cancer 2022, 13, 533–538. [Google Scholar] [CrossRef]
- McCambridge, A.J.; Boesch, R.P.; Mullon, J.J. Sedation in Bronchoscopy: A Review. Clin. Chest Med. 2018, 39, 65–77. [Google Scholar] [CrossRef]
- Olkkola, K.T.; Ahonen, J. Midazolam and other benzodiazepines. Handb. Exp. Pharmacol. 2008, 182, 335–360. [Google Scholar]
- Watts, M.R.; Geraghty, R.; Moore, A.; Saunders, J.; Swift, C.G. Premedication for bronchoscopy in older patients: A double-blind comparison of two regimens. Respir. Med. 2005, 99, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Lo, Y.L.; Lin, T.Y.; Fang, Y.F.; Wang, T.Y.; Chen, H.C.; Chou, C.L.; Chung, F.T.; Kuo, C.H.; Feng, P.H.; Liu, C.Y. Feasibility of bispectral index-guided propofol infusion for flexible bronchoscopy sedation: A randomized controlled trial. PLoS ONE 2011, 6, e27769. [Google Scholar] [CrossRef] [PubMed]
- Stolz, D.; Kurer, G.; Meyer, A.; Chhajed, P.N.; Pflimlin, E.; Strobel, W.; Tamm, M. Propofol versus combined sedation in flexible bronchoscopy: A randomised non-inferiority trial. Eur. Respir. J. 2009, 34, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Clark, G.; Licker, M.; Younossian, A.B.; Soccal, P.M.; Frey, J.G.; Rochat, T.; Diaper, J.; Bridevaux, P.O.; Tschopp, J.M. Titrated sedation with propofol or midazolam for flexible bronchoscopy: A randomised trial. Eur. Respir. J. 2009, 34, 1277–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, J.; Jeon, Y.; Park, H.P.; Lim, Y.J.; Oh, Y.S. Comparison of alfetanil and ketamine in combination with propofol for patient-controlled sedation during fiberoptic bronchoscopy. Acta Anaesthesiol. Scand. 2005, 49, 1334–1338. [Google Scholar] [CrossRef]
- Gasparini, S. It is time for patients to undergo bronchoscopy without discomfort. Eur. Respir. J. 2011, 38, 507–509. [Google Scholar] [CrossRef]
- Jantz, M.A. The old and the new of sedation for bronchoscopy. Chest 2009, 135, 4–6. [Google Scholar] [CrossRef]
- Lee, S. Dexmedetomidine: Present and future directions. Korean, J. Anesthesiol. 2019, 72, 323–330. [Google Scholar] [CrossRef]
- Sinha, S.K.; Joshiraj, B.; Chaudhary, L.; Hayaran, N.; Kaur, M.; Jain, A. A comparison of dexmedetomidine plus ketamine combination with dexmedetomidine alone for awake fiberoptic nasotracheal intubation: A randomized controlled study. J. Anaesthesiol. Clin. Pharmacol. 2014, 30, 514–519. [Google Scholar]
- Deutsch, E.; Tobias, J.D. Hemodynamic and respiratory changes following dexmedetomidine administration during general anesthesia: Sevoflurane vs desflurane. Paediatr. Anaesthesia. 2007, 17, 438–444. [Google Scholar] [CrossRef]
- Koroglu, A.; Teksan, H.; Sagir, O.; Yucel, A.; Toprak, H.I.; Ersoy, O.M. A comparison of the sedative, hemodynamic, and respiratory effects of dexmedetomidine and propofol in children undergoing magnetic resonance imaging. Anesth. Analg. 2006, 103, 63–67. [Google Scholar] [CrossRef]
- Venn, R.M.; Hell, J.; Grounds, R.M. Respiratory effects of dexmedetomidine in the surgical patient requiring intensive care. Crit. Care 2000, 4, 302–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, W.; Ma, G.; Su, Q.G.; Fang, Y.; Gu, B.C.; Zou, X.M. Dexmedetomidine versus midazolam for conscious sedation in postoperative patients undergoing flexible bronchoscopy: A randomized study. J. Int. Med. Res. 2012, 40, 1371–1380. [Google Scholar] [CrossRef] [PubMed]
- Goneppanavar, U.; Magazine, R.; Periyadka Janardhana, B.; Krishna Achar, S. Intravenous Dexmedetomidine Provides Superior Patient Comfort and Tolerance Compared to Intravenous Midazolam in Patients Undergoing Flexible Bronchoscopy. Pulm. Med. 2015, 2015, 727530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, J.H.; Lee, S.W.; Lee, J.H.; Lee, E.H.; Do, S.H.; Kim, C.S. Randomized double-blind study of remifentanil and dexmedetomidine for flexible bronchoscopy. Br. J. Anaesth. 2012, 108, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022); John Wiley & Sons: Hoboken, NJ, USA, 2022; Available online: www.training.cochrane.org/handbook (accessed on 4 August 2022).
