
The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study
 ,
, 

Abstract
1. Introduction
2. Materials and Methods
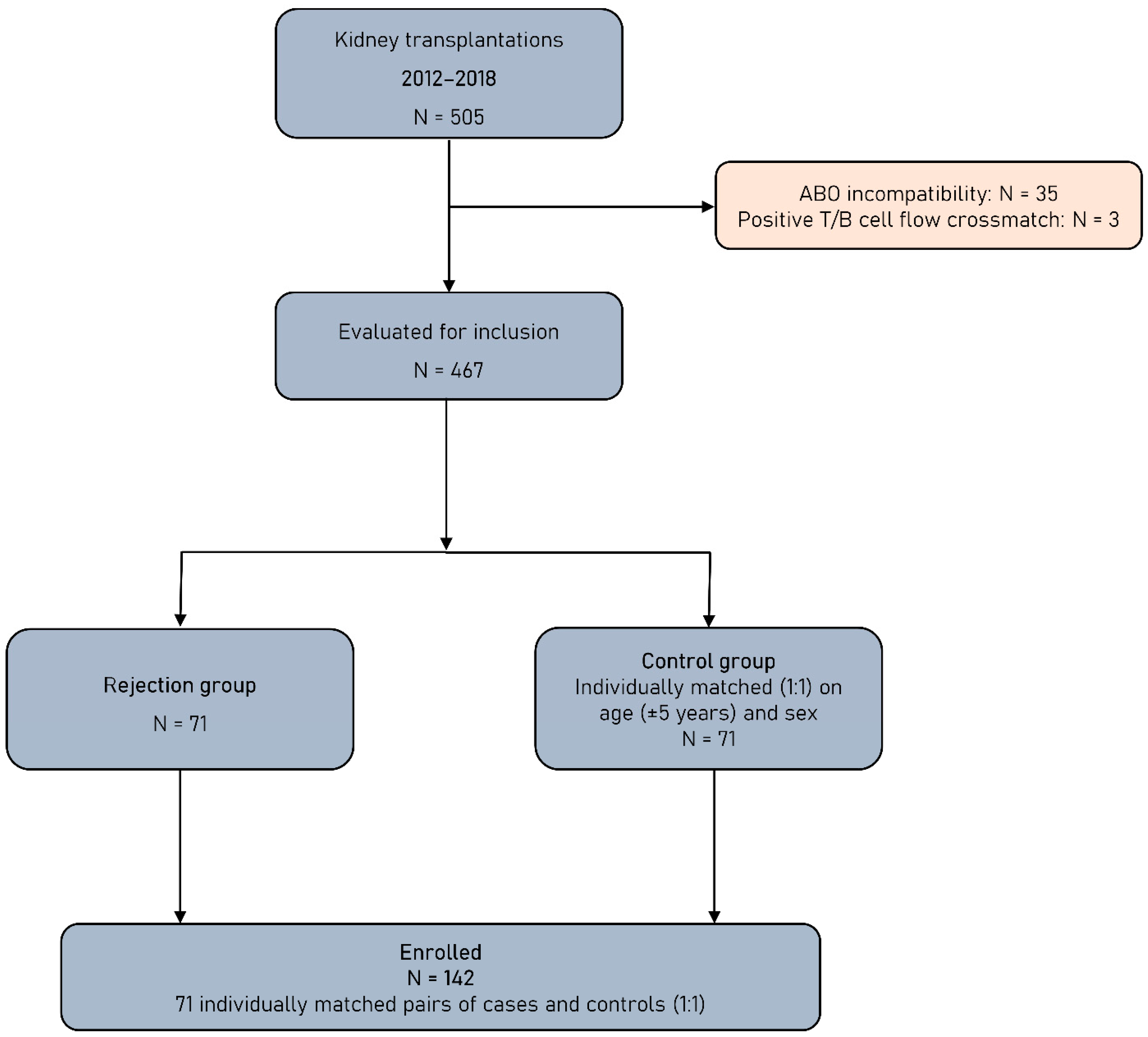
2.1. Study Population
2.2. Immunosuppression
2.3. Serum Collection and Laboratory Evaluations
2.4. Statistical Analysis
3. Results
3.1. Patients and Transplant Characteristics
3.2. Pretransplant Anti-AT1RAbs and HLA-DSAs
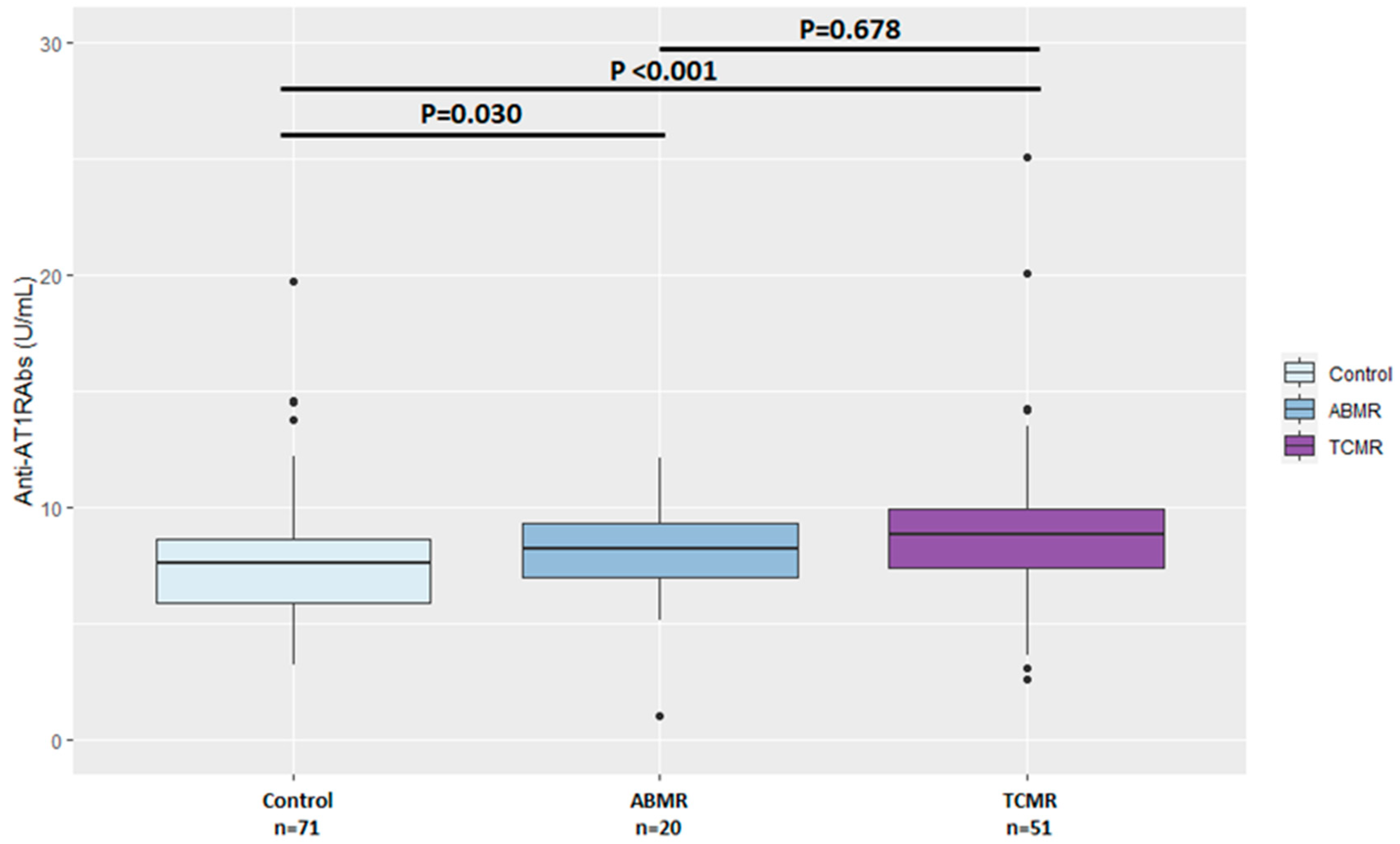
3.3. Anti-AT1RAbs and HLA-DSAs at the Time of Transplant Biopsy
3.4. Anti-AT1RAbs and HLA-DSAs at Follow-Up
3.5. Graft and Patient Outcomes
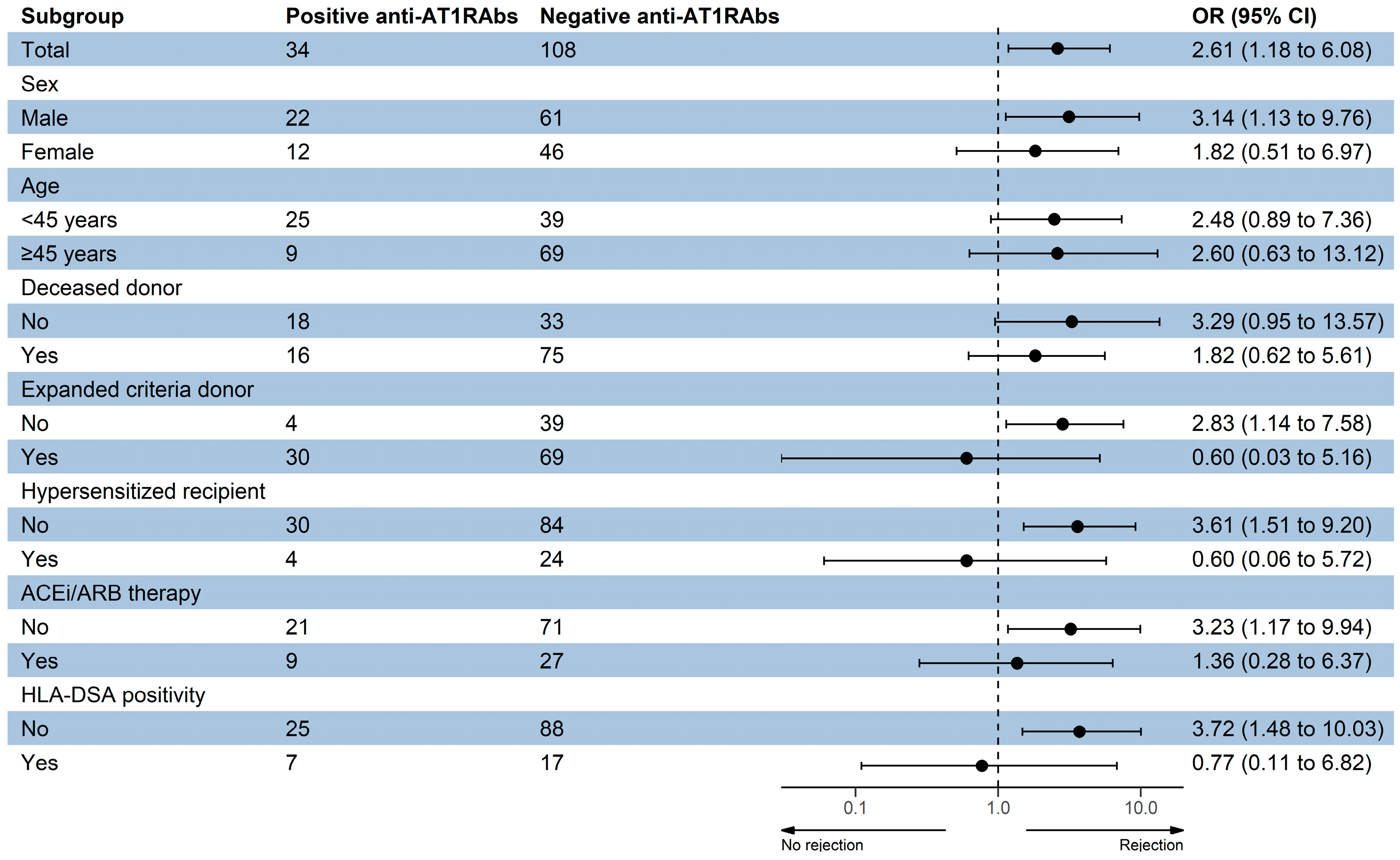
3.6. Anti-AT1RAbs Positivity and Transplant Outcomes
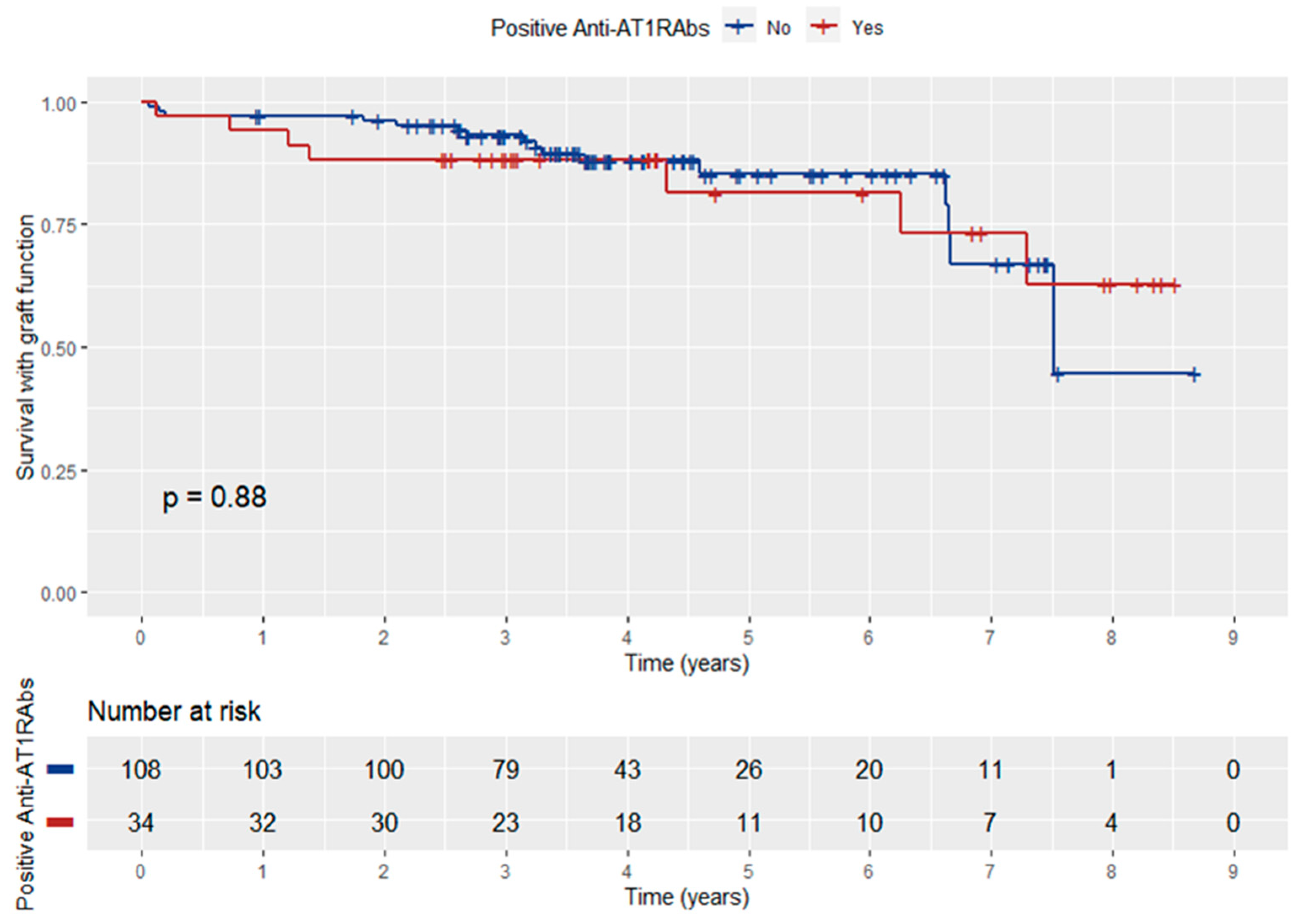
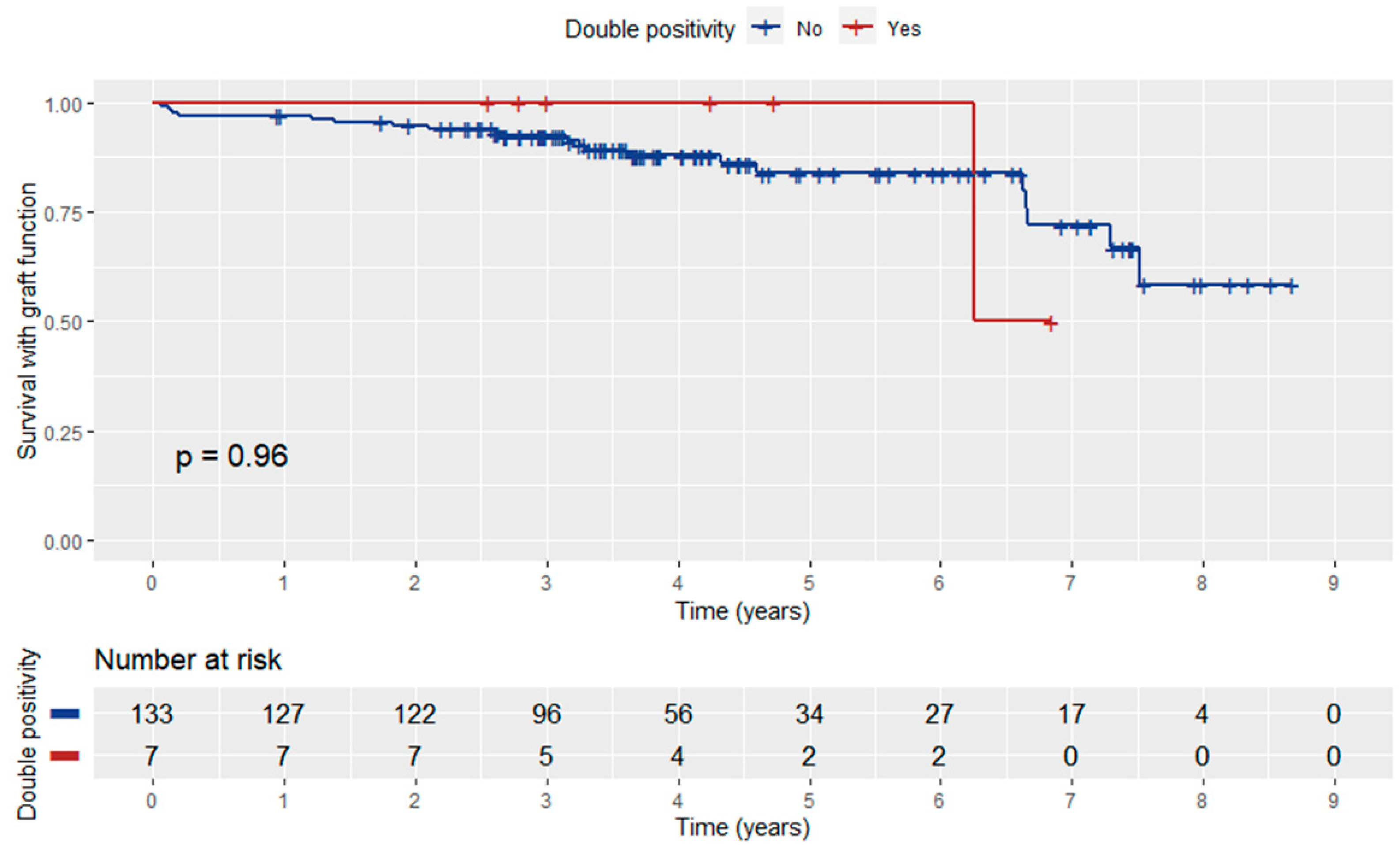
3.7. Graft Function according to Anti-AT1RAbs Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Terasaki, P.I. Deduction of the Fraction of Immunologic and Non-Immunologic Failure in Cadaver Donor Transplants. Clin. Transpl. 2003, 449–452. [Google Scholar]
- Sigdel, T.K.; Sarwal, M.M. Moving beyond HLA: A Review of NHLA Antibodies in Organ Transplantation. Hum. Immunol. 2013, 74, 1486–1490. [Google Scholar] [CrossRef] [PubMed]
