
Quantitative Assessment of Upper Limb Movement in Post-Stroke Adults for Identification of Sensitive Measures in Reaching and Lifting Activities

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
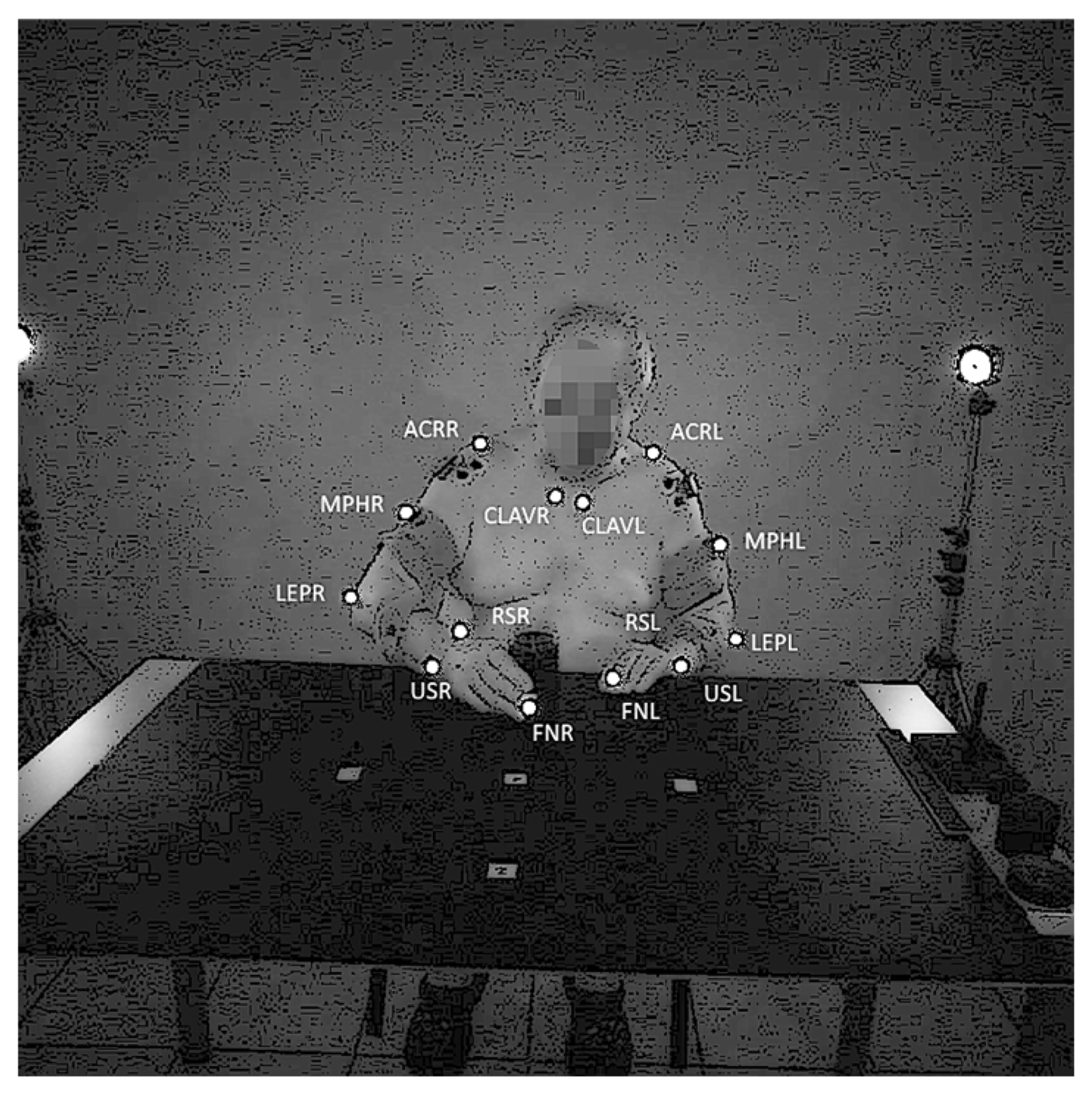
Study Protocol
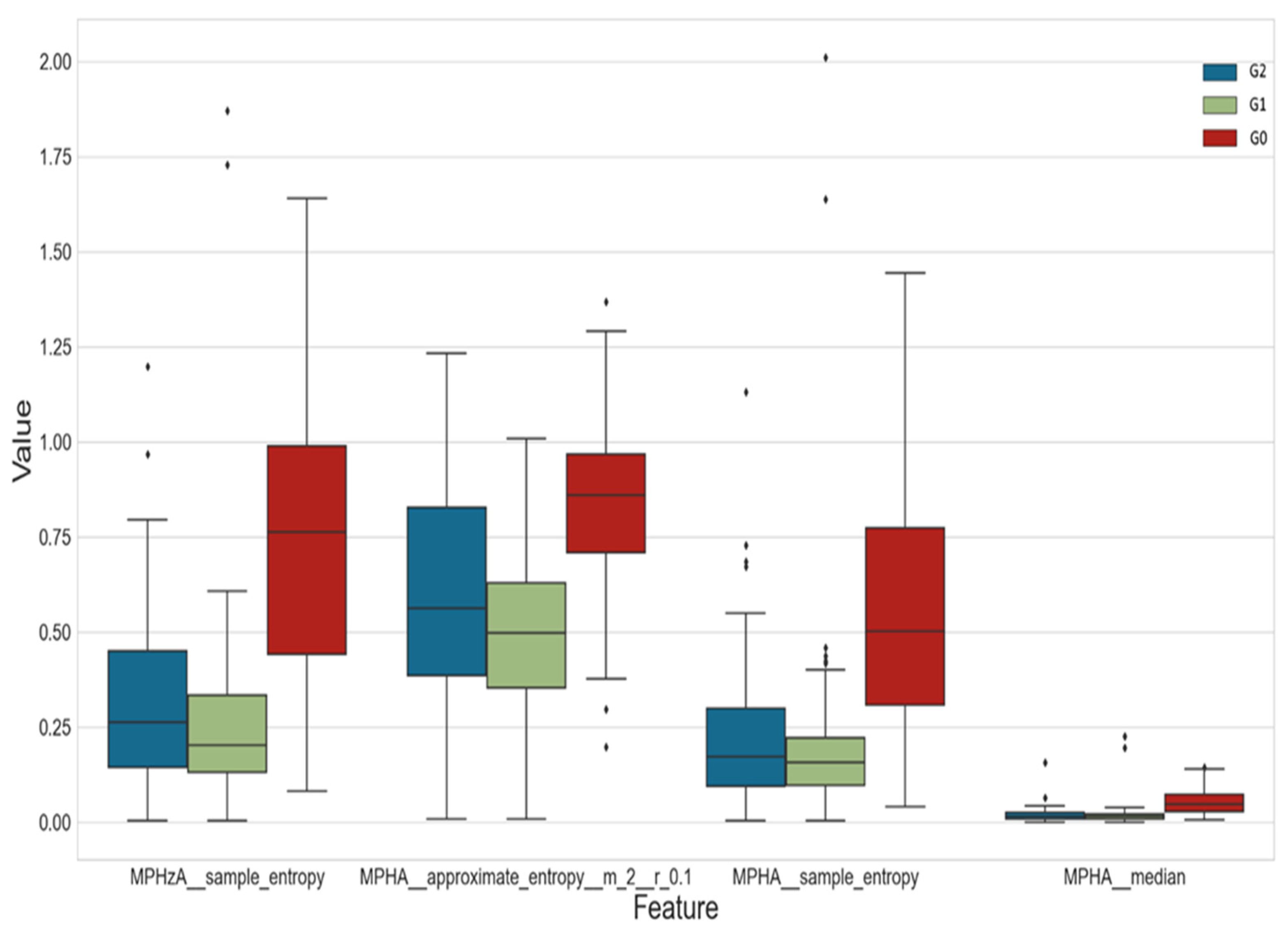
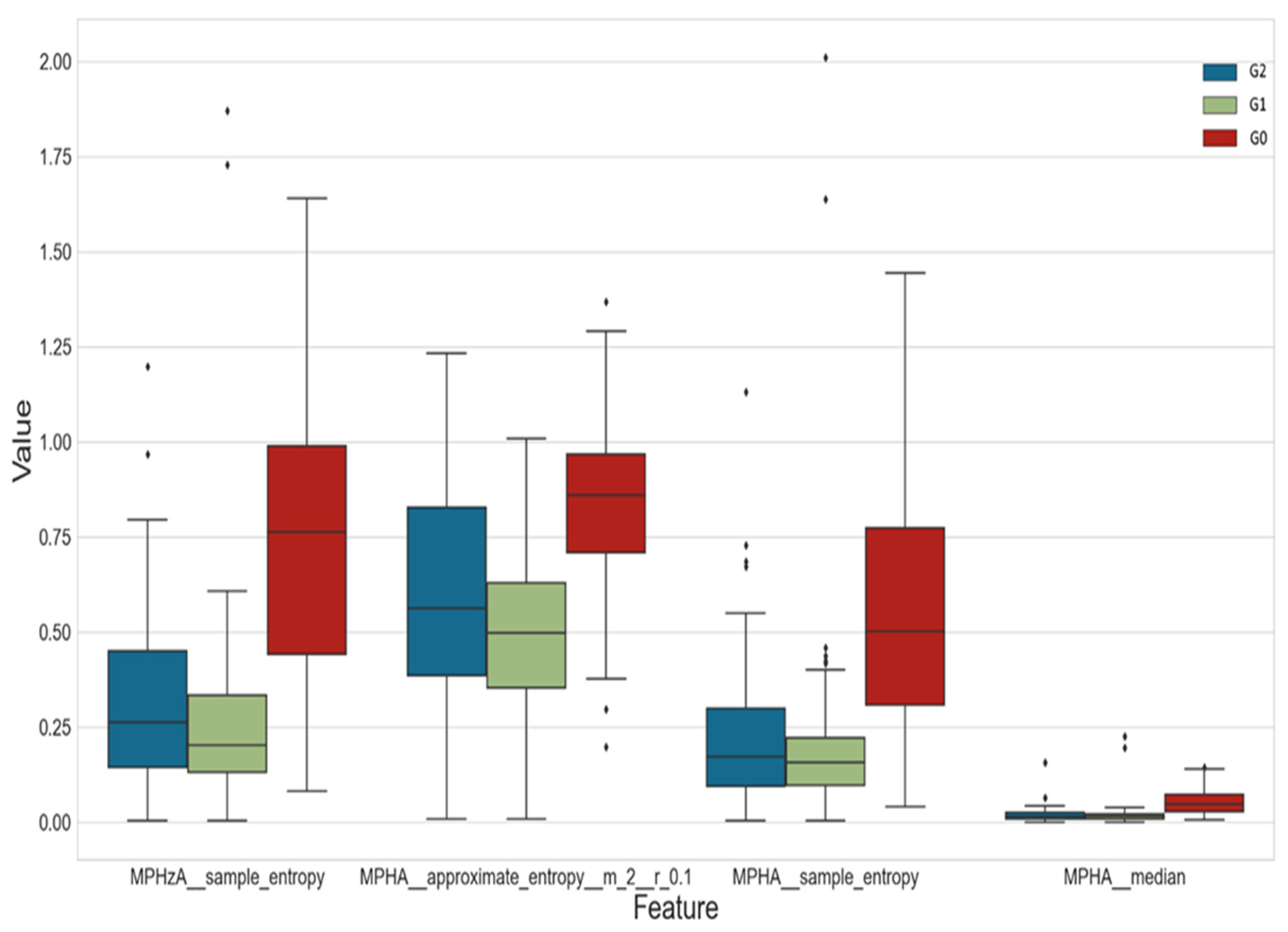
3. Results
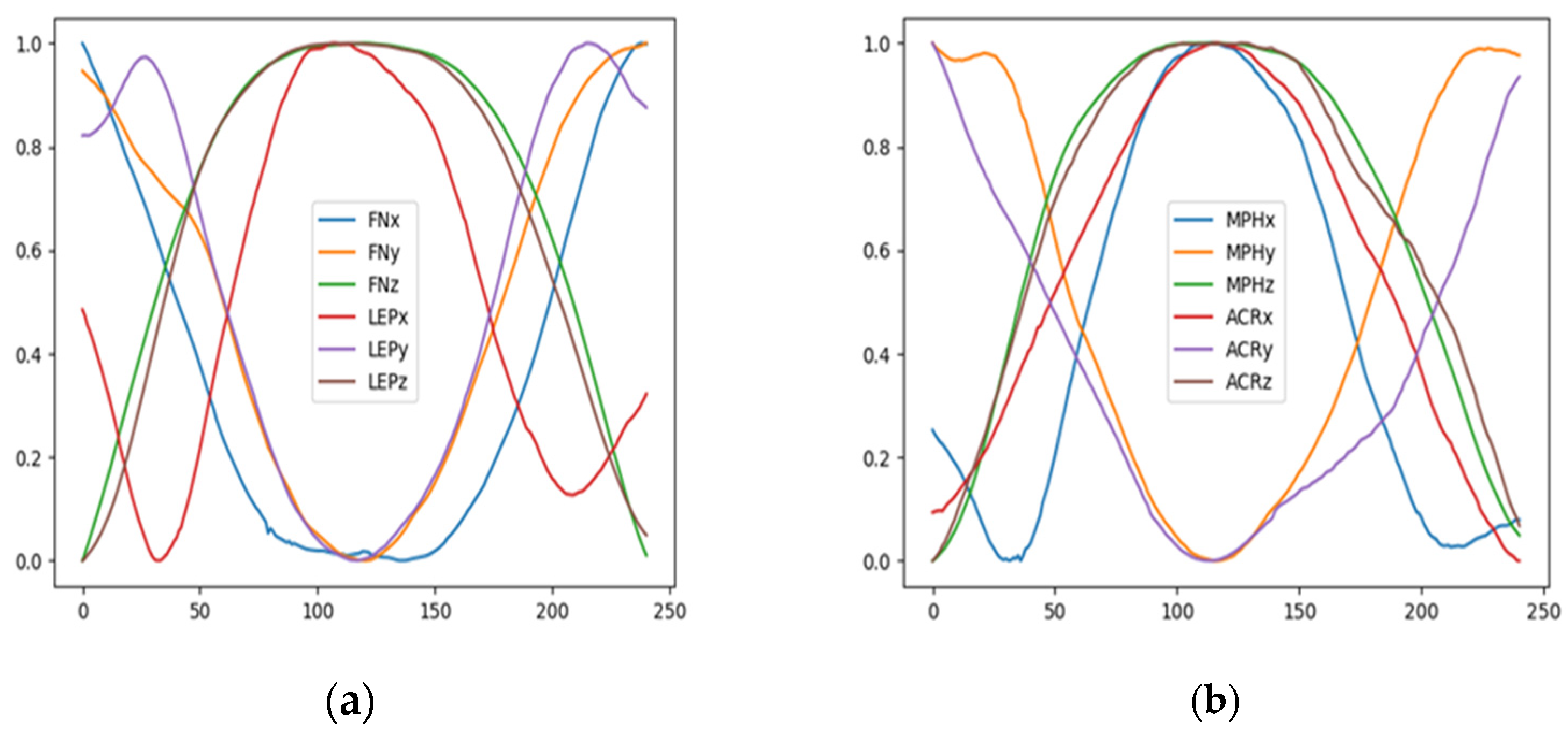
Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sathian, K.; Buxbaum, L.J.; Cohen, L.G.; Krakauer, J.W.; Lang, C.E.; Corbetta, M.; Fitzpatrick, S.M. Neurological principles and rehabilitation of action disorders: Common clinical deficits. Neurorehabil. Neural Repair. 2011, 25, 21S–32S. [Google Scholar] [CrossRef] [PubMed]
- Béjot, Y.; Bailly, H.; Durier, J.; Giroud, M. Epidemiology of stroke in Europe and trends for the 21st century. Presse Med. 2016, 45(12 Pt2), e391–e398. [Google Scholar] [CrossRef] [PubMed]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef] [PubMed]
- Resquín, F.; Gonzalez-Vargas, J.; Ibáñez, J.; Brunetti, F.; Dimbwadyo, I.; Carrasco, L.; Alves, S.; Gonzalez-Alted, C.; Gomez-Blanco, A.; Pons, J.L. Adaptive hybrid robotic system for rehabilitation of reaching movement after a brain injury: A usability study. J. Neuroeng. Rehabil. 2017, 14, 104. [Google Scholar] [CrossRef]
- Pike, S.; Cusick, A.; Wales, K.; Cameron, L.; Turner-Stokes, L.; Ashford, S.; Lannin, N.A. Psychometric properties of measures of upper limb activity performance in adults with and without spasticity undergoing neurorehabilitation-A systematic review. PLoS ONE 2021, 16, e0246288. [Google Scholar] [CrossRef] [PubMed]
