
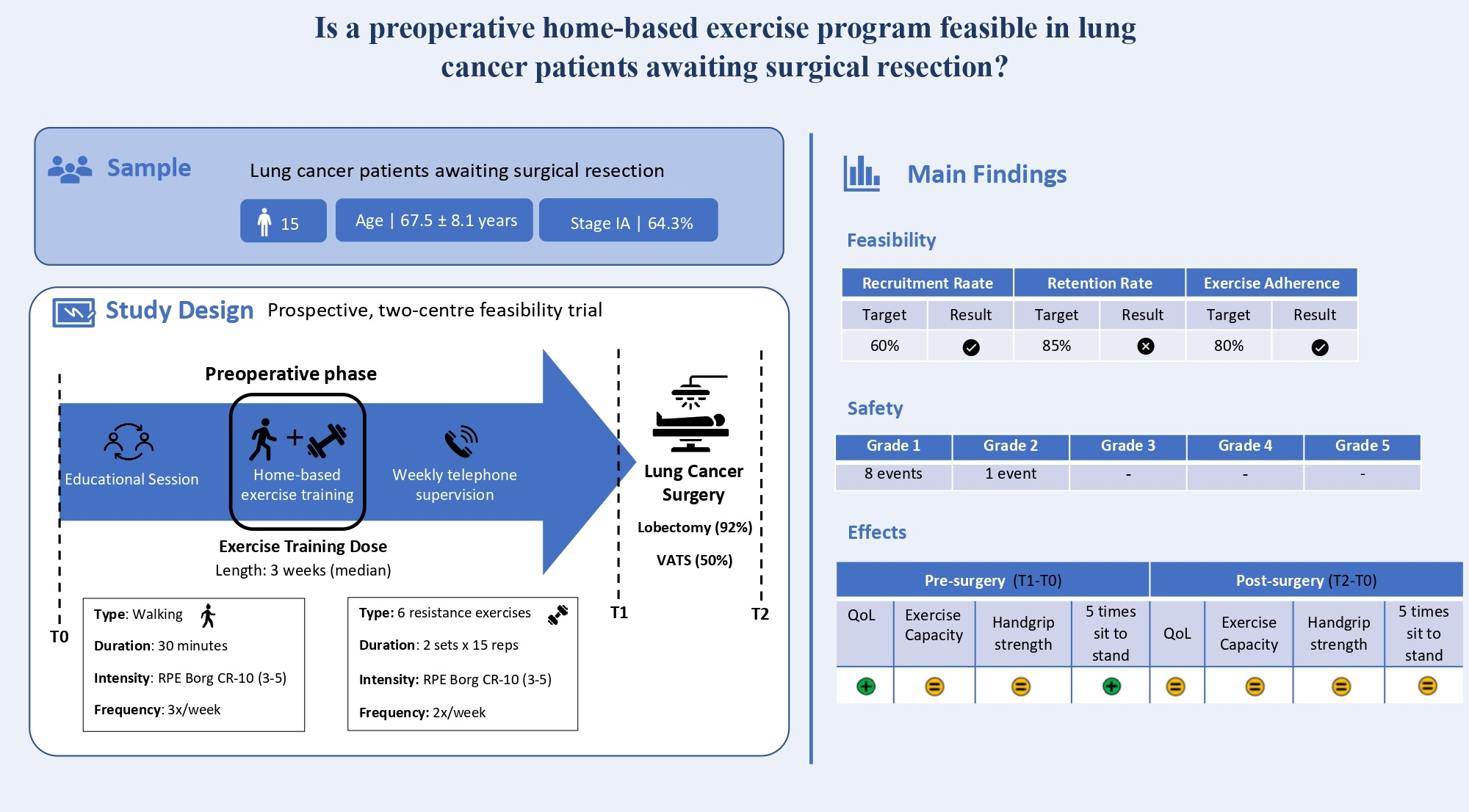
Home-Based Preoperative Exercise Training for Lung Cancer Patients Undergoing Surgery: A Feasibility Trial
 , , , and
, , , and
Abstract
:
1. Introduction
2. Material and Methods
2.1. Design
2.2. Participants
2.3. Intervention
2.4. Study Outcomes
2.4.1. Primary Outcomes
2.4.2. Secondary Outcomes
2.5. Data Collection
2.6. Sample Size Estimation
2.7. Statistical Analysis
3. Results
3.1. Feasibility: Recruitment and Retention Rates
3.2. Feasibility: Exercise Adherence and Acceptability
3.3. Safety
3.4. Preliminary Effects: Changes in HRQOL
3.5. Preliminary Effects: Changes in Physical Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bugge, A.S.; Kongerud, J.S.; Valberg, M.; Solberg, S.K.; Brustugun, O.T.; Lund, M.B. Long-term survival after surgical resection for non-small cell lung cancer. Eur. Respir. J. 2017, 50, PA4292. [Google Scholar]
- Avery, K.N.L.; Blazeby, J.M.; Chalmers, K.A.; Batchelor, T.J.P.; Casali, G.; Internullo, E.; Krishnadas, R.; Evans, C.; West, D. Impact on Health-Related Quality of Life of Video-Assisted Thoracoscopic Surgery for Lung Cancer. Ann. Surg. Oncol. 2020, 27, 1259–1271. [Google Scholar] [CrossRef] [PubMed]
- Nugent, S.M.; Golden, S.E.; Hooker, E.R.; Sullivan, D.R.; Thomas, C.R.; Deffebach, M.E.; Sukumar, M.S.; Schipper, P.H.; Tieu, B.H.; Moghanaki, D.; et al. Longitudinal Health-related Quality of Life among Individuals Considering Treatment for Stage i Non-Small-Cell Lung Cancer. Ann. Am. Thorac. Soc. 2020, 17, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.M.; Gosdin, M.M.; Cooke, D.T.; Apesoa-Varano, E.C.; Kratz, A.L. Health-Related Quality of Life After Lobectomy for Lung Cancer: Conceptual Framework and Measurement. Ann. Thorac. Surg. 2020, 110, 1840–1846. [Google Scholar] [CrossRef]
- Agostini, P.; Cieslik, H.; Rathinam, S.; Bishay, E.; Kalkat, M.S.; Rajesh, P.B.; Steyn, R.S.; Singh, S.; Naidu, B. Postoperative pulmonary complications following thoracic surgery: Are there any modifiable risk factors? Thorax 2010, 65, 815–818. [Google Scholar] [CrossRef]
- Lugg, S.T.; Agostini, P.J.; Tikka, T.; Kerr, A.; Adams, K.; Bishay, E.; Kalkat, M.S.; Steyn, R.S.; Rajesh, P.B.; Thickett, D.R.; et al. Long-term impact of developing a postoperative pulmonary complication after lung surgery. Thorax 2016, 71, 171–176. [Google Scholar] [CrossRef]
- Perera, S.K.; Jacob, S.; Wilson, B.E.; Ferlay, J.; Bray, F.; Sullivan, R.; Barton, M. Global demand for cancer surgery and an estimate of the optimal surgical and anaesthesia workforce between 2018 and 2040: A population-based modelling study. Lancet. Oncol. 2021, 22, 182–189. [Google Scholar] [CrossRef]
- Carli, F.; Gillis, C.; Scheede-Bergdahl, C. Promoting a culture of prehabilitation for the surgical cancer patient. Acta Oncol. 2017, 56, 128–133. [Google Scholar] [CrossRef]
- Tew, G.A.; Ayyash, R.; Durrand, J.; Danjoux, G.R. Clinical guideline and recommendations on pre-operative exercise training in patients awaiting major non-cardiac surgery. Anaesthesia 2018, 73, 750–768. [Google Scholar] [CrossRef]
