

Development and Validation of a Prognostic Model for Overall Survival in Patients with Primary Pelvis and Spine Osteosarcoma: A Population-Based Study and External Validation

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
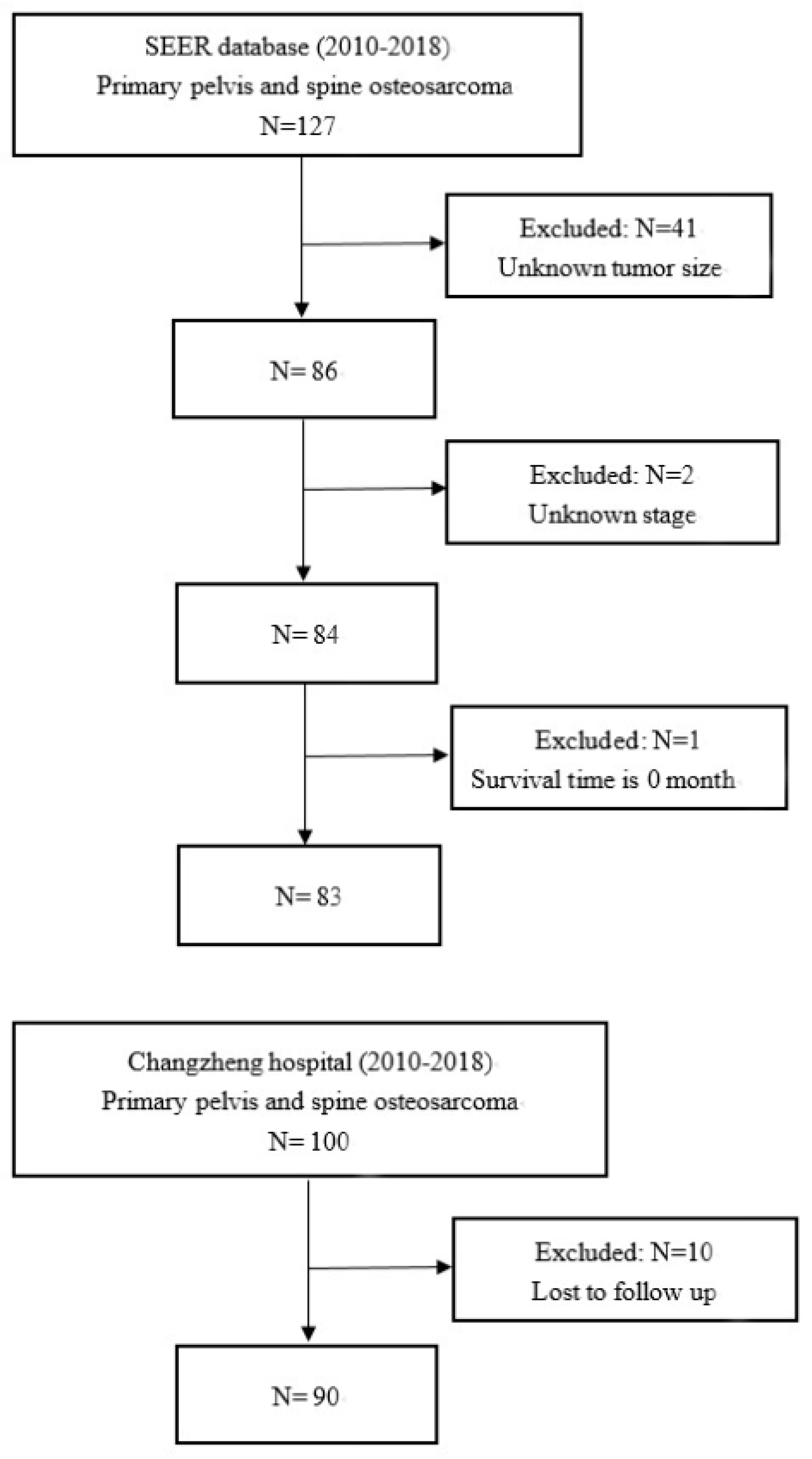
2.1. Study Design and Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Baseline Characteristics
3.2. Statistical Analysis of Prognostic Factors in SEER Cohort
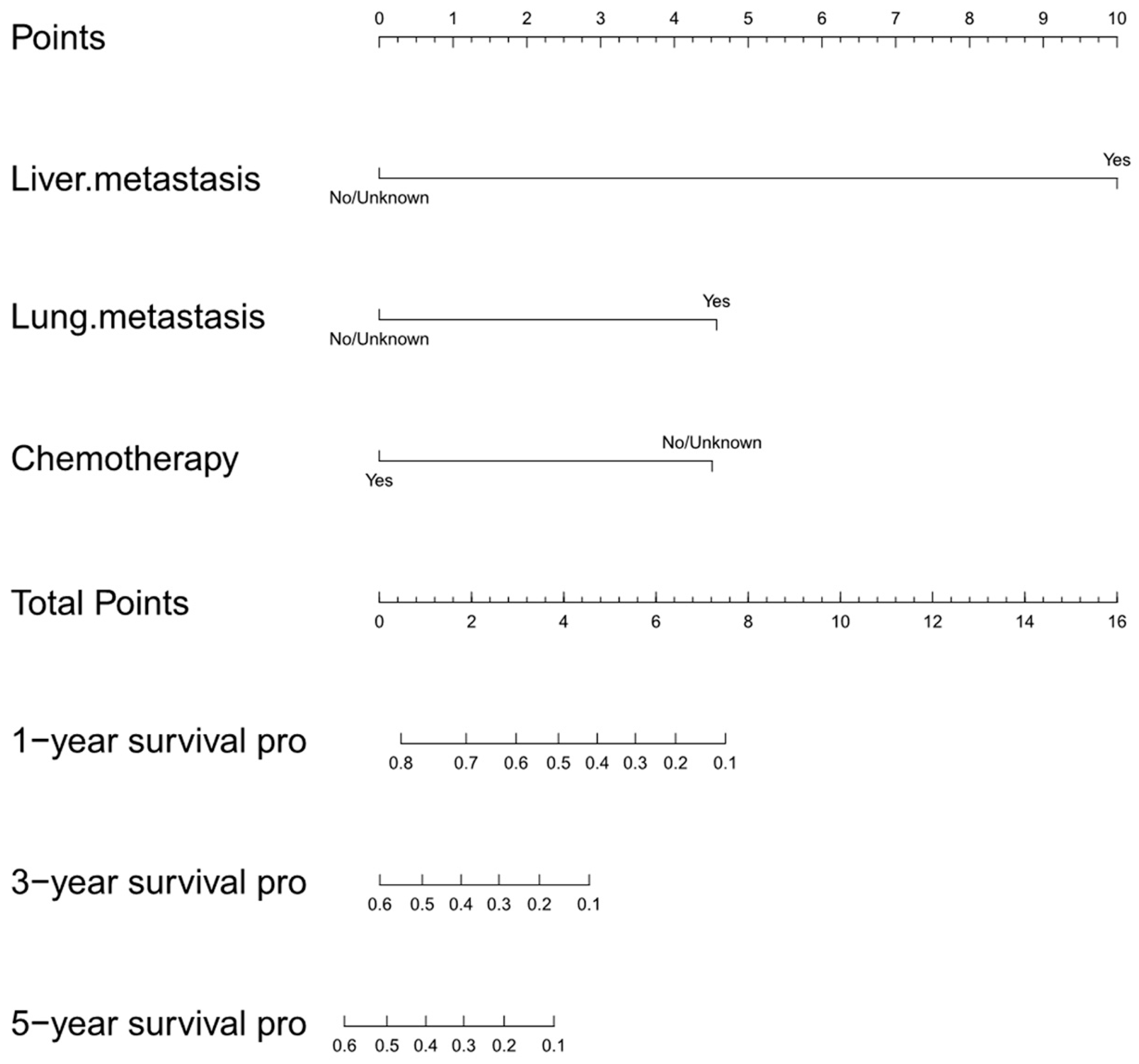
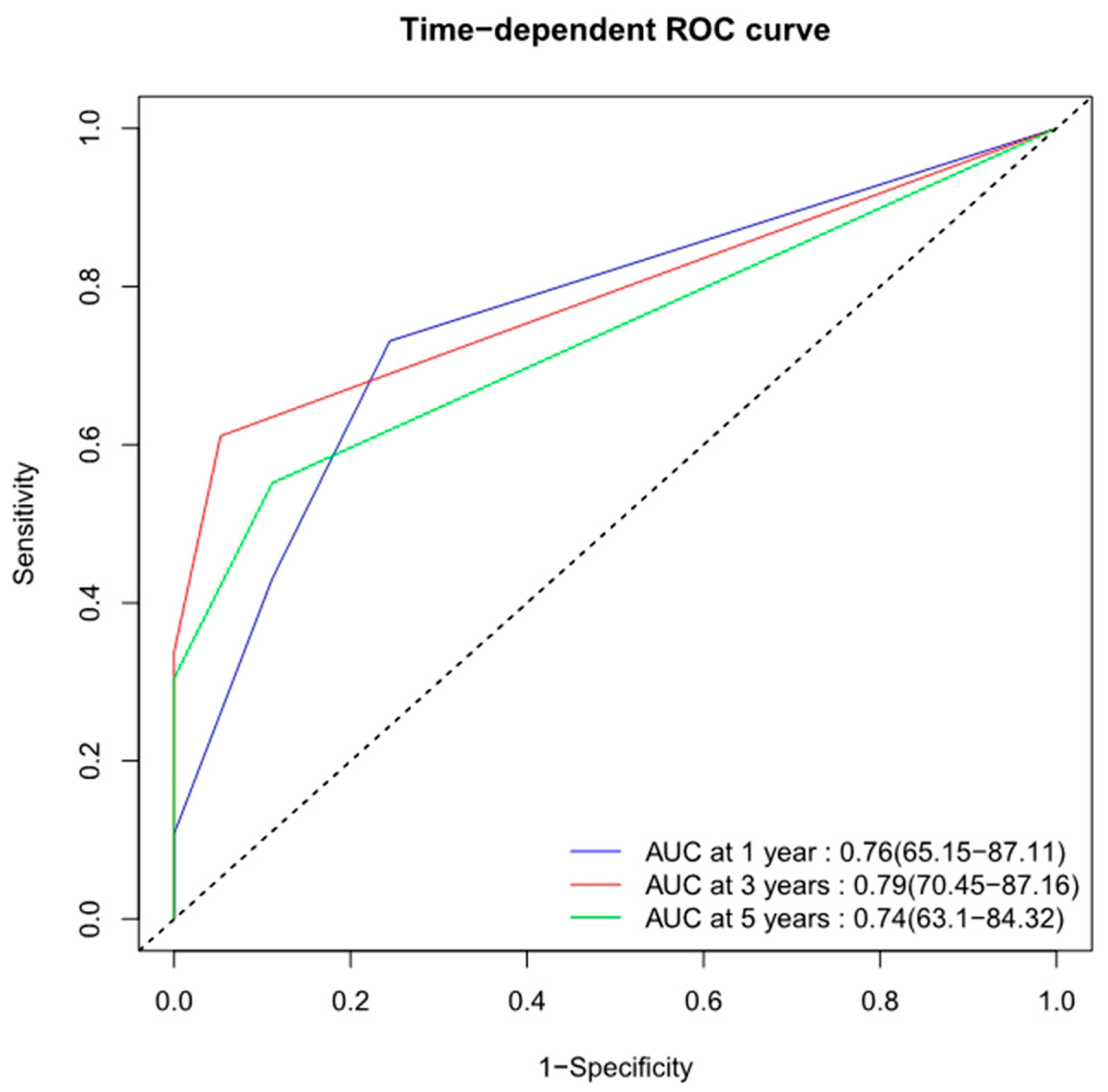
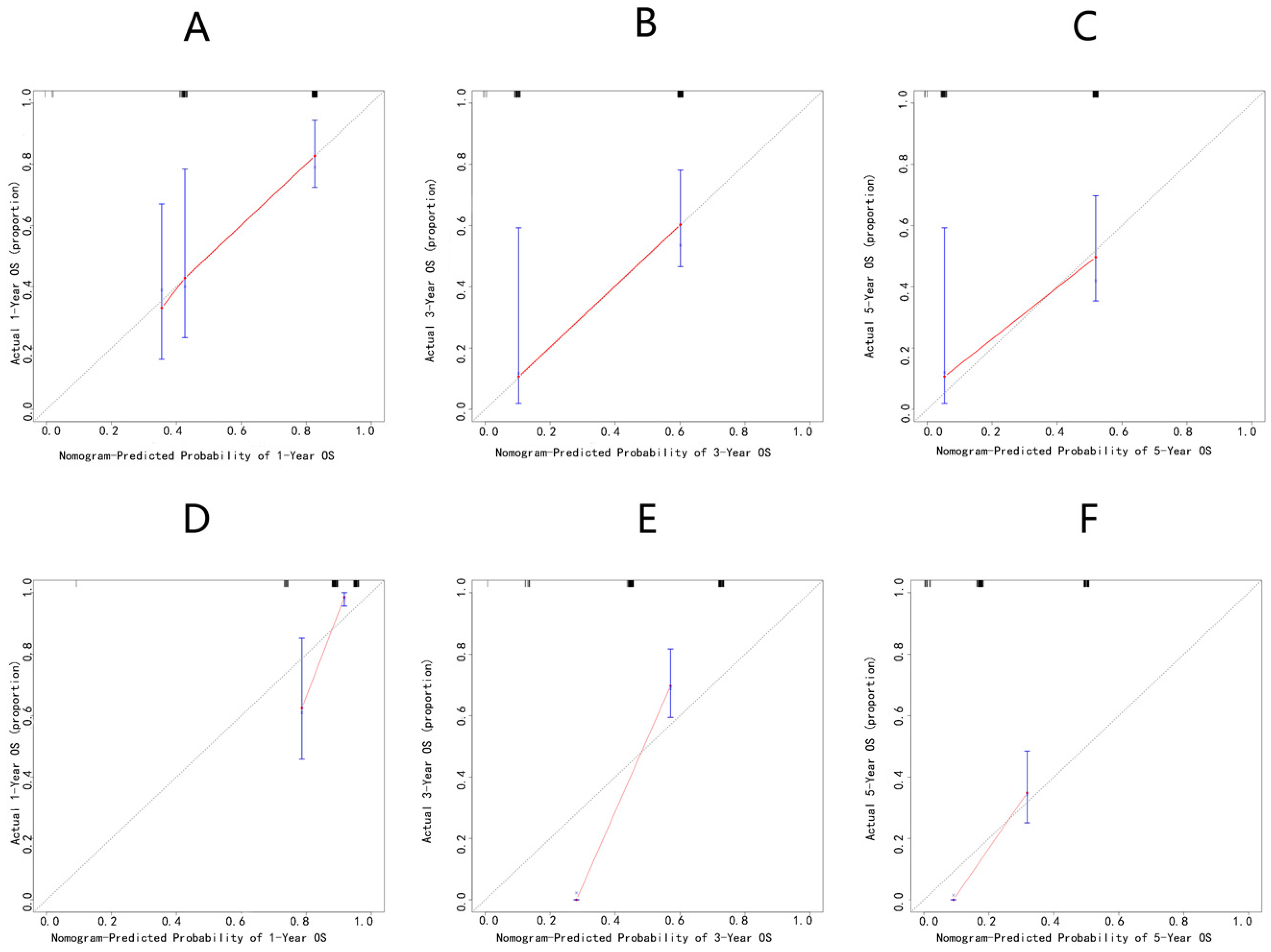
3.3. Development and Validation of the Initial Nomogram
3.4. Statistical Analysis of Prognostic Factors in Changzheng Cohort
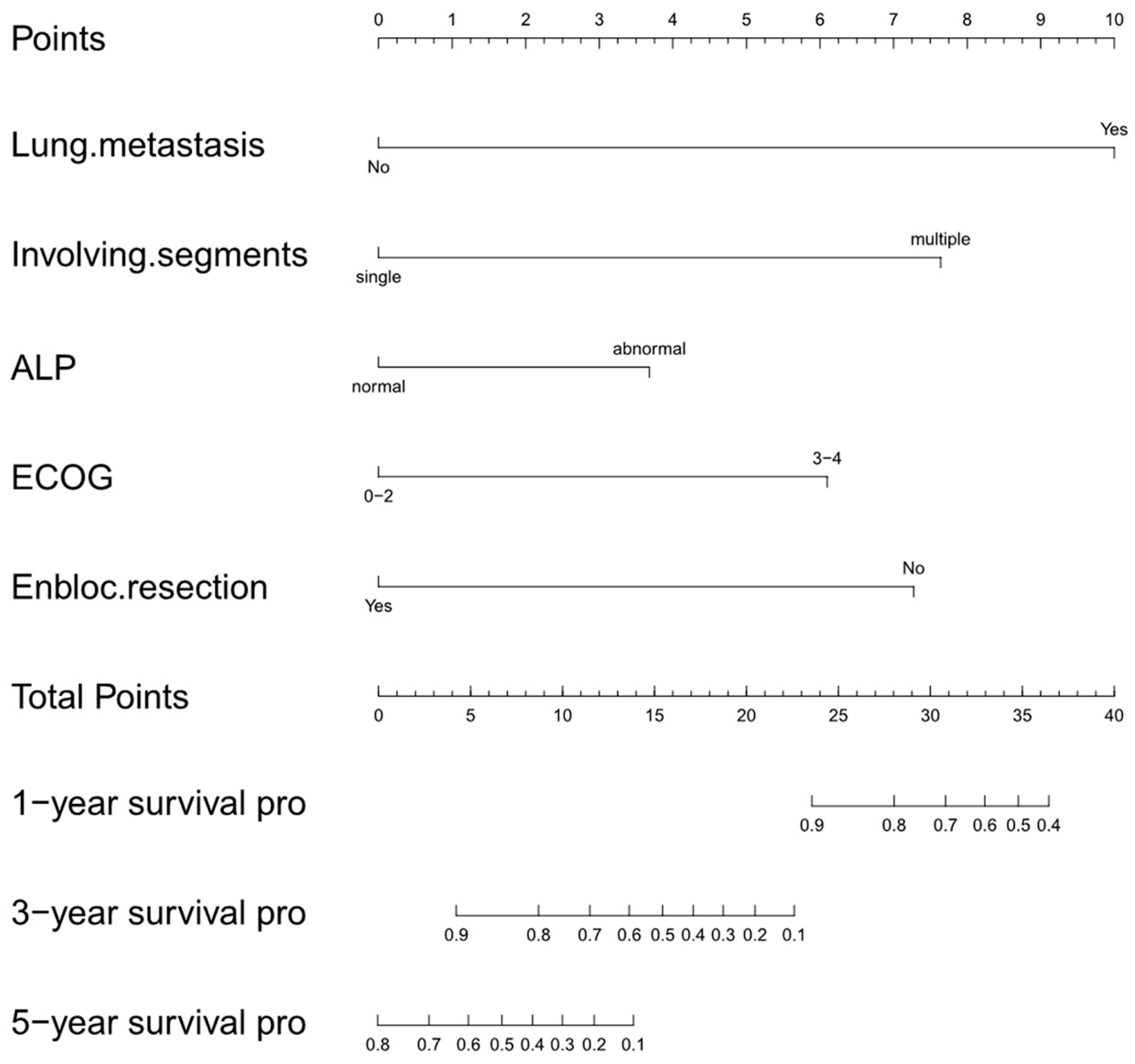
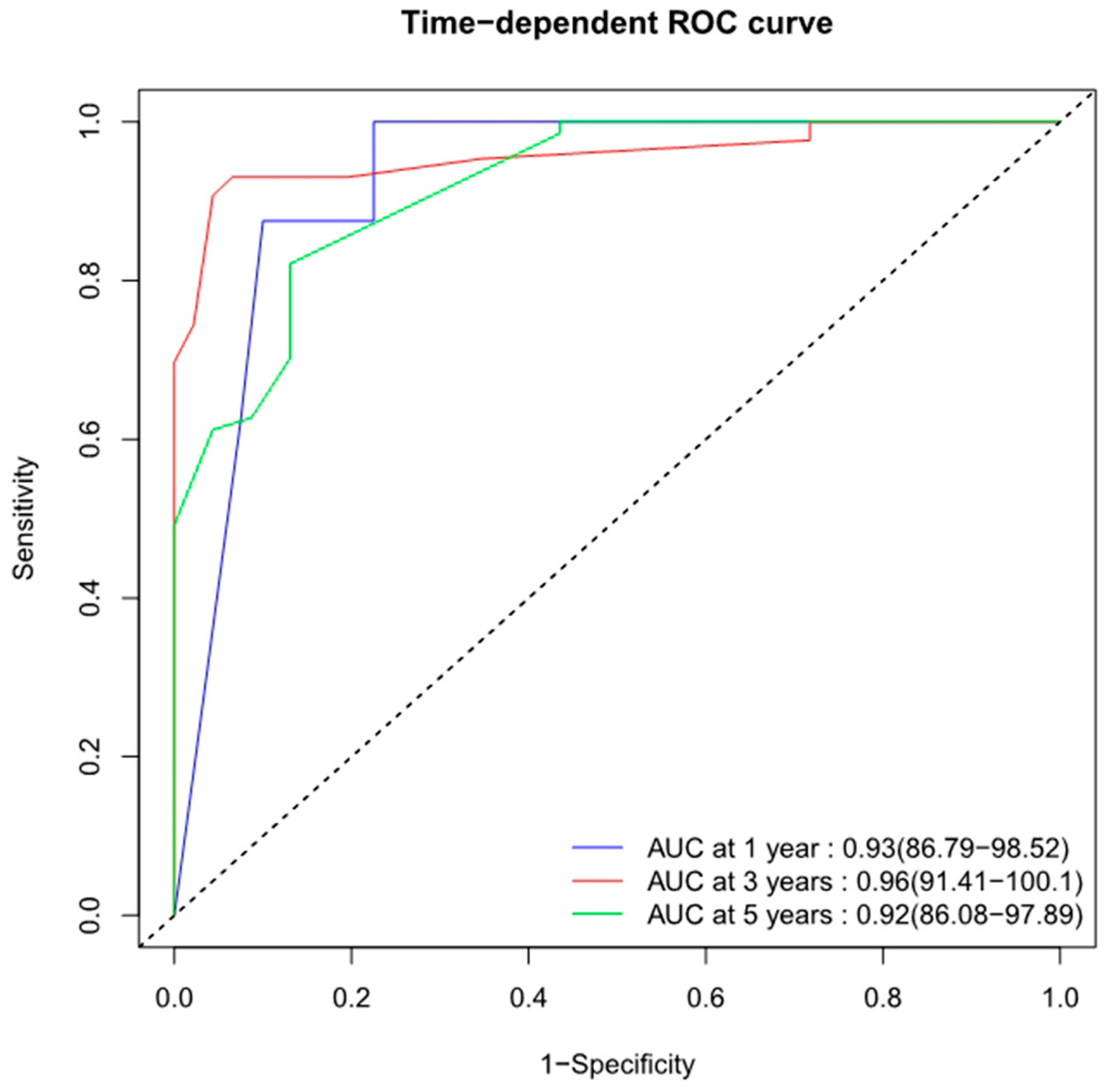
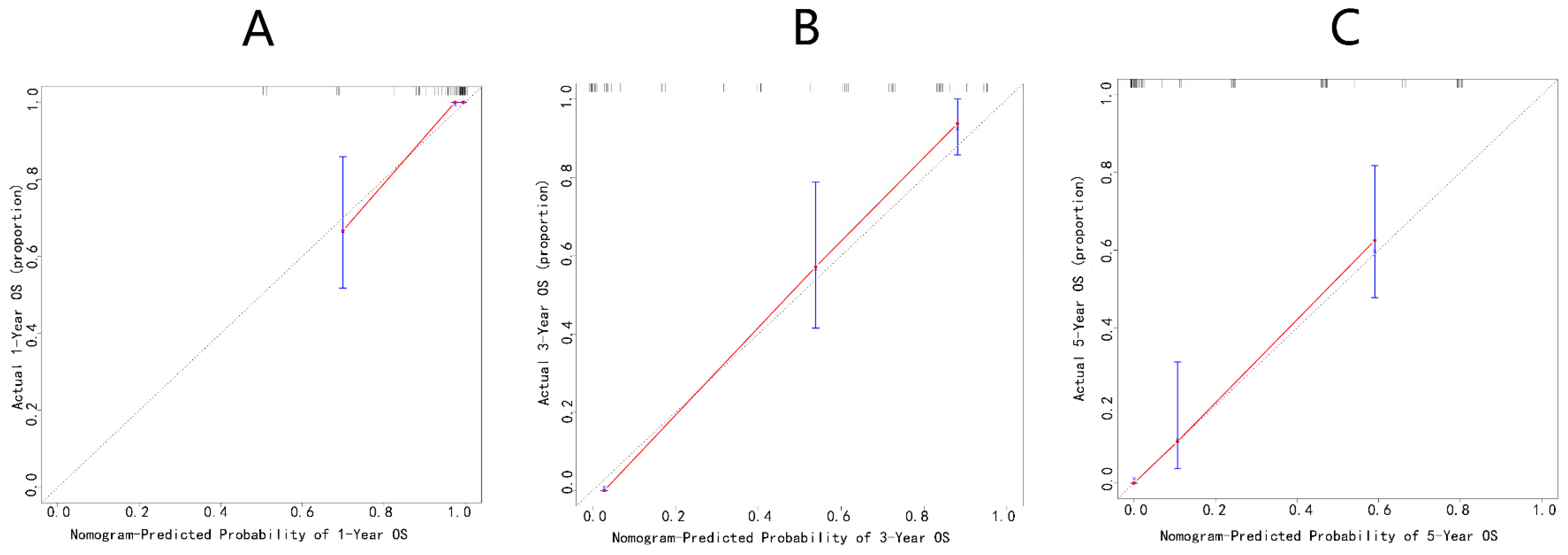
3.5. Development and Validation of Changzheng Nomogram
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barwick, K.W.; Huvos, A.G.; Smith, J. Primary osteogenic sarcoma of the vertebral column: A clinicopathologic correlation of ten patients. Cancer 1980, 46, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Fahey, M.; Spanier, S.S.; Vander Griend, R.A. Osteosarcoma of the pelvis. A clinical and histopathological study of twenty-five patients. J. Bone Jt. Surg. Am. 1992, 74, 321–330. [Google Scholar] [CrossRef]
- Ilaslan, H.; Sundaram, M.; Unni, K.K.; Shives, T.C. Primary vertebral osteosarcoma: Imaging findings. Radiology 2004, 230, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Mirabello, L.; Troisi, R.J.; Savage, S.A. Osteosarcoma incidence and survival rates from 1973 to 2004: Data from the Surveillance, Epidemiology, and End Results Program. Cancer 2009, 115, 1531–1543. [Google Scholar] [CrossRef]
- Shives, T.C.; Dahlin, D.C.; Sim, F.H.; Pritchard, D.J.; Earle, J.D. Osteosarcoma of the spine. J. Bone Jt. Surg. Am. 1986, 68, 660–668. [Google Scholar] [CrossRef]
- Raymond, A.K.; Jaffe, N. Osteosarcoma multidisciplinary approach to the management from the pathologist’s perspective. Cancer Treat Res. 2009, 152, 63–84. [Google Scholar]
- Ozaki, T.; Flege, S.; Kevric, M.; Lindner, N.; Maas, R.; Delling, G.; Schwarz, R.; von Hochstetter, A.R.; Salzer-Kuntschik, M.; Berdel, W.E.; et al. Osteosarcoma of the pelvis: Experience of the Cooperative Osteosarcoma Study Group. J. Clin. Oncol. 2003, 21, 334–341. [Google Scholar] [CrossRef]