- Hijikata, N.; Kawakami, M.; Ishii, R.; Tsuzuki, K.; Nakamura, T.; Okuyama, K.; Liu, M. Item Difficulty of Fugl-Meyer Assessment for Upper Extremity in Persons with Chronic Stroke With Moderate-to-Severe Upper Limb Impairment. Front. Neurol. 2020, 11, 577855. [Google Scholar] [CrossRef]
- Olesh, E.V.; Yakovenko, S.; Gritsenko, V. Automated Assessment of Upper Extremity Movement Impairment due to Stroke. PLoS ONE 2014, 9, e104487. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer assessment of motor recovery after stroke: A critical review of its measurement properties. Neurorehabil. Neural Repair. 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Johansson, G.M.; Grip, H.; Levin, M.F.; Häger, C.K. The added value of kinematic evaluation of the timed finger-to-nose test in persons post-stroke. J. Neuroeng. Rehabil. 2017, 14, 11. [Google Scholar] [CrossRef]
- Subramanian, S.K.; Baniña, M.C.; Sambasivan, K.; Haentjens, K.; Finestone, H.M.; Sveistrup, H.; Levin, M.F. Motor-Equivalent Intersegmental Coordination Is Impaired in Chronic Stroke. Neurorehabil. Neural Repair 2020, 34, 210–221. [Google Scholar] [CrossRef]
- Mesquita, I.A.; Fonseca, P.F.P.D.; Pinheiro, A.R.V.; Velhote Correia, M.F.P.; Silva, C.I.C.D. Methodological considerations for kinematic analysis of upper limbs in healthy and poststroke adults Part II: A systematic review of motion capture systems and kinematic metrics. Top Stroke Rehabil. 