- Angaswamy, N.; Tiriveedhi, V.; Sarma, N.J.; Subramanian, V.; Klein, C.; Wellen, J.; Shenoy, S.; Chapman, W.C.; Mohanakumar, T. Interplay between Immune Responses to HLA and Non-HLA Self-Antigens in Allograft Rejection. Hum. Immunol. 2013, 74, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Reed, E.F. The Importance of Non-HLA Antibodies in Transplantation. Nat. Rev. Nephrol. 2016, 12, 484–495. [Google Scholar] [CrossRef]
- Philogene, M.C.; Johnson, T.; Vaught, A.J.; Zakaria, S.; Fedarko, N. Antibodies against Angiotensin II Type 1 and Endothelin A Receptors: Relevance and Pathogenicity. Hum. Immunol. 2019, 80, 561–567. [Google Scholar] [CrossRef]
- Reinsmoen, N.L. Role of Angiotensin II Type 1 Receptor-Activating Antibodies in Solid Organ Transplantation. Hum. Immunol. 2013, 74, 1474–1477. [Google Scholar] [CrossRef] [PubMed]
- Sorohan, B.M.; Ismail, G.; Leca, N.; Tacu, D.; Obrișcă, B.; Constantinescu, I.; Baston, C.; Sinescu, I. Angiotensin II Type 1 Receptor Antibodies in Kidney Transplantation: An Evidence-Based Comprehensive Review. Transplant. Rev. 2020, 34, 100573. [Google Scholar] [CrossRef]