- West, M.A.; Jack, S.; Grocott, M.P.W. Prehabilitation before surgery: Is it for all patients? Best Pract. Res. Clin. Anaesthesiol. 2021, 35, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Philip, E.J.; Coups, E.J.; Feinstein, M.B.; Park, B.J.; Wilson, D.J.; Ostroff, J.S. Physical activity preferences of early-stage lung cancer survivors. Support Care Cancer 2014, 22, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Cavalheri, V.; Granger, C. Preoperative exercise training for patients with non-small cell lung cancer. Cochrane Database Syst. Rev. 2017, 2017, CD012020. [Google Scholar] [CrossRef] [PubMed]
- Rosero, I.D.; Ramírez-Vélez, R.; Lucia, A.; Martínez-Velilla, N.; Santos-Lozano, A.; Valenzuela, P.L.; Morilla, I.; Izquierdo, M. Systematic review and meta-analysis of randomized, controlled trials on preoperative physical exercise interventions in patients with non-small-cell lung cancer. Cancers 2019, 11, 944. [Google Scholar] [CrossRef]
- Steffens, D.; Beckenkamp, P.R.; Hancock, M.; Solomon, M.; Young, J. Preoperative exercise halves the postoperative complication rate in patients with lung cancer: A systematic review of the effect of exercise on complications, length of stay and quality of life in patients with cancer. Br. J. Sport. Med. 2018, 52, 344. [Google Scholar] [CrossRef]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardiothorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef]
- Ferreira, V.; Agnihotram, R.V.; Bergdahl, A.; van Rooijen, S.J.; Awasthi, R.; Carli, F.; Scheede-Bergdahl, C. Maximizing patient adherence to prehabilitation: What do the patients say? Support. Care Cancer 2018, 26, 2717–2723. [Google Scholar] [CrossRef]
- Waterland, J.L.; Ismail, H.; Amin, B.; Granger, C.L.; Denehy, L.; Riedel, B. Patient acceptance of prehabilitation for major surgery: An exploratory survey. Support. Care Cancer 2021, 29, 779–785. [Google Scholar] [CrossRef]
- Hardcastle, S.J.; Maxwell-Smith, C.; Kamarova, S.; Lamb, S.; Millar, L.; Cohen, P.A. Factors influencing non-participation in an exercise program and attitudes towards physical activity amongst cancer survivors. Support Care Cancer 2018, 26, 1289–1295. [Google Scholar] [CrossRef]
- Jones, L.W.; Courneya, K.S. Exercise counseling and programming preferences of cancer survivors. Cancer Pract. 2002, 10, 208–215. [Google Scholar] [CrossRef]
- Sebio García, R.; Yáñez-Brage, M.I.; Giménez Moolhuyzen, E.; Salorio Riobo, M.; Lista Paz, A.; Borro Mate, J.M. Preoperative exercise training prevents functional decline after lung resection surgery: A randomized, single-blind controlled trial. Clin. Rehabil. 2017, 31, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, I.; Chesterfield-Thomas, G.; Toghill, H. Pre-treatment optimization with pulmonary rehabilitation in lung cancer: Making the inoperable patients operable. EClinicalMedicine 2020, 31, 100663. [Google Scholar] [CrossRef]
- Licker, M.; Karenovics, W.; Diaper, J.; Frésard, I.; Triponez, F.; Ellenberger, C.; Schorer, R.; Kayser, B.; Bridevaux, P.O. Short-Term Preoperative High-Intensity Interval Training in Patients Awaiting Lung Cancer Surgery: A Randomized Controlled Trial. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2017, 12, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, C.; Kayser, B. Preoperative high-intensity interval training is effective and safe in deconditioned patients with lung cancer: A randomized clinical trial. J. Rehabil. Med. 2019, 51, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Driessen, E.J.; Peeters, M.E.; Bongers, B.C.; Maas, H.A.; Bootsma, G.P.; van Meeteren, N.L.; Janssen-Heijnen, M.L. Effects of prehabilitation and rehabilitation including a home-based component on physical fitness, adherence, treatment tolerance, and recovery in patients with non-small cell lung cancer: A systematic review. Crit. Rev. Oncol./Hematol. 2017, 114, 63–76. [Google Scholar] [CrossRef]