2019, 26, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Valevicius, A.M.; Boser, Q.A.; Lavoie, E.B.; Chapman, C.S.; Pilarski, P.M.; Hebert, J.S.; Vette, A.H. Characterization of normative angular joint kinematics during two functional upper limb tasks. Gait Posture 2019, 69, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Kanzler, C.M.; Lambercy, O.; Luft, A.R.; Veerbeek, J.M. Systematic Review on Kinematic Assessments of Upper Limb Movements After Stroke. Stroke 2019, 50, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Valevicius, A.M.; Jun, P.Y.; Hebert, J.S.; Vette, A.H. Use of optical motion capture for the analysis of normative upper body kinematics during functional upper limb tasks: A systematic review. J. Electromyogr. Kinesiol. 2018, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.E.; Crowner, B.E.; Kluding, P.M.; Nichols, D.; Rose, D.K.; Yoshida, R.; Pinto Zipp, G. Outcome measures for individuals with stroke: Process and recommendations from the American Physical Therapy Association neurology section task force. Phys. Ther. 2013, 93, 1383–1396. [Google Scholar] [CrossRef]
- Schwarz, A.; Veerbeek, J.M.; Held, J.P.O.; Buurke, J.H.; Luft, A.R. Measures of Interjoint Coordination Post-stroke Across Different Upper Limb Movement Tasks. Front. Bioeng. Biotechnol. 2021, 8, 620805. [Google Scholar] [CrossRef]
- Huang, V.S.; Krakauer, J.W. Robotic neurorehabilitation: A computational motor learning perspective. J. Neuroeng. Rehabil. 2009, 6, 5. [Google Scholar] [CrossRef]
- Flash, T.; Hogan, N. The coordination of arm movements: An experimentally confirmed mathematical model. J. Neurosci. 1985, 5, 1688–1703. [Google Scholar] [CrossRef]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: Past, present and future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef]
