
Blood-Based Biomarkers Reflecting Protease 3 and MMP-12 Catalyzed Elastin Degradation as Potential Noninvasive Surrogate Markers of Endoscopic and Clinical Disease in Inflammatory Bowel Disease
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Information
2.2. Endoscopic and Clinical Disease Definitions
2.3. Biomarker Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
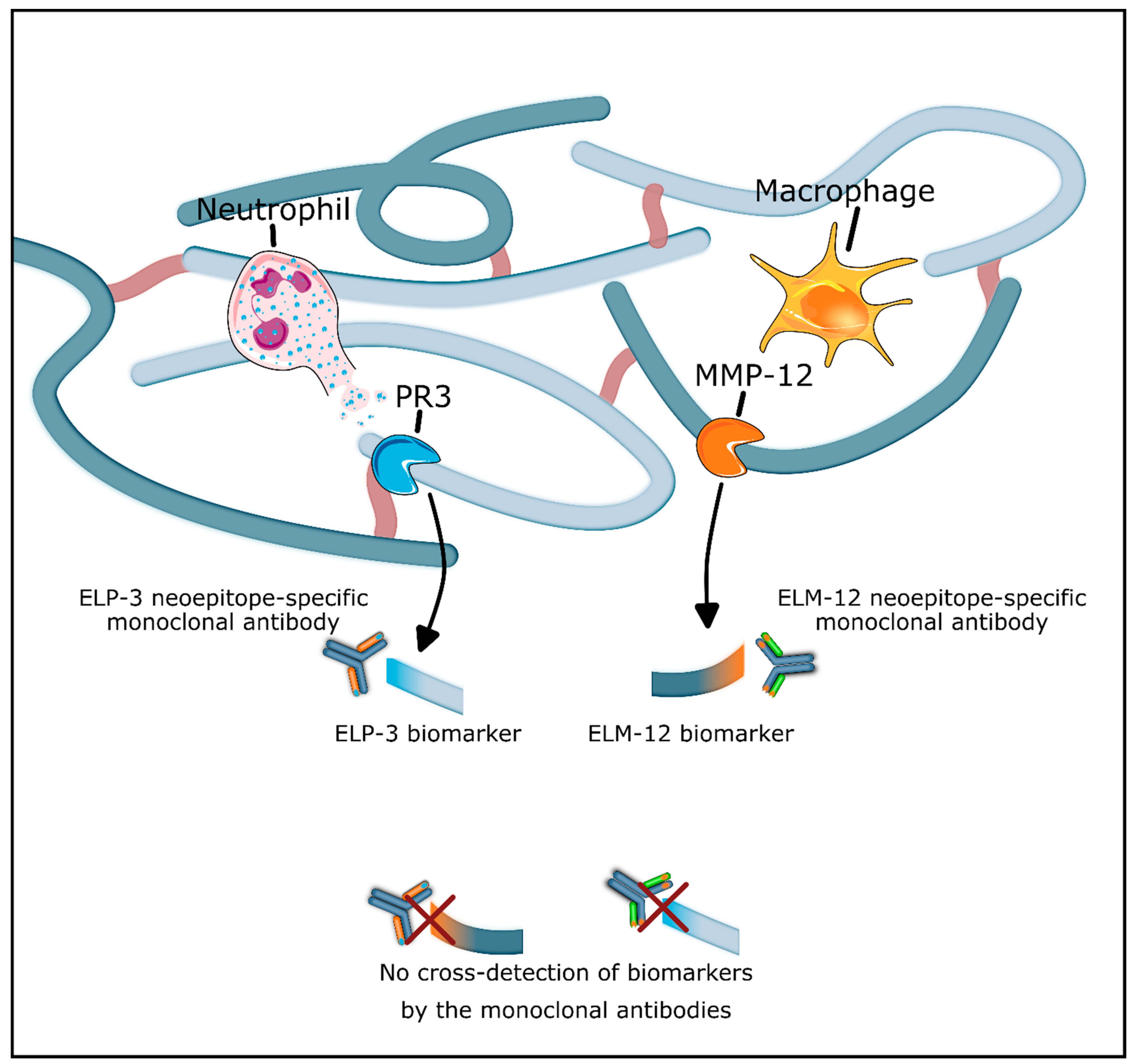
3.2. Elevation of Proteolytic Elastin Degradation in Patients with IBD
3.3. Elastin Degradation Biomarkers Are Associated with Endoscopic and Clinical Disease in CD Patients
3.4. Biomarkers of PR3- and MMP-12-Catalyzed Elastin Degradation in Patients with UC
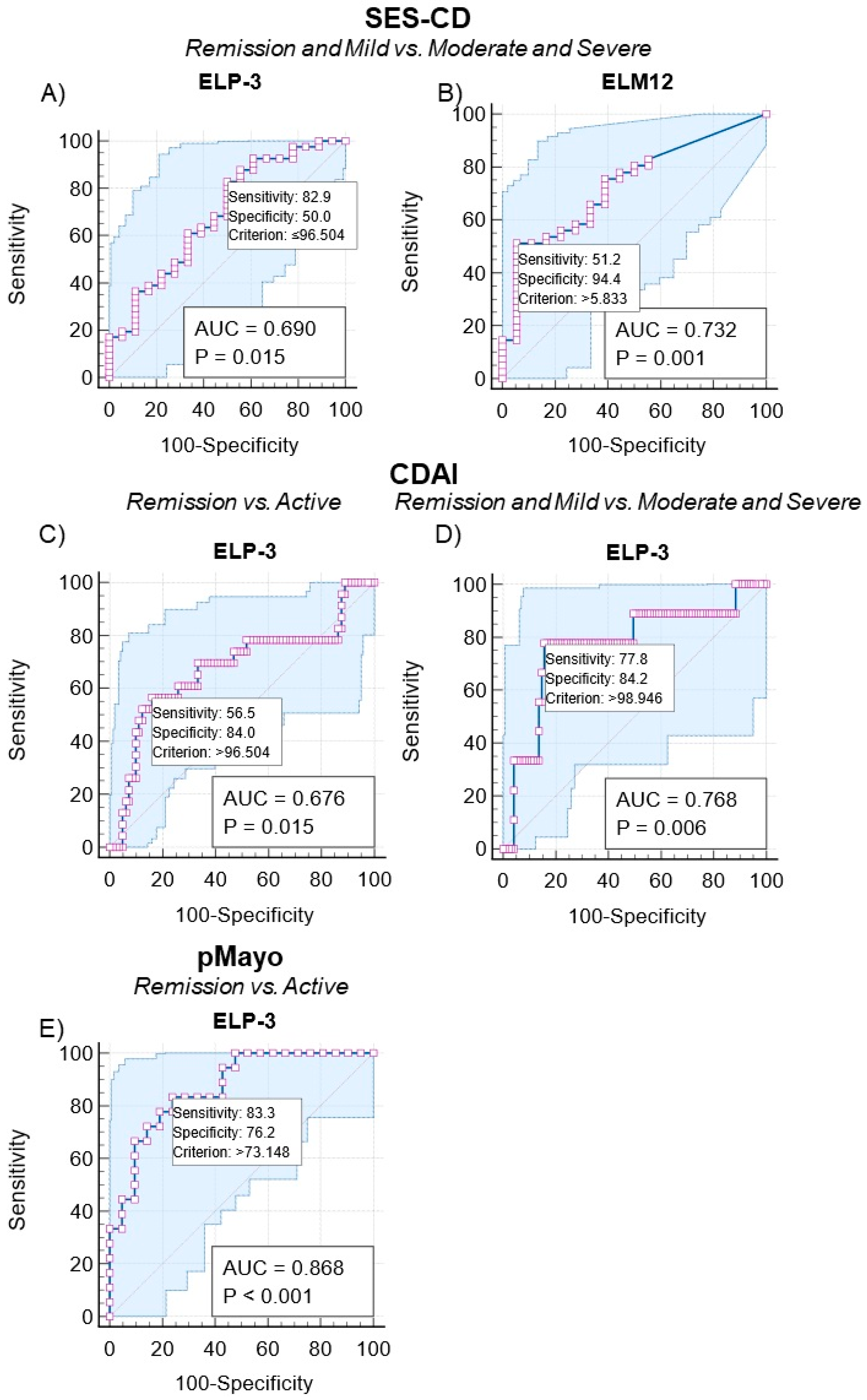
3.5. Discriminating Patients with CD and UC According to Endoscopic and Clinical Disease Activity Using Elastin Degradation Biomarkers
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Sabatino, A.; Lenti, M.V.; Giuffrida, P.; Vanoli, A.; Corazza, G.R. New insights into immune mechanisms underlying autoimmune diseases of the gastrointestinal tract. Autoimmun. Rev. 2015, 14, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C.; Sandborn, W.J. Crohn’s disease. Lancet 2012, 380, 1590–1605. [Google Scholar] [CrossRef] [PubMed]
- De Souza, H.S.P.; Fiocchi, C.; Iliopoulos, D. The IBD interactome: An integrated view of aetiology, pathogenesis and therapy. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 739–749. [Google Scholar] [CrossRef]
