Abstract
The objective of this clinical study was to collect short-term endodontic outcomes of endodontic-treated teeth (ETT) obturated with different kinds of bioceramic sealers used in combination with warm gutta-percha obturation techniques. Methods: A total of 210 endodontic treatments in 168 patients were performed. At baseline, 155 sample teeth (73.8%) showed symptoms (tenderness or pain to percussion) and 125 (59.5%) showed periapical radiolucency. Periapical radiolucency was present in 125 cases (59.5%); of these, 79 showed a lesion of 5 mm or bigger (63.2%) while lower than 5 mm in 46 cases (36.8%). Regarding ETT with radiolucency, 105 of them (84%) were in coincidence with their need for retreatment and the other 20 (16%) were necrotic teeth. The obturation techniques that were used in this study were: the continuous wave of condensation technique in 75% of cases, and carrier-based technique in 25%. Four bioceramic sealers were used: CeraSeal in 115 cases, BioRoot in 35 cases, AH Plus Bio in 40 cases, and in 20 cases, BIO-C SEALER ION. Preoperative and recall radiographs of the roots were each assigned a periapical index (PAI) score by 2 blinded, independent, and calibrated examiners. The teeth were divided into outcome categories based on the following classification: healed, unhealed, and healing. The healed and healing categories were classified as success, and the unhealed category was classified as failure on the basis of loose criteria. Minimum follow-up period was 18 months. Results: The overall success rate was 99%, with 73.3% healed, 25.7% healing, and 0.95% not healed. The success rate was 100% for initial treatment and 98.2% for retreatment. Fifty-four (N = 54) teeth showed ongoing healing. All of them were retreatment cases with periapical lesions. Regarding the success (healed and healing) versus not healed, no significant difference was found between teeth with or without periapical lesions (p < 0.05). A statistically significant difference in the distribution of healed, healing, and not-healed teeth was found between the groups of teeth with baseline lesions < 5 mm and >5 mm in diameter (p < 0.01) and those with sealer groups (p < 0.01). The success rate of used bioceramic sealers was not statistically significant different (99.1%, 100%, 97.5% and 100%, respectively, for CeraSeal, BioRoot, AH Plus Bio, and BIO-C SEALER ION). Nonetheless, the distribution of healed, healing, and not-healed teeth was different between teeth sealed with different materials (p < 0.01). From the findings of this clinical study, the following conclusion can be drawn: a correct filling of root canals made with warm gutta-percha technique combined with a bioceramic sealer allows a high success rate in endodontically treated teeth.
1. Introduction
Bioceramic sealers (BS), also known as calcium silicate-based endodontic sealers, were introduced in dentistry and their mechanical, chemical, and biological properties were studied [1,2,3,4,5]. They were launched into the dental market and their popularity progressively increased among endodontists and dental practitioners. BS cements were first used to repair root perforation and in surgical endodontics as retro filling materials [6]. A fine formulation of these materials was made available and BS are now recognized as very useful in endodontic therapy. The BS are placed into the root canal using an easy technique and thanks to the filler size less than two microns, they can penetrate into the dentinal tubules sealing them. Additionally, BS can create a chemical bond with dental substrates and are sufficiently radiopaque [7,8,9] and have antibacterial properties [10,11,12]. Additionally, BS showed to be osteoinductive and biocompatible: these characteristics might help in bone regeneration of periapical lesions [13,14]. Because of their biocompatibility and intrinsic osteoinductive capacity, when an overfill happens, an inflammatory response will not take place and during hardening, when they come in contact with tissue fluids, calcium hydroxide reacts with phosphatase enzymes, resulting in the formation of hydroxyapatite [15]. Regarding their capacity to seal the apex, no significant differences were found in the quality of obturation when single-cone, warm condensation, and carrier-based techniques using bioceramic sealers were used [16,17]. Although the single cone technique needs a large amount of cement, and that can have voids and bubbles within the sealer itself, it was advocated as the main obturation technique in combination with BS [18]. Another aspect that supported combining the single cone technique with BS was that these materials should be used without the heat in order to not accelerate their setting [19,20]. Moreover, their hydraulic capability to penetrate into the dentinal tubules can enhance the retention of the sealer and create a mechanical barrier able to prevent bacteria leakage [7].
