
Combination of Intracardiac Echocardiography and Contact Force Sensing for Left Ventricular Papillary Muscle Arrhythmias

 ,
,
Abstract
1. Introduction
2. Methods Section
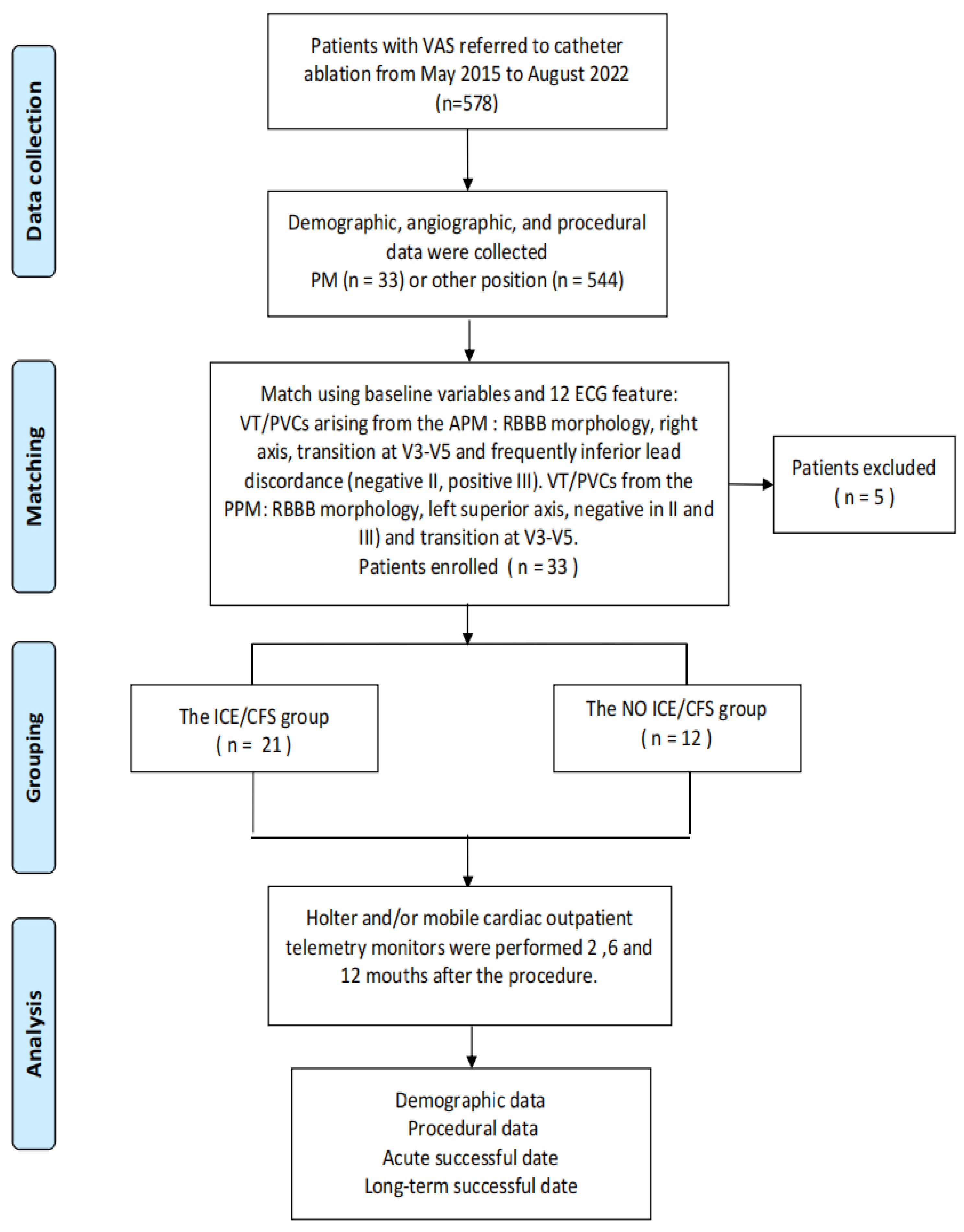
2.1. Patient Characteristics
2.2. Electrophysiology Study, Mapping and Ablation
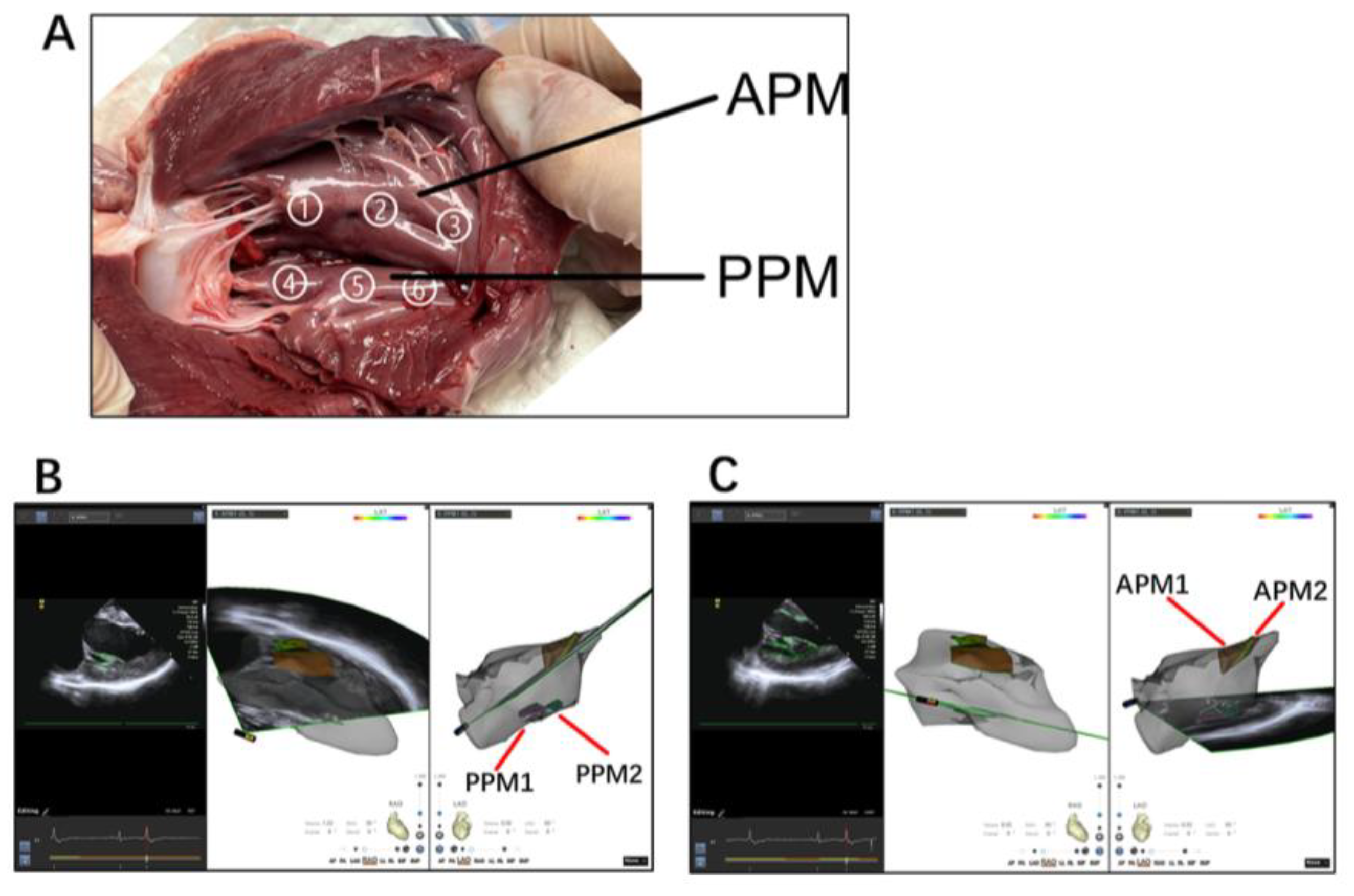
2.2.1. Intracardiac Echocardiography
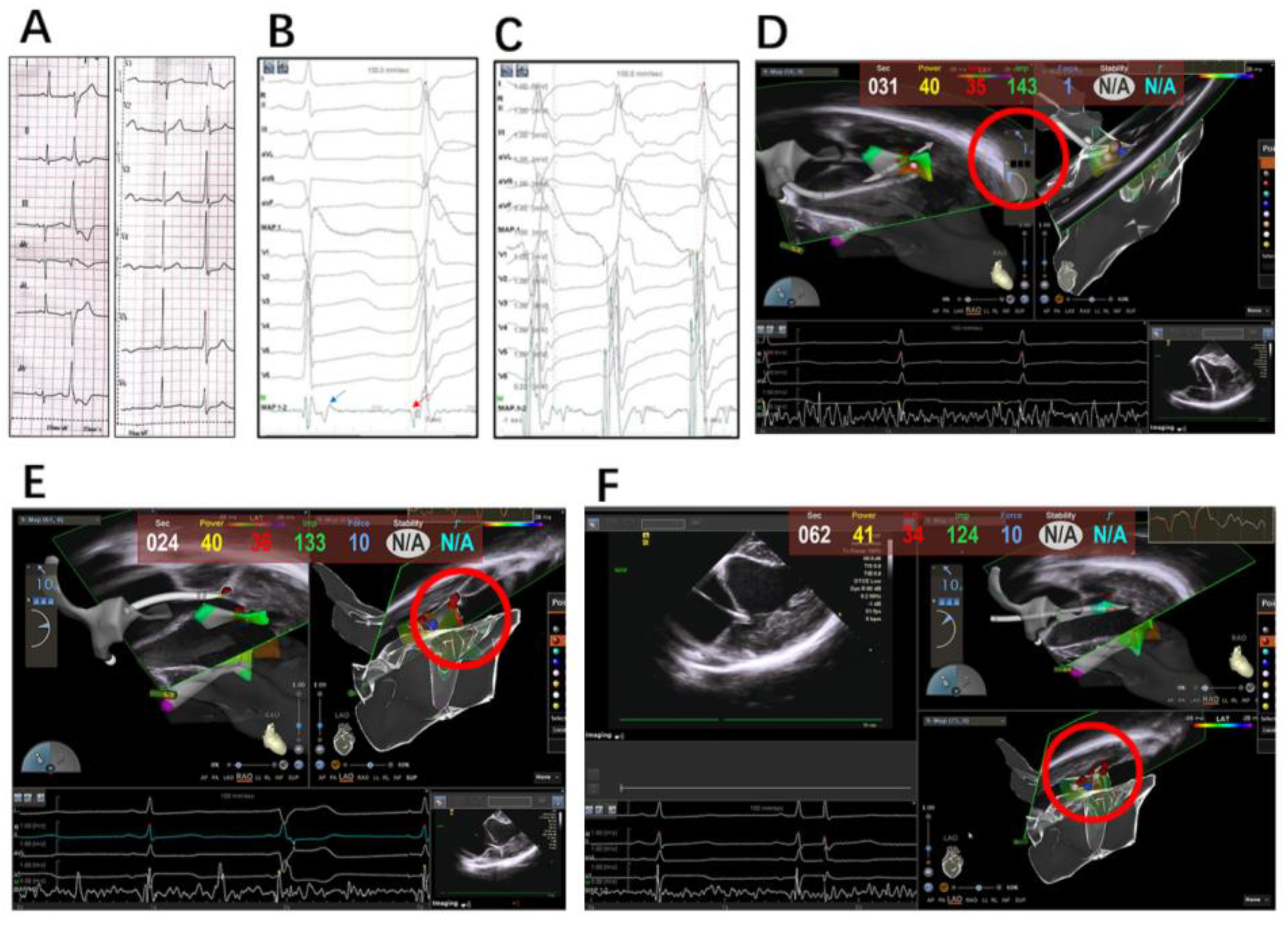
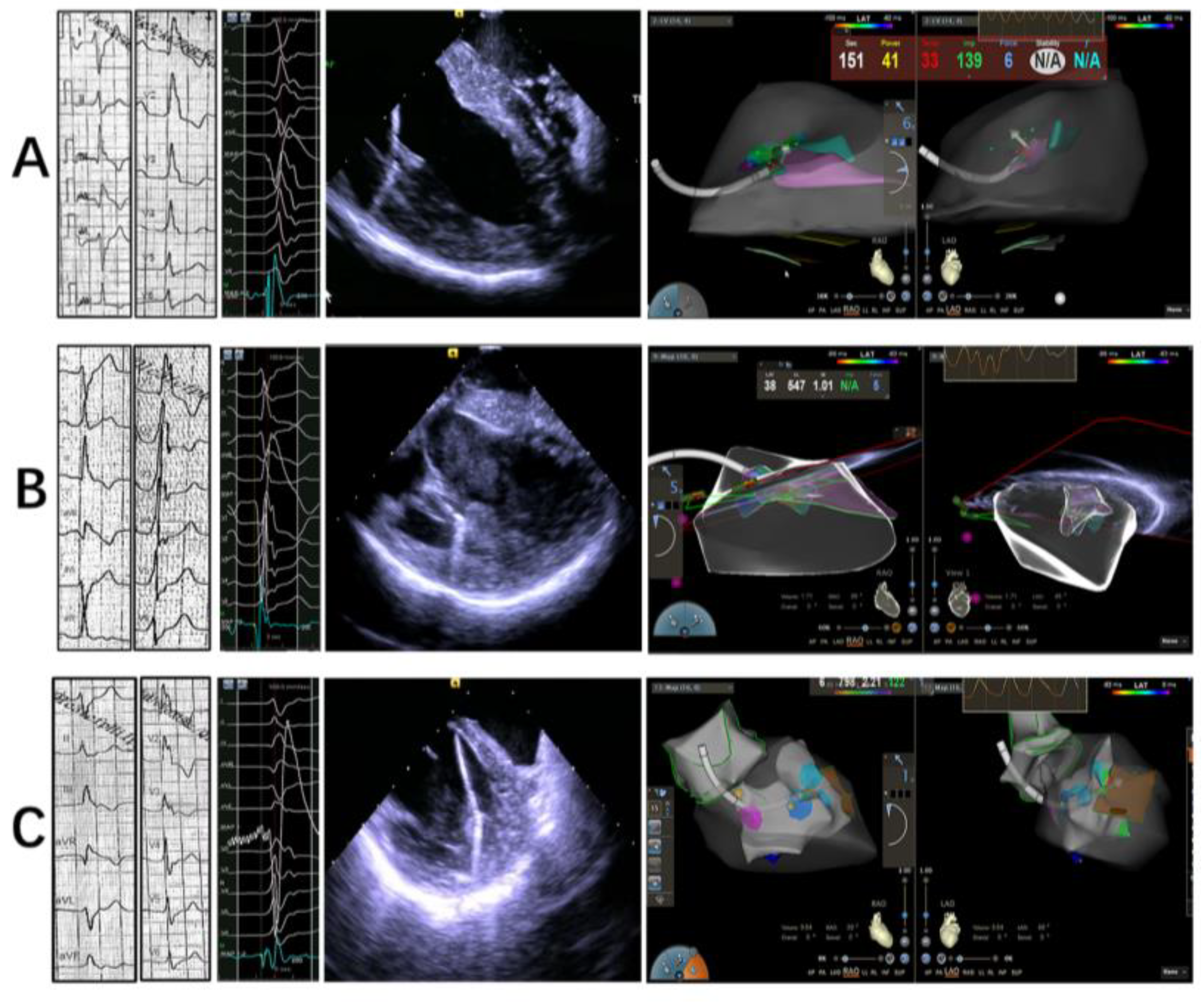
2.2.2. Mapping and Ablation
2.3. Outcomes and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Procedural Characteristics
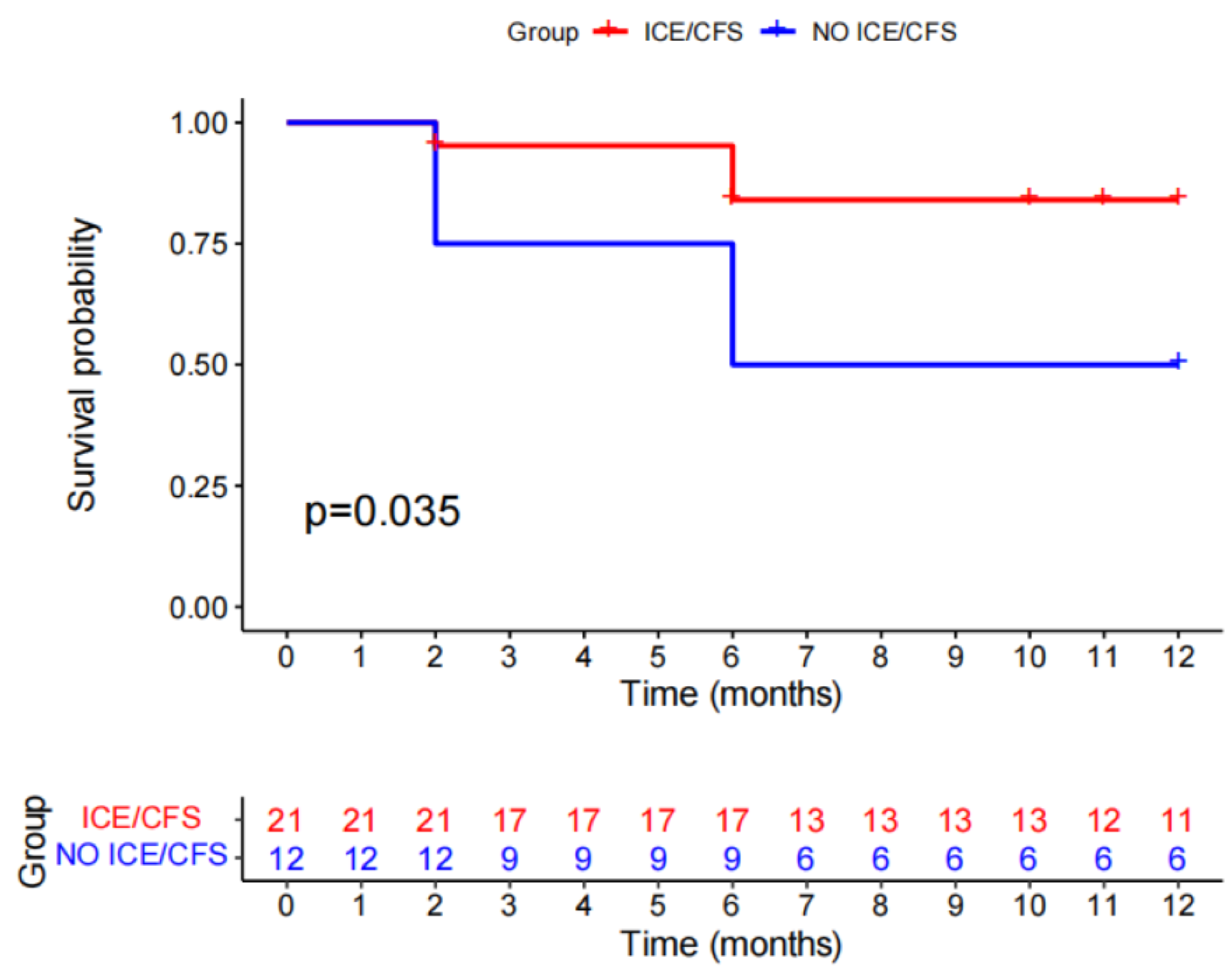
3.3. Outcome and Follow-Up
4. Discussion
4.1. Integration of Echocardiography and 3D Mapping
4.2. Contact Force
4.3. Optimizing Ablation Lesions
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bogun, F.; Desjardins, B.; Crawford, T.; Good, E.; Jongnarangsin, K.; Oral, H.; Chugh, A.; Pelosi, F.; Morady, F. Post-infarction ventricular arrhythmias originating in papillary muscles. J. Am. Coll. Cardiol. 2008, 51, 1794–1802. [Google Scholar] [CrossRef] [PubMed]
- Good, E.; Desjardins, B.; Jongnarangsin, K.; Oral, H.; Chugh, A.; Ebinger, M.; Pelosi, F.; Morady, F.; Bogun, F. Ventricular arrhythmias originating from a papillary muscle in patients without prior infarction: A comparison with fascicular arrhythmias. Heart Rhythm. 2008, 5, 1530–1537. [Google Scholar] [CrossRef] [PubMed]
- Doppalapudi, H.; Yamada, T.; McElderry, H.T.; Plumb, V.J.; Epstein, A.E.; Kay, G.N. Ventricular tachycardia originating from the posterior papillary muscle in the left ventricle: A distinct clinical syndrome. Circ. Arrhythm. Electrophysiol. 2008, 1, 23–29. [Google Scholar] [CrossRef]
