Abstract
Cleft lip and palate patients require complex interdisciplinary treatment, including maxillary expansion and secondary alveolar bone grafting. However, the evidence on these treatment procedures and outcomes is lacking. Therefore, this study aimed to survey the subjective observations of European maxillofacial surgeons and orthodontists on the maxillary expansion and bone grafting treatment protocols and the associated complications. An online questionnaire was sent to 131 centers. The questions assessed the participants’ demographic data, maxillary expansion and alveolar bone grafting protocols, and the associated complications. Descriptive statistics and a t-test were used to analyze the data. The response rate was 40.5%. The average age for maxillary expansion was 9–10 years. The secondary alveolar bone grafting was planned 5–10 months after the expansion. The most common complications were asymmetric expansion, relapse, and fistula formation. The protocols and materials used vary widely among centers. Anatomical alterations and developmental processes, like tooth eruption adjacent to the cleft, should be seriously considered for treatment planning. This survey showed that there is still a lack of consensus on these treatment procedures. Further clinical trials should focus on long-term outcome evaluation to identify treatment components for optimal alveolar bone substitution and transversal maxillary expansion treatment in patients with clefts.
1. Introduction
Cleft lip and/or palate (CL/P) is the most common craniofacial malformation resulting from incomplete fusion of the facial prominences. The prevalence of CL/P varies according to sex, ethnicity, and geographic origin [1]. Approximately one in 700 children in Europe is born with a CL/P [1]. The etiology of cleft lip and palate (CLP) is multifactorial. Both genetic and environmental risk factors contribute to etiopathogenesis, but the exact mechanisms are not clearly defined [2,3,4].
Moreover, patients with more severe CLP phenotypes and isolated cleft palates are more likely to have associated congenital malformations and syndromes [2]. They often present with developmental and congenital dental anomalies in tooth number (agenesis, supernumerary teeth), shape, and position, in addition to severe malocclusions affecting the primary and permanent dentition [5,6,7]. Therefore, CLP patients require an early and complex interdisciplinary approach.
The surgical interventions required for CLP repair lead to scar tissue formation, palatal muscle strain, and constriction of the maxillary complex [8,9]. Furthermore, intrinsic factors affecting palatal growth may also contribute to maxillary constriction [10], often resulting in canine impaction [11]. Moreover, the lower tongue position stimulates mandibular growth, leading to crossbite and Class III malocclusion [5].
Maxillary expansion and secondary alveolar bone grafting (SABG) are essential for managing transverse skeletal discrepancy and alveolar integrity. The maxillary expansion increases the palatal volume, allows normal growth and development, and provides more space for proper tongue posture [12].
The SABG is a well-established procedure in the treatment of CLP patients. It stabilizes and provides continuity of the maxillary complex, facilitates tooth eruption, permits orthodontic tooth movement, and enhances facial appearance [13]. Both autologous and allogenic bone can be used for this procedure [14].
In non-cleft patients, rapid maxillary expansion (RME) is a well-documented treatment approach for maxillary transverse deficiency [15,16]. Various complications of RME using tooth-borne expanders in non-cleft patients have been described [17]. The most common complications are buccal tilting of the anchor teeth, buccal bone fenestration, and root resorption. Recently published data suggested that bone-borne or hybrid tooth-bone-borne RME might benefit both non-affected [18] and affected patients [19]. Hence, increased sutural opening and reduced tooth tipping were observed compared with conventional tooth-borne RME, but the evidence remains limited [18]. In patients with CLP, the mid-palatal suture resistance is less or negligible compared with non-cleft individuals. As a result, lighter expansion forces are required [20]. Therefore, special expansion protocols should be considered for patients with affected craniofacial structures [21,22,23].
In patients with CLP, the timing of RME compared with the SABG is fundamental for the expansion prognosis and the alveolar bone volume preservation. Many authors favor transverse orthodontic expansion before bone grafting. Advantages such as improved access when repairing the nasal floor, better postoperative healing and hygiene, reduced anatomical resistance, and a decreased probability of reopening the oronasal fistula have been reported [24]. However, recent data show that maxillary expansion after SABG is, at some point, advantageous [24,25] due to the applied dynamic load and the narrower defect to repair [24,26]. Functional stimuli, such as tooth eruption, orthodontic tooth movement, and expansion, could increase the success rate of the bone graft [26]. Nevertheless, expansion after bone grafting compromises the healing process and increases the incidence of fistula formation [27]. A literature review by Wang et al. [28] reveals that no randomized clinical trials provide evidence of the outcome and stability of palatal expansion in relation to SABG.
Despite improving CLP care in Europe in the last two decades, there is a lack of evidence on RME timing and long-term treatment stability in patients with CLP [29]. This study was performed to give insight into the experience and subjective observations of the maxillofacial surgeons and orthodontists on the treatment protocols and outcomes of RME and SABG in patients with CLP in the European cleft centers.
2. Materials and Methods
2.1. Study Design
This study was approved by the Ethics Committee of the Charité–Universitätsmedizin Berlin (EA4/085/19). The authors conducted an online cross-sectional European survey in the English language. An online survey platform (Survio.com) was used.
The questionnaire (Appendix A) consisted of 38 questions, requiring approximately 6–10 min to complete. It mainly consisted of multiple-choice questions, and multiple responses were possible. The questions assessed the following aspects:
- Participants’ background expertise and the center’s general information
- Protocol of RME (timing related to SABG, types of appliances used, activation and retention protocol)
- Generalized, technical, and oral complications
All participants received an email invitation with information on the research and a link to the online survey. The first email invitation was sent on 29 March 2020. A monthly reminder was sent to increase participation until October 2020. The questionnaire was available for response until 3 December 2020. The survey was voluntary, and the data was collected and processed anonymously.
2.2. Study Population
The questionnaire included orthodontic and surgical aspects. Therefore, orthodontists and/or craniofacial surgeons in European CLP centers were the target population. As both specialists on the cleft team possess the knowledge necessary to complete the questionnaire, only one participant was contacted from each center. Nevertheless, in case of difficulties, participants were encouraged to forward their survey link to another team member who could complete the survey to their best knowledge.