The long-term success of endodontic treatments is based on adequate 3-dimensional (3D) cleaning, shaping, and 3-dimensional obturation of the complex root canal system [21,22]. The role of endodontic sealers in combination with different types of endodontic obturation techniques was investigated and BS were proposed into the market as indicated only in combination with single-cone technique because the BS are unadvisable to come into contact with heat [19,23,24]. Otherwise, they can harden instantly. However, a recent study evaluated the use of several BS in combination with warm gutta-percha techniques, showing promising results [16].
Predictable and reliable results may be obtained only with clinical trials. Clinical trials are much more reliable than in laboratory studies made in both retrospective and prospective ways [25,26]. When a prospective clinical trial is made, only a few specific parameters are evaluated in a limited number of specimens and they take place in specialized centers. Through a retrospective study, a wider number of specimens can be collected and it may reflect more the clinical behavior of practitioners. The objective of this study was to evaluate outcomes of endodontically treated teeth (ETT) obturated with BS used in combination with warm gutta-percha obturation techniques.
The tested null hypotheses were: (1) there was no difference in the endodontic success of different BS; (2) there was no difference in the endodontic success of ETT with periapical lesions showing different sizes of the lesion (more or less than 5 mm); (3) there was no difference in the endodontic success of ETT with and without extrusion of BS; (4) there was no difference in the endodontic success of ETT of initial vs. retreated teeth.
2. Materials and Methods
Over 1 year (March 2020 to March 2021), one expert operator (DP) made 210 endodontic treatments in 168 patients (85 men, 83 women; age range: 19 to 81 years; media: 61 years). Patients required different endodontic therapies. Consecutive patients were selected from the authors’ offices. The size of the sample was calculated with a margin of error of 5%, and a confidence level of 95%, accordingly, with a population size of 500 of patients in need of endodontic treatment. Then, it was decided to include in this survey only primary endodontic-treated teeth or nonsurgical retreatments (112 of nonsurgical retreatments and 98 of primary endodontic treatments) with a follow-up of at least 18 months or longer (mean follow up 19.7 months) and all patients, after being endodontically treated, were placed in a recall periodical program of oral hygiene from the beginning of 2022.
The clinical protocol was performed in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All patients were informed and provided their written consent. The study was approved by the Ethical Committee of the University of Siena (protocol code PR001; data of approval 21 October 2019).
Inclusion criteria were the following: periodontally healthy or successfully treated patients in need of one or more endodontic treatments.
Exclusion criteria were the following: patients with an age lower than 18 years, pregnancy, disabilities, previous prosthodontic restorations of abutment teeth, deep bone defects, pulp capping, heavy occlusal contacts or history of bruxism, systemic disease or severe medical complications, allergic history concerning methacrylates, high incidence of caries, xerostomia, and lack of compliance.
A total of 210 teeth were collected and of them, 100 were maxillary posteriors (47.6%), 73 mandibular posteriors (34.7%), and 37 anterior teeth (17.7%), uppers and lowers; 85 ETT belonged to the mandible (40.5%) and 125 (59.5%) to maxillae.
At baseline, 155 sample teeth (73.8%) showed symptoms (tenderness/pain to percussion) and 125 (59.5%) had periapical radiolucency and of these, 79 showed a lesion of 5 mm or bigger (63.2%), while 46 showed a lesion smaller than 5 mm (36.8%). Regarding ETT with radiolucency, 105 of them (84%) were in need for retreatment and the other 20 (16%) were necrotic teeth.
The performed obturation techniques were the continuous wave of condensation technique in 158 cases (75%) and the carrier-based technique in 52 (25%), mainly in presence of very curved and narrow canals. All obturations were performed using a bioceramic sealer. Four BS were randomly selected accordingly with their availability: CeraSeal (Sweden & Martina, Due Carrare PD, Italy) in 115 cases (54.5%), BioRoot (Septodont, Saint Mour des Fousses, France) in 35 cases (16.7%), AH Plus Bio (Dentsply, Kostanz, Germany) in 40 cases (19%), and in 20 cases, (9.5%) BIO-C SEALER ION+ (Angelus, Londrina, Brasil).
Table 1 reports demographic characteristics of the patient.

Table 1.
Population demographics and type of treatment. (PARL, periapical radiolucency; RCT, root canal treatment; ReTx, retreatment).