- Shimshoni, E.; Yablecovitch, D.; Baram, L.; Dotan, I.; Sagi, I. ECM remodelling in IBD: Innocent bystander or partner in crime? The emerging role of extracellular molecular events in sustaining intestinal inflammation. Gut 2015, 64, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, J.; Lindholm, M.; Langholm, L.; Kjeldsen, J.; Bay-Jensen, A.; Karsdal, M.; Manon-Jensen, T. The intestinal tissue homeostasis—The role of extracellular matrix remodeling in inflammatory bowel disease. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 977–993. [Google Scholar] [CrossRef] [PubMed]
- Kirov, S.; Sasson, A.; Zhang, C.; Chasalow, S.; Dongre, A.; Steen, H.; Stensballe, A.; Andersen, V.; Birkelund, S.; Bennike, T.B. Degradation of the extracellular matrix is part of the pathology of ulcerative colitis. Mol. Omics 2019, 15, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Kirkegaard, T.; Hansen, A.; Bruun, E.; Brynskov, J. Expression and localisation of matrix metalloproteinases and their natural inhibitors in fistulae of patients with Crohn’s disease. Gut 2004, 53, 701–709. [Google Scholar] [CrossRef]
- Atreya, R.; Neurath, M.F. Current and Future Targets for Mucosal Healing in Inflammatory Bowel Disease. Visc. Med. 2017, 33, 82–88. [Google Scholar] [CrossRef]
- Lenti, M.V.; Di Sabatino, A. Intestinal fibrosis. Mol. Asp. Med. 2019, 65, 100–109. [Google Scholar] [CrossRef]
- Hirten, R.P.; Shah, S.; Sachar, D.B.; Colombel, J.-F. The Management of Intestinal Penetrating Crohn’s Disease. Inflamm. Bowel Dis. 2018, 24, 752–765. [Google Scholar] [CrossRef]
