
Comparison of Early and Late Surgeries after Coronary Stent Implantation in Patients with Normal Preoperative Troponin Level: A Retrospective Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion and Exclusion Criteria
2.3. Data Acquisition
2.4. Outcomes and Follow-Up
2.5. Statistical Analysis
2.6. IPTW
2.7. Sample Size Calculation
3. Results
3.1. Demographics Data and Operative Characteristics
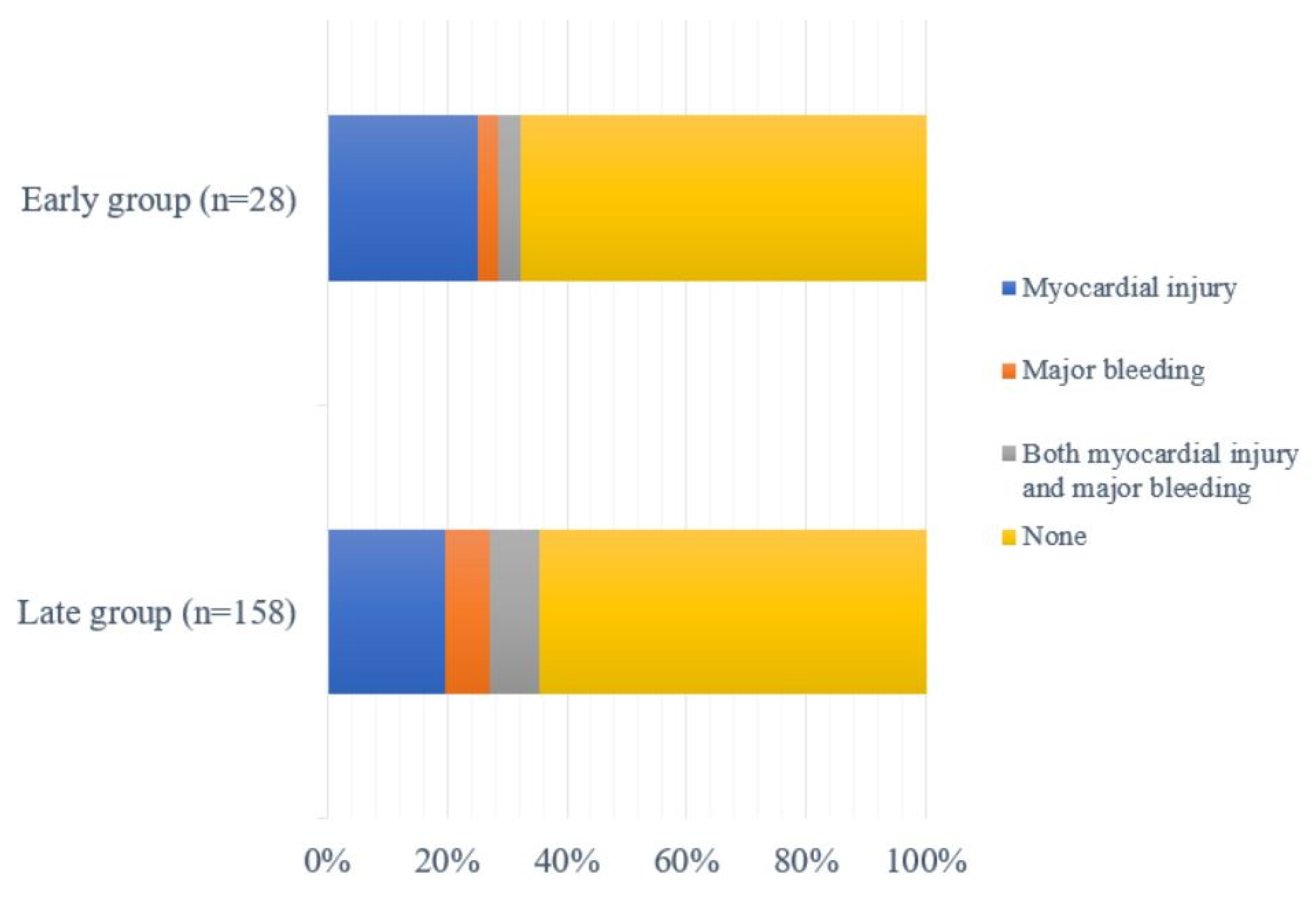
3.2. Myocardial Injury and Postoperative Complications
3.3. IPTW
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Weighted Cohort after IPTW | ||||
|---|---|---|---|---|
| Early Surgery (n = 28.3) | Late Surgery (n = 105.5) | p-Value | Test SMD | |
| Age, year | 66.91 (8.29) | 68.11 (8.25) | 0.533 | 0.145 |
| Female | 2.6 (9.3) | 5.4 (5.1) | 0.56 | 0.162 |
| BMI, kg/m2 | 25.10 (2.68) | 24.78 (3.18) | 0.637 | 0.112 |
| ASA PS ≥ IV | 28.3 (100.0) | 105.5 (100.0) | NA | <0.001 |
| Nonvascular surgery | 21.6 (76.3) | 82.0 (77.7) | 0.884 | 0.034 |
| Emergency surgery | 3.3 (11.6) | 6.4 (6.1) | 0.514 | 0.196 |
| Etiology of stent insertion, angina pectoris | 18.1 (63.7) | 70.3 (66.6) | 0.805 | 0.061 |
| Use of any antiplatelets | 28.3 (100.0) | 105.5 (100.0) | NA | <0.001 |
| Discontinued days of antiplatelets | 4.97 (3.74) | 3.70 (2.29) | 0.214 | 0.409 |
| Comorbidity | ||||
| Diabetus Melitus | 11.4 (40.1) | 40.9 (38.8) | 0.917 | 0.026 |
| Hypertension | 22.3 (78.7) | 71.0 (67.3) | 0.26 | 0.258 |
| Chronic kidney diseases | 1.3 (4.5) | 8.1 (7.6) | 0.605 | 0.131 |
| Preoperative atrial fibrillation | 1.3 (4.5) | 6.9 (6.5) | 0.728 | 0.087 |
| Peripheral vascular diseases | 4.6 (16.4) | 18.5 (17.5) | 0.899 | 0.030 |
| Stroke or TIA | 4.4 (15.4) | 18.9 (17.9) | 0.775 | 0.068 |
References
- Berger, P.B.; Kleiman, N.S.; Pencina, M.J.; Hsieh, W.H.; Steinhubl, S.R.; Jeremias, A.; Sonel, A.; Browne, K.; Barseness, G.; Cohen, D.J.; et al. Frequency of major noncardiac surgery and subsequent adverse events in the year after drug-eluting stent placement results from the EVENT (Evaluation of Drug-Eluting Stents and Ischemic Events) Registry. JACC Cardiovasc. Interv. 2010, 3, 920–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawn, M.T.; Graham, L.A.; Richman, J.S.; Itani, K.M.; Henderson, W.G.; Maddox, T.M. Risk of major adverse cardiac events following noncardiac surgery in patients with coronary stents. JAMA 2013, 310, 1462–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caplan, R.A.; Connis, R.T.; Nickinovich, D.G.; Riedel, B.J.; Fleisher, L.A.; Joshi, G.P. Practice alert for the perioperative management of patients with coronary artery stents: A report by the American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology 2009, 110, 22–23. [Google Scholar] [CrossRef] [Green Version]
- Vetter, T.R.; Short, R.T., 3rd; Hawn, M.T.; Marques, M.B. Perioperative management of the patient with a coronary artery stent. Anesthesiology 2014, 121, 1093–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2016, 68, 1082–1115. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Juni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [CrossRef]