The following preoperative data were recorded for each case: demographic data, tooth location, number of root canals, previous endodontic treatment, clinical signs and symptoms, vitality tests, and radiographic periapical status. Based on these findings, the preoperative condition was classified as one of the following: vital, non-vital, previously endodontically treated, with or without periapical lesion, and symptomatic or asymptomatic.
For each tooth, the following intra-operative data were written in the clinical records: how many appointments were needed to complete the treatment, presence of complications such as perforation, breakage of files and flare-up; length of canal filling (at apical level, 1 mm short or more and beyond). The endodontic and restorative procedures were performed accordingly with Pontoriero et al. [27]. Finally, the roots were obturated with gutta-percha cones and one of the four bioceramic sealers tested following a continuous wave of condensation technique (75%) or a carrier-based technique (Thermafil, Dentsply, Konstanz, Germany) depending on the root canal anatomy.
The build-up and restorative procedures were performed as described by Pontoriero et al. [27].
Postoperatively, the same preoperative data were collected also accordingly with Pontoriero et al. [27] and the evaluation parameters made by the European Society of Endodontology 2006 [28] were followed. The primary authors (DP) made all the visits at the follow-ups.
The entity of the lesion was recorded and evaluated. Consequently, endodontic treatments were classified as failures when pain was present, and/or swelling and sinus tract. Radiographically, a lesion appeared after endodontic treatment, when a pre-existing lesion increased in size, and when a lesion remained the same, it was considered as failure [29]. Additionally, preoperatively and at each recall, the Periapical Index (PAI) score system was used [30,31] by 2 blinded, independent, and calibrated examiners (D. P., M.F.) and each endodontically treated tooth received the highest score for any of the roots.
The treated roots were classified as the following [32]:
- Healed: teeth in good function, without symptoms and without radiographic periapical lesion;
- Not healed: nonfunctional teeth with symptoms with or without radiographic periapical lesion or teeth without symptoms with unchanged, new, or enlarged radiographic periapical lesion;
- Healing: teeth that are without symptoms and good function, with a decreased size of radiographic periapical lesion.
The clinical evaluation ‘success’ was referred to healed and healing categories and ‘failure’ to the not-healed teeth was classified as failure. Figure 1 show examples of each category. When a disagreement on the radiographic and/or clinical evaluation between the two evaluators was present, a discussion was made and a final consensus was reached. Examples of each outcome category are shown in Figure 1a–d.
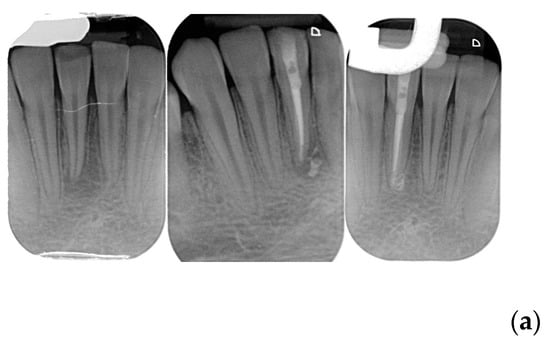
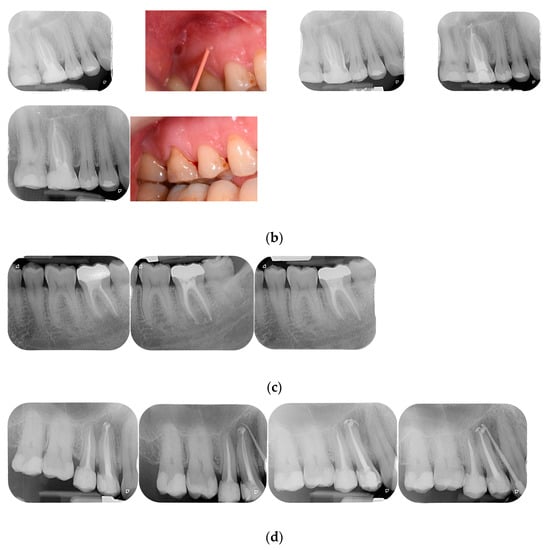
Figure 1.
(a) Healed lower incisor at 12 months recall. (b) Healed upper first molar at 18 months recall. (c) A lower second molar in healing process after 6 months. (d) Not healed first upper bicuspid at 8 months recall.