- Sehle, A.; Stuerner, J.; Hassa, T.; Spiteri, S.; Schoenfeld, M.A.; Liepert, J. Behavioral and neurophysiological effects of an intensified robot-assisted therapy in subacute stroke: A case control study. J. Neuroeng. Rehabil. 2021, 18, 6. [Google Scholar] [CrossRef]
- Kwakkel, G.; van Wegen, E.E.H.; Burridge, J.H.; Winstein, C.J.; van Dokkum, L.E.H.; Alt Murphy, M.; Levin, M.F.; Krakauer, J.W.; ADVISORY group. Standardized Measurement of Quality of Upper Limb Movement After Stroke: Consensus-Based Core Recommendations From the Second Stroke Recovery and Rehabilitation Roundtable. Neurorehabil. Neural Repair 2019, 33, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Wey, H.Y.; Desai, V.R.; Duong, T.Q. A review of current imaging methods used in stroke research. Neurol. Res. 2013, 35, 1092–1102. [Google Scholar] [CrossRef] [PubMed]
- Liang, P.; Kwong, W.H.; Sidarta, A.; Yap, C.K.; Tan, W.K.; Lim, L.S.; Chan, P.Y.; Kuah, C.W.K.; Wee, S.K.; Chua, K.; et al. An Asian-centric human movement database capturing activities of daily living. Sci. Data 2020, 7, 290. [Google Scholar] [CrossRef] [PubMed]
- Blaszczyszyn, M.; Szczesna, A.; Opara, J.; Konieczny, M.; Pakosz, P.; Balko, S. Functional differences in upper limb movement after early and chronic stroke based on kinematic motion indicators. Biomed. Pap. Med. Fac. Univ. Palacky. Olomouc Czech Repub. 2018; ahead of print. [Google Scholar] [CrossRef]