- Van Herendael, H.; Zado, E.S.; Haqqani, H.; Tschabrunn, C.M.; Callans, D.J.; Frankel, D.S.; Lin, D.; Garcia, F.; Hutchinson, M.D.; Riley, M.; et al. Catheter ablation of ventricular fibrillation: Importance of left ventricular outflow tract and papillary muscle triggers. Heart Rhythm. 2014, 11, 566–573. [Google Scholar] [CrossRef]
- Santoro, F.; Di Biase, L.; Hranitzky, P.; Sanchez, J.E.; Santangeli, P.; Perini, A.P.; Burkhardt, J.D.; Natale, A. Ventricular fibrillation triggered by PVCs from papillary muscles: Clinical features and ablation. J. Cardiovasc. Electrophysiol. 2014, 25, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Dal-Bianco, J.P.; Levine, R.A. Anatomy of the mitral valve apparatus: Role of 2D and 3D echocardiography. Cardiol. Clin. 2013, 31, 151–164. [Google Scholar] [CrossRef]
- Madhavan, M.; Asirvatham, S.J. The fourth dimension: Endocavitary ventricular tachycardia. Circ. Arrhythm. Electrophysiol. 2010, 3, 302–304. [Google Scholar] [CrossRef]
- Yamada, T.; Doppalapudi, H.; McElderry, H.T.; Okada, T.; Murakami, Y.; Inden, Y.; Yoshida, Y.; Yoshida, N.; Murohara, T.; Epstein, A.E.; et al. Electrocardiographic and electrophysiological characteristics in idiopathic ventricular arrhythmias originating from the papillary muscles in the left ventricle: Relevance for catheter ablation. Circ. Arrhythm. Electrophysiol. 2010, 3, 324–331. [Google Scholar] [CrossRef]
- Enriquez, A.; Supple, G.E.; Marchlinski, F.E.; Garcia, F.C. How to map and ablate papillary muscle ventricular arrhythmias. Heart Rhythm. 2017, 14, 1721–1728. [Google Scholar] [CrossRef]