2.1. Outcome Evaluation
The outcomes assessment are reported in Table 2 and classified accordingly with Chybowski et al., 2018 [32]. In order to identify possible prognostic factors, many variables related to the patient, the tooth, and the treatment were evaluated. Patient factors examined included the sex and age of the patient. Tooth-related factors included tooth type, pulpal and periapical diagnosis, pocket depths, sinus tract, presence/absence of periapical lesion, lesion size, and preoperative percussion and palpation sensitivity. Treatment factors evaluated included treatment type (initial treatment or retreatment), type of BS, sealer extrusion, follow-up time.
Table 2.
The table reports the full recorded outcomes.
2.2. Statistical Analysis
For the purpose of statistical analysis, contingency tables were created with the success outcome categories in column (i.e., number of healed, healing, not-healed teeth) and the parameters of potential clinical interest in row (i.e., number of teeth in patients with age > 50 years, with baseline size of the lesion > 5mm, with apical extrusion of sealer, treated with different sealers). The expected percentage of successful treatments, arbitrarily set at 98%, was used as the basis to calculate the needed sample size to identify a 2% between-group difference with the conventional 5% type I error and 20% type II error. Based on that, 77 teeth per group were needed to have an 80% statistical power [33]. The Pearson chi-square test was used to compare the distribution of values in the different cells. A p value < 0.05 was considered significant, and all tests were 2-sided. Statistical analysis was performed with SPSS v26.0 software (IBM Corp, Armonk, NY, USA).
3. Results
The overall success rate was 99%, with 73.3% healed, 25.7% healing, and 0.95% not healed. The success rate was 100% for initial treatment and 98.2% for retreatment. Fifty-four (N = 54) teeth showed ongoing healing. All of them were retreatment cases with periapical lesions. Regarding the success (healed and healing) versus not healed, no significant difference was found between teeth with or without periapical lesions. However, 154 ETT were classified as healed and 54 ETT as healing.
Patients younger or older than 50 years had a similar rate of healed teeth (75.8% vs. 69.5%), without any difference in success rate (98.8% vs. 99.2%) (p = 0.31).
A statistically significant difference in the distribution of healed, healing, and not-healed teeth was found between the groups of teeth with baseline lesions < 5 mm and >5 mm in diameter (p < 0.01), showing that when the lesions were smaller, the healing process was faster than those with lesions that were bigger than 5 mm in diameter.
Eighty-five treated teeth (40.5%) showed extrusion of the sealer on one or more root(s). The distribution of healed, healing, and not-healed teeth was different between teeth with or without sealer extrusion, with the latter group including a higher percentage of healed teeth (p < 0.01). In particular, the two cases recording an outcome “not healed” showed extrusion of the sealer, with a periapical lesion wider than 5 mm that required retreatment. The presence of extrusion of the sealer was more frequently observed when a preoperative lesion was present (69%) compared with when no lesion was present (31%) (p < 0.01). Although success was not different between initial treatment and retreatment groups, and between groups with and without sealer extrusion, the number of healed roots was higher on roots of initial treatment and without sealer extrusion at the apex.
The success rate of used BS was not statistically significantly different (99.1%, 100%, 97.5%, and 100%, respectively, for CeraSeal, BioRoot, AH Plus Bio, and BIO-C SEALER ION). Nonetheless, the distribution of healed, healing, and not-healed teeth was different between teeth sealed with different materials (p < 0.01).
After being endodontically treated, 125 (59.5%) ETT were restored by direct resin composite restorations using mainly a fiber reinforced flowable resin composite (EveryXFlow GC Co., Tokyo, Japan), and 85 (40.5%) posts were luted. A total of 50 (23.8%) direct restorations remained as final restoration, 92 single crowns (43.8%), 30 (14.3%) partial adhesive crowns, and 38 (18.1%) abutments of fixed bridges were the final treatments.
4. Discussion
Recently, BS were used in clinical trials under controlled conditions. Some authors highlighted that there were no differences between BS and resin and/or zinc phosphate sealers [34,35,36,37,38,39,40], which was also in case of unintentional apical extrusion of sealers [40]. The BS were used with single cone obturation technique [32,34,35,36,37,38,39,40,41] versus zinc phosphate or resin sealers in combination with warm vertical compaction, and the clinical results were always very good. From the results of these clinical trials, it can be speculated that BS can be used in combination with single cone as continuous wave of condensation techniques, and their outcomes are similar to those observed with zinc phosphate and/or resin endodontic sealers.