- Szczęsna, A.; Błaszczyszyn, M.; Kawala-Sterniuk, A. Convolutional neural network in upper limb functional motion analysis after stroke. Peer J. 2020, 8, e10124. [Google Scholar] [CrossRef]
- Jarrassé, N.; Proietti, T.; Crocher, V.; Robertson, J.; Sahbani, A.; Morel, G.; Roby-Brami, A. Robotic exoskeletons: A perspective for the rehabilitation of arm coordination in stroke patients. Front. Hum. Neurosci. 2014, 8, 947. [Google Scholar] [CrossRef]
- Huang, X.; Naghdy, F.; Naghdy, G.; Du, H.; Todd, C. Robot-assisted post-stroke motion rehabilitation in upper extremities: A survey. Int. J. Dis. Hum. Dev. 2017, 16, 233–247. [Google Scholar] [CrossRef]
- Nagymáté, G.; Rita, M.K. Application of OptiTrack Motion Capture Systems in Human Movement Analysis: A Systematic Literature Review. RIiM 2018, 5, 1–9. [Google Scholar] [CrossRef]
- Wu, G.; van der Helm, F.C.; Veeger, H.E.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Heller, A.; Wade, D.T.; Wood, V.A.; Sunderland, A.; Hewer, R.L.; Ward, E. Arm function after stroke: Measurement and recovery over the first three months. J. Neurol. Neurosurg. Psychiatry 1987, 50, 714–719. [Google Scholar] [CrossRef]
- Christ, M.; Braun, N.; Neuffer, J.; Kempa-Liehr, A.W. Time series feature extraction on basis of scalable hypothesis tests (tsfresh—A python package). Neurocomputing 2018, 307, 72–77. [Google Scholar] [CrossRef]
- Dindorf, C.; Teufl, W.; Taetz, B.; Bleser, G.; Fröhlich, M. Interpretability of Input Representations for Gait Classification in Patients after Total Hip Arthroplasty. Sensors 2020, 20, 4385. [Google Scholar] [CrossRef] [PubMed]