- Mochizuki, A.; Nagahara, D.; Takahashi, H.; Saito, R.; Fujito, T.; Miura, T. Worsening of mitral valve regurgitation after radiofrequency catheter ablation of ventricular arrhythmia originating from a left ventricular papillary muscle. HeartRhythm Case Rep. 2017, 3, 215–218. [Google Scholar] [CrossRef][Green Version]
- Desimone, C.V.; Hu, T.; Ebrille, E.; Syed, F.F.; Vaidya, V.R.; Cha, Y.M.; Valverde, A.M.; Friedman, P.A.; Suri, R.M.; Asirvatham, S.J. Catheter ablation related mitral valve injury: The importance of early recognition and rescue mitral valve repair. J. Cardiovasc. Electrophysiol. 2014, 25, 971–975. [Google Scholar] [CrossRef]
- Latchamsetty, R.; Yokokawa, M.; Morady, F.; Kim, H.M.; Mathew, S.; Tilz, R.; Kuck, K.H.; Nagashima, K.; Tedrow, U.; Stevenson, W.G.; et al. Multicenter Outcomes for Catheter Ablation of Idiopathic Premature Ventricular Complexes. JACC Clin. Electrophysiol. 2015, 1, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Proietti, R.; Rivera, S.; Dussault, C.; Essebag, V.; Bernier, M.L.; Ayala-Paredes, F.; Badra-Verdu, M.; Roux, J.F. Intracardiac echo-facilitated 3D electroanatomical mapping of ventricular arrhythmias from the papillary muscles: Assessing the ‘fourth dimension’ during ablation. Europace 2017, 19, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Rivera, S.; Tomas, L.; Ricapito, M.P.; Nicolas, V.; Reinoso, M.; Caro, M.; Mondragon, I.; Albina, G.; Giniger, A.; Scazzuso, F. Updated results on catheter ablation of ventricular arrhythmias arising from the papillary muscles of the left ventricle. J. Arrhythm. 