- Mani, B.; George, S.; Saif Khan, M.; King, H. Propofol versus dexmedetomidine as a sole sedative for diagnostic flexible bronchoscopy: A randomized double-blind study. Ain Shams, J. Anaesthesiol. 2015, 8, 573–579. [Google Scholar]
- Shoukry, R.A. Safety and efficacy of dexmedetomidine sedation for elective fiberoptic bronchoscopy: A comparative study with propofol. Egypt. J. Anaesth. 2016, 32, 483–488. [Google Scholar] [CrossRef] [Green Version]
- Yuan, F.; Fu, H.; Yang, P.; Sun, K.; Wu, S.; Lv, M.; Dong, Z.; Dong, T. Dexmedetomidine-fentanyl versus propofol-fentanyl in flexible bronchoscopy: A randomized study. Exp. Ther. Med. 2016, 12, 506–512. [Google Scholar] [CrossRef] [Green Version]
- Magazine, R.; Venkatachala, S.K.; Goneppanavar, U.; Surendra, V.U.; Guddattu, V.; Chogtu, B. Comparison of midazolam and low-dose dexmedetomidine in flexible bronchoscopy: A prospective, randomized, double-blinded study. Indian, J. Pharmacol. 2020, 52, 23–30. [Google Scholar]
- Riachy, M.; Khayat, G.; Ibrahim, I.; Aoun, Z.; Dabar, G.; Bazarbachi, T.; Khalil, N.; Habr, B. A randomized double-blind controlled trial comparing three sedation regimens during flexible bronchoscopy: Dexmedetomidine, alfentanil and lidocaine. Clin. Respir. J. 2018, 12, 1407–1415. [Google Scholar] [CrossRef] [Green Version]
- Shafa, A.; Habibzadeh, M.; Shetabi, H.; Agil, A. Comparing the hemodynamic effects of nebulized dexmedetomidine and nebulized lidocaine in children undergoing fiberoptic bronchoscopy. J. Zanjan Univ. Med. Sci. Health Serv. 2019, 27, 14–19. [Google Scholar] [CrossRef]
- Lee, J.A.; Rowen, D.W.; Rose, D.D. Bronchial thermoplasty: A novel treatment for severe asthma requiring monitored anesthesia care. AANA J. 2011, 79, 480–483. [Google Scholar] [PubMed]
- Tsai, C.J.; Chu, K.S.; Chen, T.I.; Lu, D.V.; Wang, H.M.; Lu, I.C. A comparison of the effectiveness of dexmedetomidine versus propofol target-controlled infusion for sedation during fibreoptic nasotracheal intubation. Anaesthesia 2010, 65, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Riker, R.R.; Shehabi, Y.; Bokesch, P.M.; Ceraso, D.; Wisemandle, W.; Koura, F.; Whitten, P.; Margolis, B.D.; Byrne, D.W.; Ely, E.W.; et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: A randomized trial. JAMA 2009, 301, 489–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, X.Y.; Cao, J.P.; He, Q.; Shi, X.Y. Dexmedetomidine for the management of awake fibreoptic intubation. Cochrane Database Syst. Rev. 2014, 2014, Cd009798. [Google Scholar] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Description |
|---|---|
| Population | patients undergoing bronchoscopy in outpatient clinics |
| Intervention | Anesthetic drugs are used alone or in combination to maintain continuous sedation during bronchoscopy |
| Comparison | Dexmedetomidine vs. other anesthetic drugs |