- Schwab, J.; Gasbarrini, A.; Bandiera, S.; Boriani, L.; Amendola, L.; Picci, P.; Ferrari, S.; Boriani, S. Osteosarcoma of the mobile spine. Spine 2012, 37, E381–E386. [Google Scholar] [CrossRef]
- Zils, K.; Bielack, S.; Wilhelm, M.; Werner, M.; Schwarz, R.; Windhager, R.; Hofmann-Wackersreuther, G.; Andus, T.; Kager, L.; Kuehne, T.; et al. Osteosarcoma of the mobile spine. Ann. Oncol. 2013, 24, 2190–2195. [Google Scholar] [CrossRef]
- Guo, W.; Sun, X.; Ji, T.; Tang, X. Outcome of surgical treatment of pelvic osteosarcoma. J. Surg. Oncol. 2012, 106, 406–410. [Google Scholar] [CrossRef]
- Lefebvre, G.; Renaud, A.; Rocourt, N.; Cortet, B.; Ceugnart, L.; Cotten, A. Primary vertebral osteosarcoma: Five cases. Joint Bone Spine 2013, 80, 534–537. [Google Scholar] [CrossRef]
- Picci, P.; Sangiorgi, L.; Rougraff, B.T.; Neff, J.R.; Casadei, R.; Campanacci, M. Relationship of chemotherapy-induced necrosis and surgical margins to local recurrence in osteosarcoma. J. Clin. Oncol. 1994, 12, 2699–2705. [Google Scholar] [CrossRef]
- Chen, L.; Liu, X.; Li, M.; Wang, S.; Zhou, H.; Liu, L.; Cheng, X. A novel model to predict cancer-specific survival in patients with early-stage uterine papillary serous carcinoma (UPSC). Cancer Med. 2020, 9, 988–998. [Google Scholar] [CrossRef]
- Jiang, R.; He, S.; Sun, H.; Gong, H.; Yang, X.; Cai, X.; Wei, H.; Xiao, J. Identifying the Risk Factors and Estimating the Prognosis in Patients with Pelvis and Spine Ewing Sarcoma: A Population-Based Study. Spine 2021, 46, 1315–1325. [Google Scholar] [CrossRef]
- van den Hoven, I.; van Klaveren, D.; Verheuvel, N.C.; van la Parra, R.F.D.; Voogd, A.C.; de Roos, W.K.; Bosscha, K.; Heuts, E.M.; Tjan-Heijnen, V.C.G.; Roumen, R.M.H.; et al. Predicting the extent of nodal involvement for node positive breast cancer patients: Development and validation of a novel tool. J. Surg. Oncol. 2019, 120, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, D.; Xie, J.; Li, Y.; Wang, Y.; Li, C.; Xiang, J.; Zhang, Y.; Hu, H.; Sun, Y.; et al. Development and Validation of Web-Based Nomograms to Precisely Predict Conditional Risk of Site-Specific Recurrence for Patients With Completely Resected Non-small Cell Lung Cancer: A Multiinstitutional Study. Chest 2018, 154, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Wang, S.; Huang, L.; Wang, J.; Shi, D.; Li, Y.; Tong, T.; Peng, W. A clinical-radiomics nomogram for the preoperative prediction of lung metastasis in colorectal cancer patients with indeterminate pulmonary nodules. Eur. Radiol. 