- Mehta, S.R.; Bainey, K.R.; Cantor, W.J.; Lordkipanidze, M.; Marquis-Gravel, G.; Robinson, S.D.; Sibbald, M.; So, D.Y.; Wong, G.C.; Abunassar, J.G.; et al. 2018 Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology Focused Update of the Guidelines for the Use of Antiplatelet Therapy. Can. J. Cardiol. 2018, 34, 214–233. [Google Scholar] [CrossRef] [Green Version]
- Albaladejo, P.; Marret, E.; Samama, C.M.; Collet, J.P.; Abhay, K.; Loutrel, O.; Charbonneau, H.; Jaber, S.; Thoret, S.; Bosson, J.L.; et al. Non-cardiac surgery in patients with coronary stents: The RECO study. Heart 2011, 97, 1566–1572. [Google Scholar] [CrossRef]
- Hollis, R.H.; Graham, L.A.; Richman, J.S.; Deierhoi, R.J.; Hawn, M.T. Adverse cardiac events in patients with coronary stents undergoing noncardiac surgery: A systematic review. Am. J. Surg. 2012, 204, 494–501. [Google Scholar] [CrossRef]
- Cruden, N.L.; Harding, S.A.; Flapan, A.D.; Graham, C.; Wild, S.H.; Slack, R.; Pell, J.P.; Newby, D.E.; Scottish Coronary Revascularisation Register Steering, C. Previous coronary stent implantation and cardiac events in patients undergoing noncardiac surgery. Circ. Cardiovasc. Interv. 2010, 3, 236–242. [Google Scholar] [CrossRef] [Green Version]
- Rabbitts, J.A.; Nuttall, G.A.; Brown, M.J.; Hanson, A.C.; Oliver, W.C.; Holmes, D.R.; Rihal, C.S. Cardiac risk of noncardiac surgery after percutaneous coronary intervention with drug-eluting stents. Anesthesiology 2008, 109, 596–604. [Google Scholar] [CrossRef] [Green Version]
- Holcomb, C.N.; Graham, L.A.; Richman, J.S.; Rhyne, R.R.; Itani, K.M.; Maddox, T.M.; Hawn, M.T. The incremental risk of noncardiac surgery on adverse cardiac events following coronary stenting. J. Am. Coll. Cardiol. 2014, 64, 2730–2739. [Google Scholar] [CrossRef] [Green Version]
- Wijeysundera, D.N.; Wijeysundera, H.C.; Yun, L.; Wasowicz, M.; Beattie, W.S.; Velianou, J.L.; Ko, D.T. Risk of elective major noncardiac surgery after coronary stent insertion: A population-based study. Circulation 2012, 126, 1355–1362. [Google Scholar] [CrossRef] [Green Version]
- Egholm, G.; Kristensen, S.D.; Thim, T.; Olesen, K.K.; Madsen, M.; Jensen, S.E.; Jensen, L.O.; Sorensen, H.T.; Botker, H.E.; Maeng, M. Risk Associated With Surgery Within 12 Months After Coronary Drug-Eluting Stent Implantation. J. Am. Coll. Cardiol. 2016, 68, 2622–2632. [Google Scholar] [CrossRef]
- Thim, T.; Egholm, G.; Kristensen, S.D.; Olesen, K.K.W.; Madsen, M.; Jensen, S.E.; Jensen, L.O.; Sørensen, H.T.; Bøtker, H.E.; Maeng, M. Risk of Myocardial Infarction and Death After Noncardiac Surgery Performed Within the First Year After Coronary Drug-Eluting Stent Implantation for Acute Coronary Syndrome or Stable Angina Pectoris. Am. J. Cardiol. 2021, 160, 14–20. [Google Scholar] [CrossRef]
