
Attitudes of Anesthesiologists toward Artificial Intelligence in Anesthesia: A Multicenter, Mixed Qualitative–Quantitative Study
 , , , , , ,
, , , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Study Participants
2.4. Part One: In-Depth Interviews
2.5. Part Two: Online Survey
2.6. Statistical Analysis
3. Results
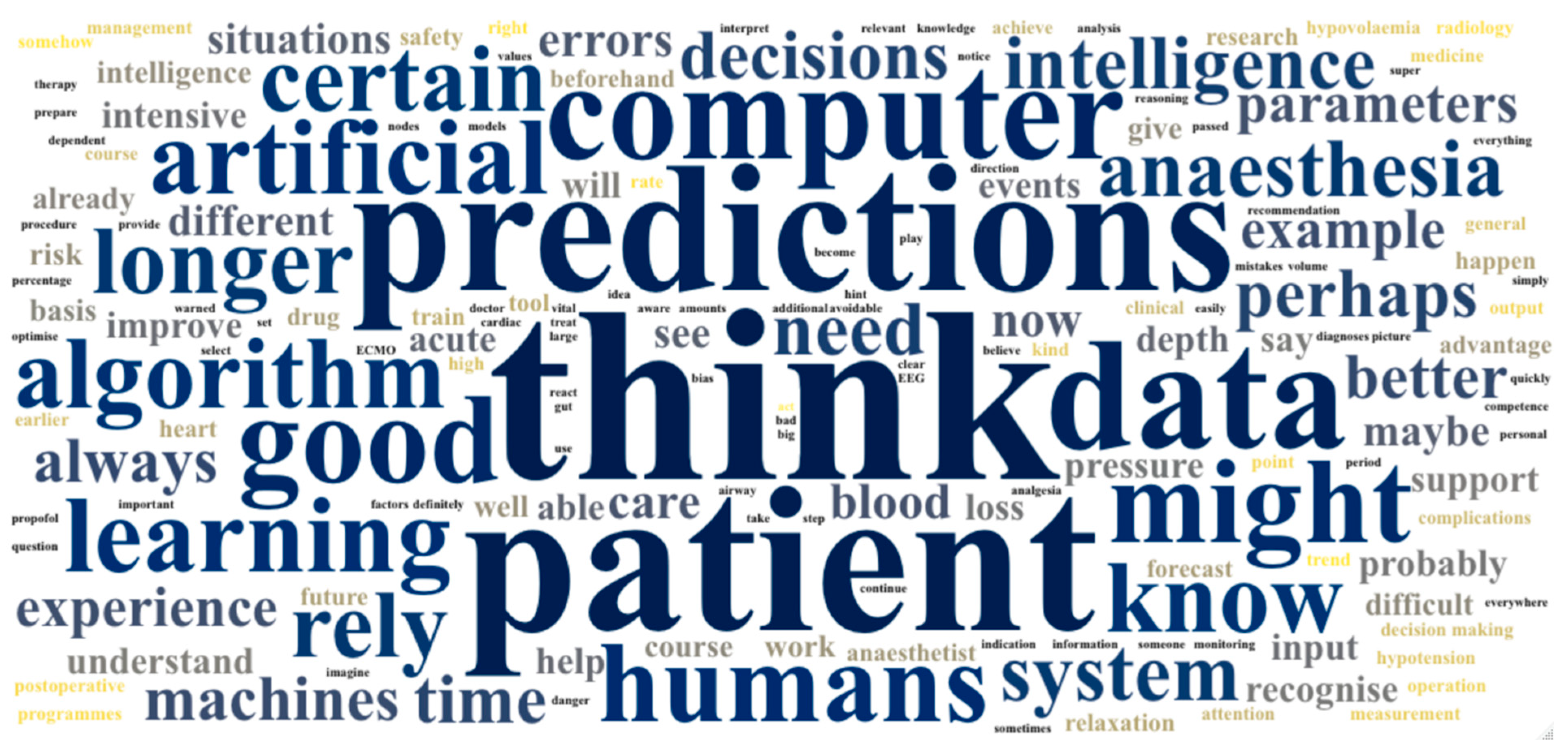
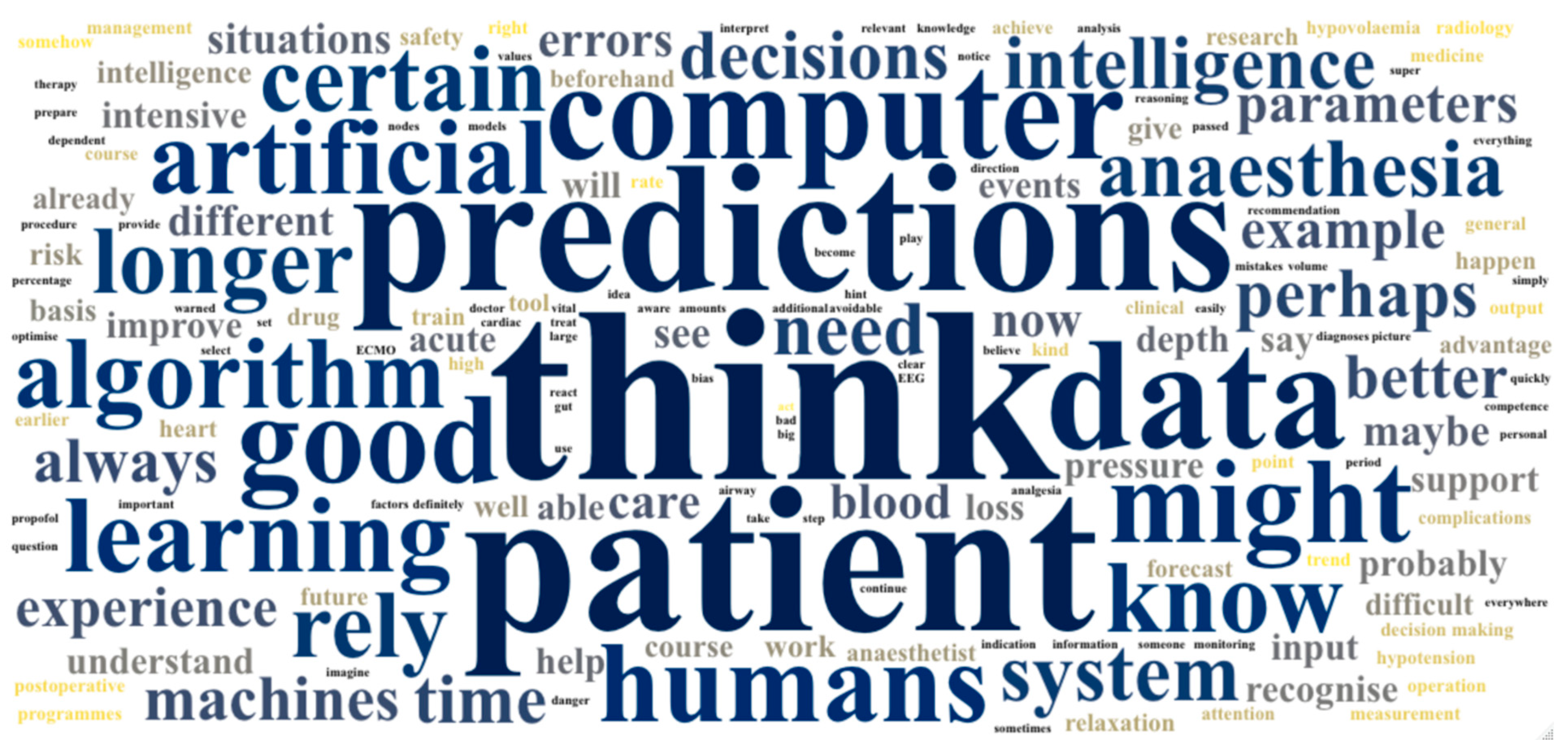
3.1. Part One: In-Depth Interviews
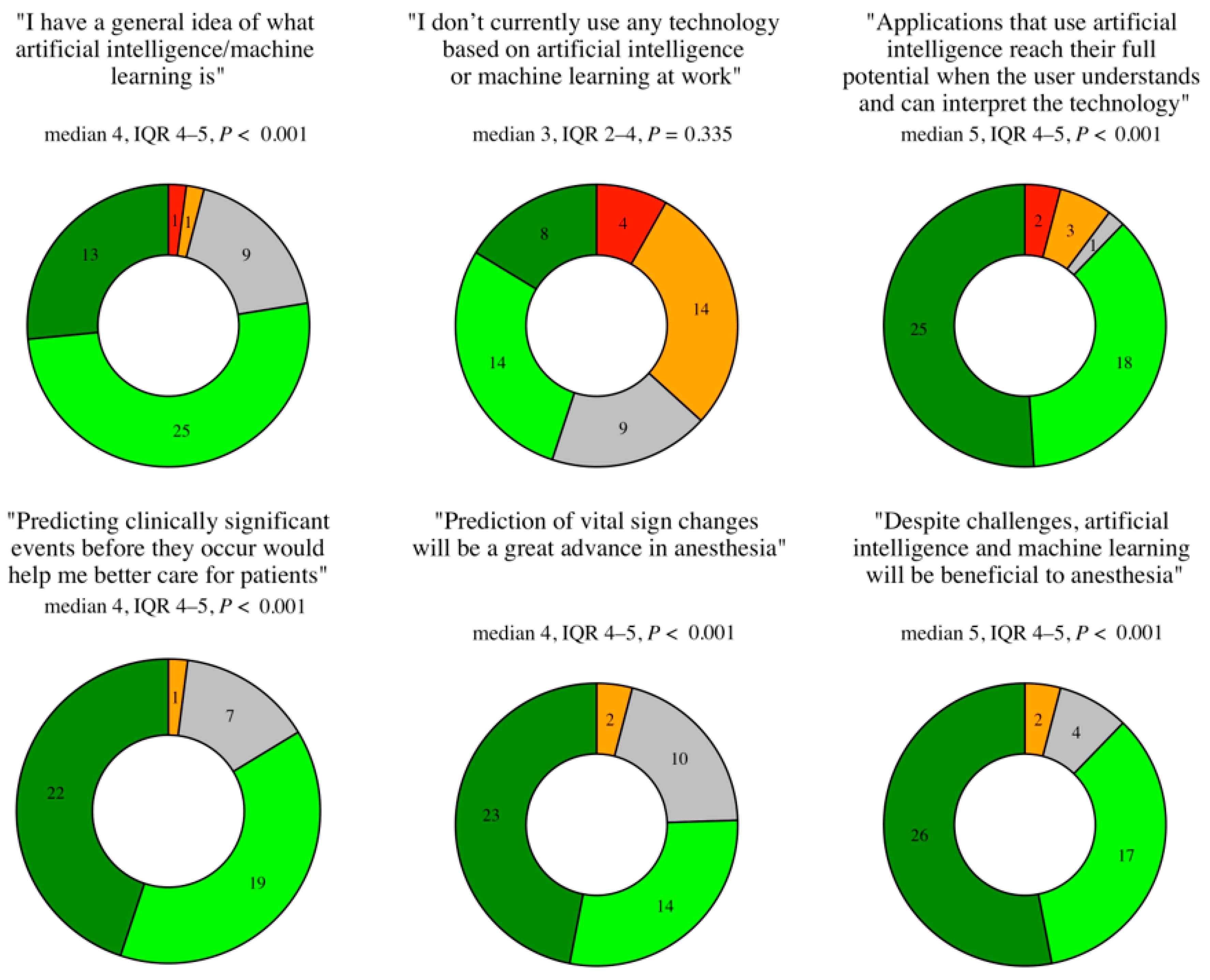
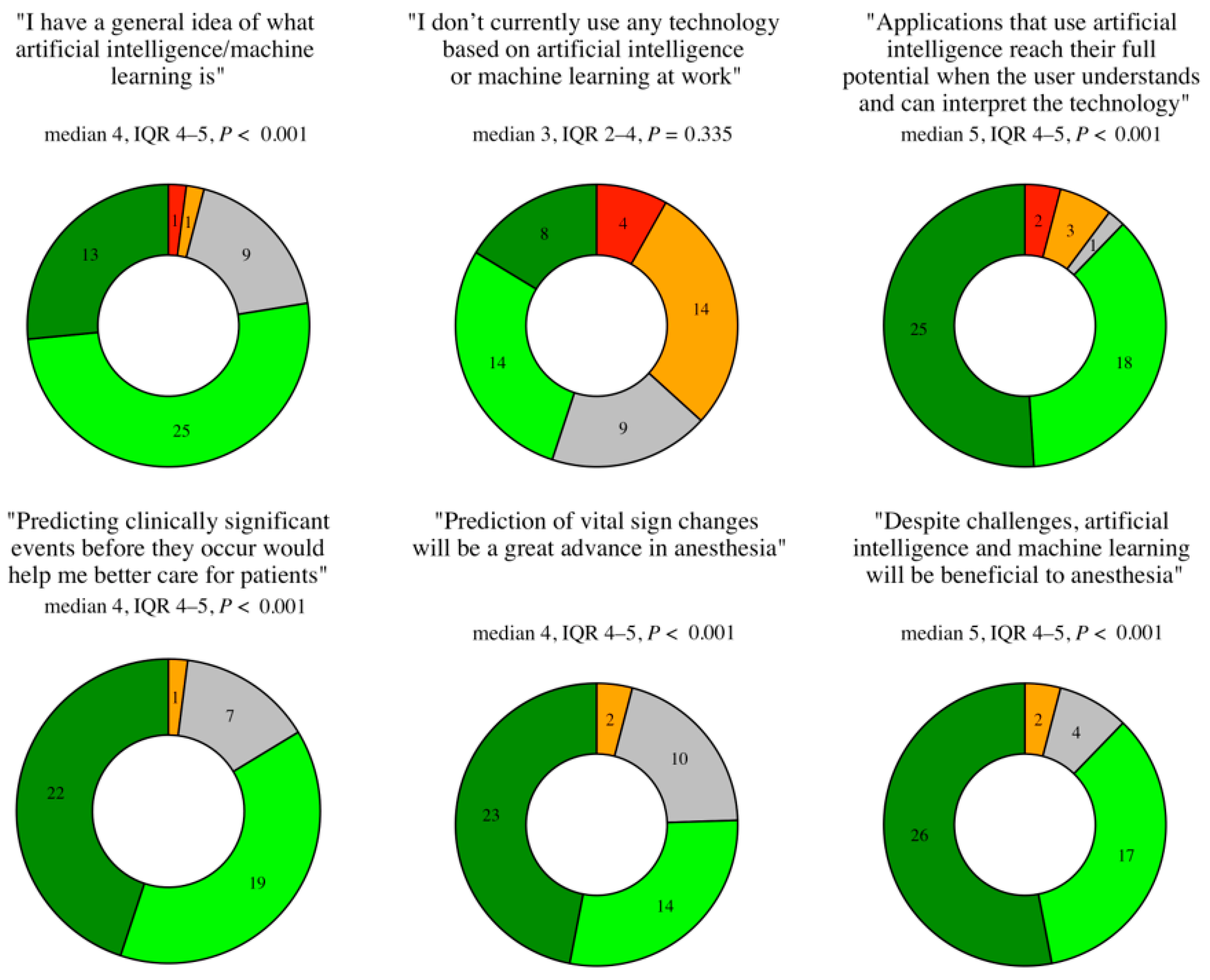
3.2. Part Two: Online Survey
4. Discussion
4.1. Principal Findings
4.2. Comparison to Prior Work
4.3. Limitations
4.4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Questions
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of any applications of artificial intelligence or machine learning in anesthesia?

- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- Was verstehen Sie unter den Begriffen «künstliche Intelligenz» oder «maschinelles Lernen»?
- Sind Ihnen Anwendungen von künstlicher Intelligenz in der Anästhesie bekannt?
- Welche Vor- und Nachteile könnte die künstliche Intelligenz in der Anästhesie Ihrer Meinung nach haben?
- Insbesondere, was halten Sie von der Verwendung künstlicher Intelligenz zur Erstellung von Vorhersagen?
- Welche Vorhersagen («Predictions») sind Ihrer Meinung nach besonders nützlich?