- Giral, M.; Foucher, Y.; Dufay, A.; Van Huyen, J.P.D.; Renaudin, K.; Moreau, A.; Philippe, A.; Hegner, B.; Dechend, R.; Heidecke, H.; et al. Pretransplant Sensitization against Angiotensin II Type 1 Receptor Is a Risk Factor for Acute Rejection and Graft Loss. Am. J. Transplant. 2013, 13, 2567–2576. [Google Scholar] [CrossRef]
- Taniguchi, M.; Rebellato, L.M.; Cai, J.; Hopfield, J.; Briley, K.P.; Haisch, C.E.; Catrou, P.G.; Bolin, P.; Parker, K.; Kendrick, W.T.; et al. Higher Risk of Kidney Graft Failure in the Presence of Anti-Angiotensin II Type-1 Receptor Antibodies. Am. J. Transplant. 2013, 13, 2577–2589. [Google Scholar] [CrossRef]
- Dragun, D.; Müller, D.N.; Bräsen, J.H.; Fritsche, L.; Nieminen-Kelhä, M.; Dechend, R.; Kintscher, U.; Rudolph, B.; Hoebeke, J.; Eckert, D.; et al. Angiotensin II Type 1–Receptor Activating Antibodies in Renal-Allograft Rejection. N. Engl. J. Med. 2005, 352, 558–569. [Google Scholar] [CrossRef]