- Kaluza, G.L.; Joseph, J.; Lee, J.R.; Raizner, M.E.; Raizner, A.E. Catastrophic outcomes of noncardiac surgery soon after coronary stenting. J. Am. Coll. Cardiol. 2000, 35, 1288–1294. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.H.; Fasseas, P.; Orford, J.L.; Lennon, R.J.; Horlocker, T.; Charnoff, N.E.; Melby, S.; Berger, P.B. Clinical outcome of patients undergoing non-cardiac surgery in the two months following coronary stenting. J. Am. Coll. Cardiol. 2003, 42, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Schouten, O.; van Domburg, R.T.; Bax, J.J.; de Jaegere, P.J.; Dunkelgrun, M.; Feringa, H.H.; Hoeks, S.E.; Poldermans, D. Noncardiac surgery after coronary stenting: Early surgery and interruption of antiplatelet therapy are associated with an increase in major adverse cardiac events. J. Am. Coll. Cardiol. 2007, 49, 122–124. [Google Scholar] [CrossRef] [Green Version]
- van Kuijk, J.P.; Flu, W.J.; Schouten, O.; Hoeks, S.E.; Schenkeveld, L.; de Jaegere, P.P.; Bax, J.J.; van Domburg, R.T.; Serruys, P.W.; Poldermans, D. Timing of noncardiac surgery after coronary artery stenting with bare metal or drug-eluting stents. Am. J. Cardiol. 2009, 104, 1229–1234. [Google Scholar] [CrossRef] [PubMed]
- Vicenzi, M.N.; Meislitzer, T.; Heitzinger, B.; Halaj, M.; Fleisher, L.A.; Metzler, H. Coronary artery stenting and non-cardiac surgery--a prospective outcome study. Br. J. Anaesth. 2006, 96, 686–693. [Google Scholar] [CrossRef] [Green Version]
- Grines, C.L.; Bonow, R.O.; Casey, D.E., Jr.; Gardner, T.J.; Lockhart, P.B.; Moliterno, D.J.; O’Gara, P.; Whitlow, P. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: A science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation 2007, 115, 813–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anwaruddin, S.; Askari, A.T.; Saudye, H.; Batizy, L.; Houghtaling, P.L.; Alamoudi, M.; Militello, M.; Muhammad, K.; Kapadia, S.; Ellis, S.G. Characterization of post-operative risk associated with prior drug-eluting stent use. JACC Cardiovasc. Interv. 2009, 2, 542–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D. Third universal definition of myocardial infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.L.; Collins, G.S.; Spence, J.; Daurès, J.P.; Devereaux, P.J.; Landais, P.; Le Manach, Y. Double-adjustment in propensity score matching analysis: Choosing a threshold for considering residual imbalance. BMC Med. Res. Methodol. 2017, 17, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Waes, J.A.; Nathoe, H.M.; de Graaff, J.C.; Kemperman, H.; de Borst, G.J.; Peelen, L.M.; van Klei, W.A. Myocardial injury after noncardiac surgery and its association with short-term mortality. Circulation 2013, 127, 2264–2271. [Google Scholar] [CrossRef] [Green Version]
- Ruetzler, K.; Smilowitz, N.R.; Berger, J.S.; Devereaux, P.J.; Maron, B.A.; Newby, L.K.; de Jesus Perez, V.; Sessler, D.I.; Wijeysundera, D.N. Diagnosis and Management of Patients With Myocardial Injury After Noncardiac Surgery: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e287–e305. [Google Scholar] [CrossRef]