In this clinical study, success (healed and healing), and failure (not healed) rates were, respectively, 99% and 0.95%. Healed was recorded in 100% of first treatment cases, whilst in case of retreatment in 55.2% of cases were classified as healed, and 43.2% were still healing; this can be due to the fact that almost all retreatment cases showed a periapical lesion and they needed a longer time to heal completely. When there was no periapical lesion, 100% success was recorded.
Four types of BS were tested, and their success rates were similar: between 97.5% and 100%. For that, the first null hypothesis was accepted. However, it must be highlighted that only one material was used in more than 100 cases (CeraSeal in 115 sample teeth), whilst BioRoot, AH Plus Bio, and BIO-C SEALER ION were used, respectively, in 35, 40, and 20 teeth. A wider number of samples of the last three BS and a more uniform distribution of them are desirable in further randomized controlled trials.
Regarding the second tested null hypothesis, i.e., that there was no difference in the endodontic success of ETT with periapical lesion of more or less 5 mm in size at the beginning of the treatment was accepted, the cumulative success rate (healed and healing) showed no statistical significance difference.
However, the size of the periapical lesion showed to be important; when the lesion was lower than 5 mm in diameter, 81% of roots were classified as healed, but when the lesion was wider than 5 mm, only 54.3% were healed. These results were expected because of the short-term observation time.
The third tested null hypothesis was that there was no difference in the endodontic success of ETT with and without extrusion was accepted. In fact, the cumulative success rate (healed and healing) showed, respectively, 97.6% and 100%.
However, when there was no extrusion of the sealer, only 8.8% of ETT showed healing, whilst when it was present, 50.6% of roots were classified as healing. It was also noted that extrusion was usually present when the apex was already opened by the necrosis and was combined with the periapical lesion. From a clinical point of view, it was observed that the presence of postoperative pain was not influenced by the sealer’s extrusion [26].
Regarding the fourth null hypothesis that there was no difference in the endodontic success of ETT of initial vs. retreated teeth, it was accepted because there was no difference in cumulative success rate between the two groups.
Only two failures were recorded and were both retreatments, with a periapical lesion, wider 5 mm in size, with sealer extrusion. From the other side, 208 (99%) cases were classified as a success, and these excellent results can be due to the appropriate shaping and cleaning of root canals [32,41], the obturation procedure [32], the hydraulic effect that pushes the bioceramic sealer into the dental tubules sealing them [42,43,44], and the osteogenic characteristic of this new material [45].
When all the roots were obturated using warm techniques, voids were never noted within the obturation. Additionally, no one root showed short obturation in length.
The clinical evaluation of endodontic outcomes that consider “success” the complete resolution of the periapical radiolucency can be “strict” [46] or “stringent” [47], while choosing a mere reduction in the size of the periapical radiolucency [29,32] was described as setting a “loose” [47] or “lenient” [46] threshold. In this study, it was decided to follow a “loose” [34] or “lenient” [35] threshold. In order to support the adoption of “loose” criteria, the radiographic assessment method was chosen [31]. This system provided a scale of five scores, ranging from healthy to severe periodontitis with exacerbating features [31]. It was based on radiographs with verified histological diagnosis and can be suitable in epidemiological studies [48]. Additionally, the endodontic failure usually occurs within the first years of clinical service [49]. However, it must be noted that the observation time was short, too short to permit complete healing of wide periapical radiolucency [28,48]. However, the expected success rates using the “strict” criteria would be lower than those based on the “loose” criteria [28,29]. All the patients collected in this study were in a recall program to confirm, or disprove, the outcomes under a longer observation period.
Comparing the outcomes of this study with those recently published by the same authors [27], it may be noted that the skill and knowledge of the operators can allow high quality of endodontic treatment and good prognosis. The “operator” could be considered one of the most important factors concerning the outcomes in dentistry and in endodontics.
Regarding the type of build-up, the findings of this study confirmed that the materials and procedure used do not affect the final outcome [50].
Some limitations of this study can be underlined. Firstly, the wider number of ETT should be enrolled; also, the good outcomes of this study were related to the skill and knowledge of one single expert, and it would be of some interest to extend the number of endodontists. Additionally, the limited observation time was short and the patients of this study were in a recall program to collect longer data and to confirm the reported outcomes. Finally, a multicenter prospective study is desirable to confirm the findings of this study.