- Alachkar, N.; Gupta, G.; Montgomery, R.A. Angiotensin Antibodies and Focal Segmental Glomerulosclerosis. N. Engl. J. Med. 2013, 368, 971–973. [Google Scholar] [CrossRef]
- Deltombe, C.; Gillaizeau, F.; Anglicheau, D.; Morelon, E.; Trébern-Launay, K.; Le Borgne, F.; Rimbert, M.; Guérif, P.; Malard-Castagnet, S.; Foucher, Y.; et al. Is Pre-Transplant Sensitization against Angiotensin II Type 1 Receptor Still a Risk Factor of Graft and Patient Outcome in Kidney Transplantation in the Anti-HLA Luminex Era? A Retrospective Study. Transpl. Int. 2017, 30, 1150–1160. [Google Scholar] [CrossRef]
- Haas, M.; Sis, B.; Racusen, L.C.; Solez, K.; Glotz, D.; Colvin, R.B.; Castro, M.C.R.; David, D.S.R.; David-Neto, E.; Bagnasco, S.M.; et al. Banff 2013 Meeting Report: Inclusion of C4d-Negative Antibody-Mediated Rejection and Antibody-Associated Arterial Lesions. Am. J. Transplant. 2014, 14, 272–283. [Google Scholar] [CrossRef]
- Sis, B.; Mengel, M.; Haas, M.; Colvin, R.B.; Halloran, P.F.; Racusen, L.C.; Solez, K.; Baldwin III, W.M.; Bracamonte, E.R.; Broecker, V.; et al. Banff ’09 Meeting Report: Antibody Mediated Graft Deterioration and Implementation of Banff Working Groups. Am. J. Transplant. 2010, 10, 464–471. [Google Scholar] [CrossRef]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef]
- Metzger, R.A.; Delmonico, F.L.; Feng, S.; Port, F.K.; Wynn, J.J.; Merion, R.M. Expanded criteria donors for kidney transplantation. Am. J. Transplant. 2003, 3, 114–125. [Google Scholar] [CrossRef]
- Vittoraki, A.; Ioannou, S.; Vallindra, H.; Siorenta, A.; Milonas, A.; Seimenis, N.; Apostolaki, M.; Iniotaki, A. Treating sera with ethylenediaminetetraacetic acid: A promising technical solution for the complement-mediated prozone effect in anti-HLA antibody detection by single antigen bead assay. Hum. Immunol. 2015, 76, 65. [Google Scholar] [CrossRef]
- Therneau, T. A Package for Survival Analysis in R; R Package Version 3.5-5; Springer: New York, NY, USA, 2023; Available online: https://CRAN.R-project.org/package=survival (accessed on 16 February 2023).
- Kassambara, A.; Kosinski, M.; Biecek, P. Drawing Survival Curves Using “ggplot2”; R Package Survminer Version 0.4.8; 2020; Available online: https://CRAN.R-project.org/package=survminer (accessed on 16 February 2023).