- Godet, G.; Le Manach, Y.; Lesache, F.; Perbet, S.; Coriat, P. Drug-eluting stent thrombosis in patients undergoing non-cardiac surgery: Is it always a problem? Br. J. Anaesth. 2008, 100, 472–477. [Google Scholar] [CrossRef] [Green Version]
- Helwani, M.A.; Amin, A.; Lavigne, P.; Rao, S.; Oesterreich, S.; Samaha, E.; Brown, J.C.; Nagele, P. Etiology of Acute Coronary Syndrome after Noncardiac Surgery. Anesthesiology 2018, 128, 1084–1091. [Google Scholar] [CrossRef]
- Wasowicz, M.; Syed, S.; Wijeysundera, D.N.; Starzyk, L.; Grewal, D.; Ragoonanan, T.; Harsha, P.; Travis, G.; Carroll, J.; Karkouti, K.; et al. Effectiveness of platelet inhibition on major adverse cardiac events in non-cardiac surgery after percutaneous coronary intervention: A prospective cohort study. Br. J. Anaesth. 2016, 116, 493–500. [Google Scholar] [CrossRef] [Green Version]
- Verbree-Willemsen, L.; Grobben, R.B.; van Waes, J.A.; Peelen, L.M.; Nathoe, H.M.; van Klei, W.A.; Grobbee, D.E. Causes and prevention of postoperative myocardial injury. Eur. J. Prev. Cardiol. 2019, 26, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Chin-Quee, S.L.; Hsu, S.H.; Nguyen-Ehrenreich, K.L.; Tai, J.T.; Abraham, G.M.; Pacetti, S.D.; Chan, Y.F.; Nakazawa, G.; Kolodgie, F.D.; Virmani, R.; et al. Endothelial cell recovery, acute thrombogenicity, and monocyte adhesion and activation on fluorinated copolymer and phosphorylcholine polymer stent coatings. Biomaterials 2010, 31, 648–657. [Google Scholar] [CrossRef]
- Lee, D.H.; de la Torre Hernandez, J.M. The Newest Generation of Drug-eluting Stents and Beyond. Eur. Cardiol. 2018, 13, 54–59. [Google Scholar] [CrossRef]
- Otsuka, F.; Vorpahl, M.; Nakano, M.; Foerst, J.; Newell, J.B.; Sakakura, K.; Kutys, R.; Ladich, E.; Finn, A.V.; Kolodgie, F.D.; et al. Pathology of second-generation everolimus-eluting stents versus first-generation sirolimus- and paclitaxel-eluting stents in humans. Circulation 2014, 129, 211–223. [Google Scholar] [CrossRef] [Green Version]
- Palmerini, T.; Biondi-Zoccai, G.; Della Riva, D.; Mariani, A.; Genereux, P.; Branzi, A.; Stone, G.W. Stent thrombosis with drug-eluting stents: Is the paradigm shifting? J. Am. Coll. Cardiol. 2013, 62, 1915–1921. [Google Scholar] [CrossRef] [Green Version]
- Kedhi, E.; Stone, G.W.; Kereiakes, D.J.; Serruys, P.W.; Parise, H.; Fahy, M.; Simonton, C.A.; Sudhir, K.; Sood, P.; Smits, P.C. Stent thrombosis: Insights on outcomes, predictors and impact of dual antiplatelet therapy interruption from the SPIRIT II, SPIRIT III, SPIRIT IV and COMPARE trials. EuroIntervention 2012, 8, 599–606. [Google Scholar] [CrossRef]
- Cornelissen, A.; Vogt, F.J. The effects of stenting on coronary endothelium from a molecular biological view: Time for improvement? J. Cell. Mol. Med. 2019, 23, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Sardu, C.; Paolisso, P.; Sacra, C.; Mauro, C.; Minicucci, F.; Portoghese, M.; Rizzo, M.R.; Barbieri, M.; Sasso, F.C.; D’Onofrio, N.; et al. Effects of Metformin Therapy on Coronary Endothelial Dysfunction in Patients With Prediabetes With Stable Angina and Nonobstructive Coronary Artery Stenosis: The CODYCE Multicenter Prospective Study. Diabetes Care 2019, 42, 1946–1955. [Google Scholar] [CrossRef] [Green Version]
