
Intense Pulsed Light Therapy in the Treatment of Dry Eye Diseases: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
- Paper published either in English or French.
- Trials including more than 20 patients.
- Adult patients diagnosed with DED or MGD and no other conditions that could affect the different assessments such as acute inflammation, contact lens wearing, previous IPL treatment, or other local eyelid treatment.
- Trials that compared IPL therapy ± meibomian gland expression (MGX) with sham treatment, eyelid hygiene, MGX alone, or no treatment.
2.2. Search Strategy
2.3. Selection Process and Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias in Included Studies
3.4. Syntheses Results
3.5. Heterogeneity Analysis
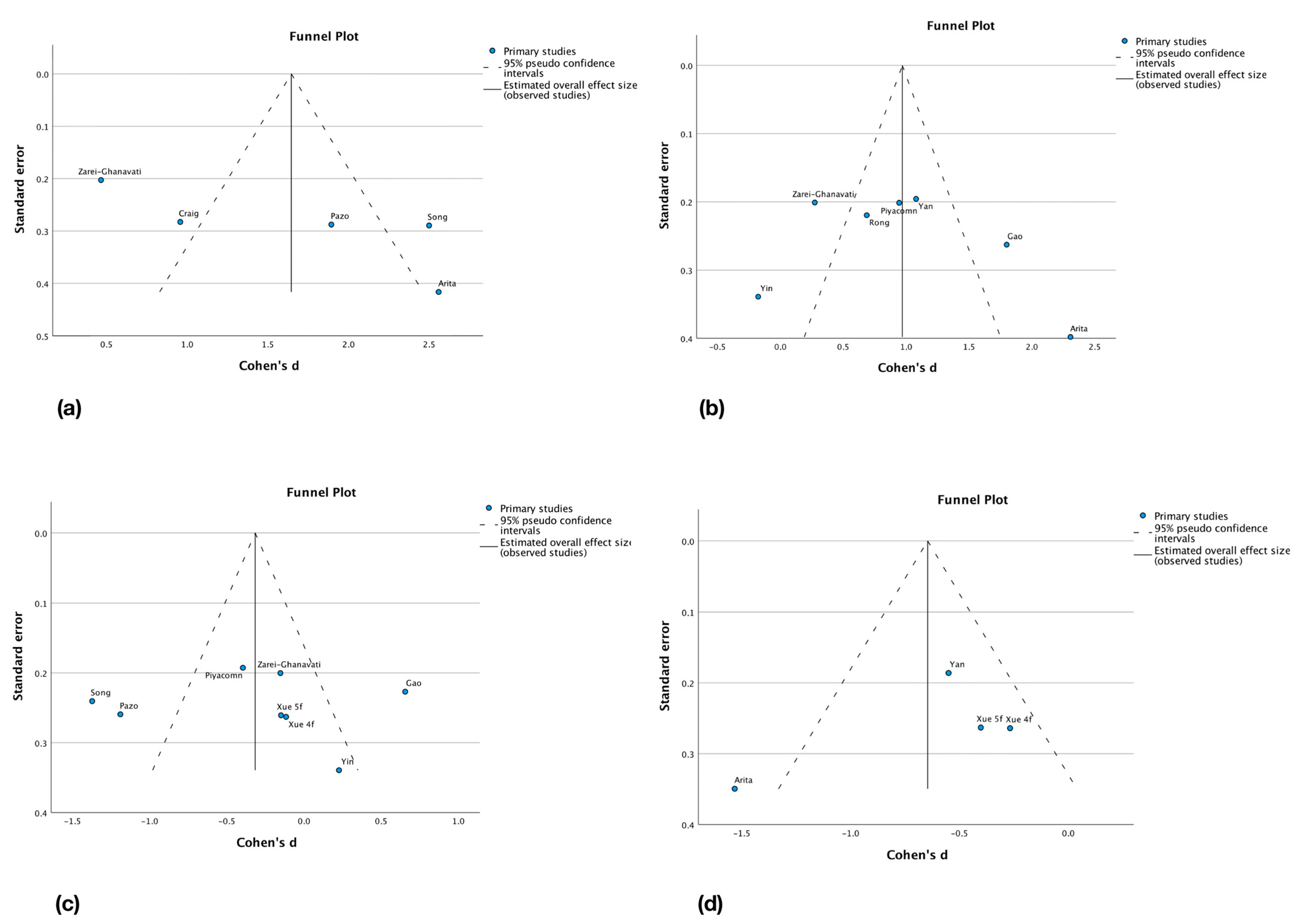
3.6. Reporting Biases Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DED | Dry eye disease |
| IPL | Intense pulsed light |
| MGD | Meibomian gland dysfunction |
| MGX | Meibomian gland expression |
| NIBUT | Non-invasive break-up time |
| OSDI | Ocular surface disease index |
| SPEED | Standard patient evaluation of eye dryness |
| TBUT | Tear break-up time |
References
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.-S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II Epidemiology Report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.-K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Rouen, P.A.; White, M.L. Dry Eye Disease: Prevalence, Assessment, and Management. Home Healthc. Now 2018, 36, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Maeng, K.J.; Lee, K.; Kim, S.; Park, C.K.; Kim, E.W.; Lee, S.Y.; Bae, H.W.; Seong, G.J.; Kim, C.Y. Effects of Glaucoma Medication on Dry Eye Syndrome and Quality of Life in Patients with Glaucoma. Korean J. Ophthalmol. 2021, 35, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Rakofsky, J.J.; Rakofsky, S.I.; Dunlop, B.W. Dry Those Crying Eyes: The Role of Depression and Antidepressants in Dry Eye Disease. J. Clin. Psychopharmacol. 2021, 41, 295–303. [Google Scholar] [CrossRef]
- Muhafiz, E.; Bayhan, S.A.; Bayhan, H.A.; Gürdal, C. Effects of chronic smoking on the meibomian glands. Int. Ophthalmol. 2019, 39, 2905–2911. [Google Scholar] [CrossRef]
- Muhafiz, E.; Ölçen, M.; Erten, R.; Bozkurt, E. Evaluation of Meibomian Glands in Obstructive Sleep Apnea-Hypopnea Syndrome. Cornea 2020, 39, 685–690. [Google Scholar] [CrossRef]
- Adiguzel, S.; Palamar, M.; Yargucu, F.; Oksel, F.; Yagci, A. Evaluation of Ocular Surface and Meibomian Glands in Patients With Scleroderma. Cornea 2021, 40, 977–981. [Google Scholar] [CrossRef]