- Coats, V.; Maltais, F.; Simard, S.; Fréchette, É.; Tremblay, L.; Ribeiro, F.; Saey, D. Feasibility and effectiveness of a home-based exercise training program before lung resection surgery. Can. Respir. J. 2013, 20, e10–e16. [Google Scholar] [CrossRef]
- Belot, A.; Fowler, H.; Njagi, E.N.; Luque-Fernandez, M.A.; Maringe, C.; Magadi, W.; Exarchakou, A.; Quaresma, M.; Turculet, A.; Peake, M.D.; et al. Association between age, deprivation and specific comorbid conditions and the receipt of major surgery in patients with non-small cell lung cancer in England: A population-based study. Thorax 2019, 74, 51–59. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A.; Altman, D.; Bretz, F.; Campbell, M.; et al. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- de Rooij, M.; van der Leeden, M.; Avezaat, E.; Häkkinen, A.; Klaver, R.; Maas, T.; Peter, W.F.; Roorda, L.D.; Lems, W.F.; Dekker, J. Development of comorbidity-adapted exercise protocols for patients with knee osteoarthritis. Clin. Interv. Aging 2014, 9, 829–842. [Google Scholar] [CrossRef]
- Riebe, D.; Franklin, B.A.; Thompson, P.D.; Garber, C.E.; Whitfield, G.P.; Magal, M.; Pescatello, L.S. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. Med. Sci. Sport. Exerc. 2015, 47, 2473–2479. [Google Scholar] [CrossRef] [PubMed]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R. Consensus on Exercise Reporting Template (CERT): Explanation and Elaboration Statement. Br. J. Sport. Med. 2016, 50, 1428–1437. [Google Scholar] [CrossRef] [PubMed]
- Santa Mina, D.; Petrella, A.; Currie, K.L.; Bietola, K.; Alibhai, S.M.H.; Trachtenberg, J.; Ritvo, P.; Matthew, A.G. Enablers and barriers in delivery of a cancer exercise program: The Canadian experience. Curr. Oncol. 2015, 22, 374–384. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sport. Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Machado, P.; Morgado, M.; Raposo, J.; Mendes, M.; Ferreira, L.E.; Roque, A. OncoEnergy—Manual de Exercício Físico para Pessoas com Cancro; Escola Superior de Saúde do Politécnico de Leiria: Leiria, Portugal, 2021. [Google Scholar] [CrossRef]
- Hayes, S.C.; Newton, R.U.; Spence, R.R.; Galvão, D.A. The Exercise and Sports Science Australia position statement: Exercise medicine in cancer management. J. Sci. Med. Sport 2019, 22, 1175–1199. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sport. Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed]
- Karvinen, K.H.; Vallance, J.; Walker, P.R. Newly diagnosed lung cancer patients’ preferences for and beliefs about physical activity prior to chemotherapy. Psychol. Health Med. 2016, 21, 593–600. [Google Scholar] [CrossRef]
- Leach, H.J.; Devonish, J.A.; Bebb, D.G.; Krenz, K.A.; Culos-Reed, S.N. Exercise preferences, levels and quality of life in lung cancer survivors. Support. Care Cancer 2015, 23, 3239–3247. [Google Scholar] [CrossRef]