The EUROCLEFT project book [30], in combination with an online search for publicly available updated addresses, was used as a guide to extract the centers and their email accounts. In total, 150 European CLP centers were found. The questionnaire was distributed to 131 European CLP centers. We could not find the email addresses of the remaining 19 centers; therefore, we excluded them from this study.
2.3. Statistical Analysis
The data was managed and stored using Microsoft Excel© 2023. Statistical analysis was performed using the statistical software Stata/SETM (version 11.1). The results were analyzed using descriptive and analytic statistics, including means, frequencies, and standard deviations. A t-test was used to check for possible associations between variables. The significance level was set at p < 0.05.
3. Results
3.1. Participants
In total, 54 questionnaires out of 131 were returned, corresponding to a response ratio of 40.5%. Most clinicians (70%) have at least ten years of treatment experience with CLP patients. In 44% of the centers, a caseload of fewer than 40 patients per year was reported. Only 19% of the participating centers have more than 80 CLP patients per year, and 37% have between 41 and 80 patients (Figure 1). Orthodontists comprised most participants (84%), and the remaining 16% were maxillofacial surgeons. More than half of the participants (68%) use RME to treat CLP patients.
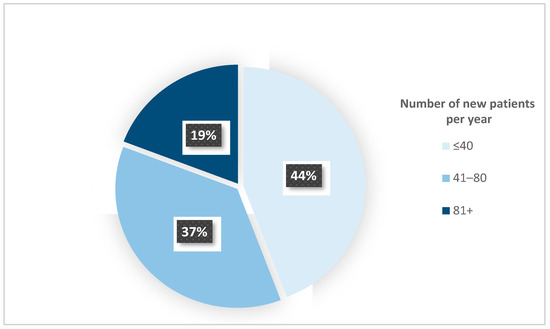
Figure 1.
The annual centers’ caseload of patients with CLP.
3.2. RME Protocol and Relation to the SABG
Factors affecting the timing of RME were mainly the patient’s age and the amount of expansion required. Some participants also considered other factors such as surgeries planned, cleft size, lateral incisor and/or canine root development, and the severity of the functional mandibular shift. In addition, ENT (Ear, Nose, Throat) problems, lack of space in the dental arch, logopedic indications, and patients’ cooperation were also considered (Figure 2).
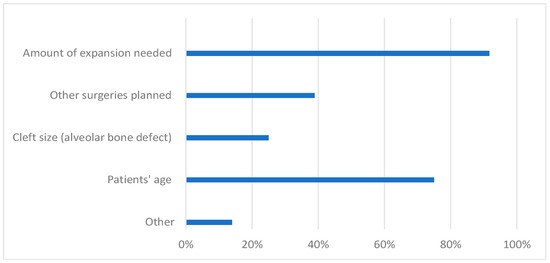
Figure 2.
Factors affecting the timing of RME treatment according to the clinicians (percentage of the participants).
The average age for performing RME was 9.4 ± 2.1 years in females and 9.9 ± 2.2 years in males. The youngest patients treated with RME were four years old, and the oldest were 20, both males and females. The average age for SABG was around 9.6 ± 1.8 years in females and 9.7 ± 1.8 years in males (Figure 3).
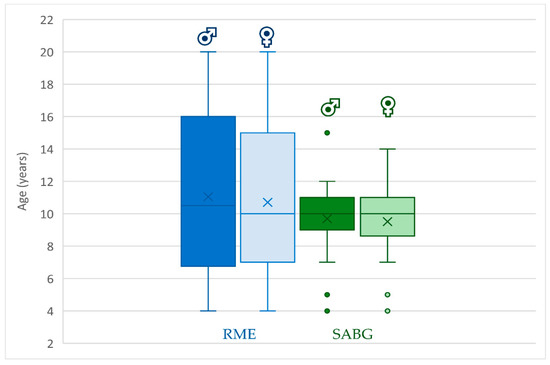
Figure 3.
Age span for RME and SABG for males and females (Dots placed past the line edges indicate outliers).
The iliac crest was the bone of choice for the SABG for 82% of the responders. Other sources of bone grafts, such as the mandibular symphyseal bone, tibia, and allogenic tissue-engineered bone, were used by less than 10% of the participants. Clinicians were asked about the timing of RME in relation to SABG and were allowed to give multiple answers. The majority of the clinicians (78%) perform RME before SABG, while 22% perform RME after SABG. Since this question allowed for multiple answers per participant, 25% of clinicians also indicated that their choice of timing was patient-dependent (Figure 4). An estimated time between SABG and RME treatment provided by the cleft team experts ranged between a minimum of 5.5 ± 3.6 months and a maximum of 15.3 ± 10 months. Most responders (84%) performed SABG before the canine eruption, and only 2% performed it independently of the canine eruption stage. Almost 18% of the participants plan SABG, depending on the developmental stage of the lateral incisor.
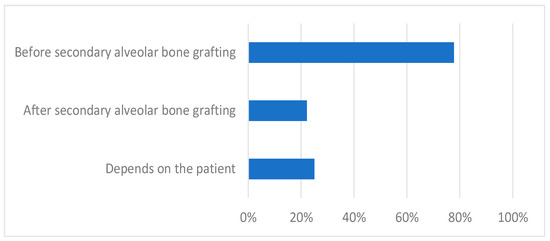
Figure 4.
Timing of RME in relation to SABG according to the clinicians (percentage of participants).
The average duration of the active RME phase was 1.8 ± 0.9 months; the shortest time was two weeks, and the most prolonged period was four months. For most participants (81%), the activation protocol was one to two turns daily.
3.3. RME Appliances and Retention Protocol
Tooth-borne expanders were used by 97% of the clinicians, and bone-tooth-borne hybrid expanders by 22%. Less than 20% of the responders used other devices, such as bone-borne and tooth-tissue-borne expanders. Most participants (77%) used the standard screw for the RME appliance. Fan expanders were used by 31%, and only a few participants used other screws like memory (5.7%) and super screws (5.7%).