2019, 29, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Cates, J.M. Comparison of the AJCC, MSTS, and Modified Spanier Systems for Clinical and Pathologic Staging of Osteosarcoma. Am. J. Surg. Pathol. 2017, 41, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Jawad, M.U.; Haleem, A.A.; Scully, S.P. Malignant sarcoma of the pelvic bones: Treatment outcomes and prognostic factors vary by histopathology. Cancer 2011, 117, 1529–1541. [Google Scholar] [CrossRef]
- Fu, Y.; Lan, T.; Cai, H.; Lu, A.; Yu, W. Meta-analysis of serum lactate dehydrogenase and prognosis for osteosarcoma. Medicine 2018, 97, e0741. [Google Scholar] [CrossRef]
- Han, J.; Yong, B.; Luo, C.; Tan, P.; Peng, T.; Shen, J. High serum alkaline phosphatase cooperating with MMP-9 predicts metastasis and poor prognosis in patients with primary osteosarcoma in Southern China. World J. Surg. Oncol. 2012, 10, 37. [Google Scholar] [CrossRef] [PubMed]
- Shimose, S.; Kubo, T.; Fujimori, J.; Furuta, T.; Ochi, M. A novel assessment method of serum alkaline phosphatase for the diagnosis of osteosarcoma in children and adolescents. J. Orthop. Sci. 2014, 19, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Cates, J.M.M. Simple staging system for osteosarcoma performs equivalently to the AJCC and MSTS systems. J. Orthop. Res. 2018, 36, 2802–2808. [Google Scholar] [CrossRef]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A system for the surgical staging of musculoskeletal sarcoma. Clin. Orthop. Relat. Res. 1980, 153, 106–120. [Google Scholar] [CrossRef]
- Hart, R.A.; Boriani, S.; Biagini, R.; Currier, B.; Weinstein, J.N. A system for surgical staging and management of spine tumors. A clinical outcome study of giant cell tumors of the spine. Spine 1997, 22, 1773–1782; discussion 1783. [Google Scholar] [CrossRef] [PubMed]
- Tokuhashi, Y.; Matsuzaki, H.; Oda, H.; Oshima, M.; Ryu, J. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine 2005, 30, 2186–2191. [Google Scholar] [CrossRef]
- Tomita, K.; Kawahara, N.; Kobayashi, T.; Yoshida, A.; Murakami, H.; Akamaru, T. Surgical strategy for spinal metastases. Spine 2001, 26, 298–306. [Google Scholar] [CrossRef]
- McGirt, M.J.; Gokaslan, Z.L.; Chaichana, K.L. Preoperative grading scale to predict survival in patients undergoing resection of malignant primary osseous spinal neoplasms. Spine J. 2011, 11, 190–196. [Google Scholar] [CrossRef]