2019, 35, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Mariani, M.V.; Piro, A.; Magnocavallo, M.; Chimenti, C.; Della Rocca, D.; Santangeli, P.; Natale, A.; Fedele, F.; Lavalle, C. Catheter ablation for papillary muscle arrhythmias: A systematic review. Pacing Clin. Electrophysiol. 2022, 45, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Gianni, C.; Sanchez, J.E.; Della Rocca, D.G.; Al-Ahmad, A.; Horton, R.P.; Di Biase, L.; Natale, A. Intracardiac Echocardiography to Guide Catheter Ablation of Atrial Fibrillation. Card. Electrophysiol. Clin. 2021, 13, 303–311. [Google Scholar] [CrossRef]
- Goya, M.; Frame, D.; Gache, L.; Ichishima, Y.; Tayar, D.O.; Goldstein, L.; Lee, S.H.Y. The use of intracardiac echocardiography catheters in endocardial ablation of cardiac arrhythmia: Meta-analysis of efficiency, effectiveness, and safety outcomes. J. Cardiovasc. Electrophysiol. 2020, 31, 664–673. [Google Scholar] [CrossRef]
- Lin, A.N.; Shirai, Y.; Liang, J.J.; Chen, S.; Kochar, A.; Hyman, M.C.; Santangeli, P.; Schaller, R.D.; Frankel, D.S.; Arkles, J.S.; et al. Strategies for Catheter Ablation of Left Ventricular Papillary Muscle Arrhythmias: An Institutional Experience. JACC Clin. Electrophysiol. 2020, 6, 1381–1392. [Google Scholar] [CrossRef]
- Reichlin, T.; Baldinger, S.H.; Pruvot, E.; Bisch, L.; Ammann, P.; Altmann, D.; Berte, B.; Kobza, R.; Haegeli, L.; Schlatzer, C.; et al. Impact of contact force sensing technology on outcome of catheter ablation of idiopathic pre-mature ventricular contractions originating from the outflow tracts. Europace 2021, 23, 603–609. [Google Scholar] [CrossRef]