For retention, most clinicians (83%) used the same RME appliance as in the active phase. Removable appliances, a quad-helix, or a transpalatal arch were used by 20% of the clinicians. The average retention period ranged from 8 ± 5.5 to 15 ± 9.5 months.
3.4. Treatment Complications
Several complications related to the appliance were reported. Loosening of the RME device was the most frequently reported technical complication, noticed in 1.6 ± 1.9 out of ten patients. Almost 1 ± 1.5 out of ten patients experienced complications such as screw blockage, appliance breakage, and confusion on how to activate the screw.
The most frequently reported general side effect in around 2 ± 2.3 patients out of ten was pain. On average, 1 ± 1.5 out of ten patients had headaches and dizziness. Less than one out of ten patients had other general complications such as metal allergies, a feeling of pressure or discomfort in the nose, difficulties in speaking, swallowing, and oral hygiene maintenance.
Relapse and instability were the most frequent intraoral complications. In around 2 ± 2.2 out of ten patients, cleft openings, fistulas, asymmetrical or limited skeletal expansion, and buccal tilting of anchor teeth were noticed. Furthermore, intraoral complications such as failure of maxillary suture opening, infection, decubitus on the tongue or the palatal mucosa, and tissue necrosis and/or hematomas were noticed in around one out of every ten patients. Other complications include buccal bone thickness and marginal bone level loss in the anchored teeth, elongation of non-anchor teeth, caries, root resorptions, severe gingivitis, and buccal dehiscence, which were observed in around one out of ten patients. Less frequently observed complications such as buccal fenestrations, gingival recession, tooth loss, discoloration, and devitalization of teeth were reported (Figure 5).
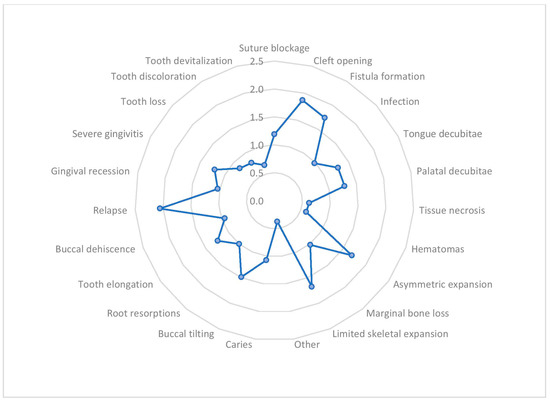
Figure 5.
The average frequency of intraoral complications of RME in out of ten patients.
The nasal widening was seen in 1.5 ± 2 patients out of ten and was the most reported extraoral complication. Swelling, reddening, exostosis on the nasal bridge, and epistaxis were less frequently observed (less than one out of ten patients).
In cases where the SABG was performed before RME, 24% of the clinicians noticed bone resorption in the SABG, 36% experienced no resorption, and 39% were unaware of it. Half of the participants reported up to 25% bone resorption when the SABG was performed before the RME. Most clinicians (70%) never observed resorption of more than 75% of the bone graft when SABG was performed before RME. The most common observed amount of bone resorption was 1–25% when SABG was performed after RME, according to 58% of the participants. Nevertheless, when SABG was performed after RME, resorption of more than 75% of the bone graft was observed in less than 26% of the patients, according to half of the responders (Table 1). Soft tissue scarring from previous surgeries was a limitation for RME, according to 43% of the clinicians, and 11% were unsure if there was any effect.

Table 1.
Comparison of the reported bone resorption (%) when SABG is performed before or after RME.
The correlation between clinicians’ years of experience and the complications of the RME was negative for most of the complications and statistically not significant (p > 0.05). The relapse of the RME and the retention period were not statistically correlated (r < 0.1). Similarly, no correlation (r = −0.2, p = 0.3) was found between the clinicians’ experience and the amount of SABG resorption. The correlation between the average time between RME and SABG and the amount of SABG resorption was not significant (p = 0.4). There was a weak but statistically significant correlation between the amount of bone resorption and the relapse rate (r = 0.5, p = 0.02).
Most centers (89%) keep records of their patients treated with RME. More than 80% of the participants used dental models and photographs for patient documentation. Most clinicians (69%) used radiographs as part of their protocol. Some participants indicated using computed tomography (23%) and occlusal bite registration (34%). Only 6% used periodontal probing as part of their patient records.
4. Discussion
The interaction of different disciplines on a national or international level is demanded in managing patients with craniofacial anomalies [5,6]. Meticulous patient documentation, well-planned longitudinal studies, sharing clinical experience, and patient values integration would provide the best scientific evidence for treating patients with CLP. Healthcare models should focus on prevention, identifying risk factors, and population groups for integrated and long-term personalized care [2,3,4,31]. Furthermore, patients with CLP have broad phenotypic variability and different degrees of severity. In many instances, late identification or late expression of some phenotypes makes a precise diagnosis of an associated malformation or syndrome challenging [2,31].
Patients with CLP are more likely to have a missing midpalatal suture [32]; in addition, early surgical interventions can disrupt the intrinsic growth potential, resulting in maxillary hypoplasia [33]. Procedures like RME and SABG are necessary for CLP patients as they bear aesthetic and functional advantages.
There is no consensus on the treatment protocols for patients with CLP among the European centers [34]. Moreover, the lack of data on the RME protocol in relation to the SABG and the associated complications [28] led us to this survey. Experienced clinicians from the European cleft centers gave their insight on this topic.
RME was performed before SABG in most of the centers (78%). The mean age of maxillary expansion has been reported at 9.4 ± 2.1 and 9.9 ± 2.2 years for females and males, respectively. The amount of maxillary expansion and the patients’ age were the most critical factors for the timing of the maxillary expansion. Besides these factors, other planned surgeries, such as the cleft size, canine eruption, crossbite, and forced bite guidance, were also substantially considered. Performing RME in adults is controversial, but it has to be evaluated if this also applies to patients with CLP [35,36].