- Marfella, R.; Sardu, C.; Balestrieri, M.L.; Siniscalchi, M.; Minicucci, F.; Signoriello, G.; Calabrò, P.; Mauro, C.; Pieretti, G.; Coppola, A.; et al. Effects of incretin treatment on cardiovascular outcomes in diabetic STEMI-patients with culprit obstructive and multivessel non obstructive-coronary-stenosis. Diabetol. Metab. Syndr. 2018, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Marfella, R.; Sardu, C.; Calabrò, P.; Siniscalchi, M.; Minicucci, F.; Signoriello, G.; Balestrieri, M.L.; Mauro, C.; Rizzo, M.R.; Paolisso, G.; et al. Non-ST-elevation myocardial infarction outcomes in patients with type 2 diabetes with non-obstructive coronary artery stenosis: Effects of incretin treatment. Diabetes Obes. Metab. 2018, 20, 723–729. [Google Scholar] [CrossRef]
- Paolisso, P.; Bergamaschi, L.; Gragnano, F.; Gallinoro, E.; Cesaro, A.; Sardu, C.; Mileva, N.; Foà, A.; Armillotta, M.; Sansonetti, A.; et al. Outcomes in diabetic patients treated with SGLT2-Inhibitors with acute myocardial infarction undergoing PCI: The SGLT2-I AMI PROTECT Registry. Pharmacol. Res. 2023, 187, 106597. [Google Scholar] [CrossRef]
- Paolisso, P.; Bergamaschi, L.; Santulli, G.; Gallinoro, E.; Cesaro, A.; Gragnano, F.; Sardu, C.; Mileva, N.; Foà, A.; Armillotta, M.; et al. Infarct size, inflammatory burden, and admission hyperglycemia in diabetic patients with acute myocardial infarction treated with SGLT2-inhibitors: A multicenter international registry. Cardiovasc. Diabetol. 2022, 21, 77. [Google Scholar] [CrossRef] [PubMed]
- Tokushige, A.; Shiomi, H.; Morimoto, T.; Furukawa, Y.; Nakagawa, Y.; Kadota, K.; Iwabuchi, M.; Shizuta, S.; Tada, T.; Tazaki, J.; et al. Incidence and outcome of surgical procedures after coronary bare-metal and drug-eluting stent implantation: A report from the CREDO-Kyoto PCI/CABG registry cohort-2. Circ. Cardiovasc. Interv. 2012, 5, 237–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossini, R.; Tarantini, G.; Musumeci, G.; Masiero, G.; Barbato, E.; Calabro, P.; Capodanno, D.; Leonardi, S.; Lettino, M.; Limbruno, U.; et al. A Multidisciplinary Approach on the Perioperative Antithrombotic Management of Patients With Coronary Stents Undergoing Surgery: Surgery After Stenting 2. JACC Cardiovasc. Interv. 2018, 11, 417–434. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Tantry, U.S.; Park, H.W.; Shin, E.S.; Geisler, T.; Gorog, D.A.; Gurbel, P.A.; Jeong, Y.H. Ethnic Difference of Thrombogenicity in Patients with Cardiovascular Disease: A Pandora Box to Explain Prognostic Differences. Korean Circ. J. 2021, 51, 202–221. [Google Scholar] [CrossRef]


| Variables | Early Surgery | Late Surgery | p |
|---|---|---|---|
| (n = 28) | (n = 158) | ||
| Age, year | 67.3 (8.1) | 68.3 (8.3) | 0.55 |
| Female | 1 (4) | 18 (12) | 0.32 |
| BMI, kg/m2 | 25.0 (2.6) | 24.6 (3.2) | 0.54 |
| Weight, kg | 68.7 (7.4) | 67.9 (10.6) | 0.71 |
| Height, cm | 165.8 (6.2) | 165.9 (7.5) | 0.91 |
| ASA PS | 0.06 | ||