Appendix B. Coding Schemes

{kind=link}
{kind=link}
{kind=link}
| 1.1 Little/no prior knowledge |
| 1.2 Information technology |
| 1.3 Capabilities |
| 1.4 Clinical support tool |
| 2.1 Clinical |
| 2.2 Research |
| 2.3 Other specialty |
| 2.4 Non-AI/-ML example |
| 2.5 None |
| 3.1 Pros |
| 3.1.1 Technical pros |
| 3.1.2 Human–computer interaction pros |
| 3.2 Cons |
| 3.2.1 Technical cons |
| 3.2.2 Human–computer interaction cons |
| 4.1 Positive statement |
| 4.2 Negative statement |
| 4.3 Cautious/neutral statement |
| 4.4 Not possible/technology too immature |
| 5.1 Risk stratification |
| 5.2 Vital sign prediction |
| 5.3 Treatment guide |
| 5.4 Not useful/technologically impossible |
| 5.5 Event type |
Appendix C. Online Survey
Appendix D. Interview Transcripts
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
- 1.
- What do you understand by the terms “artificial intelligence” or “machine learning”?
- 2.
- Are you aware of applications of artificial intelligence in anaesthesia?
- 3.
- What do you think are the advantages and disadvantages of artificial intelligence in anaesthesia?
- 4.
- In particular, what do you think about the use of artificial intelligence to make predictions?
- 5.
- Which predictions do you think are most useful clinically?
References
- Benjamens, S.; Dhunnoo, P.; Meskó, B. The state of artificial intelligence-based FDA-approved medical devices and algorithms: An online database. npj Digit. Med. 2020, 3, 118. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; Depristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Nagendran, M.; Chen, Y.; Lovejoy, C.A.; Gordon, A.; Komorowski, M.; Harvey, H.; Topol, E.J.; Ioannidis, J.P.A.; Collins, G.; Maruthappu, M. Artificial intelligence versus clinicians: Systematic review of design, reporting standards, and claims of deep learning studies. BMJ 2020, 368, m689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, D.A.; Witkowski, E.; Gao, L.; Meireles, O.; Rosman, G. Artificial Intelligence in Anesthesiology. Anesthesiology 2020, 132, 379–394. [Google Scholar] [CrossRef]
- Brogi, E.; Cyr, S.; Kazan, R.; Giunta, F.; Hemmerling, T.M. Clinical Performance and Safety of Closed-Loop Systems: A Systematic Review and Meta-analysis of Randomized Con-trolled Trials. Anesth. Analg. 2017, 124, 446–455. [Google Scholar] [CrossRef]
- Wijnberge, M.; Geerts, B.F.; Hol, L.; Lemmers, N.; Mulder, M.P.; Berge, P.; Schenk, J.; Terwindt, L.E.; Hollmann, M.W.; Vlaar, A.P.; et al. Effect of a Machine Learning–Derived Early Warning System for Intraoperative Hypotension vs Standard Care on Depth and Duration of Intraoperative Hypotension During Elective Noncardiac Surgery: The HYPE Randomized Clinical Trial. JAMA 2020, 323, 1052–1060. [Google Scholar] [CrossRef]
- Eltorai, A.E.M.; Bratt, A.K.; Guo, H.H. Thoracic Radiologists’ Versus Computer Scientists’ Perspectives on the Future of Artificial Intelligence in Radiology. J. Thorac. Imaging 2020, 35, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Maassen, O.; Fritsch, S.; Palm, J.; Deffge, S.; Kunze, J.; Marx, G.; Riedel, M.; Schuppert, A.; Bickenbach, J. Future Medical Artificial Intelligence Application Requirements and Expectations of Physicians in German University Hospitals: Web-Based Survey. J. Med. Internet Res. 2021, 23, e26646. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, D.P.; Giese, D.; Brodehl, S.; Chon, S.H.; Staab, W.; Kleinert, R.; Maintz, D.; Baeßler, B. Medical students’ attitude towards artificial intelligence: A multicentre survey. Eur. Radiol. 2019, 29, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Huisman, M.; Ranschaert, E.; Parker, W.; Mastrodicasa, D.; Koci, M.; de Santos, D.P.; Coppola, F.; Morozov, S.; Zins, M.; Bohyn, C.; et al. An international survey on AI in radiology in 1,041 radiologists and radiology residents part 1: Fear of replacement, knowledge, and attitude. Eur. Radiol. 2021, 31, 7058–7066. [Google Scholar] [CrossRef] [PubMed]