5. Conclusions
From the findings of this clinical study, the following conclusion can be drawn: a proper obturation of root canals made with warm gutta-percha technique combined with a bioceramic sealer allows a high success rate in endodontically treated teeth.
A periapical lesion does not compromise the quality of the final outcomes.
Author Contributions
Conceptualization, D.I.K.P. and M.F.; methodology, E.F.C. and D.I.K.P.; software, D.M.; validation, D.I.K.P., E.F.C., and V.M.; formal analysis, D.M.; investigation, D.I.K.P., V.M., and E.F.C.; resources, M.F.; data curation, D.I.K.P., M.F., and D.M.; writing—original draft preparation, D.I.K.P. ad ECF; writing—review and editing, M.F.; visualization, M.F.; supervision, D.I.K.P. and M.F.; project administration, D.I.K.P.; funding acquisition, M.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional of Ethical Committee of University of Siena (protocol code PR001; date of approval 21 October 2019).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study. Written informed consent was obtained from the patients to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to containing personal information.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jeong, J.W.; DeGraft-Johnson, A.; Dorn, S.O.; Di Fiore, P.M. Dentinal Tubule penetration of a calcium silicate–based root canal sealer with different obturation. J. Endod. 2017, 43, 633–637. [Google Scholar] [CrossRef]
- Akesl, H.; Makowka, S.; Bosaid, F.; Sarkar, D.; Azim, A.A. Effect of heat application on the physical properties and chemical structure of calcium silicate-based sealers. Clin. Oral Investig. 2021, 25, 2717–2725. [Google Scholar] [CrossRef] [PubMed]
- Donnermeyer, D.; Ibing, M.; Burklein, S.; Weber, I.; Reitze, M.P.; Schafer, E. Physico-chemical investigation of endodontic sealers exposed to simulated intracanal heat application: Hydraulic calcium silicate-based sealers. Materials 2021, 14, 728. [Google Scholar] [CrossRef]
- Abdellatif, D.; Amato, A.; Calapaj, M.; Pisano, M.; Iandolo, A. A novel modified obturation technique using biosealers: An ex vivo study. J. Conserv. Dent. 2023, 24, 369–373. [Google Scholar]
- Pontoriero, D.I.K.; Ferrari Cagidiaco, E.; Cardinali, F.; Fornara, R.; Amato, M.; Grandini, S.; Ferrari, M. Sealing ability of two bioceramic sealers used in combination with three obturation techniques. J. Osseointegr. 2022, 14, 143–148. [Google Scholar]
- Viola, N.V.; Tanomaru Filho, M.; Cerri, P.S. Mta versus portland cement: Review of literature. RSBO Rev. Sul-Bras. De Odontol. 2011, 8, 446–452. [Google Scholar]
- Prati, C.; Gandolfi, M.G. Calcium silicate bioactive cements: Biological perspectives and clinical applications. Dent. Mater. 2015, 31, 351–370. [Google Scholar] [CrossRef]
- Utneja, S.; Nawal, R.R.; Talwar, S.; Verma, M. Current perspectives of bio-ceramic technology in endodontics: Calcium enriched mixture cement—Review of its composition, properties and applications. Restor. Dent. Endod. 2015, 40, 1–13. [Google Scholar] [CrossRef]
- Jitaru, S.; Hodisan, I.; Timis Lucian, A.; Bud, M. The use of bioceramics in endodontics—Literature review. Clujul. Med. 2016, 89, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Arora, V.; Nikhil, V.; Sharma, N.; Arora, P. Bioactive dentin replacement. J. Dent. Med. Sci. 2013, 12, 51–57. [Google Scholar] [CrossRef]
- Malhotra, N.; Agarwal, A.; Mala, K. Mineral trioxide aggregate: A review of physical properties. Compend. Contin. Educ. Dent. 2013, 34, e25–e32. [Google Scholar]
- Parirokh, M.; Torabinejad, M. Mineral trioxide aggregate: A comprehensive literature review—Part I: Chemical, physical, and antibacterial properties. J. Endod. 2010, 36, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; Parirokh, M. Mineral trioxide aggregate: A comprehensive literature review—Part II: Leakage and biocompatibility investigations. J. Endod. 2010, 36, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Parirokh, M.; Torabinejad, M. Mineral trioxide aggregate: A comprehensive literature review—Part III: Clinical applications, drawbacks, and mechanism of action. J. Endod. 2010, 36, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; Parirokh, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part II: Other clinical applications and complications. Int. Endod. J. 2018, 51, 284–317. [Google Scholar] [CrossRef]