- Wo, H.T.; Liao, F.C.; Chang, P.C.; Chou, C.C.; Wen, M.S.; Wang, C.C.; Yeh, S.J. Circumferential ablation at the base of the left ventricular papillary muscles: A highly effective approach for ventricular arrhythmias originating from the papillary muscles. Int. J. Cardiol. 2016, 220, 876–882. [Google Scholar] [CrossRef]
- Nussinovitch, U.; Wang, P.; Narayan, S.; Viswanathan, M.; Badhwar, N.; Zheng, L.; Sauer, W.H.; Nguyen, D.T. Perpendicular catheter orientation during papillary muscle ablation results in larger, deeper lesions. J. Cardiovasc. Electrophysiol. 2022, 33, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Yokokawa, M.; Good, E.; Desjardins, B.; Crawford, T.; Jongnarangsin, K.; Chugh, A.; Pelosi, F., Jr.; Oral, H.; Morady, F.; Bogun, F. Predictors of successful catheter ablation of ventricular arrhythmias arising from the papillary muscles. Heart Rhythm. 2010, 7, 1654–1659. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | ICE/CFS Group (n = 21) | No ICE/CFS Group (n = 12) | Overall (n = 33) | p Value |
|---|---|---|---|---|
| Demographics | ||||
| Age (y, Mean ± SD) | 48 ± 16 | 51 ± 13 | 49 ± 15 | 0.651 |
| Gender (%male) | 71.40% | 66.7% | 69.7% | 1.000 |
| Smoking (%) | 42.90% | 33.33% | 39.40% | 0.719 |
| Comorbidities (%) | ||||
| Coronary heart disease | 42.90% | 25.00% | 36.40% | 0.457 |
| Hypertension | 25.80% | 16.70% | 24.20% | 0.678 |
| Duration of symptoms | 11.88 ± 14.95 | 20.55 ± 21.96 | 15.29 ± 18.16 | 0.187 |
| Cardiac function | ||||
| LVEF | 0.57 ± 0.09 | 0.59 ± 0.07 | 0.58 ± 0.08 | 0.823 |
| LVD | 52.15 ± 4.90 | 48.44 ± 5.65 | 51.00 ± 5.33 | 0.084 |
| LAD | 38.65 ± 5.77 | 37.78 ± 6.66 | 38.38 ± 5.96 | 0.723 |
| Laboratory test | ||||
| CNTI (ng/dL) | 1.91 ± 1.74 | 1.60 ± 1.53 | 1.82 ± 1.66 | 0.391 |