- Moser, A.; Korstjens, I. Series: Practical guidance to qualitative research. Part 1: Introduction. Eur. J. Gen. Pract. 2017, 23, 271–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenhalgh, T.; Annandale, E.; Ashcroft, R.; Barlow, J.; Black, N.; Bleakley, A.; Boaden, R.; Braithwaite, J.; Britten, N.; Carnevale, F.; et al. An open letter to The BMJ editors on qualitative research. BMJ 2016, 352, i563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obermeyer, Z.; Topol, E.J. Artificial intelligence, bias, and patients’ perspectives. Lancet 2021, 397, 2038. [Google Scholar] [CrossRef]
- Saint, S.; Kowalski, C.P.; Banaszak-Holl, J.; Forman, J.; Damschroder, L.; Krein, S.L. How Active Resisters and Organizational Constipators Affect Health Care–Acquired Infection Prevention Efforts. Jt. Comm. J. Qual. Patient Saf. 2009, 35, 239–246. [Google Scholar] [CrossRef]
- Shafer, S.L.; Egan, T. Target-Controlled Infusions. Anesth. Analg. 2016, 122, 1–3. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Francis, J.J.; Johnston, M.; Robertson, C.; Glidewell, L.; Entwistle, V.; Eccles, M.P.; Grimshaw, J. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol. Health 2010, 25, 1229–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obermeyer, Z.; Lee, T.H. Lost in Thought—The Limits of the Human Mind and the Future of Medicine. N. Engl. J. Med. 2017, 377, 1209–1211. [Google Scholar] [CrossRef] [Green Version]
- Liyanage, H.; Liaw, S.-T.; Jonnagaddala, J.; Schreiber, R.; Kuziemsky, C.; Terry, A.L.; de Lusignan, S. Artificial Intelligence in Primary Health Care: Perceptions, Issues, and Challenges. Yearb. Med. Informatics 2019, 28, 041–046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinho, A.; Kroesen, M.; Chorus, C. A healthy debate: Exploring the views of medical doctors on the ethics of artificial intelligence. Artif. Intell. Med. 2021, 121, 102190. [Google Scholar] [CrossRef] [PubMed]
- Shelmerdine, S.C.; Rosendahl, K.; Arthurs, O.J. Artificial intelligence in paediatric radiology: International survey of health care professionals’ opinions. Pediatr. Radiol. 2021, 52, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Staartjes, V.E.; Stumpo, V.; Kernbach, J.M.; Klukowska, A.M.; Gadjradj, P.S.; Schröder, M.L.; Veeravagu, A.; Stienen, M.N.; van Niftrik, C.H.B.; Serra, C.; et al. Machine learning in neurosurgery: A global survey. Acta Neurochir. 2020, 162, 3081–3091. [Google Scholar] [CrossRef]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med. Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Samuel, A.L. Some Studies in Machine Learning Using the Game of Checkers. IBM J. Res. Dev. 1959, 3, 210–229. [Google Scholar] [CrossRef]
- Ramos, K.; Linscheid, R.; Schafer, S. Real-time information-seeking behavior of residency physicians. Fam. Med. 2003, 35, 257–260. [Google Scholar] [PubMed]
- Collado-Mesa, F.; Alvarez, E.; Arheart, K. The Role of Artificial Intelligence in Diagnostic Radiology: A Survey at a Single Radiology Residency Training Program. J. Am. Coll. Radiol. 2018, 15, 1753–1757. [Google Scholar] [CrossRef] [PubMed]
- Gianfrancesco, M.A.; Tamang, S.; Yazdany, J.; Schmajuk, G. Potential Biases in Machine Learning Algorithms Using Electronic Health Record Data. JAMA Intern. Med. 2018, 178, 1544–1547. [Google Scholar] [CrossRef] [PubMed]
- Mullainathan, S.; Obermeyer, Z. Does Machine Learning Automate Moral Hazard and Error? Am. Econ. Rev. 2017, 107, 476–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amann, J.; Blasimme, A.; Vayena, E.; Frey, D.; Madai, V.I.; Precise4Q consortium. Explainability for artificial intelligence in healthcare: A multidisciplinary perspective. BMC Med. Inform. Decis. Mak. 2020, 20, 310. [Google Scholar] [CrossRef]