| II | 7 (25) | 74 (47) | |
| III | 20 (71) | 81 (51) | |
| IV | 1 (4) | 3 (2) | |
| Hypertension | 18 (64) | 113 (72) | 0.44 |
| Diabetes mellitus | 11 (39) | 62 (39) | >0.99 |
| Metformin | 4 (14) | 28 (18) | |
| Sulfonylurea | 2 (7) | 21 (13) | |
| Dipeptidyl Peptidase-4 inhibitor | 3 (11) | 21 (13) | |
| Insulin | 1 (4) | 7 (4) | |
| Alpha glucosidase | 0 (0) | 2 (1) | |
| Thiazolidinediones | 1 (4) | 0 (0) | |
| No antidiabetic medication | 2 (7) | 5 (3) | |
| Stroke or transient ischemia attack | 5 (18) | 35 (22) | 0.61 |
| Chronic kidney disease | 1 (4) | 18 (11) | 0.32 |
| Structural heart disease a | 3 (11) | 21 (13) | >0.99 |
| Left ventricular ejection fraction < 30% | 0 (0) | 2 (1) | >0.99 |
| Atrial fibrillation | 2 (7) | 11 (7) | >0.99 |
| Peripheral vascular disease | 5 (18) | 27 (17) | >0.99 |
| Revised cardiac risk index | 0.74 | ||
| 0 | 2 (7) | 9 (6) | |
| 1 | 14 (55) | 91 (60) | |
| 2 | 9 (32) | 49 (31) | |
| 3 | 3 (11) | 9 (6) | |
| Serum creatinine ≥ 2.0 mg/dL | 1 (4) | 12 (8) | 0.70 |
| Hemoglobin, g/dL | 12.5 (1.9) | 12.7 (2.1) | 0.62 |
| CRP, mg/dL b | 0.13 (0.06, 0.71) | 0.25 (0.07,0.88) | 0.58 |
| NT-proBNP, ng/dL c | 88.2 (46.6, 715.0) | 148 (67.5, 503.4) | 0.75 |
| Albumin, g/dL | 4.0 (0.5) | 4.0 (0.5) | 0.59 |
| Cholesterol | 123.9 (37.1) | 134.8 (32.1) | 0.11 |
| LDL cholesterol d | 66.5 (25.7) | 75.3 (25.3) | 0.16 |
| Glucose, mg/dL | 136.8 (46.3) | 129.7 (53.9) | 0.52 |
| Surgery | |||
| Major vascular | 7 (25) | 39 (25) | 0.74 |
| Non major-vascular (sub-category, below) | 21 (75) | 119 (75.3) | |
| Cholecystectomy | 2 (7) | 16 (10) | |
| Gastrectomy | 5 (18) | 10 (7) | |
| Hepatobiliary | 1 (4) | 17 (11) | |
| Colorectal surgery | 2 (7) | 10 (6) | |
| Nephrectomy-cystectomy | 0 (0) | 2 (1) | |
| Kidney transplantation | 0 (0) | 2 (1) | |
| Liver transplantation | 0 (0) | 5 (3) | |
| Other abdominal surgery | 10 (36) | 62 (39) | |
| Thoracic surgery | 5 (18) | 21 (13) | |
| Carotid endarterectomy | 6 (21) | 36 (23) | |
| Emergency surgery | 3 (11) | 13 (8) | 0.71 |
| Intraoperative estimated blood loss, ml | 125 (80, 450) | 200 (100, 700) | 0.33 |
| Intraoperative transfusion | 4 (14) | 43 (27) | 0.15 |
| Surgery duration, min | 174.5 (117, 206) | 192 (122, 262) | 0.21 |
| Coronary stent data | |||
| Causes of coronary stent implantation | 0.99 | ||
| Acute Myocardial Injury | 9 (32) | 52 (33) | |
| Angina pectoris | 17 (61) | 94 (60) | |
| Not known | 2 (7) | 12 (7) | |
| Coronary stent type | 0.11 | ||
| DES | 16 (57) | 65 (41) | |
| First generation | 1 (6) | 26 (40) | |
| Durable polymer coated | 11 (69) | 29 (45) | |
| Biodegradable polymer coated | 2 (13) | 4 (6) | |
| Polymer free drug coated | 1 (6) | 0 (0) | |
| Unknown DES type | 1 (6) | 6 (9) | |
| BMS | 4 (14) | 14 (9) | |
| Unknown stent type | 8 (29) | 79 (50) | |
| Coronary stent numberb | 0.61 | ||
| 1 | 17 (63) | 76 (67) | |
| 2 | 7 (26) | 30 (27) | |
| 3 | 3 (11) | 7 (6) | |
| Coronary stent siteb | 0.10 | ||
| Left anterior descending | 16 (57) | 62 (39) | |