- Alcazar, J.; Losa-Reyna, J.; Rodriguez-Lopez, C.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Alegre, L.M. The sit-to-stand muscle power test: An easy, inexpensive and portable procedure to assess muscle power in older people. Exp. Gerontol. 2018, 112, 38–43. [Google Scholar] [CrossRef]
- Buffart, L.M.; Newton, R.U.; Chinapaw, M.J.; Taaffe, D.R.; Spry, N.A.; Denham, J.W.; Joseph, D.J.; Lamb, D.S.; Brug, J.; Galvão, D.A. The effect, moderators, and mediators of resistance and aerobic exercise on health-related quality of life in older long-term survivors of prostate cancer. Cancer 2015, 121, 2821–2830. [Google Scholar] [CrossRef]
- Scherr, J.; Wolfarth, B.; Christle, J.W.; Pressler, A.; Wagenpfeil, S.; Halle, M. Associations between Borg’s rating of perceived exertion and physiological measures of exercise intensity. Eur. J. Appl. Physiol. 2013, 113, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Fairman, C.M.; Lafountain, R.L.; Lucas, A.R.; Focht, B.C. Monitoring resistance exercise intensity using ratings of perceived exertion in previously untrained patients with prostate cancer undergoing androgen deprivation therapy. J. Strength Cond. Res. 2018, 32, 1360–1365. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.P.; Borg, G.A.V. Borg’s scales in strength training; from theory to practice in young and older adults. Appl. Physiol. Nutr. Metab. 2011, 36, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Pincivero, D.M.; Coelho, A.J.; Campy, R.M. Perceived exertion and maximal quadriceps femoris muscle strength during dynamic knee extension exercise in young adult males and females. Eur. J. Appl. Physiol. 2003, 89, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Zamunér, A.R.; Moreno, M.A.; Camargo, T.M.; Graetz, J.P.; Rebelo, A.C.S.; Tamburús, N.Y.; da Silva, E. Assessment of Subjective Perceived Exertion at the Anaerobic Threshold with the Borg CR-10 Scale. J. Sport. Sci. Med. 2011, 10, 130–136. [Google Scholar]
- Singh, B.; Spence, R.; Steele, M.L.; Hayes, S.; Toohey, K. Exercise for Individuals with Lung Cancer: A Systematic Review and Meta-Analysis of Adverse Events, Feasibility, and Effectiveness. Semin. Oncol. Nurs. 2020, 36, 151076. [Google Scholar] [CrossRef]
- Frost, R.; Levati, S.; McClurg, D.; Brady, M.; Williams, B. What Adherence Measures Should Be Used in Trials of Home-Based Rehabilitation Interventions? A Systematic Review of the Validity, Reliability, and Acceptability of Measures. Arch. Phys. Med. Rehabil. 2017, 98, 1241–1256.e1245. [Google Scholar] [CrossRef]
- Scott, B.R.; Duthie, G.M.; Thornton, H.R.; Dascombe, B.J. Training Monitoring for Resistance Exercise: Theory and Applications. Sport. Med. 2016, 46, 687–698. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef]
- El-Kotob, R.; Giangregorio, L.M. Pilot and feasibility studies in exercise, physical activity, or rehabilitation research. Pilot Feasibility Stud. 2018, 4, 137. [Google Scholar] [CrossRef]
- Saito, M.; Ueshima, K.; Saito, M.; Iwasaka, T.; Daida, H.; Kohzuki, M.; Makita, S.; Adachi, H.; Yokoi, H.; Omiya, K.; et al. Safety of exercise-based cardiac rehabilitation and exercise testing for cardiac patients in Japan: A nationwide survey. Circ. J. Off. J. Jpn. Circ. Soc. 2014, 78, 1646–1653. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0; US Department of Health and Human Services, National Institutes of Health. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf (accessed on 1 February 2022).