- Baudouin, C.; Messmer, E.M.; Aragona, P.; Geerling, G.; Akova, Y.; Benítez-Del-Castillo, J.; Boboridis, K.; Merayo-Lloves, J.; Rolando, M.; Labetoulle, M. Revisiting the vicious circle of dry eye disease: A focus on the pathophysiology of meibomian gland dysfunction. Br. J. Ophthalmol. 2016, 100, 300–306. [Google Scholar] [CrossRef]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-Del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. TFOS DEWS II Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef]
- Hu, J.; Zhu, S.; Liu, X. Efficacy and safety of a vectored thermal pulsation system (Lipiflow®) in the treatment of meibomian gland dysfunction: A systematic review and meta-analysis. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 260, 25–39. [Google Scholar] [CrossRef]
- Craig, J.P.; Chen, Y.H.; Turnbull, P.R.K. Prospective Trial of Intense Pulsed Light for the Treatment of Meibomian Gland Dysfunction. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1965–1970. [Google Scholar] [CrossRef]
- Suwal, A.; Hao, J.-L.; Zhou, D.-D.; Liu, X.-F.; Suwal, R.; Lu, C.-W. Use of Intense Pulsed Light to Mitigate Meibomian Gland Dysfunction for Dry Eye Disease. Int. J. Med. Sci. 2020, 17, 1385–1392. [Google Scholar] [CrossRef]
- Papageorgiou, P.; Clayton, W.; Norwood, S.; Chopra, S.; Rustin, M. Treatment of rosacea with intense pulsed light: Significant improvement and long-lasting results. Br. J. Dermatol. 2008, 159, 628–632. [Google Scholar] [CrossRef]
- Fishman, H.A.; Periman, L.M.; Shah, A.A. Real-Time Video Microscopy of In Vitro Demodex Death by Intense Pulsed Light. Photobiomodul. Photomed. Laser Surg. 2020, 38, 472–476. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Korb, D.R.; Greiner, J.v.; Herman, J. Comparison of Fluorescein Break-Up Time Measurement Reproducibility Using Standard Fluorescein Strips Versus the Dry Eye Test (DET) Method. Cornea 2001, 20, 811–815. [Google Scholar] [CrossRef]
- Pauk, S.V.; Petriček, I.; Jukić, T.; Popović-Suić, S.; Tomić, M.; Kalauz, M.; Jandroković, S.; Masnec, S. Noninvasive tear film break-up time assessment using handheld lipid layer examination instrument. Acta Clin. Croat. 2019, 58, 63–71. [Google Scholar]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and Validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Özcura, F.; Aydin, S.; Helvaci, M.R. Ocular Surface Disease Index for the Diagnosis of Dry Eye Syndrome. Ocul. Immunol. Inflamm. 2007, 15, 389–393. [Google Scholar] [CrossRef]
- Keir, N.; Ngo, W.; Situ, P.; Korb, D.; Blackie, C.; Simpson, T. Evaluation of the Standard Patient Evaluation of Eye Dryness (SPEED) Questionnaire. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6028. [Google Scholar]
- Asiedu, K. Rasch Analysis of the Standard Patient Evaluation of Eye Dryness Questionnaire. Eye Contact Lens 2017, 43, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Chen, Y.; Li, J.; Wu, Y.; Lin, X.; Deng, X.; Zhao, Y.E. Comparative Evaluation in Intense Pulsed Light Therapy Combined with or without Meibomian Gland Expression for the Treatment of Meibomian Gland Dysfunction. Curr. Eye Res. 2021, 46, 1125–1131. [Google Scholar] [CrossRef]