- Mukherjee, D.; Chaichana, K.L.; Gokaslan, Z.L.; Aaronson, O.; Cheng, J.S.; McGirt, M.J. Survival of patients with malignant primary osseous spinal neoplasms: Results from the Surveillance, Epidemiology, and End Results (SEER) database from 1973 to 2003. J. Neurosurg. Spine 2011, 14, 143–150. [Google Scholar] [CrossRef]
- Biermann, J.S.; Chow, W.; Reed, D.R.; Lucas, D.; Adkins, D.R.; Agulnik, M.; Benjamin, R.S.; Brigman, B.; Budd, G.T.; Curry, W.T.; et al. NCCN Guidelines Insights: Bone Cancer, Version 2.2017. J. Natl. Compr. Canc. Netw. 2017, 15, 155–167. [Google Scholar] [CrossRef]
- Schoenfeld, A.J.; Hornicek, F.J.; Pedlow, F.X.; Kobayashi, W.; Garcia, R.T.; DeLaney, T.F.; Springfield, D.; Mankin, H.J.; Schwab, J.H. Osteosarcoma of the spine: Experience in 26 patients treated at the Massachusetts General Hospital. Spine J. 2010, 10, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Hao, H.; Chen, L.; Huang, D.; Ge, J.; Qiu, Y.; Hao, L. Meta-analysis of alkaline phosphatase and prognosis for osteosarcoma. Eur. J. Cancer Care 2017, 26, e12536. [Google Scholar] [CrossRef] [PubMed]
- de Nigris, F.; Zanella, L.; Cacciatore, F.; De Chiara, A.; Fazioli, F.; Chiappetta, G.; Apice, G.; Infante, T.; Monaco, M.; Rossiello, R.; et al. YY1 overexpression is associated with poor prognosis and metastasis-free survival in patients suffering osteosarcoma. BMC Cancer 2011, 11, 472. [Google Scholar] [CrossRef]
- Zhu, K.-P.; Zhang, C.-L.; Hu, J.-P.; Zhang, L. A novel circulating hsa_circ_0081001 act as a potential biomarker for diagnosis and prognosis of osteosarcoma. Int. J. Biol. Sci. 2018, 14, 1513–1520. [Google Scholar]
- Zhu, K.-P.; Ma, X.-L.; Zhang, C.-L. Overexpressed circPVT1, a potential new circular RNA biomarker, contributes to doxorubicin and cisplatin resistance of osteosarcoma cells by regulating ABCB1. Int. J. Biol. Sci. 2018, 14, 321–330. [Google Scholar]
- Aoude, A.; Fortin, M.; Aldebeyan, S.; Ouellet, J.; Amiot, L.P.; Weber, M.H.; Jarzem, P. The revised Tokuhashi score; analysis of parameters and assessment of its accuracy in determining survival in patients afflicted with spinal metastasis. Eur. Spine J. 2018, 27, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Boriani, S.; Bandiera, S.; Biagini, R.; Bacchini, P.; Boriani, L.; Cappuccio, M.; Chevalley, F.; Gasbarrini, A.; Picci, P.; Weinstein, J.N. Chordoma of the mobile spine: Fifty years of experience. Spine 2006, 31, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Boriani, S.; De Iure, F.; Bandiera, S.; Campanacci, L.; Biagini, R.; Di Fiore, M.; Bandello, L.; Picci, P.; Bacchini, P. Chondrosarcoma of the mobile spine: Report on 22 cases. Spine 2000, 25, 804–812. [Google Scholar] [CrossRef]