- Therapeutics Good Administration Department of Health and Ageing Australian Government. The Australian Clinical Trial Handbook: A Simple, Practical Guide to the Conduct of Clinical Trials to International Standards of Good Clinical Practice (GCP) in the Australian Context; American Society of Hand Therapists: Mount Laurel, NJ, USA, 2006.
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; Haes, J.C.J.M.D.; et al. The European organization for research and treatment of cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Hjermstad, M.J.; Fossa, S.D.; Bjordal, K.; Kaasa, S. Test/retest study of the European Organization for Research and Treatment of Cancer Core Quality-of-Life Questionnaire. J. Clin. Oncol. 1995, 13, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Pais-Ribeiro, J.; Pinto, C.; Santos, C. Validation study of the portuguese version of the QLQ-C30-V.3. Psicol. Saúde Doenças 2008, 9, 89–102. [Google Scholar]
- Giesinger, J.M.; Kieffer, J.M.; Fayers, P.M.; Groenvold, M.; Petersen, M.A.; Scott, N.W.; Sprangers, M.A.G.; Velikova, G.; Aaronson, N.K. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J. Clin. Epidemiol. 2016, 69, 79–88. [Google Scholar] [CrossRef]
- Singh, S.J.; Morgan, M.D.; Scott, S.; Walters, D.; Hardman, A.E. Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax 1992, 47, 1019–1024. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Weber, K.; Volland, G.; Kashman, N. Reliability and validity of grip and pinch strength evaluations. J. Hand Surg. 1984, 9, 222–226. [Google Scholar] [CrossRef]
- Fess, E. Clinical assessment recommendations. Am. Soc. Hand Ther. 1981, 6–8. [Google Scholar]
- Trutschnigg, B.; Kilgour, R.D.; Reinglas, J.; Rosenthall, L.; Hornby, L.; Morais, J.A.; Vigano, A. Precision and reliability of strength (Jamar vs. Biodex handgrip) and body composition (dual-energy X-ray absorptiometry vs. bioimpedance analysis) measurements in advanced cancer patients. Appl. Physiol. Nutr. Metab. 2008, 33, 1232–1239. [Google Scholar] [CrossRef]
- Beauchamp, M.K.; Hao, Q.; Kuspinar, A.; D’Amore, C.; Scime, G.; Ma, J.; Mayhew, A.; Bassim, C.; Wolfson, C.; Kirkland, S.; et al. Reliability and Minimal Detectable Change Values for Performance-Based Measures of Physical Functioning in the Canadian Longitudinal Study on Aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, 2030–2038. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.; Bromley, K.; Sutton, C.J.; McCray, G.; Myers, H.L.; Lancaster, G.A. Determining sample size for progression criteria for pragmatic pilot RCTs: The hypothesis test strikes back! Pilot Feasibility Stud. 2021, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Lancaster, G.A. Pilot and feasibility studies come of age! Pilot Feasibility Stud. 2015, 1, 1. [Google Scholar] [CrossRef]
- Sim, J. Should treatment effects be estimated in pilot and feasibility studies? Pilot Feasibility Stud. 2019, 5, 107. [Google Scholar] [CrossRef]
- Lancaster, G.A.; Dodd, S.; Williamson, P.R. Design and analysis of pilot studies: Recommendations for good practice. J. Eval. Clin. Pract. 2004, 10, 307–312. [Google Scholar] [CrossRef]
- Koller, M.; Musoro, J.Z.; Tomaszewski, K.; Coens, C.; King, M.T.; Sprangers, M.A.G.; Groenvold, M.; Cocks, K.; Velikova, G.; Flechtner, H.-H.; et al. Minimally important differences of EORTC QLQ-C30 scales in patients with lung cancer or malignant pleural mesothelioma—Interpretation guidance derived from two randomized EORTC trials. Lung Cancer 2022, 167, 65–72. [Google Scholar] [CrossRef]