- Liu, R.; Rong, B.; Tu, P.; Tang, Y.; Song, W.; Toyos, R.; Toyos, M.; Yan, X. Analysis of Cytokine Levels in Tears and Clinical Correlations After Intense Pulsed Light Treating Meibomian Gland Dysfunction. Am. J. Ophthalmol. 2017, 183, 81–90. [Google Scholar] [CrossRef]
- Ren, X.; Chou, Y.; Wang, Y.; Chen, Y.; Liu, Z.; Li, X. Comparison of intense pulsed light and near-infrared light in the treatment of dry eye disease: A prospective randomized study. Acta Ophthalmol. 2021, 99, e1307–e1314. [Google Scholar] [CrossRef]
- Huang, X.; Qin, Q.; Wang, L.; Zheng, J.; Lin, L.; Jin, X. Clinical results of Intraductal Meibomian gland probing combined with intense pulsed light in treating patients with refractory obstructive Meibomian gland dysfunction: A randomized controlled trial. BMC Ophthalmol. 2019, 19, 211. [Google Scholar] [CrossRef]
- Pazo, E.E.; Huang, H.; Fan, Q.; Zhang, C.; Yue, Y.; Yang, L.; Xu, L.; Moore, J.E.; He, W. Intense Pulse Light for Treating Post-LASIK Refractory Dry Eye. Photobiomodul. Photomed. Laser Surg. 2020, 39, 155–163. [Google Scholar] [CrossRef]
- Gao, Y.-F.; Liu, R.-J.; Li, Y.-X.; Huang, C.; Liu, Y.-Y.; Hu, C.-X.; Qi, H. Comparison of anti-inflammatory effects of intense pulsed light with tobramycin/dexamethasone plus warm compress on dry eye associated meibomian gland dysfunction. Int. J. Ophthalmol. 2019, 12, 1708–1713. [Google Scholar] [CrossRef]
- Yan, X.; Hong, J.; Jin, X.; Chen, W.; Rong, B.; Feng, Y.; Huang, X.; Li, J.; Song, W.; Lin, L.; et al. The Efficacy of Intense Pulsed Light Combined With Meibomian Gland Expression for the Treatment of Dry Eye Disease Due to Meibomian Gland Dysfunction: A Multicenter, Randomized Controlled Trial. Eye Contact Lens 2021, 47, 45–53. [Google Scholar] [CrossRef]
- Song, Y.; Yu, S.; He, X.; Yang, L.; Wu, Y.; Qin, G.; Zhang, Q.; Talwar, G.D.S.; Xu, L.; Moore, J.E.; et al. Tear film interferometry assessment after intense pulsed light in dry eye disease: A randomized, single masked, sham-controlled study. Contact Lens Anterior Eye 2022, 45, 101499. [Google Scholar] [CrossRef]
- Rong, B.; Tang, Y.; Tu, P.; Liu, R.; Qiao, J.; Song, W.; Toyos, R.; Yan, X. Intense Pulsed Light Applied Directly on Eyelids Combined with Meibomian Gland Expression to Treat Meibomian Gland Dysfunction. Photomed. Laser Surg. 2018, 36, 326–332. [Google Scholar] [CrossRef]
- Yin, Y.; Liu, N.; Gong, L.; Song, N. Changes in the Meibomian Gland After Exposure to Intense Pulsed Light in Meibomian Gland Dysfunction (MGD) Patients. Curr. Eye Res. 2018, 43, 308–313. [Google Scholar] [CrossRef]