- Pontoriero, D.I.K.; Madaro, G.; Vanagolli, V.; Benedicenti, S.; Verniani, G.; Ferrari Cagidiaco, E.; Grandini, S.; Ferrari, M. Sealing ability of a bioceramic sealer used in combination with cold and warm obturation techniques. J. Osseointegr. 2021, 13, 248–255. [Google Scholar]
- Gade, V.J.; Belsare, L.D.; Patil, S.; Bhede, R.; Gade, J.R. Evaluation of push-out bond strength of endosequence BC sealer with lateral condensation and thermoplasticized technique: An in vitro study. J. Conserv. Dent. 2015, 18, 124–127. [Google Scholar]
- Celikten, B.; Uzuntas, C.I.; Orhan, A. Micro-CT assessment of the sealing ability of three root canal filling techniques. J. Oral Sci. 2015, 57, 361–366. [Google Scholar] [CrossRef]
- Camilleri, J. Sealers and warm gutta-percha obturation techniques. J. Endod. 2015, 41, 72–78. [Google Scholar] [CrossRef]
- DeLong, C.; He, J.; Woodmansey, K.F. The effect of obturation technique on the push-out bond strength of calcium silicate sealers. J. Endod. 2015, 41, 385–388. [Google Scholar] [CrossRef]
- Torabinejad, M.; Bahjri, K. Essential elements of evidence-based endodontics: Steps involved in concluding clinical research. J. Endod. 2005, 31, 563–569. [Google Scholar] [CrossRef]
- Berghenholtz, G.; Kvist, T. Evidence-base endodontics. Endod. Top. 2014, 31, 3–18. [Google Scholar] [CrossRef]
- Atmeh, A.R.; Hadis, M.; Camilleri, J. Real-time chemical analysis of root filling materials with heating: Guidelines for safe temperature levels. Int. Endod. J. 2020, 53, 698–708. [Google Scholar] [CrossRef]
- Yamauchi, S.; Watanabe, S.; Okiji, T. Effects of heating on the physical properties of premixed calcium silicate-based root canal sealers. J. Oral Sci. 2020, 63, 65–69. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors Int. Endod. J. 2008, 41, 6–31. [Google Scholar]
- Zhang, X.; Pei, X.; Pei, X.; Wan, Q.; Chen, J.; Wang, J. Success and Complication Rates of Root-Filled Teeth Restored with Zirconia Posts: A Critical Review. Int. J. Prosthodont. 2019, 32, 411–419. [Google Scholar] [CrossRef]
- Pontoriero, D.K.I.; Grandini, S.; Spagnuolo, G.; Discepoli, N.; Benedicenti, S.; Maccagnola, V.; Mosca, A.; Ferrari Cagidiaco, E.; Ferrari, M. Clinical outcomes of endodontic treatments and restorations with and without posts up to 18 years. J. Clin. Med. 2021, 10, 908. [Google Scholar] [CrossRef]
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endodon. J. 2006, 39, 921–930. [Google Scholar] [CrossRef]
- Kim, J.H.; Cho, S.Y.; Choi, Y.; Kim, D.H.; Shin, S.J.; Jung, I.Y. Clinical efficacy of sealer-based obturation using calcium silicate sealers: A randomized clinical trial. J. Endod. 2022, 48, 144–151. [Google Scholar] [CrossRef]
- Orstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring systems for radiographic assessment of apical periodontitis. Endod. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef]
- Orstavik, D. Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. Int. Endod. J. 1996, 29, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Chybowski, E.A.; Glickman, G.N.; Patel, Y. Clinical outcome of non-surgical root canal treatment using a single-cone technique with Endosequence bioceramic sealer: A retrospective analysis. J. Endod. 2018, 44, 941–945. [Google Scholar] [CrossRef]
- Manfredini, D.; Tognini, F.; Biondi, K.; Bosco, M. Sample size calculation on temporomandibolar disorders. Minerva Stomatatol. 2003, 52, 309–319. [Google Scholar]