- Morano, M.T.; Araújo, A.S.; Nascimento, F.B.; Da Silva, G.F.; Mesquita, R.; Pinto, J.S.; De Moraes Filho, M.O.; Pereira, E.D. Preoperative pulmonary rehabilitation versus chest physical therapy in patients undergoing lung cancer resection: A pilot randomized controlled trial. Arch. Phys. Med. Rehabil. 2013, 94, 53–58. [Google Scholar] [CrossRef]
- Elshahat, S.; Treanor, C.; Donnelly, M. Factors influencing physical activity participation among people living with or beyond cancer: A systematic scoping review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 50. [Google Scholar] [CrossRef]
- Dueck, A.C.; Mendoza, T.R.; Mitchell, S.A.; Reeve, B.B.; Castro, K.M.; Rogak, L.J.; Atkinson, T.M.; Bennett, A.V.; Denicoff, A.M.; O’Mara, A.M.; et al. Validity and Reliability of the US National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). JAMA Oncol. 2015, 1, 1051–1059. [Google Scholar] [CrossRef]
- Scott, J.M.; Thomas, S.M.; Herndon, J.E., 2nd; Douglas, P.S.; Yu, A.F.; Rusch, V.; Huang, J.; Capaci, C.; Harrison, J.N.; Stoeckel, K.J.; et al. Effects and tolerability of exercise therapy modality on cardiorespiratory fitness in lung cancer: A randomized controlled trial. J. Cachexia Sarcopenia Muscle 2021, 12, 1465. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, T.S.; Scott, J.M.; Michalski, M.; Capaci, C.; Thomas, S.; Herndon, J.E.; Sasso, J.; Eves, N.D.; Jones, L.W. Novel Methods for Reporting of Exercise Dose and Adherence: An Exploratory Analysis. Med. Sci. Sport. Exerc. 2018, 50, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Hung, R.; Krebs, P.; Coups, E.J.; Feinstein, M.B.; Park, B.J.; Burkhalter, J.; Ostroff, J.S. Fatigue and functional impairment in early-stage non-small cell lung cancer survivors. J. Pain Symptom Manag. 2011, 41, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Walling, A.M.; Weeks, J.C.; Kahn, K.L.; Tisnado, D.; Keating, N.L.; Dy, S.M.; Arora, N.K.; Mack, J.W.; Pantoja, P.M.; Malin, J.L. Symptom Prevalence in Lung and Colorectal Cancer Patients. J. Pain Symptom Manag. 2015, 49, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Pompili, C.; McLennan Battleday, F.; Chia, W.L.; Chaudhuri, N.; Kefaloyannis, E.; Milton, R.; Papagiannopoulos, K.; Tcherveniakov, P.; Brunelli, A. Poor preoperative quality of life predicts prolonged hospital stay after VATS lobectomy for lung cancer. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2021, 59, 116–121. [Google Scholar] [CrossRef]
- Pompili, C.; Velikova, G.; White, J.; Callister, M.; Robson, J.; Dixon, S.; Franks, K.; Brunelli, A. Poor preoperative patient-reported quality of life is associated with complications following pulmonary lobectomy for lung cancer. Eur. J. Cardio-Thorac. Surg. 2017, 51, 526–531. [Google Scholar] [CrossRef]
- Machado, P.; Pimenta, S.; Oliveiros, B.; Ferreira, J.P.; Martins, R.A.; Cruz, J. Effect of Exercise Training on Quality of Life after Colorectal and Lung Cancer Surgery: A Meta-Analysis. Cancers 2021, 13, 4975. [Google Scholar] [CrossRef]
- Boujibar, F.; Gillibert, A.; Bonnevie, T.; Rinieri, P.; Montagne, F.; Selim, J.; Cuvelier, A.; Gravier, F.E.; Baste, J.M. The 6-minute stepper test and the sit-to-stand test predict complications after major pulmonary resection via minimally invasive surgery: A prospective inception cohort study. J. Physiother. 2022, 68, 130–135. [Google Scholar] [CrossRef]