- Xue, A.L.; Wang, M.T.M.; Ormonde, S.E.; Craig, J.P. Randomised double-masked placebo-controlled trial of the cumulative treatment efficacy profile of intense pulsed light therapy for meibomian gland dysfunction. Ocul. Surf. 2020, 18, 286–297. [Google Scholar] [CrossRef]
- Arita, R.; Fukuoka, S.; Morishige, N. Therapeutic efficacy of intense pulsed light in patients with refractory meibomian gland dysfunction. Ocul. Surf. 2019, 17, 104–110. [Google Scholar] [CrossRef]
- Piyacomn, Y.; Kasetsuwan, N.; Reinprayoon, U.; Satitpitakul, V.; Tesapirat, L. Efficacy and Safety of Intense Pulsed Light in Patients With Meibomian Gland Dysfunction—A Randomized, Double-Masked, Sham-Controlled Clinical Trial. Cornea 2020, 39, e18. [Google Scholar] [CrossRef]
- Zarei-Ghanavati, S.; Hassanzadeh, S.; Khorasani, A.A.; Ehsaei, A.; Bakhtiari, E. Efficacy of five-flash intense pulsed light therapy technique in patients with meibomian gland dysfunction. Clin. Exp. Optom. 2021, 105, 687–693. [Google Scholar] [CrossRef]
- Deeks, J.; Higgins, J.; Altman, D. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions, Version 6.3; updated February 2022; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2022. [Google Scholar]
- Vollert, J.; Cook, N.R.; Kaptchuk, T.J.; Sehra, S.T.; Tobias, D.K.; Hall, K.T. Assessment of Placebo Response in Objective and Subjective Outcome Measures in Rheumatoid Arthritis Clinical Trials. JAMA Netw. Open 2020, 3, e2013196. [Google Scholar] [CrossRef]
- Wang, J.; Li, S.; Yeh, T.N.; Chakraborty, R.; Graham, A.D.; Yu, S.X.; Lin, M.C. Quantifying Meibomian Gland Morphology Using Artificial Intelligence. Optom. Vis. Sci. 2021, 98, 1094–1103. [Google Scholar] [CrossRef]
- Yazdani, M.; Elgstøen, K.B.P.; Rootwelt, H.; Shahdadfar, A.; Utheim, A.; Utheim, T.P. Tear Metabolomics in Dry Eye Disease: A Review. Int. J. Mol. Sci. 2019, 20, 3755. [Google Scholar] [CrossRef]
- Düzgün, E.; Özkur, E. The effect of oral isotretinoin therapy on meibomian gland morphology and dry eye tests. J. Dermatol. Treat. 2022, 33, 762–768. [Google Scholar] [CrossRef]
- Xiao, J.; Adil, M.Y.; Chen, X.; Utheim, A.; Ræder, S.; Tønseth, K.A.; Lagali, N.S.; Dartt, D.A.; Utheim, T.P. Functional and Morphological Evaluation of Meibomian Glands in the Assessment of Meibomian Gland Dysfunction Subtype and Severity. Am. J. Ophthalmol. 2020, 209, 160–167. [Google Scholar] [CrossRef]
- Valencia-Nieto, L.; Novo-Diez, A.; Blanco-Vázquez, M.; López-Miguel, A. Therapeutic Instruments Targeting Meibomian Gland Dysfunction. Ophthalmol. Ther. 2020, 9, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.S.; Rhim, J.W.; Park, J.H. Combination treatment with intense pulsed light, thermal pulsation (LipiFlow), and meibomian gland expression for refractory meibomian gland dysfunction. Int. Ophthalmol. 2022, 42, 3311–3319. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Country | Year | Number of Patients | Age (Years) | Sex Ratio M/F | Instrument Model | Power (J/cm2) | Frequency and Number of Sessions | TG | CG | Longest Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Arita [36] | Japan | 2019 | 42 | TG: 61.0 ± 18.0 CG: 61.9 ± 12.2 | TG: 9/13 CG: 8/12 | A | 11–14 | 3w 8 sessions | IPL + MGX | MGX only | 32w |