| CK-MB (ng/dL) | 3.13 ± 7.67 | 0.71 ± 0.21 | 2.29 ± 6.25 | 0.938 |
| CK (u/L) | 129.57 ± 209.89 | 60.25 ± 32.13 | 110.45 ± 180.88 | 0.069 |
| NT-pro BNP (ng/mL) | 478.25 ± 836.15 | 335.67 ± 278.43 | 449.73 ± 753.40 | 0.933 |
| AAD Pre | 66.70% | 83.30% | 72.70% | 0.429 |
| AAD Post | 76.20% | 75.00% | 75.80% | 1.000 |
| Variables | ICE/CFS Group (n = 21) | No ICE/CFS Group (n = 12) | p Value |
|---|---|---|---|
| LV PAP VA target | 1.000 | ||
| Anterolateral PM | 7 (33.33%) | 4 (33.33%) | |
| Posteromedial PM | 14 (66.67%) | 8 (66.67%) | |
| Location targeted | NA | ||
| Tip | 5 (23.80%) | NA | |
| Body | 11 (52.38%) | NA | |
| Base | 5 (23.80%) | NA | |
| Hyperechogenicity on ICE | 6 (28.50%) | NA | NA |
| Type of LV access | 1.000 | ||
| Transaortic approach | 14 (66.67%) | 8 (66.67%) | |
| Combined access | 7 (33.33%) | 4 (33.33%) | |
| Average contact force (g) | 7.52 ± 3.311 | NA | NA |
| Total RF duration (s) | 258.24 ± 141.39 | 302.83 ± 135.80 | 0.405 |
| Total procedure time (min) | 157.38 ± 49.38 | 158.08 ± 67.88 | 0.973 |
| Total X-ray time (S) | 165.67 ± 47.80 | 365.00 ± 183.73 | <0.001 |
| Lesions | 4.90 ± 2.23 | 10.17 ± 5.89 | 0.006 |
| Early site (ms) | 35.10 ± 5.08 | 34.25 ± 4.35 | 0.618 |
| Acute success | 100% | 66.67% | 0.012 |
| Long-time recurrence | 14.20% | 50.00% | 0.044 |
| Cost performance | 7864.86 ± 769.79 | 4519.03 ± 1504.44 | <0.001 |
| N= | Age | Sex | Clinical | ICE/CFS | Origin | Location | PVC Burden | |
|---|---|---|---|---|---|---|---|---|
| Preprocedure (%) | Postprocedure (%) | |||||||
| Patient 1 | 34 | F | PVC | 0 | PPM | NA | 15.65 | 11.94 |
| Patient 2 | 62 | M | PVC | 0 | PPM | NA | 20.82 | 0.95 |