- Yoav, B.; and Yekutieli, D. The control of the false discovery rate in multiple testing under dependency. Ann. Stat. 2001, 29, 1165–1188. [Google Scholar] [CrossRef]
- Lum, P.S.; Shu, L.; Bochniewicz, E.M.; Tran, T.; Chang, L.C.; Barth, J.; Dromerick, A.W. Improving Accelerometry-Based Measurement of Functional Use of the Upper Extremity After Stroke: Machine Learning Versus Counts Threshold Method. Neurorehabil. Neural Repair 2020, 34, 1078–1087. [Google Scholar] [CrossRef]
- van der Vliet, R.; Selles, R.W.; Andrinopoulou, E.R.; Nijland, R.; Ribbers, G.M.; Frens, M.A.; Meskers, C.; Kwakkel, G. Predicting Upper Limb Motor Impairment Recovery after Stroke: A Mixture Model. Ann. Neurol. 2020, 87, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Regterschot, G.R.H.; Bussmann, J.B.J.; Fanchamps, M.H.J.; Meskers, C.G.M.; Ribbers, G.M.; Selles, R.W. Objectively measured arm use in daily life improves during the first 6 months poststroke: A longitudinal observational cohort study. J. Neuroeng. Rehabil. 2021, 18, 51. [Google Scholar] [CrossRef]
- Maffiuletti, N.A. Physiological and methodological considerations for the use of neuromuscular electrical stimulation. Eur. J. Appl. Physiol. 2010, 110, 223–234. [Google Scholar] [CrossRef]
- Konieczny, M.; Pakosz, P.; Domaszewski, P.; Błaszczyszyn, M.; Kawala-Sterniuk, A. Analysis of Upper Limbs Target-Reaching Movement and Muscle Co-Activation in Patients with First Time Stroke for Rehabilitation Progress Monitoring. Appl. Sci. 2022, 12, 1551. [Google Scholar] [CrossRef]