According to this survey, the SABG was planned around 9–10 years ago, before the canine eruption. The recommended timing for SABG is between 9 and 11 years [37]. The stage of development of the canine or lateral incisor on the cleft side should also be taken into consideration instead of the patient’s age [38,39]. SABG is often performed just before the canine eruption, but if the lateral incisor is present and erupting on the cleft side, SABG can be performed earlier [38,39]. Only three participants performed SABG around age five for quick normalized dental arch forms and periodontal support of the teeth adjacent to the cleft. An Early SABG procedure performed before or during the eruption of the lateral incisor could benefit the patient, but more studies are needed to explore this approach [40].
The SABG, after maxillary expansion, can stabilize the expanded maxilla and prevent relapse [8,41,42,43], which agrees with most of the responders to this survey. SABG can stabilize the expanded alveolar segments and allow the spontaneous eruption of these teeth in the grafted area [44]. However, relapse has also been described when using this protocol [45]. On the other hand, more recent literature describes the benefits of SABG before RME [15,46,47,48], claiming that this practice supports the mid-palatal suture opening and can provide more stability for RME. However, the results can be unpredictable [25]. In our study, only 22.2% of the clinicians performed SABG before RME.
There are different approaches when considering the period between the two procedures. Around 6–12 weeks after SABG, expansion can be initiated [43,49]. Others recommend waiting for at least three months after grafting [25]. Further research is needed to investigate the appropriate timing for RME after SABG [46]. The average period between SABG and RME was 5.5–15.3 months. The duration of this period was not statistically correlated with the amount of SABG resorption.
Maxillary alveolar reconstruction in patients with unilateral CLP was similarly effective using allogenic or autologous bone grafts [14]. Allogenic bone grafting using 3D plotting enhanced with osteogenic cells is a promising approach that requires further investigation [50]. Autologous bone grafts, both cortical or cancellous bones, can be used. Cancellous grafts incorporate faster than cortical bone, enabling tooth eruption [51]. Most of our participants used cancellous bone from the iliac crest, and 34% used the cortical bone. Other sources of bone grafts, such as the mandibular symphyseal bone, tibia, and allogenic tissue-engineered bone, were used by less than 10% of the participants. If a sizeable alveolar cleft is present, it can be reconstructed using bone from the iliac crest. In cases of smaller defects, bone substitutes from the chin can be used, as only a small amount can be collected [38]. The advantages of using mandibular bone are a shorter operative time and hospital stay, and no extraoral scar formation [52].
A review by Barillas et al. [53] stated that maxillary expansion after the SABG does not cause significant loss in bone volume or density. However, those authors [53] recommended caution with the reported results and suggested further experimental studies to evaluate the success of SABG in relation to RME. Some clinicians (24%) noticed bone resorption in the SABG independent of the timing of RME. It was reported that significant bone loss occurs between 3 and 12 months after grafting [46]. Placing the SABG under physiologic stress can help preserve the bone [13,54]. The most common amount of experienced bone resorption after/before RME was between 1 and 25%. In contrast, other researchers noticed that the average bone loss was 49.5% during the first year after surgery [55] but remained almost constant the following two years [55]. In some studies, the mean bone graft volume loss was around 36% [13,56].
Using tooth-borne expanders such as the Hyrax has the advantage of working on the short clinical crowns of the primary dentition and increasing twisting rigidity [57]. Our results showed that 97% of clinicians use tooth-borne expanders, which coincides with a recent European survey [29].
Researchers agree that the latest treatment time for RME is during puberty for non-cleft orthodontic patients [15,28,46,58]. In this survey, the oldest age indicated by the participants was 20 years of age, and the youngest was four years. A Belgian research group recommends correcting severe transverse maxillary constriction at a relatively young age through combined maxillary osteotomy and orthodontic expansion, due to the absence of a healthy midpalatal suture [59]. As a result, the need for a three-piece osteotomy at an adult age is reduced [59].
When considering the retention protocols, most clinicians follow the 8–15-month retention phase. Few clinicians had a one-month only and the most 24 months retention period reported. In contrast, published data shows that most clinicians follow a protocol with a three-month retention phase [17]. However, the six-month retention phase is also prevalent. Our results suggested no significant correlation between the retention period and the relapse of RME, implying that it is case-specific. Palatal strain, scar tissue, and hard and soft tissue deficiencies in that area contribute to deterioration and instability, making it more complex compared with non-cleft patients.
The treatment complications in our questionnaire were divided into technical, general, intra- and extra-oral. The most common technical difficulty reported in the literature [17] was the loosening of the appliance, which corresponds with our results. Moving to the general complications, pain was the most common one. As other researchers have reported, the pain was mainly noticed in the molar region and was greater in patients who received the activation twice daily [60]. RME with an up-to-two-times-daily activation protocol was employed by most European centers [29]. Our results showed that most clinicians used one to two activations daily, and only two clinicians used them three to four times-a-day. Pain was the most common complication.
Although most clinicians had more than ten years of experience, the most common intraoral complications prevailed. Relapse and instability were the most common intra-oral complications, in addition to fistula formation and asymmetric expansion. A statistically significant correlation was found between the amount of bone resorption and the relapse and instability rates (r = 0.5, p = 0.02). Buccal tilting up to 24° of the first molars is due to the teeth tilting and the deformation of the alveolar processes [61]. Figueiredo et al. concluded that buccal tiling was similar on both cleft and non-cleft sides, and symmetric expansion was achieved, but more effectively in the molar area [62]. Widening of the nose was the most common extraoral complication, according to our participants. Since nose growth takes a long time, the changes are discreet [17]. However, recent literature reveals that nasal and alar base widths increased significantly after expansion [63,64]. A nasal widening of around 2 mm was seen in a study [65] evaluated through photometric analysis. Epistaxis is a less common complication, mainly occurring after surgically assisted palatal expansion [66].