- Boriani, S.; Bandiera, S.; Donthineni, R.; Amendola, L.; Cappuccio, M.; De Iure, F.; Gasbarrini, A. Morbidity of en bloc resections in the spine. Eur. Spine J. 2010, 19, 231–241. [Google Scholar] [CrossRef]
- Demura, S.; Kato, S.; Shinmura, K.; Yokogawa, N.; Shimizu, T.; Handa, M.; Annen, R.; Kobayashi, M.; Yamada, Y.; Murakami, H.; et al. Perioperative complications of total en bloc spondylectomy for spinal tumours. Bone Jt. J. 2021, 103-B, 976–983. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total n = 173 No. (%) | Training Cohort n = 83 No. (%) | Validation Cohort n = 90 No. (%) | p Value |
|---|---|---|---|---|
| Age (yrs, median, IQR) | 32 (19–55.5) | 42 (22–67) | 30 (18.75–47.25) | 0.003 * |
| Sex | 0.282 | |||
| female | 74 (43) | 39 (47) | 35 (39) | |
| male | 99 (57) | 44 (53) | 55 (61) | |
| Marital status | 0.069 | |||
| married | 77 (45) | 31 (37) | 46 (51) | |
| other | 96 (55) | 52 (63) | 44 (49) | |
| Race recode | <0.0001 * | |||
| black | 9 (5) | 9 (11) | 0 (0) | |
| white | 67 (39) | 67 (81) | 0 (0) | |
| other | 97 (56) | 7 (8) | 90 (100) | |
| Laterality | 0.225 | |||
| left | 64 (37) | 29 (35) | 35 (39) | |
| right | 68 (39) | 29 (35) | 39 (43) | |
| paired | 1 (1) | 1 (1) | 0 (0) | |
| not a paired | 40 (23) | 24 (29) | 16 (18) | |
| Grade | <0.0001 * | |||
| unknown | 17 (10) | 17 (21) | 0 (0) | |
| I | 10 (6) | 1 (1) | 9 (10) | |
| II | 52 (30) | 1 (1) | 51 (57) | |
| III and IV | 94 (54) | 64 (77) | 30 (33) | |
| T | <0.0001 * | |||
| Tx | 2 (1) | 2 (2) | 0 (0) | |
| T1 | 60 (35) | 29 (35) | 31 (34) | |
| T2 | 52 (30) | 46 (55) | 6 (7) | |
| T3 | 12 (7) | 2 (2) | 10 (11) | |
| T4 | 47 (27) | 4 (5) | 43 (48) | |
| N | 0.002 * | |||
| Nx | 6 (3) | 6 (7) | 0 (0) | |
| N0 | 147 (85) | 73 (88) | 74 (82) | |
| N1 | 20 (12) | 4 (5) | 16 (18) | |
| Tumor size (mm, median, IQR) | 70 (50.25–106.5) | 100 (65–130) | 58.5 (44.25–79.25) | <0.0001 * |
| Liver metastasis | 0.954 | |||
| no | 171 (99) | 82 (99) | 89 (99) | |
| yes | 2 (1) | 1 (1) | 1 (1) | |
| Lung metastasis | 0.566 | |||
| no | 130 (75) | 64 (77) | 66 (73) | |
| yes | 43 (25) | 19 (23) | 24 (27) | |
| Stage | 0.134 | |||
| localized | 45 (26) | 16 (19) | 29 (32) | |
| regional | 81 (47) | 41 (49) | 40 (44) | |