- Abeysekera, W. Sooriyarachchi Use of Schoenfeld’s Global Test to Test the Proportional Hazards Assumption in the Cox Proportional Hazards Model: An Application to a Clinical Study. J. Natl. Sci. Found. Sri Lanka 2009, 37, 41–51. [Google Scholar] [CrossRef]
- Reinsmoen, N.L.; Lai, C.-H.; Heidecke, H.; Haas, M.; Cao, K.; Ong, G.; Naim, M.; Wang, Q.; Mirocha, J.; Kahwaji, J.; et al. Anti-Angiotensin Type 1 Receptor Antibodies Associated with Antibody Mediated Rejection in Donor HLA Antibody Negative Patients. Transplantation 2010, 90, 1473–1477. [Google Scholar] [CrossRef] [PubMed]
- Malheiro, J.; Tafulo, S.; Dias, L.; Martins, L.S.; Fonseca, I.; Beirão, I.; Castro-Henriques, A.; Cabrita, A. Deleterious Effect of Anti-Angiotensin II Type 1 Receptor Antibodies Detected Pretransplant on Kidney Graft Outcomes Is Both Proper and Synergistic with Donor-Specific Anti-HLA Antibodies. Nephrology 2019, 24, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Huh, H.J.; Lee, K.W.; Park, J.B.; Kim, S.-J.; Huh, W.; Jang, H.R.; Kwon, G.Y.; Moon, H.H.; Kang, E.-S. Pre-Transplant Angiotensin II Type 1 Receptor Antibodies and Anti-Endothelial Cell Antibodies Predict Graft Function and Allograft Rejection in a Low-Risk Kidney Transplantation Setting. Ann. Lab. Med. 2020, 40, 398–408. [Google Scholar] [CrossRef]
- Gareau, A.J.; Wiebe, C.; Pochinco, D.; Gibson, I.W.; Ho, J.; Rush, D.N.; Nickerson, P.W. Pre-Transplant AT1R Antibodies Correlate with Early Allograft Rejection. Transpl. Immunol. 2018, 46, 29–35. [Google Scholar] [CrossRef]
- Banasik, M.; Boratyńska, M.; Kościelska-Kasprzak, K.; Kamińska, D.; Bartoszek, D.; Żabińska, M.; Myszka, M.; Zmonarski, S.; Protasiewicz, M.; Nowakowska, B.; et al. The Influence of Non-HLA Antibodies Directed against Angiotensin II Type 1 Receptor (AT1R) on Early Renal Transplant Outcomes. Transpl. Int. 2014, 27, 1029–1038. [Google Scholar] [CrossRef]
- Amico, P.; Hönger, G.; Bielmann, D.; Lutz, D.; Garzoni, D.; Steiger, J.; Mihatsch, M.J.; Dragun, D.; Schaub, S. Incidence and Prediction of Early Antibody-Mediated Rejection Due to Non-Human Leukocyte Antigen-Antibodies. Transplantation 2008, 85, 1557–1563. [Google Scholar] [CrossRef]
- Min, J.W.; Lee, H.; Choi, B.S.; Park, C.W.; Yang, C.W.; Kim, Y.-S.; Choi, Y.J.; Oh, E.-J.; Chung, B.H. Clinical Impact of Pre-Transplant Antibodies Against Angiotensin II Type I Receptor and Major Histocompatibility Complex Class I-Related Chain A in Kidney Transplant Patients. Ann. Lab. Med. 2018, 38, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Pearl, M.H.; Zhang, Q.; Palma Diaz, M.F.; Grotts, J.; Rossetti, M.; Elashoff, D.; Gjertson, D.W.; Weng, P.; Reed, E.F.; Tsai Chambers, E. Angiotensin II Type 1 Receptor Antibodies Are Associated with Inflammatory Cytokines and Poor Clinical Outcomes in Pediatric Kidney Transplantation. Kidney Int. 2018, 93, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Philogene, M.C.; Zhou, S.; Lonze, B.E.; Bagnasco, S.; Alasfar, S.; Montgomery, R.A.; Kraus, E.; Jackson, A.M.; Leffell, M.S.; Zachary, A.A. Pre-Transplant Screening for Non-HLA Antibodies: Who Should Be Tested? Hum. Immunol. 2018, 79, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Méndez, E.A.; Arreola-Guerra, J.M.; Morales-Buenrostro, L.E.; Ramírez, J.B.; Calleja, S.; Castelán, N.; Salcedo, I.; Vilatobá, M.; Contreras, A.G.; Gabilondo, B.; et al. Pre-transplant angiotensin II type 1 receptor antibodies: A risk factor for decreased kidney graft function in the early post-transplant period? Clin. Transpl. 2013, 343–350. [Google Scholar]
- Cuevas, E.; Arreola-Guerra, J.M.; Hernández-Méndez, E.A.; Salcedo, I.; Castelán, N.; Uribe-Uribe, N.O.; Vilatobá, M.; Contreras-Saldívar, A.G.; Sánchez-Cedillo, A.I.; Ramírez, J.B.; et al. Pretransplant Angiotensin II Type 1-Receptor Antibodies Are a Risk Factor for Earlier Detection of de Novo HLA Donor-Specific Antibodies. Nephrol. Dial. Transplant. 2016, 31, 1738–1745. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Viglietti, D.; Bouatou, Y.; Philippe, A.; Pievani, D.; Aubert, O.; Duong Van Huyen, J.-P.; Taupin, J.-L.; Glotz, D.; Legendre, C.; et al. Non-HLA Agonistic Anti-Angiotensin II Type 1 Receptor Antibodies Induce a Distinctive Phenotype of Antibody-Mediated Rejection in Kidney Transplant Recipients. Kidney Int. 2019, 96, 189–201. [Google Scholar] [CrossRef]