- Graunaite, I.; Skucaite, N.; Lodiene, G.; Agentiene, I.; Machiulskiene, V.J. Effect of Resin-based and Bioceramic Root Canal Sealers on Postoperative Pain: A Split-mouth Randomized Controlled Trial. J. Endod. 2018, 44, 689–693. [Google Scholar] [CrossRef]
- Shim, K.; Jang, Y.E.; Kim, Y. Comparison of the effects of bioceramic and conventional resin-based sealers on postoperative pain after nonsurgical riit canal treatment: A randomized controlled clinical study. Materials 2021, 14, 2661. [Google Scholar] [CrossRef]
- Yu, Y.H.; Kushnir, L.; Kohli, M.; Karabucak, B. Comparing the incidence of postoperative pain after root canal filling warm vertical obturation with resin-based sealerand sealer-based obturation with calcium silicate-based sealer: A prospective clinical trial. Clin. Oral Investig. 2021, 25, 5033–5042. [Google Scholar] [CrossRef]
- Cosar, M.; Demirci, G.K.; Caliskan, M.K. The effect of two different root canal sealers on treatment outcome and post-obturation pain in single-visit root canal treatment: A prospective randomized clinical trial. Int. Endod. J. 2022, 17, 13870. [Google Scholar] [CrossRef]
- Chopra, V.; Davis, G.; Baysan, A. Clinical and radiographic outcome of non-surgical endodontic treatment using calcium silicate-based versus resin-based sealers—A systematic review and meta-analysis of clinical studies. J. Funct. Biomater. 2022, 13, 38. [Google Scholar] [CrossRef]
- Song, M.; Park, M.G.; Kwak, S.W.; Kim, R.H.; Ha, J.H.; Kim, H.C. Pilot evaluation of sealer-based root canal obturation using epoxy-resin-based and calcium-silicate-based sealers: A randomized clinical trial. Materials 2022, 15, 5146. [Google Scholar] [CrossRef]
- Drumond, J.P.S.C.; Maeda, W.; Nascimento, W.M.; Campos, D.; Prado, M.C.; Jesus Soares, A.; Frozoni, M.J. Comparison of Postobturation Pain Experience after Apical Extrusion of Calcium Silicate–and Resin–Based Root Canal Sealers. J. Endod. 2021, 47, 1278–1284. [Google Scholar] [CrossRef]
- Bardini, G.; Casula, L.; Ambu, E.; Musu, D.; Mercadè, M.; Cotti, E. A 12-month follow-up of primary and secondary root canal treatment in teeth obturated with a hydraulic sealer. Clin. Oral Investig. 2021, 15, 2757–2764. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: Part 1—Periapical health. Int. Endod. J. 2011, 44, 583–609. [Google Scholar] [CrossRef]
- De Bem, I.A.; de Oliveira, R.A.; Weissheimer, T. Effect of ultrasonic activation of endodontic sealers on intratubular penetration and bond strength to root dentin. J. Endod. 2020, 46, 1302–1308. [Google Scholar] [CrossRef]
- Egemen, A.; Belli, S. The effect of primary root canal treatment on dentinal tubule penetration of calcium silicate-based sealers during endodontic retreatment. J. Endod. 2022, 48, 1169–1177. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.N.; Hong, J.U.; Kim, S.M. Anti-inflammatory and osteogenic effects of calcium silicate-based root canal sealers. J. Endod. 2019, 45, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.; Mor, C. The success of endodontic therapy healing and functionality. J. Calif. Dent. Assoc. 2004, 32, 493–503. [Google Scholar] [CrossRef]
- Bender, I.B.; Seltzer, S.; Soltanoff, W. Endodontic success of a reappraisal of criteria. I. Oral Surg. Oral Med. Oral Pathol. 1966, 22, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Boucher, Y.; Matossian, L.; Rilliard, F.; Machtou, P. Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. Int. Endod. J. 2002, 35, 229–238. [Google Scholar] [CrossRef]
- Estrela, C.; Holland, R.; Rodrigues, C.; Alencar, A.H.G.; Sousa-Neto, M.D.; Pecora, J.D. Characterization of Successful Root Canal Treatment. Braz. Dent. J. 2014, 25, 3–11. [Google Scholar] [CrossRef]
- Ferrari, M.; Ferrari Cagidiaco, E.; Goracci, C.; Sorrentino, R.; Zarone, F.; Grandini, S.; Joda, T. Posterior partial crowns out of lithium disilicate (LS2) with or without posts: A randomized controlled prospective clinical trial with a 3-year follow up. J. Dent. 2019, 83, 12–19. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).