| Antiplatelets (or anticoagulants) use | <0.001 | ||
| None | 0 (0) | 3 (2) | |
| Aspirin only | 1 (4) | 70 (44) | |
| Clopidogrel only | 0 (0) | 22 (14) | |
| Dual (aspirin + clopidogrel) | 27 (96) | 60 (38) | |
| Warfarin | 0 (0) | 3 (2) | |
| Discontinued days of any antiplatelets (or anticoagulants) | 3.4 (3.1) | 4.4 (4.0) | 0.25 |
| Variables | Unmatched Cohort | Weighted Cohort after IPTW | ||||||
|---|---|---|---|---|---|---|---|---|
| Early Surgery (n = 28) | Late Surgery (n = 158) | Odds Ratio (95% CI) a | p | Early Surgery (n = 28.3) | Late Surgery (n = 105.5) | Odds Ratio (95% CI) b | p | |
| Myocardial injury | 8 (28.6) | 44 (27.8) | 1.067 (0.404, 2.482) | 0.886 | 8.8 (31.1) | 32.5 (30.8) | 1.035 (0.400, 2.447) | 0.939 |
| Myocardial infarction | 0 (0) | 9 (5.7) | 0.276 (0.000, 2.276) | 0.398 | 0.0 (0.0) | 6.9 (6.6) | 0.232 (0.000, 1.995) | 0.330 |
| MACE | 3 (10.7) | 23 (14.6) | 0.791 (0.159, 2.367) | 0.707 | 3.3 (11.8) | 17.4 (16.5) | 0.748(0.163, 2.251) | 0.636 |
| In-stent thrombosis | 0 | 0 | NA | NA | 0 | 0 | NA | NA |
| Emergent coronary revascularization | 0 (0) | 2 (1.3) | 1.098 (0.000, 13.648) | 0.953 | 0.0 (0.0) | 1.9 (1.8) | 0.746 (0.000, 9.460) | 0.854 |
| Major bleeding | 2 (7.1) | 25 (15.8) | 0.494 (0.064, 1.645) | 0.319 | 0.8 (3.0) | 18.1 (17.1) | 0.227 (0.006, 1.014) | 0.113 |
| Stroke | 0 (0) | 3 (1.9) | 0.779 (0.000, 8.248) | 0.872 | 0.0 (0.0) | 1.9 (1.8) | 0.758 (0.000, 9.711) | 0.862 |
| Thrombosis | 1 (3.6) | 4 (2.5) | 1.873 (0.072, 10.547) | 0.522 | 0.8 (3.0) | 2.8 (2.6) | 1.516 (0.038, 10.540) | 0.695 |
| Heart failure | 2 (7.1) | 7 (4.4) | 1.906 (0.239, 7.607) | 0.403 | 2.5 (8.8) | 5.6 (5.3) | 1.892 (0.300, 7.697) | 0.394 |
| Newly onset atrial fibrillation or flutter | 1 (3.6) | 13 (8.2) | 0.588 (0.022, 2.566) | 0.555 | 0.8 (3.0) | 10.5 (10.0) | 0.416 (0.010, 1.973) | 0.358 |
| New dialysis | 0 (0) | 3 (1.9) | 0.779 (0.000, 8.248) | 0.872 | 0.0 (0.0) | 2.2 (2.1) | 0.672 (0.000, 8.063) | 0.801 |
| Clavien-Dindo surgical complications ≥ 1 | 7 (25.0) | 58 (36.7) | 0.599 (0.215, 1.408) | 0.268 | 5.5 (19.3) | 39.7 (37.6) | 0.423 (0.132, 1.069) | 0.090 |
| Postoperative hospital stay, days | 12.5 (17.9) | 11.1 (14.7) | 1.449 (-4.664, 7.562) | 0.642 | 10.90 (16.68) | 10.15 (12.13) | 0.750 (-4.813, 6.312) | 0.792 |
| In-hospital mortality | 0 (0) | 1 (0.6) | 1.842 (0.000, 58.189) | 0.714 | 0.0 (0.0) | 1.0 (1.0) | 1.208 (0.000, 32.219) | 0.910 |
| Univariable Analysis | Multiple Logistic Regression | |||||
|---|---|---|---|---|---|---|
| Myocardial Injury (n = 52) | No Myocardial Injury (n = 134) | OR, 95% CI | p Value | aOR, 95% CI | p Value | |
| Early surgery | 8 (15.4) | 20 (14.9) | 1.034 (0.418, 2.558) | 0.937 | 1.249 (0.478, 3.262) | 0.65 |
| Age, year | 70.0 (9.5) | 67.4 (7.7) | 1.045 (1.004, 1.089) | 0.033 | ||
| BMI, kg/m2 | 24.9 (3.5) | 24.6 (3.0) | 1.032 (0.926, 1.150) | 0.568 | ||
| Female | 9 (17.3) | 11 (8.2) | 2.595 (0.964, 6.985) | 0.059 | 2.749 (0.969, 7.795) | 0.057 |
| Surgery type | 25 (48.1) | 21 (15.7) | 5.010 (2.399, 10.464) | <0.001 | 5.060 (2.407, 10.635) | <0.001 |