- Carroll, R.P.; Riceman, M.; Hope, C.M.; Zeng, A.; Deayton, S.; Bennett, G.D.; Coates, P.T. Angiotensin II Type-1 Receptor Antibody (AT1Rab) Associated Humoral Rejection and the Effect of Peri Operative Plasma Exchange and Candesartan. Hum. Immunol. 2016, 77, 1154–1158. [Google Scholar] [CrossRef]
- Philogene, M.C.; Bagnasco, S.; Kraus, E.S.; Montgomery, R.A.; Dragun, D.; Leffell, M.S.; Zachary, A.A.; Jackson, A.M. Anti-Angiotensin II Type 1 Receptor and Anti-Endothelial Cell Antibodies: A Cross-Sectional Analysis of Pathological Findings in Allograft Biopsies. Transplantation 2017, 101, 608–615. [Google Scholar] [CrossRef]
- Lee, J.; Huh, K.H.; Park, Y.; Park, B.G.; Yang, J.; Jeong, J.C.; Lee, J.; Park, J.B.; Cho, J.-H.; Lee, S.; et al. The Clinicopathological Relevance of Pretransplant Anti-Angiotensin II Type 1 Receptor Antibodies in Renal Transplantation. Nephrol. Dial. Transplant. 2017, 32, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Gimferrer, I.; Warner, P.; Nelson, K.; Sibulesky, L.; Bakthavatsalam, R.; Leca, N. Preformed Angiotensin II Type-1 Receptor Antibodies Are Associated With Rejection After Kidney Transplantation: A Single-Center, Cohort Study. Transplant. Proc. 2018, 50, 3467–3472. [Google Scholar] [CrossRef] [PubMed]
- Kang, Z.-Y.; Liu, C.; Liu, W.; Li, D.-H. Effect of Anti-Angiotensin II Type 1 Receptor Antibodies on the Outcomes of Kidney Transplantation: A Systematic Review and Meta-Analysis. Nephrol. Dial. Transplant. 2022, 37, 1171–1180. [Google Scholar] [CrossRef]
- Arnold, M.-L.; Ntokou, I.-S.; Doxiadis, I.I.N.; Spriewald, B.M.; Boletis, J.N.; Iniotaki, A.G. Donor-Specific HLA Antibodies: Evaluating the Risk for Graft Loss in Renal Transplant Recipients with Isotype Switch from Complement Fixing IgG1/IgG3 to Noncomplement Fixing IgG2/IgG4 Anti-HLA Alloantibodies. Transpl. Int. 2014, 27, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Lukitsch, I.; Kehr, J.; Chaykovska, L.; Wallukat, G.; Nieminen-Kelhä, M.; Batuman, V.; Dragun, D.; Gollasch, M. Renal Ischemia and Transplantation Predispose to Vascular Constriction Mediated by Angiotensin II Type 1 Receptor-Activating Antibodies. Transplantation 2012, 94, 8–13. [Google Scholar] [CrossRef]
- Delville, M.; Lamarthée, B.; Pagie, S.; See, S.B.; Rabant, M.; Burger, C.; Gatault, P.; Giral, M.; Thaunat, O.; Arzouk, N.; et al. Early Acute Microvascular Kidney Transplant Rejection in the Absence of Anti-HLA Antibodies Is Associated with Preformed IgG Antibodies against Diverse Glomerular Endothelial Cell Antigens. J. Am. Soc. Nephrol. 2019, 30, 692–709. [Google Scholar] [CrossRef]
- Zorn, E.; See, S.B. Is There a Role for Natural Antibodies in Rejection Following Transplantation? Transplantation 2019, 103, 1612–1619. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients (n = 142) | Rejection Group (n = 71) | Control Group (n = 71) | p-Value |
|---|---|---|---|---|
| Age at transplantation | 45.8 ± 13.0 | 42.8 ± 12.9 | 48.8 ± 12.5 | 0.005 |
| Male sex | 83 (58.5%) | 44 (62.0%) | 39 (54.9%) | 0.496 |
| Donor age | 54.8 ± 13.9 | 54.6 ± 12.6 | 54.9 ± 15.3 | 0.890 |
| Donor male sex | 56 (39.4%) | 26 (36.6%) | 30 (42.2%) | 0.607 |
| Deceased donor | 91 (64.1%) | 40 (56.3%) | 51 (71.8%) | 0.080 |
| Expanded criteria donor | 43 (30.3%) | 15 (21.1%) | 28 (39.4%) | 0.131 |
| Cold ischemia time (h) | 17 [15–20.6] | 17.5 [16–19.5] | 17 [14.8–20.8] | 0.316 |
| Time on dialysis (years) | 6.3 [2.1–9.5] | 4.2 [1.8–8.2] | 6.9 [2.6–10.0] | 0.103 |
| Primary renal disease | ||||
| Diabetes mellitus | 4 (2.8%) | 3 (4.2%) | 1 (1.4%) | 0.085 |
| Hypertension | 8 (5.6%) | 1 (1.4%) | 7 (9.8%) | |
| Glomerulonephritis | 33 (23.2%) | 18 (25.3%) | 15 (21.1%) | |
| Polycystic kidney disease | 21 (14.7%) | 8 (11.2) | 13 (18.3%) | |
| Obstructive uropathy/Reflux nephropathy/Interstitial nephritis | 18 (12.6%) | 13 (18.3%) | 5 (7.0%) | |
| Unknown | 50 (35.2%) | 25 (35.2%) | 25 (35.2%) | |
| Other | 8 (5.6%) | 3 (4.2%) | 5 (7.0%) | |
| Re-transplantation | 17 (12.0%) | 12 (16.9%) | 5 (7.0%) | 0.119 |
| Hypersensitized recipient | 29 (20.4%) | 18 (25.3%) | 11 (15.4%) | 0.271 |
| HLA mismatches | 3 [2–4] | 3 [3, 4] | 3 [2–4] | 0.679 |
| Delayed graft function | 79 (55.6%) | 41 (57.7%) | 38 (53.5%) | 0.734 |