Almost all clinicians keep records of the CLP patients treated with RME, such as dental models and photographs. Computed tomography was used by 23%, similar to the results reported in recent literature [34,63]. Considering that CLP is a 3D facial deformity, using cone beam computed tomography helps achieve better care for those patients [67].
The sex distribution and phenotyping of the CLP patients were not clearly differentiated in this survey. Moreover, some associated malformations, whether isolated or as part of an underlined syndrome, are not diagnosed before the 4th or 5th year of age because of phenotypic variability or mild expression [68]. Some syndromes may be identified later in life because they are associated with learning difficulties or psychiatric symptoms, such as the 22q11DS syndrome [69]. Therefore, it would be hard for the participants to make a strict differentiation between syndromic and non-syndromic CLP individuals.
This survey might not represent all European centers, but almost half of the contacted centers (n = 54), providing a response rate of 40.5%, shared their long-standing experience in the field. Most of the responders had clinical experience of more than ten years, and 37% had more than 20 years of experience treating CLP patients, which adds to the strength of these findings. In addition, most of the responses correlated with the evidence-based literature. The CLP centers (n = 77) that did not respond to our questionnaire can be related to the tight schedules of clinicians [70]. Due to the anonymous data collection in this study, it is hard to rule out response bias. In the literature, there is no agreed-upon standard for acceptable response rates. However, low response rates increase the probability of response bias [71,72]. Our response rate of 40.5% is comparable to similar surveys in this field [30,34]. More studies are required globally to provide adequate evidence for treating these patients [73].
Further research, surveys, and randomized clinical trials should focus on the preferred bone for dentoalveolar reconstruction and the timing of RME in relation to SABG for the best bone volume preservation in treating patients with CLP.
5. Conclusions
The largest part of the responders used the following protocol:
- The average age for performing RME was 9–10 years. Taking into consideration the amount of expansion and the planned SABG.
- The SABG was planned 5–10 months after the RME.
- The canine root maturation stage and, in some cases, the lateral incisor developmental stage define the SABG timing.
- The retention period of RME was approximately 8–15 months after the last activation using the same orthodontic device.
Most participants have long-standing experience and a substantial caseload per year, which adds to the strength of these findings. Nevertheless, a lack of consensus exists on RME and SABG protocols, timing, and stability used for CLP treatment.
Author Contributions
Conceptualization, T.B.; methodology, T.B., N.K. and T.H.; software, T.H. and N.K.; validation T.B., T.H., N.K. and M.K.; formal analysis, N.K., T.H. and M.K.; investigation, N.K., T.H., M.K. and T.B; data curation, T.H. and N.K.; writing—original draft preparation, T.H. and N.K.; writing—review and editing, T.B. and N.K.; visualization, N.K.; supervision, and project administration, T.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This survey was approved by the Ethics Committee of the Charité–Universitätsmedizin Berlin (EA4/085/19).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We acknowledge financial support from the Open Access Publication Fund of Charité–Universitätsmedizin Berlin and the German Research Foundation (DFG). The authors would like to thank all the participants who responded to the survey.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
A survey on complications of rapid maxillary expansion in cleft lip and palate patients in the European cleft centers.
Table A1.
A survey on complications of rapid maxillary expansion in cleft lip and palate patients in the European cleft centers.
|
|
|
|
|
|
|
|
|
|
|
|
| Average age for boys………………….. Average age for girls………………….. |
| Age span for boys; minimum at…..maximum at……. Age span for girls; minimum at…..maximum at……. |
| Average age for boys………………….. Average age for girls………………….. |
|
|
|
|
| Minimum……………….. Maximum………………. |
|
|
| …………………………. |
|
|
|
|
|
|
|
|
| Minimum ……………………….. Maximum ……………………….. |
|
|
| ……….. |
|
|
| ………….. |
|
|
| ……….. |
|
|
| …………….. |
|
|
|
|
|
|
|
|
|
|
(75–100% of bone resorption with no continuous bony bridge through the cleft)? |
|
|
|
|
|
|
|
|
|
| …………….. |
References
- Mossey, P.A.; Modell, B. Epidemiology of oral clefts 2012: An international perspective. Cleft Lip Palate 2012, 16, 1–18. [Google Scholar]
- Jamilian, A.; Sarkarat, F.; Jafari, M.; Neshandar, M.; Amini, E.; Khosravi, S.; Ghassemi, A. Family history and risk factors for cleft lip and palate patients and their associated anomalies. Stomatologija 2017, 19, 78–83. [Google Scholar] [PubMed]
- Maili, L.; Letra, A.; Silva, R.; Buchanan, E.P.; Mulliken, J.B.; Greives, M.R.; Teichgraeber, J.F.; Blackwell, S.J.; Ummer, R.; Weber, R. PBX-WNT-P63-IRF6 pathway in nonsyndromic cleft lip and palate. Birth Defects Res. 2020, 112, 234–244. [Google Scholar] [CrossRef]
- Bartzela, T.N. Treatment Outcome in Patients with Bilateral Cleft Lip and Palate. An Intercentre Study on Dentofacial Morphology until 12 Years of Age; Radboud University Nijmegen Medical Centre: Nijmegen, The Netherlands, 2011. [Google Scholar]