- Hayasaka, T.; Kawano, K.; Kurihara, K.; Suzuki, H.; Nakane, M.; Kawamae, K. Creation of an artificial intelligence model for intubation difficulty classification by deep learning (convolutional neural network) using face images: An observational study. J. Intensiv. Care 2021, 9, 38. [Google Scholar] [CrossRef]
- Hu, Y.-J.; Ku, T.-H.; Jan, R.-H.; Wang, K.; Tseng, Y.-C.; Yang, S.-F. Decision tree-based learning to predict patient controlled analgesia consumption and readjustment. BMC Med. Informatics Decis. Mak. 2012, 12, 131. [Google Scholar] [CrossRef] [Green Version]
- Blease, C.; Kaptchuk, T.J.; Bernstein, M.H.; Mandl, K.D.; Halamka, J.D.; DesRoches, C.M. Artificial Intelligence and the Future of Primary Care: Exploratory Qualitative Study of UK General Practitioners’ Views. J. Med. Internet Res. 2019, 21, e12802. [Google Scholar] [CrossRef] [Green Version]
- Layard Horsfall, H.; Palmisciano, P.; Khan, D.Z.; Muirhead, W.; Koh, C.H.; Stoyanov, D.; Marcus, H.J. Attitudes of the Surgical Team Toward Artificial Intelligence in Neurosurgery: International 2-Stage Cross-Sectional Survey. World Neurosurg. 2021, 146, e724–e730. [Google Scholar] [CrossRef]
- Ruiz Morilla, M.D.; Sans, M.; Casasa, A.; Giménez, N. Implementing technology in healthcare: Insights from physicians. BMC Med. Inform. Decis. Mak. 2017, 17, 92. [Google Scholar] [CrossRef] [Green Version]
- Schepman, A.; Rodway, P. Initial validation of the general attitudes towards Artificial Intelligence Scale. Comput. Hum. Behav. Rep. 2020, 1, 100014. [Google Scholar] [CrossRef] [PubMed]
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 4: Trustworthiness and publishing. Eur. J. Gen. Pract. 2018, 24, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Participant Characteristics | Part One: Interviews (n = 21) | Part Two: Survey (n = 49) |
|---|---|---|
| Age (y) | 33 (26–55 [28–35]) | 34 (25–55 [28–37]) |
| Male | 5 (24%) | - |
| Female | 16 (76%) | - |
| Experience (y) | 3 (0–25 [2–8]) | 4 (1–26 [2–7]) |
| Resident | 17 (81%) | 34 (69%) |
| Attending | 4 (19%) | 15 (31%) |
| Participating Center | UKF, UKW | UKF, UKW, USZ |
| Question | Code | Statements | Example Statement(s) |
|---|---|---|---|
| What do you understand by the terms “artificial intelligence” or “machine learning”? | Little/no prior knowledge | 4/90 (4%) | “I don’t really have a clue about that” (participant 16) |
| Information technology | 44/90 (49%) | “With the help of algorithms that people program … they train a system” (participant 7) | |
| Capabilities | 34/90 (38%) | “Computers [which] adjust and perfect their predictions based on performance” (participant 3) “Computers learn new things themselves” (participant 4) | |
| Clinical support tool | 8/90 (9%) | “Integrate computing into everyday clinical life” (participant 2) | |
| Are you aware of any applications of artificial intelligence or machine learning in anesthesia? | Research | 7/42 (17%) | “There’s a lot of research going on right now, and we’re also carrying out the ENVISION study, which uses AI” (participant 18) |
| Other specialty | 5/42 (12%) | “I’ve heard of it in radiology” (participant 13) | |
| Non-AI/-ML example | 7/42 (17%) | “We have an EEG monitor. I assume that this is relevant” (participant 13) | |
| None | 23/42 (55%) | “I can’t think of anything” (participant 10) |
| Question | Code | Number | Example Statement(s) |
|---|---|---|---|
| What do you think are the advantages and disadvantages of artificial intelligence in anesthesia? | Technical pros | 24/105 (23%) | “Machines don’t get tired, they don’t have bad days, they usually function better, they have a better memory than any human being and they have an unlimited capacity for learning” (participant 8) “We rely a lot on experience, on feeling—and that is sometimes justified—but I think that in some areas, artificial intelligence is more precise and perhaps makes better decisions than humans” (participant 20) |