- Kenny, P.M.; King, M.T.; Viney, R.C.; Boyer, M.J.; Pollicino, C.A.; McLean, J.M.; Fulham, M.J.; McCaughan, B.C. Quality of life and survival in the 2 years after surgery for non-small-cell lung cancer. J. Clin. Oncol. 2008, 26, 233–241. [Google Scholar] [CrossRef]
- Nagamatsu, Y.; Maeshiro, K.; Kimura, N.Y.; Nishi, T.; Shima, I.; Yamana, H.; Shirouzu, K. Long-term recovery of exercise capacity and pulmonary function after lobectomy. J. Thorac. Cardiovasc. Surg. 2007, 134, 1273–1278. [Google Scholar] [CrossRef]
- Edvardsen, E.; Anderssen, S.A.; Borchsenius, F.; Skjønsberg, O.H. Reduction in cardiorespiratory fitness after lung resection is not related to the number of lung segments removed. BMJ Open Sport Exerc. Med. 2015, 1, e000032. [Google Scholar] [CrossRef] [PubMed]
- Frost, R.; McClurg, D.; Brady, M.; Williams, B. Optimising the validity and completion of adherence diaries: A multiple case study and randomised crossover trial. Trials 2016, 17, 489. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Participants (n = 15) | Underwent Surgery (n = 12) |
|---|---|---|
| Age (years), mean (SD) | 67.5 (8.1) | 66.4 (7.2) |
| BMI (kg/m2), mean (SD) | 26.3 (3.4) | 26.5 (3.1) |
| Sex (males), no. (%) | 9 (60) | 7 (58.3%) |
| Educational level, no. (%) | ||
| <10 years | 10 (66.7) | 8 (66.7) |
| ≥10 years | 5 (33.3) | 3 (33.3) |
| Smoking status, no. (%) | ||
| Current | 7 (46.7) | 5 (41.7) |
| Former | 5 (33.3) | 5 (41.7) |
| Never | 3 (20) | 2 (16.7) |
| Cancer diagnosis, no. (%) | ||
| NSCLC | 12 (80) | 10 (83.3) |
| Neuroendocrine tumor | 2 (13.3) | 2 (16.7) |
| No diagnosis * | 1 (6.7) | |
| Histological subtype a, no. (%) | ||
| Adenocarcinoma | 11 (78.6) | 9 (75) |
| Squamous cell carcinoma | 1 (7.1) | 1 (8.3) |
| Carcinoid | 2 (14.3) | 2 (16.7) |
| Tumor stage b, no. (%) | ||
| IA | 9 (64.3) | 8 (66.7) |
| IB | 3 (21.4) | 2 (16.7) |
| IIA | 1 (7.1) | 1 (8.3) |
| IIB | 1 (7.1) | 1 (8.3) |
| Comorbidities, no (%) | ||
| Hypertension | 7 (46.7) | 6 (50) |
| Cardiovascular disease | 5 (33.3) | 3 (25) |
| COPD | 4 (26.7) | 4 (33.3) |
| Other | 8 (53.3) | 6 (50) |
| Charlson comorbidity index c, mean (SD) | 3.5 (1.7) | 3.5 (1.6) |
| SpO2 (%), mean (SD) | 96.3 (2.1) | 95.8 (2.1) |
| Pulmonary function, mean (SD) | ||
| FVC (% predicted) | 92.1 (11.8) | 93 (12.8) |
| FEV1 (% predicted) | 81.9 (21.4) | 81.2 (23.9) |
| DLCO (% predicted) | 72.4 (20.8) | 69.7 (22.1) |
| Resection degree, no. (%) | ||
| Lobectomy | 11 (91.7) | |
| Bilobectomy | 1 (8.3) | |
| Surgical approach, no. (%) | ||
| VATS | 6 (50) | |
| Open Surgery | 6 (50) | |
| Length of hospital stay (days), median (IQR) | 3 (2.5) |
| Variable | Aerobic Exercise | Resistance Exercise | ||||||
|---|---|---|---|---|---|---|---|---|
 |  | |||||||
| Number of sessions, median (IQR) | 9 (8–10) | 7 (6–8) | ||||||
| Attendance rate (%), median (IQR) | 100 (89–100) | 100 (100–117) | ||||||
| Compliance rate (%), median (IQR) | 104 (83–138) | 111 (100–119) | ||||||
| Weekly training volume (min/reps), median (IQR) | 104 (83–145) | 450 (420–500) | ||||||
| Intensity (RPE) a, mean (SD) | 3.5 (0.2) | 3.4 (0.2) | ||||||
| Adverse events b | Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
| Arthralgia, no. of events | 4 | 1 | ||||||
| Foot pain, no. of events | 1 | |||||||
| Leg muscle soreness, no. of events | 3 | |||||||
| Adverse events per number of sessions completed, no. (%) | 4 per 135 (3) | 5 per 103 (4.9) | ||||||
 aerobic exercise;
aerobic exercise;  resistance exercise. a based on Borg Category Ratio scale (0–10 scale); b based on the Common Terminology Criteria for Adverse Events (Version 5.0).