- Bartzela, T.N.; Carels, C.E.; Bronkhorst, E.M.; Kuijpers-Jagtman, A.M. Tooth agenesis patterns in unilateral cleft lip and palate in humans. Arch. Oral Biol. 2013, 58, 596–602. [Google Scholar] [CrossRef]
- Bartzela, T.N. Treatment approaches to syndromes affecting craniofacial and dental structures. J. World Fed. Orthod. 2019, 8, 131–137. [Google Scholar] [CrossRef]
- Bartzela, T.N.; Carels, C.E.; Bronkhorst, E.M.; Rønning, E.; Rizell, S.; Kuijpers-Jagtman, A.M. Tooth agenesis patterns in bilateral cleft lip and palate. Eur. J. Oral Sci. 2010, 118, 47–52. [Google Scholar] [CrossRef]
- Filho, L.C.; De Almeida, A.; Ursi, W. Rapid maxillary expansion in cleft lip and palate patients. J. Clin. Orthod. JCO 1994, 28, 34–39. [Google Scholar]
- Townend, P.I. Technique of rapid expansion in patients with cleft lip and palate. Br. J. Orthod. 1980, 7, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Šmahel, Z.; Velemínská, J.; Trefný, P.; Müllerová, Ž. Three-dimensional morphology of the palate in patients with bilateral complete cleft lip and palate at the stage of permanent dentition. Cleft Palate-Craniofacial J. 2009, 46, 399–408. [Google Scholar] [CrossRef]
- Bizzarro, M.; Generali, C.; Maietta, S.; Martorelli, M.; Ferrillo, M.; Flores-Mir, C.; Perillo, L. Association between 3D palatal morphology and upper arch dimensions in buccally displaced maxillary canines early in mixed dentition. Eur. J. Orthod. 2018, 40, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Generali, C.; Primozic, J.; Richmond, S.; Bizzarro, M.; Flores-Mir, C.; Ovsenik, M.; Perillo, L. Three-dimensional evaluation of the maxillary arch and palate in unilateral cleft lip and palate subjects using digital dental casts. Eur. J. Orthod. 2017, 39, 641–645. [Google Scholar] [CrossRef]
- Zhang, W.; Shen, G.; Wang, X.; Yu, H.; Fan, L. Evaluation of alveolar bone grafting using limited cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Scalzone, A.; Flores-Mir, C.; Carozza, D.; d’Apuzzo, F.; Grassia, V.; Perillo, L. Secondary alveolar bone grafting using autologous versus alloplastic material in the treatment of cleft lip and palate patients: Systematic review and meta-analysis. Prog. Orthod. 2019, 20, 6. [Google Scholar] [CrossRef]
- Garib, D.G.; Henriques, J.F.C.; Janson, G.; Freitas, M.R.; Coelho, R.A. Rapid maxillary expansion—Tooth tissue-borne versus tooth-borne expanders: A computed tomography evaluation of dentoskeletal effects. Angle Orthod. 2005, 75, 548–557. [Google Scholar] [PubMed]
- da Silva Filho, O.G.; do Prado Montes, L.A.; Torelly, L.F. Rapid maxillary expansion in the deciduous and mixed dentition evaluated through posteroanterior cephalometric analysis. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 268–275. [Google Scholar] [CrossRef]
- Schuster, G.; Borel-Scherf, I.; Schopf, P.M. Frequency of and complications in the use of RPE appliances—Results of a survey in the Federal State of Hesse, Germany. J. Orofac. Orthop. 2005, 66, 148–161. [Google Scholar] [CrossRef] [PubMed]
- Krüsi, M.; Eliades, T.; Papageorgiou, S.N. Are there benefits from using bone-borne maxillary expansion instead of tooth-borne maxillary expansion? A systematic review with meta-analysis. Prog. Orthod. 2019, 20, 9. [Google Scholar] [CrossRef]
- Meng, W.-Y.; Ma, Y.-Q.; Shi, B.; Liu, R.-K.; Wang, X.-M. The comparison of biomechanical effects of the conventional and bone-borne palatal expanders on late adolescence with unilateral cleft palate: A 3-dimensional finite element analysis. BMC Oral. Health 2022, 22, 600. [Google Scholar] [CrossRef]
- Jain, D.; Shrivastav, S.; Jain, N.K. Maxillary expansion in cleft lip and palate cases—A review. Int. J. 2015, 3, 1455–1461. [Google Scholar]
- Pan, X.; Qian, Y.; Yu, J.; Wang, D.; Tang, Y.; Shen, G. Biomechanical effects of rapid palatal expansion on the craniofacial skeleton with cleft palate: A three-dimensional finite element analysis. Cleft Palate-Craniofacial J. 2007, 44, 149–154. [Google Scholar] [CrossRef]
- Figueiredo, D.S.F.; Bartolomeo, F.U.C.; Romualdo, C.R.; Palomo, J.M.; Horta, M.C.R.; Andrade, I.J.; Oliveira, D.D. Dentoskeletal effects of 3 maxillary expanders in patients with clefts: A cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 73–81. [Google Scholar] [CrossRef]
- Luyten, J.; De Roo, N.M.; Christiaens, J.; Van Overberghe, L.; Temmerman, L.; De Pauw, G.A. Rapid maxillary expansion vs slow maxillary expansion in patients with cleft lip and/or palate: A systematic review and meta-analysis. Angle Orthod. 2023, 93, 95–103. [Google Scholar] [CrossRef]
- Seifeldin, S.A. Is alveolar cleft reconstruction still controversial? (review of literature). Saudi Dent. J. 2016, 28, 3–11. [Google Scholar] [CrossRef]
- da Silva Filho, O.G.; Boiani, E.; de Oliveira Cavassan, A.; Santamaria, M.J. Rapid maxillary expansion after secondary alveolar bone grafting in patients with alveolar cleft. Cleft Palate-Craniofacial J. 2009, 46, 331–338. [Google Scholar] [CrossRef]
- Bergland, O.; Semb, G.; Abyholm, F.E. Elimination of the residual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment. Cleft Palate J. 1986, 23, 175–205. [Google Scholar] [PubMed]