| distant | 47 (27) | 26 (32) | 21 (23) | |
| Surgery | <0.0001 * | |||
| no | 47 (27) | 41 (49) | 6 (7) | |
| yes | 126 (73) | 42 (51) | 84 (93) | |
| Radiotherapy | 0.129 | |||
| no/unknown | 124 (72) | 55 (66) | 69 (77) | |
| yes | 49 (28) | 28 (34) | 21 (23) | |
| Chemotherapy | <0.0001 * | |||
| no/unknown | 65 (38) | 16 (19) | 49 (54) | |
| yes | 108 (62) | 67 (81) | 41 (46) | |
| Vital status | <0.0001 * | |||
| alive | 36 (21) | 36 (43) | 0 (0) | |
| dead | 137 (79) | 47 (57) | 90 (100) | |
| Follow up (m, median, IQR) | 22 (11–52) | 14 (7–33) | 37.5 (20–61.25) | <0.0001 * |
| Characteristic | Number of Patients (%) | Characteristic | Number of Patients (%) |
|---|---|---|---|
| Demographics | ALP (u/L, median, IQR) | 175.5 (118.75–211.5) | |
| Age (yrs, median, IQR) | 30 (18.75–47.25) | LDH (u/L, median, IQR) | 231 (169.75–297.5) |
| Sex | Diabetes | ||
| female | 35 (39) | no | 83 (92) |
| male | 55 (61) | yes | 7 (8) |
| Marital status | Hypertension | ||
| married | 46 (51) | no | 77 (86) |
| other | 44 (49) | yes | 13 (14) |
| Clinical features | Hyperlipidemia | ||
| Laterality | no | 77 (86) | |
| left | 35 (39) | yes | 13 (14) |
| right | 39 (43) | Smoking history | |
| paired | 0 (0) | no | 74 (82) |
| not paired | 16 (18) | yes | 16 (18) |
| Grade | Family history | ||
| I | 9 (10) | no | 84 (93) |
| II | 51 (57) | yes | 6 (7) |
| III and IV | 30 (33) | Patient status | |
| T | Loss of weight | ||
| T1 | 31 (34) | <5 kg | 51 (57) |
| T2 | 6 (7) | ≥5 kg | 39 (43) |
| T3 | 10 (11) | Frankel | |
| T4 | 43 (48) | A–C | 42 (47) |
| N | D–E | 48 (53) | |
| N0 | 74 (82) | ECOG | |
| N1 | 16 (18) | 0–2 | 47 (52) |
| Liver metastasis | 3–4 | 43 (48) | |
| no | 89 (99) | VAS | |
| yes | 1 (1) | 0–6 | 34 (38) |
| Lung metastasis | 7–10 | 56 (62) | |
| no | 66 (73) | Treatment | |
| yes | 24 (27) | First intervention (m, median, IQR) | 4 (2–6.5) |
| Brain metastasis | Radiotherapy | ||
| no | 86 (96) | no | 69 (77) |
| yes | 4 (4) | yes | 21 (23) |
| Stage | Chemotherapy | ||
| localized | 29 (32) | no | 49 (54) |
| regional | 40 (44) | yes | 41 (46) |
| distant | 21 (23) | Surgery | |
| Medical information | no | 6 (7) | |
| Nature of lesions | yes | 84 (93) | |
| osteolytic | 24 (27) | En bloc resection | |
| osteoblastic | 43 (48) | no | 76 (84) |
| mixed | 23 (25) | yes | 14 (16) |
| Involving segments | Vital status | ||
| single | 61 (68) | alive | 0 (0) |
| multiple | 29 (32) | dead | 90 (100) |