| Patient 3 | 26 | F | PVC | 0 | PPM | NA | 17.98 | 0.48 |
| Patient 4 | 56 | M | PVC and VT | 0 | PPM | NA | 24.41 | 0.61 |
| Patient 5 | 55 | F | PVC | 0 | APM | NA | 22.46 | 13.48 |
| Patient 6 | 61 | M | PVC | 0 | PPM | NA | 16.99 | 15.12 |
| Patient 7 | 36 | M | PVC | 0 | PPM | NA | 19.43 | 16.98 |
| Patient 8 | 52 | M | PVC | 0 | PPM | NA | 11.37 | 2.46 |
| Patient 9 | 48 | M | PVC | 0 | APM | NA | 24.53 | 11.35 |
| Patient 10 | 53 | M | PVC | 0 | APM | NA | 17.53 | 0.20 |
| Patient 11 | 69 | F | PVC | 0 | APM | NA | 11.63 | 1.43 |
| Patient 12 | 74 | F | PVC and VT | 0 | PPM | NA | 13.20 | 10.37 |
| Patient 13 | 46 | M | PVC | 1 | PPM | Base | 31.20 | 0.59 |
| Patient 14 | 63 | M | PVC | 1 | APM | Body | 19.95 | 0.88 |
| Patient 15 | 59 | M | PVC and VT | 1 | PPM | Body | 15.16 | 1.27 |
| Patient 16 | 39 | M | PVC | 1 | APM | Tip | 20.18 | 0.66 |
| Patient 17 | 5F | F | PVC | 1 | APM | Base | 16.00 | 16.20 |
| Patient 18 | 42 | F | PVC and VT | 1 | PPM | Body | 14.37 | 0.46 |
| Patient 19 | 58 | M | PVC | 1 | PPM | Base | 17.08 | 0.15 |
| Patient 20 | 68 | M | PVC | 1 | PPM | Base | 15.09 | 0.27 |
| Patient 21 | 14 | M | PVC | 1 | PPM | Body | 10.44 | 0.52 |
| Patient 22 | 46 | M | PVC and VT | 1 | PPM | Body | 37.59 | 1.17 |
| Patient 23 | 56 | M | PVC | 1 | PPM | Body | 20.92 | 18.28 |
| Patient 24 | 45 | F | PVC and VT | 1 | PPM | Tip | 20.67 | 1.16 |
| Patient 25 | 53 | F | PVC | 1 | APM | Tip | 16.82 | 0.83 |
| Patient 26 | 69 | M | PVC | 1 | PPM | Body | 16.98 | 1.61 |
| Patient 27 | 66 | M | PVC | 1 | PPM | Tip | 15.24 | 1.10 |
| Patient 28 | 60 | M | PVC and VT | 1 | PPM | Body | 10.80 | 0.83 |