- Luque-Martín, E.; Tobella-Camps, M.L.; Rivera-Baró, A. Alveolar graft in the cleft lip and palate patient: Review of 104 cases. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e531. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Chou, J. Maxillary expansion and timing of secondary alveolar bone grafting: A review of the current literature. J. Oral Maxillofac. Surg. 2014, 72, e14–e15. [Google Scholar] [CrossRef]
- Francisco, I.; Antonarakis, G.S.; Caramelo, F.; Fernandes, M.H.; Vale, F. Cleft orthodontic care in Europe: A cross-sectional survey. Healthcare 2022, 10, 1555. [Google Scholar] [CrossRef]
- Shaw, B. The Eurocleft Project 1996–2000; Ios Press: Amsterdam, The Netherlands, 2000; Volume 43. [Google Scholar]
- Bartzela, T.N.; Carels, C.; Maltha, J.C. Update on 13 syndromes affecting craniofacial and dental structures. Front. Physiol. 2017, 8, 1038. [Google Scholar] [CrossRef] [PubMed]
- Zapatero, Z.D.; Carlson, A.R.; Kosyk, M.S.; Kalmar, C.L.; Swanson, J.W.; Bartlett, S.P.; Vossough, A.; Taylor, J.A. What is the role of midfacial sutures in the development of maxillary hypoplasia in children with cleft palate? J. Craniofacial Surg. 2022, 33, 827–829. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Johnson, C.A.; Smith, A.A.; Salmon, B.; Shi, B.; Brunski, J.; Helms, J.A. Disrupting the intrinsic growth potential of a suture contributes to midfacial hypoplasia. Bone 2015, 81, 186–195. [Google Scholar] [CrossRef]
- Francisco, I.; Antonarakis, G.S.; Caramelo, F.; Paula, A.B.; Marto, C.M.; Carrilho, E.; Fernandes, M.H.; Vale, F. Current treatment of cleft patients in Europe from a provider perspective: A cross-sectional survey. Int. J. Environ. Res. Public Health 2022, 19, 10638. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.J. The role of the transverse dimension in orthodontic diagnosis and treatment, In McNamara JA Jr, ed. Growth modification: What works, what doesn’t and why? Monograph 36, Craniofacial growth series. Cent. Hum. Growth Dev. Ann Arbor Univ. Mich. 1999, 35, 153–192. [Google Scholar]
- Proffit, W.R.; Fields, H.W.J.; Sarver, D.M. Contemporary Orthodontics; Elsevier Health Sciences: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Boyne, P.J. Secondary bone grafting of residual alveolar and palatal clefts. J. Oral Surg. 1972, 30, 87–92. [Google Scholar]
- van der Molen, A.B.M.; van Breugel, J.M.; Janssen, N.G.; Admiraal, R.J.; van Adrichem, L.N.; Bierenbroodspot, F.; Bittermann, D.; van den Boogaard, M.-J.H.; Broos, P.H.; Dijkstra-Putkamer, J.J. Clinical practice guidelines on the treatment of patients with cleft lip, alveolus, and palate: An executive summary. J. Clin. Med. 2021, 10, 4813. [Google Scholar] [CrossRef] [PubMed]
- De Mulder, D.; Cadenas de Llano-Pérula, M.; Jacobs, R.; Verdonck, A.; Willems, G. Three-dimensional radiological evaluation of secondary alveolar bone grafting in cleft lip and palate patients: A systematic review. Dentomaxillofacial Radiol. 2019, 48, 20180047. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, F.H.d.S.L.; Drummond, R.J.; Frota, C.M.; Bartzela, T.N.; Dos Santos, P.B. Comparison of early and conventional autogenous secondary alveolar bone graft in children with cleft lip and palate: A systematic review. Orthod. Craniofacial Res. 2020, 23, 385–397. [Google Scholar] [CrossRef]
- Robertson, N.; Fish, J. Some observations on rapid expansion followed by bone grafting in cleft lip and palate. Cleft Palate J. 1972, 9, 236–245. [Google Scholar]
- Isaacson, R.J.; Murphy, T.D. Some efifects of rapid maxillary expansion in cleft lip and palate patients. Angle Orthod. 1964, 34, 143–154. [Google Scholar]
- Uzel, A.; Benlidayı, M.E.; Kürkçü, M.; Kesiktaş, E. The effects of maxillary expansion on late alveolar bone grafting in patients with unilateral cleft lip and palate. J. Oral Maxillofac. Surg. 2019, 77, 607–614. [Google Scholar] [CrossRef]
- Bartzela, T.N.; Mang de la Rosa, M.R.; Wolf, K.; Schmidt, A.; Opitz, C. Apical root resorption after orthodontic treatment in patients with unilateral cleft lip and palate. Clin. Oral Investig. 2020, 24, 1807–1819. [Google Scholar] [CrossRef]
- Nicholson, P.; Plint, D. A long-term study of rapid maxillary expansion and bone grafting in cleft lip and palate patients. Eur. J. Orthod. 1989, 11, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-J.; Pan, X.-G.; Qian, Y.-F.; Wang, G.-M. Impact of rapid maxillary expansion in unilateral cleft lip and palate patients after secondary alveolar bone grafting: Review and case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, e25–e30. [Google Scholar] [CrossRef]
- Garib, D.; Miranda, F.; Sathler, R.; Kuijpers-Jagtman, A.M.; Aiello, C.A. Rapid maxillary expansion after alveolar bone grafting with rhBMP-2 in UCLP evaluated by means of CBCT. Cleft Palate-Craniofacial J. 2017, 54, 474–480. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Cavassan, A.; de Albuquerque, M.D.A.; Capelozza Filho, L. Rapid maxillary expansion after secondary alveolar bone graft in a patient with bilateral cleft lip and palate. Cleft Palate-Craniofacial J. 2004, 41, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Precious, D.S. A new reliable method for alveolar bone grafting at about 6 years of age. J. Oral Maxillofac. Surg. 2009, 67, 2045–2053. [Google Scholar] [CrossRef]
- Korn, P.; Ahlfeld, T.; Lahmeyer, F.; Kilian, D.; Sembdner, P.; Stelzer, R.; Pradel, W.; Franke, A.; Rauner, M.; Range, U. 3D printing of bone grafts for cleft alveolar osteoplasty–in vivo evaluation in a preclinical model. Front. Bioeng. Biotechnol. 2020, 8, 217. [Google Scholar] [CrossRef]