| Tumor size (mm, median, IQR) | 58.5 (44.25–79.25) | Follow up (m, median, IQR) | 37.5 (20–61.25) |
| Prognostic | Univariate Analysis | Multivariate Analysis | |
|---|---|---|---|
| Factors | p Value | Hazard Ratio (95% CI) | p Value |
| Age (yrs) | 0.036 * | ||
| 0–24 | Reference | ||
| 25–59 | 1.129 (0.540–2.358) | 0.748 | |
| ≥60 | 1.499 (0.682–3.295) | 0.314 | |
| Race recode | 0.931 | ||
| black | |||
| white | |||
| other | |||
| Sex | 0.12 | ||
| female | |||
| male | |||
| Marital status | 0.478 | ||
| married | |||
| other | |||
| Laterality | 0.533 | ||
| left | |||
| right | |||
| paired | |||
| not a paired | |||
| Grade | 0.962 | ||
| unknown | |||
| I | |||
| II | |||
| III and IV | |||
| T | 0.913 | ||
| Tx | |||
| T1 | |||
| T2 | |||
| T3 | |||
| T4 | |||
| N | 0.262 | ||
| Nx | |||
| N0 | |||
| N1 | |||
| Liver metastasis | 0.004 * | ||
| no | Reference | ||
| yes | 17.201 (1.654–178.909) | 0.017 * | |
| Lung metastasis | <0.0001 * | ||
| no | Reference | ||
| yes | 3.047 (1.400–6.630) | 0.005 * | |
| Stage | 0.082 | ||
| localized | |||
| regional | |||
| distant | |||
| Tumor size | 0.64 | ||
| ≤80 mm | |||
| >80 mm | |||
| Surgery | 0.001 * | ||
| no | Reference | ||
| yes | 0.560 (0.282–1.113) | 0.098 | |
| Radiotherapy | 0.548 | ||
| no/unknown | |||
| yes | |||
| Chemotherapy | 0.001 * | ||
| no/unknown | Reference | ||
| yes | 0.296 (0.138–0.633) | 0.002 * |
| Prognostic Factors | Score |
|---|---|
| Liver metastasis | |
| no | 0 |
| yes | 10 |
| Lung metastasis | |
| no | 0 |
| yes | 4.5 |
| Chemotherapy | |
| no/unknown | 4.5 |
| yes | 0 |
| Prognostic | Univariate Analysis | Multivariate Analysis | |
|---|---|---|---|
| Factors | p Value | Hazard Ratio (95% CI) | p Value |
| Laterality | 0.396 | ||
| left | |||
| right | |||
| not paired | |||
| Grade | 0.002 * | ||
| I | Reference | ||
| II | 0.774 (0.333–1.801) | 0.552 | |
| III and IV | 1.383 (0.560–3.416) | 0.482 | |
| T | 0.077 | ||
| T1 | |||
| T2 | |||
| T3 | |||
| T4 | |||
| Liver metastasis | 1 | ||
| no | |||
| yes | |||
| Lung metastasis | <0.0001 * | ||
| no | Reference | ||
| yes | 3.673 (1.525–8.846) | 0.004 * | |
| Stage | <0.0001 * | ||
| localized | Reference | ||
| regional | 1.145 (0.616–2.129) | 0.668 | |
| distant | 2.110 (1.014–4.387) | 0.046 * | |
| Involving segments | <0.0001 * | ||
| single | Reference | ||
| multiple | 3.742 (1.802–7.770) | <0.0001 * | |
| ALP | <0.0001 * | ||