- Barth, J.; Klaesner, J.W.; Lang, C.E. Relationships between accelerometry and general compensatory movements of the upper limb after stroke. J. Neuroeng. Rehabil. 2020, 17, 138. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Marker Signals | FNR, FNL | LEPR, LEPL | MPHR, MPHL | ACRR, ACRL |
|---|---|---|---|---|
| 3D trajectories (coordinates) of markers | FNx, FNy, FNz | LEPx, LEPy, LEPz | MPHx, MPHy, MPHz | ACRx, ACRy, ACRz |
| 3D displacement of markers | FNdx, FNdy, FNdz | LEPdx, LEPdy, LEPdz | MPHdx, MPHdy, MPHdz | ACRdx, ACRdy, ACRdz |
| Displacement module | FND | LEPD | MPHD | ACRD |
| 3D velocities of markers | FNvx, FNvy, FNvz | LEPvx, LEPvy, LEPvz | MPHvx, MPHvy, MPHvz | ACRvx, ACRvy, ACRvz |
| Speed | FNV | LEPV | MPHV | ACRV |
| 3D accelerations of markers | FNax, FNay, FNaz | LEPax, LEPay, LEPaz | MPHax, MPHay, MPHaz | ACRax, ACRay, ACRaz |
| Acceleration module | FNA | LEPA | MPHA | ACRA |
| Class | Number of Participants | Recorded Upper Limb | Number of Recordings |
|---|---|---|---|
| G0 | 35 after stroke | non-affected | 105 |
| G1 | 35 after stroke | affected | 105 |
| G2 | 19 control group | the left and right healthy upper limb | 114 |
| Module | Trajectory | Acceleration | Velocity | Displacement | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ACR | 38 | A | 52 | X | 26 | X | 29 | X | 42 | X |
| 35 | V | 0 | Y | 14 | Y | 9 | Y | 11 | Y | |
| 13 | D | 0 | Z | 35 | Z | 30 | Z | 4 | Z | |
| MPH | 62 | A | 47 | X | 34 | X | 42 | X | 37 | X |
| 62 | V | 6 | Y | 12 | Y | 7 | Y | 30 | Y | |
| 15 | D | 14 | Z | 35 | Z | 53 | Z | 3 | Z | |
| LEP | 18 | A | 31 | X | 2 | X | 3 | X | 14 | X |