- Coots, B.K. Alveolar bone grafting: Past, present, and new horizons. Semin. Plast. Surg. 2012, 26, 178–183. [Google Scholar] [CrossRef]
- Nwoku, A.L.; Al Atel, A.; Al Shlash, S.; Oluyadi, B.A.; Ismail, S. Retrospective analysis of secondary alveolar cleft grafts using iliac of chin bone. J. Craniofacial Surg. 2005, 16, 864–868. [Google Scholar] [CrossRef]
- Barillas, A.P.; Michelogiannakis, D.; Rossouw, P.E.; Javed, F. Maxillary expansion in grafted alveolar arches in patients with cleft lip and palate: A literature review. Surg. Pract. Sci. 2021, 5, 100034. [Google Scholar] [CrossRef]
- Dempf, R.; Teltzrow, T.; Kramer, F.-J.; Hausamen, J.-E. Alveolar bone grafting in patients with complete clefts: A comparative study between secondary and tertiary bone grafting. Cleft Palate-Craniofacial J. 2002, 39, 18–25. [Google Scholar] [CrossRef]
- Feichtinger, M.; Mossböck, R.; Kärcher, H. Assessment of bone resorption after secondary alveolar bone grafting using three-dimensional computed tomography: A three-year study. Cleft Palate-Craniofacial J. 2007, 44, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Datana, S.; Chattopadhyay, P.; Kadu, A. Bony bridge resorption after secondary alveolar grafting and correlation with success of orthodontic treatment: A prospective volumetric cone beam computed tomography (CBCT) study. Med. J. Armed Forces India 2019, 75, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Bottrel, J.A.; Lee, K.-G.; Lunazzi, J.J.; Legan, H.L. The biomechanics of rapid maxillary sutural expansion. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Baccetti, T.; Franchi, L.; Cameron, C.G.; McNamara, J.A.J. Treatment timing for rapid maxillary expansion. Angle Orthod. 2001, 71, 343–350. [Google Scholar]
- Carpentier, S.; Van Gastel, J.; Schoenaers, J.; Carels, C.; Poorten, V.V.; Coucke, W.; Verdonck, A. Evaluation of transverse maxillary expansion after a segmental posterior subapical maxillary osteotomy in cleft lip and palate patients with severe collapse of the lateral maxillary segments. Cleft Palate-Craniofacial J. 2014, 51, 651–657. [Google Scholar] [CrossRef]
- Baruah, D.; Nagesh, S.; Sarma, H.; Mattu, N. Comparative assessment of anxiety, pain, and discomfort during rapid maxillary expansion using two different activation protocols in patients with cleft lip and palate. Cleft Palate-Craniofacial J. 2022, 59, 1010–1016. [Google Scholar] [CrossRef]
- Hicks, E.P. Slow maxillary expansion. A clinical study of the skeletal versus dental response to low-magnitude force. Am. J. Orthod. 1978, 73, 121–141. [Google Scholar] [CrossRef]
- Figueiredo, D.S.F.; Cardinal, L.; Bartolomeo, F.U.C.; Palomo, J.M.; Horta, M.C.R.; Andrade, I.J.; Oliveira, D.D. Effects of rapid maxillary expansion in cleft patients resulting from the use of two different expanders. Dent. Press J. Orthod. 2016, 21, 82–90. [Google Scholar] [CrossRef]
- Huang, J.; Li, C.-Y.; Jiang, J.-H. Facial soft tissue changes after nonsurgical rapid maxillary expansion: A systematic review and meta-analysis. Head Face Med. 2018, 14, 6. [Google Scholar] [CrossRef]
- An, J.-S.; Seo, B.-Y.; Ahn, S.-J. Differences in dentoskeletal and soft tissue changes due to rapid maxillary expansion using a tooth-borne expander between adolescents and adults: A retrospective observational study. Korean J. Orthod. 2022, 52, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.L.; Pangrazio-Kulbersh, V.; Thomas, B.W.; Kaczynski, R. Photographic analysis of facial changes associated with maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Psillas, G.; Dimas, G.G.; Papaioannou, D.; Savopoulos, C.; Constantinidis, J. Epistaxis in dental and maxillofacial practice: A comprehensive review. J. Korean Assoc. Oral Maxillofac. Surg. 2022, 48, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Parveen, S.; Husain, A.; Mascarenhas, R.; Reddy, S.G. Clinical utility of cone-beam computed tomography in patients with cleft lip palate: Current perspectives and guidelines. J. Cleft Lip Palate Craniofacial Anom. 2018, 5, 74. [Google Scholar] [CrossRef]
- Bartzela, T. Early clinical investigations and management of syndromes affecting craniofacial and dental structures. In Fundamentals of Craniofacial Malformations: Vol. 1, Disease and Diagnostics; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 271–297. [Google Scholar]
- Bassett, A.S.; McDonald-McGinn, D.M.; Devriendt, K.; Digilio, M.C.; Goldenberg, P.; Habel, A.; Marino, B.; Oskarsdottir, S.; Philip, N.; Sullivan, K. Practical guidelines for managing patients with 22q11. 2 deletion syndrome. J. Pediatr. 2011, 159, 332.e331–339.e331. [Google Scholar] [CrossRef]
- VanGeest, J.B.; Johnson, T.P.; Welch, V.L. Methodologies for improving response rates in surveys of physicians: A systematic review. Eval. Health Prof. 2007, 30, 303–321. [Google Scholar] [CrossRef]
- Höfler, M.; Pfister, H.; Lieb, R.; Wittchen, H.U. The use of weights to account for non-response and drop-out. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 291–299. [Google Scholar] [CrossRef]
- Harrison, D.L.; Draugalis, J.R. Evaluating the results of mail survey research. J. Am. Pharm. Assoc. 1996 1997, 37, 662–666. [Google Scholar] [CrossRef]
- Srivastav, S.; Tewari, N.; Goel, S.; Duggal, R.; Antonarakis, G.S.; Haldar, P. Global trends in knowledge, attitude, and awareness of orthodontists regarding the management of patients with cleft lip and/or palate: A systematic review. Cleft Palate-Craniofacial J. 2022. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).