| normal | Reference | ||
| abnormal | 1.799 (1.043–3.105) | 0.035 * | |
| LDH | <0.0001 * | ||
| normal | Reference | ||
| abnormal | 1.442 (0.766–2.714) | 0.256 | |
| Smoking history | 0.389 | ||
| no | |||
| yes | |||
| Loss of weight | 0.002 * | ||
| <5 kg | Reference | ||
| ≥5 kg | 1.405 (0.823–2.402) | 0.213 | |
| Frankel | 0.815 | ||
| A–C | |||
| D–E | |||
| ECOG | <0.0001 * | ||
| 0–2 | Reference | ||
| 3–4 | 2.573 (1.373–4.822) | 0.003 * | |
| Radiotherapy | 0.952 | ||
| no | |||
| yes | |||
| Surgery | 0.004 * | ||
| no | Reference | ||
| yes | 0.396 (0.145–1.080) | 0.07 | |
| En bloc resection | <0.0001 * | ||
| no | Reference | ||
| yes | 0.400 (0.177–0.904) | 0.028 * |
| Prognostic Factors | Score |
|---|---|
| Lung metastasis | |
| no | 0 |
| yes | 10 |
| Involving segments | |
| single | 0 |
| multiple | 7.5 |
| ALP | |
| normal | 0 |
| abnormal | 3.5 |
| ECOG | |
| 0–2 | 0 |
| 3–4 | 6 |
| En bloc resection | |
| yes | 0 |
| no | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, D.; Liu, F.; Li, B.; Xu, J.; Gong, H.; Yang, M.; Wan, W.; Jiao, J.; Liu, Y.; Xiao, J. Development and Validation of a Prognostic Model for Overall Survival in Patients with Primary Pelvis and Spine Osteosarcoma: A Population-Based Study and External Validation. J. Clin. Med. 2023, 12, 2521. https://doi.org/10.3390/jcm12072521
Wang D, Liu F, Li B, Xu J, Gong H, Yang M, Wan W, Jiao J, Liu Y, Xiao J. Development and Validation of a Prognostic Model for Overall Survival in Patients with Primary Pelvis and Spine Osteosarcoma: A Population-Based Study and External Validation. Journal of Clinical Medicine. 2023; 12(7):2521. https://doi.org/10.3390/jcm12072521
Chicago/Turabian StyleWang, Da, Fanrong Liu, Binbin Li, Jinhui Xu, Haiyi Gong, Minglei Yang, Wei Wan, Jian Jiao, Yujie Liu, and Jianru Xiao. 2023. "Development and Validation of a Prognostic Model for Overall Survival in Patients with Primary Pelvis and Spine Osteosarcoma: A Population-Based Study and External Validation" Journal of Clinical Medicine 12, no. 7: 2521. https://doi.org/10.3390/jcm12072521
APA StyleWang, D., Liu, F., Li, B., Xu, J., Gong, H., Yang, M., Wan, W., Jiao, J., Liu, Y., & Xiao, J. (2023). Development and Validation of a Prognostic Model for Overall Survival in Patients with Primary Pelvis and Spine Osteosarcoma: A Population-Based Study and External Validation. Journal of Clinical Medicine, 12(7), 2521. https://doi.org/10.3390/jcm12072521