| 7 | V | 3 | Y | 3 | Y | 0 | Y | 3 | Y | |
| 3 | D | 11 | Z | 4 | Z | 0 | Z | 2 | Z | |
| FN | 7 | A | 1 | X | 5 | X | 3 | X | 0 | X |
| 0 | V | 8 | Y | 11 | Y | 0 | Y | 6 | Y | |
| 12 | D | 11 | Z | 29 | Z | 7 | Z | 3 | Z | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Błaszczyszyn, M.; Szczęsna, A.; Konieczny, M.; Pakosz, P.; Balko, S.; Borysiuk, Z. Quantitative Assessment of Upper Limb Movement in Post-Stroke Adults for Identification of Sensitive Measures in Reaching and Lifting Activities. J. Clin. Med. 2023, 12, 3333. https://doi.org/10.3390/jcm12093333
Błaszczyszyn M, Szczęsna A, Konieczny M, Pakosz P, Balko S, Borysiuk Z. Quantitative Assessment of Upper Limb Movement in Post-Stroke Adults for Identification of Sensitive Measures in Reaching and Lifting Activities. Journal of Clinical Medicine. 2023; 12(9):3333. https://doi.org/10.3390/jcm12093333
Chicago/Turabian StyleBłaszczyszyn, Monika, Agnieszka Szczęsna, Mariusz Konieczny, Paweł Pakosz, Stefan Balko, and Zbigniew Borysiuk. 2023. "Quantitative Assessment of Upper Limb Movement in Post-Stroke Adults for Identification of Sensitive Measures in Reaching and Lifting Activities" Journal of Clinical Medicine 12, no. 9: 3333. https://doi.org/10.3390/jcm12093333
APA StyleBłaszczyszyn, M., Szczęsna, A., Konieczny, M., Pakosz, P., Balko, S., & Borysiuk, Z. (2023). Quantitative Assessment of Upper Limb Movement in Post-Stroke Adults for Identification of Sensitive Measures in Reaching and Lifting Activities. Journal of Clinical Medicine, 12(9), 3333. https://doi.org/10.3390/jcm12093333