| Craig [12] | New-Zealand | 2015 | 28 (56 eyes) | 45 ± 15 | 8/20 | B | 9–13 | D0-D15-D45 3 sessions | IPL only | Sham (2nd eye) | 45d |
| Gao [30] | China | 2019 | 82 | TG: 54.4 ± 16.2 CG: 55.2 ± 16.7 | TG: 10/31 CG: 11/30 | A | 12–14 | 1 session | IPL only | AB | 1m |
| Pazo [29] | China | 2020 | 36 | TG: 30.5 ± 5.2 CG: 31.0 ± 4.3 | TG: 9/12 CG: 7/8 | A | 11–14 | 2w 2 sessions | IPL only | No trt | 28d |
| Piyacomn [37] | Thailand | 2020 | 114 | TG: 59.0 ± 12.7 CG: 59.5 ± 11.4 | TG: 10/47 CG: 5/52 | B | 9–13 | D0-D15-D45 3 sessions | IPL only | Sham | 6m |
| Rong [33] | China | 2018 | 44 (88 eyes) | 46.3 ± 16.9 | 12/32 | A | 14–16 | 4w 3 sessions | IPL + MGX | Sham + MGX (2nd eye) | 3m |
| Song [32] | China | 2022 | 71 | TG: 28.2 ± 3.6 CG: 28.1 ± 3.7 | TG: 19/26 CG: 18/23 | A | 10–14 | 3w 3 sessions | IPL only | Sham | 3m |
| Xue [35] | New-Zealand | 2020 | 87 | TG1: 48 ± 15 TG2: 56 ± 17 CG: 55 ± 14 | TG1: 9/19 TG2: 11/18 CG: 9/21 | B | 9–13 | D0-D15-D45-D75 4 sessions | IPL only 1: 4f 2: 5f | Sham | 15w |
| Yan [31] | China | 2021 | 120 | TG: 42.4 ± 14.2 CG: 41.8 ± 14.1 | TG: 16/44 CG: 12/48 | A | 12–15 | 3w 3 sessions | IPL + MGX | WC + MGX | 9w |
| Yin [34] | China | 2018 | 35 | TG: 41.6 ± 9.7 CG: 40.8 ± 14.0 | TG: 9/9 CG: 9/8 | A | 16–17 | 1m 3 sessions | IPL only | WC | 3m |
| Zarei-Ghanavati [38] | Iran | 2021 | 100 | TG: 44 ± 16 CG: 45 ± 16 | TG: 18/32 CG: 13/37 | B | 11–13 | D0-D15-D45 3 sessions | IPL only | WC | 75d |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demolin, L.; Es-Safi, M.; Soyfoo, M.S.; Motulsky, E. Intense Pulsed Light Therapy in the Treatment of Dry Eye Diseases: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 3039. https://doi.org/10.3390/jcm12083039
Demolin L, Es-Safi M, Soyfoo MS, Motulsky E. Intense Pulsed Light Therapy in the Treatment of Dry Eye Diseases: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(8):3039. https://doi.org/10.3390/jcm12083039
Chicago/Turabian StyleDemolin, Lilian, Majda Es-Safi, Muhammad Shahnawaz Soyfoo, and Elie Motulsky. 2023. "Intense Pulsed Light Therapy in the Treatment of Dry Eye Diseases: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 8: 3039. https://doi.org/10.3390/jcm12083039
APA StyleDemolin, L., Es-Safi, M., Soyfoo, M. S., & Motulsky, E. (2023). Intense Pulsed Light Therapy in the Treatment of Dry Eye Diseases: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(8), 3039. https://doi.org/10.3390/jcm12083039