resistance exercise. a based on Borg Category Ratio scale (0–10 scale); b based on the Common Terminology Criteria for Adverse Events (Version 5.0).| Variable | Baseline (T0) (n = 12) | Post-Exercise Intervention (T1) (n = 12) | 4–5 Weeks after Surgery (T2) (n = 12) | p-Value (Time Effect) | ||
|---|---|---|---|---|---|---|
| Mean (SD) or Median (IQR) | Mean (SD) or Median (IQR) | Change (95% CI); ΔT1−T0 | Mean (SD) or Median (IQR) | Change (95% CI); ΔT2−T0 | ||
| HRQOL (EORTC-QLQ-C30 scales) § | ||||||
| Physical Functioning a | 84.5 (11.4) | 87.3 (10.8) | 2.8 (0 to 5.6) | 72.8 (16.1) | −11.6 (−26 to 2.8) | 0.007 * |
| Role Functioning b | 100 (75–100) | 100 (100–100) | 8.3 (0 to 16.5) | 91.5 (67–100) | −8.5 (−33.5 to 16.5) | 0.166 |
| Social Functioning b | 100 (83.3–100) | 100 (100–100) | 0 (−8 to 8.3) | 100 (83.5–100) | 0 (−25 to 8.3) | 0.646 |
| Emotional Functioning a | 77.1 (20.8) | 79.9 (16.5) | 2.9 (−8.8 to 14.6) | 81.9 (15.4) | 4.9 (−16.7 to 26.4) | 0.662 |
| Cognitive Functioning b | 100 (83.2–100) | 100 (83–100) | 0 (−1.7 to 8) | 83 (83–100) | −0.3 (−17 to 8.3) | 0.459 |
| Global health status a | 62.5 (20.2) | 67.4 (20.8) | 4.9 (−11.4 to 21.2) | 71.5 (16.5) | 9 (−16.3 to 34.3) | 0.498 |
| Fatigue b | 22.1 (0–33) | 0 (0–16.5) | −11 (−16.7 to 0) | 22 (16.5 to 33) | 5.4 (−11 to 27.5) | 0.044 * |
| Pain b | 0 (0–8.5) | 0 (0–17.5) | 0 (−8 to 8.5) | 17 (0–33.5) | 17 (−8 to 41.5) | 0.391 |
| Dyspnea b | 0 (0–33.2) | 0 (0–16.5) | 0 (−0.2 to 0) | 0 (0–33) | 8.3 (−0.2 to 33) | 0.129 |
| Nausea and vomiting b | 0 (0) | 0 (0) | 0 (0 to 0) | 0 (0) | 0 (0 to 0) | NA |
| Insomnia b | 16.5 (0–33.2) | 0 (0–33) | 0 (−16.5 to 0) | 16.5 (0–50) | 0 (−16.7 to 33.5) | 0.354 |
| Appetite loss b | 0 (0–0) | 0 (0–0) | 0 (0 to 0) | 0 (0–16.5) | 0 (0 to 33.5) | NA |
| Constipation b | 0 (0–0) | 0 (0–16.5) | 0 (−0.2 to 0.2) | 0 (0–50) | 0.2 (0 to 33) | 0.099 |
| Diarrhea b | 0 (0) | 0 (0–0) | 0 (0 to 0) | 0 (0–0) | 0 (0 to 0) | NA |
| Summary Score a | 89.5 (6.5) | 92.3 (6) | 2.9 (0.9 to 4.8) * | 82 (14) | −7.5 (−22 to 7) | 0.049 * |
| Physical performance | ||||||
| Incremental shuttle walk test (m) a | 451.7 (117) | 511.3 (168.4) | 57.5 (−5.5 to 120.5) | 375.4 (170) | −76.3 (−193.3 to 40.8) | 0.059 |
| Handgrip strength, right hand (kg) a | 33.4 (8.3) | 35.6 (9.7) | 2.2 (−1 to 5.3) | 34.6 (8.2) | 1.2 (−2.5 to 4.8) | 0.288 |
| Handgrip strength, left hand (kg) a | 33.2 (10.4) | 34.7 (10.3) | 1.5 (0 to 3) | 33.3 (9.1) | 0.2 (−4.8 to 5.1) | 0.434 |
| Five-times sit-to-stand (s) b | 7.8 (7.1–9.6) | 7.2 (5–7.9) | −1.5 (−2.1 to −0.9) * | 7.1 (6.6 to 8) | −0.6 (−2.4 to 1) | 0.006 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, P.; Pimenta, S.; Garcia, A.L.; Nogueira, T.; Silva, S.; Oliveiros, B.; Martins, R.A.; Cruz, J. Home-Based Preoperative Exercise Training for Lung Cancer Patients Undergoing Surgery: A Feasibility Trial. J. Clin. Med. 2023, 12, 2971. https://doi.org/10.3390/jcm12082971
Machado P, Pimenta S, Garcia AL, Nogueira T, Silva S, Oliveiros B, Martins RA, Cruz J. Home-Based Preoperative Exercise Training for Lung Cancer Patients Undergoing Surgery: A Feasibility Trial. Journal of Clinical Medicine. 2023; 12(8):2971. https://doi.org/10.3390/jcm12082971
Chicago/Turabian StyleMachado, Pedro, Sara Pimenta, Ana Luís Garcia, Tiago Nogueira, Sónia Silva, Bárbara Oliveiros, Raul A. Martins, and Joana Cruz. 2023. "Home-Based Preoperative Exercise Training for Lung Cancer Patients Undergoing Surgery: A Feasibility Trial" Journal of Clinical Medicine 12, no. 8: 2971. https://doi.org/10.3390/jcm12082971