| Major vascular surgery | ||||||
| Emergency surgery | 4 (7.7) | 12 (9.0) | 0.919 (0.274, 3.079) | 0.891 | ||
| ASA PS | ||||||
| II | 21 (40.4) | 60 (44.8) | (ref) | |||
| III | 30 (57.7) | 71 (53.0) | 1.100 (0.562, 2.154) | 0.780 | ||
| IV | 1 (1.9) | 3 (2.2) | 0.810 (0.080, 8.234) | 0.858 | ||
| Etiology of stent insertion | ||||||
| AMI | 16 (31.4) | 45 (37.2) | (ref) | |||
| Angina pectoris | 35 (68.6) | 76 (62.8) | 1.301 (0.646, 2.618) | 0.461 | ||
| Unknown | 1 (1.0) | 13 (1.0) | NA | |||
| DM | 15 (28.8) | 58 (43.3) | 0.529 (0.262, 1.069) | 0.076 | ||
| Metformin | 5 (9.6) | 28 (20.9) | 0.403 (0.146, 1.108) | 0.078 | ||
| Sulfonylurea | 3 (5.8) | 21 (15.7) | 0.330 (0.094, 1.156) | 0.083 | ||
| DPP-4-inhibitor | 4 (7.7) | 20 (14.9) | 0.475 (0.154, 1.464) | 0.195 | ||
| HTN | 35 (67.3) | 96 (71.6) | 0.777 (0.383, 1.575) | 0.483 | ||
| CKD | 10 (19.2) | 9 (6.7) | 3.398 (1.190, 9.706) | 0.022 | 2.583 (0.893, 7.468) | 0.08 |
| Atrial fibrillation | 4 (7.7) | 9 (6.7) | 1.170 (0.336, 4.076) | 0.805 | ||
| Peripheral vascular diseases | 10 (19.2) | 22 (16.4) | 0.990 (0.418, 2.341) | 0.981 | ||
| Any stroke or TIA | 7 (13.5) | 33 (24.6) | 0.409 (0.158, 1.057) | 0.065 | ||
| Preoperative antiplatelets | ||||||
| None | 1 (1.9) | 2 (1.5) | (ref) | |||
| Dual antiplatelets | 26 (50.0) | 61 (46.5) | <0.001 (0, Infinite) | 0.981 | ||
| Single antiplatelet | 25 (48.1) | 71 (53.0) | <0.001 (0, Infinite) | 0.986 | ||
| Discontinued days of antiplatelets | 4 (1,5) | 4 (1,5) | 0.931 (0.839, 1.034) | 0.182 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.H.; Lee, E.K.; Ahn, H.J.; Lee, S.M.; Kim, J.A.; Yang, M.; Choi, J.W.; Kim, J.; Jeong, H.; Kim, S.; et al. Comparison of Early and Late Surgeries after Coronary Stent Implantation in Patients with Normal Preoperative Troponin Level: A Retrospective Study. J. Clin. Med. 2023, 12, 2524. https://doi.org/10.3390/jcm12072524
Lee SH, Lee EK, Ahn HJ, Lee SM, Kim JA, Yang M, Choi JW, Kim J, Jeong H, Kim S, et al. Comparison of Early and Late Surgeries after Coronary Stent Implantation in Patients with Normal Preoperative Troponin Level: A Retrospective Study. Journal of Clinical Medicine. 2023; 12(7):2524. https://doi.org/10.3390/jcm12072524
Chicago/Turabian StyleLee, Sang Hyun, Eun Kyung Lee, Hyun Joo Ahn, Sangmin M. Lee, Jie Ae Kim, Mikyung Yang, Ji Won Choi, Jeayoun Kim, Heejoon Jeong, Seungmo Kim, and et al. 2023. "Comparison of Early and Late Surgeries after Coronary Stent Implantation in Patients with Normal Preoperative Troponin Level: A Retrospective Study" Journal of Clinical Medicine 12, no. 7: 2524. https://doi.org/10.3390/jcm12072524
APA StyleLee, S. H., Lee, E. K., Ahn, H. J., Lee, S. M., Kim, J. A., Yang, M., Choi, J. W., Kim, J., Jeong, H., Kim, S., Kim, J., & Ahn, J. (2023). Comparison of Early and Late Surgeries after Coronary Stent Implantation in Patients with Normal Preoperative Troponin Level: A Retrospective Study. Journal of Clinical Medicine, 12(7), 2524. https://doi.org/10.3390/jcm12072524