| Human-computer interaction pros | 22/105 (21%) | “It can support you in making decisions, especially when you are uncertain, [for example when] parameters are perhaps contradictory” [participant 20] | |
| Technical cons | 21/105 (20%) | “The situation can be diverse or much more differentiated than an algorithm can reckon with” (participant 2) “In medicine … there is often a gender bias, especially in drug studies, and that is a challenge to overcome” (participant 18) | |
| Human-computer interaction cons | 38/105 (36%) | “The anesthesiologist can now spontaneously decide ‘okay, I’ll give fentanyl now’ and the AI only knows that when it is given as an input” [participant 6] “If the system fails, you are left standing there and no longer know how things work” (participant 12) “If you decide to go against that recommendation, then there’s kind of an ethical and moral dilemma, right? What if the patient then dies? Then you must ask ‘What could I have done better?’ Should one always do the therapy recommended by artificial intelligence? So that’s kind of very difficult”. (participant 19) |
| Question | Code | Number | Example Statement(s) |
|---|---|---|---|
| In particular, what do you think about the use of artificial intelligence to make predictions? | Positive statement | 32/67 (48%) | “You could prepare yourself better for situations, with fewer surprises, which probably also means better patient safety” (participant 10) |
| Negative statement | 6/67 (9%) | “You perhaps lose the bigger picture a little bit” (participant 5) | |
| Cautious/neutral statement | 19/67 (28%) | “So long as there’s still someone behind it who interprets it or what it means and reacts properly to it” (participant 13) | |
| Not possible/technology too immature | 10/67 (15%) | “Things are so extremely different from patient to patient that I can’t imagine that an AI can manage that” (participant 1) | |
| Which predictions do you think are most useful clinically? | Risk stratification | 14/92 (15%) | “Outcome relevant points. [For example] Is the patient at risk of PONV, postoperative myocardial infarction, stroke, etc.?” (participant 7) |
| Vital sign predictions | 36/92 (39%) | “The viral parameters, of course” (participant 6) | |
| Treatment guide | 17/92 (18%) | “I think what I have not yet seen was the post-operative analgesic requirement, which would certainly be exciting” (participant 13) | |
| Not useful/technologically impossible | 6/92 (7%) | “If that’s even possible, to predict like that” (participant 5) | |
| Event type | 19/92 (21%) | “Acute events in the operating theatre” (participant 7) “Things that are quite subtle, and that could easily be overlooked” (participant 20) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henckert, D.; Malorgio, A.; Schweiger, G.; Raimann, F.J.; Piekarski, F.; Zacharowski, K.; Hottenrott, S.; Meybohm, P.; Tscholl, D.W.; Spahn, D.R.; et al. Attitudes of Anesthesiologists toward Artificial Intelligence in Anesthesia: A Multicenter, Mixed Qualitative–Quantitative Study. J. Clin. Med. 2023, 12, 2096. https://doi.org/10.3390/jcm12062096
Henckert D, Malorgio A, Schweiger G, Raimann FJ, Piekarski F, Zacharowski K, Hottenrott S, Meybohm P, Tscholl DW, Spahn DR, et al. Attitudes of Anesthesiologists toward Artificial Intelligence in Anesthesia: A Multicenter, Mixed Qualitative–Quantitative Study. Journal of Clinical Medicine. 2023; 12(6):2096. https://doi.org/10.3390/jcm12062096
Chicago/Turabian StyleHenckert, David, Amos Malorgio, Giovanna Schweiger, Florian J. Raimann, Florian Piekarski, Kai Zacharowski, Sebastian Hottenrott, Patrick Meybohm, David W. Tscholl, Donat R. Spahn, and et al. 2023. "Attitudes of Anesthesiologists toward Artificial Intelligence in Anesthesia: A Multicenter, Mixed Qualitative–Quantitative Study" Journal of Clinical Medicine 12, no. 6: 2096. https://doi.org/10.3390/jcm12062096