| Outcomes | Primary outcomes were hypoxemia, hypertension, hypotension, tachycardia, and bradycardia. Secondary outcomes were patient satisfaction, cough, laryngospasm, bronchospasm, and arrhythmia. |
| Study, Year | Number of Patients | ASA (I/II/III) | Age (years) | Height (cm) | Weight (kg) | BMI (kg/m2) | Intervention | Administration Route | Sedation Score | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| G D | G C | G D | G C | ||||||||
| FENG YUAN, 2016 [29] | 50 | 50 | 42/29/29 | 60.11 ± 7.27 | N/A | N/A | 21.95 ± 3.11 | 1 µg/kg Dexmedetomidine + 1 µg/kg fentanyl | 4 µg/mL propofol + 1 µg/kg fentanyl | Intravenous infusion | MOAA/S |
| Shoukry, 2016 [28] | 36 | 36 | N/A | 49.1 ± 15.1 | N/A | 79.1 ± 14.1 | N/A | 1 µg/kg Dexmedetomidine + 1 µg/kg fentanyl | 0.5–1 mg/kg propofol + 1 µg/kg fentanyl | Intravenous infusion | Ramsay Sedation Score |
| Shafa, 2019 [32] | 25 | 25 | N/A | 2.34 ± 1.77 | N/A | N/A | N/A | 2 µg/kg Dexmedetomidine | 1% Lidocaine (4 mg/kg Nebulized) | aerosol | Ramsay Sedation Score |
| Ryu, 2012 [24] | 35 | 35 | 47/23 | 52.9 | 163 | 61.35 | N/A | 0.5 mg/kg propofol + 0.4–2 µg/kg Dexmedetomidine | 0.5 mg/kg propofol + 1–5 µg/kg remifentanil | Intravenous infusion | MOAA/S |
| Riachy, 2018 [31] | 53 | 55 | N/A | 18–70 | N/A | N/A | N/A | 0.5 µg/kg Dexmedetomidine | 10 µg/kg alfentanil | Intravenous infusion | NICS |
| Mani, 2015 [27] | 30 | 30 | 39/21 | 44.75 ± 14.8 | 164.9 | 61.3 ± 6.15 | N/A | 1 μg/kg Dexmedetomidine | 1 mg/kg propofol | Intravenous infusion | MOAA/S |
| Maga- zine, 2020 [30] | 27 | 27 | N/A | 46.04 ± 13.83 | 159.92 ± 9.13 | 51.8 ± 9.27 | 20.30 ± 3.39 | 0.5 μg/kg Dexmedetomidine | 0.035 mg/kg midazolam | Intravenous infusion | Ramsay Sedation Score |
| Liao, 2012 [22] | 99 | 98 | N/A | 59.3 ± 8.75 | 161.75 ± 7.80 | 57.60 ± 9.84 | N/A | 1 µg/kg Dexmedetomidine | 2 mg midazolam | Intravenous infusion | Ramsay Sedation Score |
| Gonepp-anavar, 2015 [23] | 27 | 27 | N/A | 51.11 ± 14.45 | 162.45 ± 5.41 | 54.67 ± 10.47 | 20.60 ± 3.43 | 1 μg/kg Dexmedetomidine | 0.02 mg/kg midazolam | Intravenous infusion | Ramsay Sedation Score |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Q.; An, Q.; Zhao, L.; Wu, M.; Wang, Y.; Guo, Z. Safety and Efficacy of Dexmedetomidine for Bronchoscopy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1607. https://doi.org/10.3390/jcm12041607
Guo Q, An Q, Zhao L, Wu M, Wang Y, Guo Z. Safety and Efficacy of Dexmedetomidine for Bronchoscopy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(4):1607. https://doi.org/10.3390/jcm12041607
Chicago/Turabian StyleGuo, Qianqian, Qi An, Lin Zhao, Meng Wu, Ye Wang, and Zhenggang Guo. 2023. "Safety and Efficacy of Dexmedetomidine for Bronchoscopy: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 4: 1607. https://doi.org/10.3390/jcm12041607