| Patient 29 | 71 | M | PVC | 1 | APM | Body | 11.37 | 1.51 |
| Patient 30 | 33 | F | PVC | 1 | APM | Tip | 12.37 | 10.32 |
| Patient 31 | 19 | M | PVC | 1 | PPM | Body | 13.10 | 2.43 |
| Patient 32 | 22 | M | PVC | 1 | PPM | Base | 14.29 | 1.67 |
| Patient 33 | 47 | F | PVC and VT | 1 | APM | Body | 12.47 | 1.86 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, T.; Chang, L.; Rong, B.; Zhang, K.; Fan, G.; Kong, J.; Ling, M.; Kong, Q.; Maduray, K.; Zhao, C.; et al. Combination of Intracardiac Echocardiography and Contact Force Sensing for Left Ventricular Papillary Muscle Arrhythmias. J. Clin. Med. 2023, 12, 3154. https://doi.org/10.3390/jcm12093154
Chen T, Chang L, Rong B, Zhang K, Fan G, Kong J, Ling M, Kong Q, Maduray K, Zhao C, et al. Combination of Intracardiac Echocardiography and Contact Force Sensing for Left Ventricular Papillary Muscle Arrhythmias. Journal of Clinical Medicine. 2023; 12(9):3154. https://doi.org/10.3390/jcm12093154
Chicago/Turabian StyleChen, Tongshuai, Lujie Chang, Bing Rong, Kai Zhang, Guanqi Fan, Jing Kong, Mingying Ling, Qingyu Kong, Kellina Maduray, Cuifen Zhao, and et al. 2023. "Combination of Intracardiac Echocardiography and Contact Force Sensing for Left Ventricular Papillary Muscle Arrhythmias" Journal of Clinical Medicine 12, no. 9: 3154. https://doi.org/10.3390/jcm12093154
APA StyleChen, T., Chang, L., Rong, B., Zhang, K., Fan, G., Kong, J., Ling, M., Kong, Q., Maduray, K., Zhao, C., & Zhong, J. (2023). Combination of Intracardiac Echocardiography and Contact Force Sensing for Left Ventricular Papillary Muscle Arrhythmias. Journal of Clinical Medicine, 12(9), 3154. https://doi.org/10.3390/jcm12093154