| Induction immunosuppression | ||||
| Basiliximab | 133 (93.7%) | 68 (95.8%) | 65 (91.5%) | 0.493 |
| Anti-thymocyte globulin | 9 (6.3%) | 3 (4.2%) | 6 (8.5%) | |
| Maintenance immunosuppression | ||||
| MPA/Tacrolimus | 138 (97.2%) | 68 (95.8%) | 70 (98.6%) | 0.620 |
| MPA/Ciclosporin | 3 (2.1%) | 2 (2.8%) | 1 (1.4% | |
| Tacrolimus/Everolimus | 1 (0.7%) | 1 (1.4%) | 0 (0.0%) | |
| ACEi/ARB pre-KTx | 36/128 (28.1%) | 14/60 (23.3%) | 22/68 (32.4%) | 0.350 |
| ACEi/ARB post-KTx | 52 (36.6%) | 26 (36.6%) | 26 (36.6%) | 1 |
| Follow-up period (years) | 3.7 [2.9–5.2] | 3.4 [2.6–4.8] | 3.7 [3.3–5.5] | 0.059 |
| Time from transplantation to rejection (days) | - | 28 [12–375] | - | N/A |
| Time of follow-up after rejection (years) | - | 2.9 [2–3.9] | - | N/A |
| Parameter | All Patients (n = 142) | Rejection Group (n = 71) | Control Group (n = 71) | p-Value |
|---|---|---|---|---|
| Rejection classification (Banff 2009–2013) | ||||
| ABMR | 20 (14.1%) | 20 (28.2%) | - | |
| Acute/active | 13 (18.3%) | - | ||
| Chronic active | 7 (9.8%) | - | ||
| Borderline changes | 8 (5.6%) | 8 (11.2%) | - | |
| TCMR | 43 (30.3%) | 43 (60.6%) | - | |
| Acute | 38 (53.6%) | - | ||
| Grade IA | 16 | |||
| Grade IB | 10 | |||
| Grade IIA | 6 | |||
| Grade IIB | 6 | |||
| Chronic active | 5 (7.0%) | - | ||
| Anti-AT1RAbs pre-KTx (U/mL) | 8.2 [6.5–9.8] | 9.0 [7.4–11.3] | 7.6 [5.9–8.7] | <0.001 |
| Anti-AT1Rabs pre-KTx ≥ 10 U/mL | 34 (23.9%) | 23 (32.4%) | 11 (15.5%) | 0.031 |
| HLA-DSA pre-KTx (MFI > 1000) | 25 (17.6%) | 19 (26.7%) | 6 (8.4%) | 0.010 |
| First-year serum creatinine (mg/dL) | 1.6 [1.3–2.2] | 1.8 [1.4–2.9] | 1.6 [1.2–2.1] | 0.036 |
| End-of-follow-up serum creatinine (mg/dL) | 1.5 [1.2–2.0] | 1.8 [1.4–2.6] | 1.3 [1.1–1.6] | <0.001 |
| First-year eGFR (CKD-EPI) (mL/min/1.73 m2) | 42 [31–58] | 39 [24.3–58] | 43 [33.5–57] | 0.229 |
| End-of-follow-up eGFR (CKD-EPI) (mL/min/1.73 m2) | 47.5 [34.3–60] | 38 [23–56] | 52 [44.5–65] | <0.001 |
| Graft loss | 14 (9.9%) | 13 (18.3%) | 1 (1.4%) | 0.001 |
| Death | 9 (6.3%) | 7 (9.9%) | 2 (2.8%) | 0.166 |
| Antibodies | Pre-KTx | At Biopsy | ABMR C4d (+) | ABMR C4d (−) | TCMR |
|---|---|---|---|---|---|
| Anti-AT1RAbs (+) HLA-DSA (−) | 18 (25.4%) | 8 (11.2%) | 1 | 0 | 7 |
| Anti-AT1RAbs (−) HLA-DSA (+) | 14 (19.7%) | 22 (31%) | 5 | 7 | 10 |
| Anti-AT1RAbs (+) HLA-DSA (+) | 5 (7.0%) | 7 (9.9%) | 0 | 3 | 4 |
| Anti-AT1RAbs (−) HLA-DSA (−) | 34 (47.9) | 34 (47.9%) | 1 | 3 | 30 |
| Model | Odds Ratio | 95% Confidence Intervals | p-Value |
|---|---|---|---|
| Crude | 2.61 | 1.18–6.08 | 0.021 |
| Model 1 | 1.88 | 0.80–4.57 | 0.153 |
| Model 2 | 1.72 | 0.72–4.21 | 0.227 |
| Model 3 | 1.72 | 0.67–4.51 | 0.258 |
| Model 4 | 1.97 | 0.75–5.38 | 0.174 |
| Model | Hazard Ratio | 95% Confidence Intervals | p-Value |
|---|---|---|---|
| Crude | 1.07 | 0.43–2.69 | 0.878 |
| Model 1 | 0.79 | 0.31–2.02 | 0.619 |
| Model 2 | 0.82 | 0.32–2.14 | 0.690 |
| Model 3 | 0.43 | 0.12–1.36 | 0.215 |
| Model 4 | 0.49 | 0.13–1.89 | 0.302 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filiopoulos, V.; Vittoraki, A.; Vallianou, K.; Bellos, I.; Markaki, P.; Liapis, G.; Marinaki, S.; Iniotaki, A.; Boletis, I.N. The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study. J. Clin. Med. 2023, 12, 3112. https://doi.org/10.3390/jcm12093112
Filiopoulos V, Vittoraki A, Vallianou K, Bellos I, Markaki P, Liapis G, Marinaki S, Iniotaki A, Boletis IN. The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study. Journal of Clinical Medicine. 2023; 12(9):3112. https://doi.org/10.3390/jcm12093112
Chicago/Turabian StyleFiliopoulos, Vassilis, Angeliki Vittoraki, Kalliopi Vallianou, Ioannis Bellos, Pavlina Markaki, George Liapis, Smaragdi Marinaki, Aliki Iniotaki, and Ioannis N. Boletis. 2023. "The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study" Journal of Clinical Medicine 12, no. 9: 3112. https://doi.org/10.3390/jcm12093112
APA StyleFiliopoulos, V., Vittoraki, A., Vallianou, K., Bellos, I., Markaki, P., Liapis, G., Marinaki, S., Iniotaki, A., & Boletis, I. N. (2023). The Influence of Antibodies against Angiotensin II Type-1 Receptor on the Outcome of Kidney Transplantation: A Single-Center Retrospective Study. Journal of Clinical Medicine, 12(9), 3112. https://doi.org/10.3390/jcm12093112