- Tian, C.-M.; Zhang, Y.; Yang, M.-F.; Xu, H.-M.; Zhu, M.-Z.; Yao, J.; Wang, L.-S.; Liang, Y.-J.; Li, D.-F. Stem Cell Therapy in Inflammatory Bowel Disease: A Review of Achievements and Challenges. J. Inflamm. Res. 2023, 16, 2089–2119. [Google Scholar] [CrossRef] [PubMed]
- Domislovic, V.; Mortensen, J.H.; Lindholm, M.; Kaarsdal, M.A.; Brinar, M.; Barisic, A.; Manon-Jensen, T.; Krznaric, Z. Inflammatory Biomarkers of Extracellular Matrix Remodeling and Disease Activity in Crohn’s Disease and Ulcerative Colitis. J. Clin. Med. 2022, 11, 5907. [Google Scholar] [CrossRef] [PubMed]
- Alexdottir, M.S.; Bourgonje, A.R.; Karsdal, M.A.; Pehrsson, M.; Loveikyte, R.; van Dullemen, H.M.; Visschedijk, M.C.; Festen, E.A.M.; Weersma, R.K.; Faber, K.N.; et al. Serological Biomarkers of Extracellular Matrix Turnover and Neutrophil Activity Are Associated with Long-Term Use of Vedolizumab in Patients with Crohn’s Disease. Int. J. Mol. Sci. 2022, 23, 8137. [Google Scholar] [CrossRef] [PubMed]
- Bourgonje, A.R.; Alexdottir, M.S.; Otten, A.T.; Loveikyte, R.; Bay-Jensen, A.; Pehrsson, M.; van Dullemen, H.M.; Visschedijk, M.C.; Festen, E.A.M.; Weersma, R.K.; et al. Serological biomarkers of type I, III and IV collagen turnover are associated with the presence and future progression of stricturing and penetrating Crohn’s disease. Aliment. Pharmacol. Ther. 2022, 56, 675–693. [Google Scholar] [CrossRef] [PubMed]
- Hedtke, T.; Schräder, C.U.; Heinz, A.; Hoehenwarter, W.; Brinckmann, J.; Groth, T.; Schmelzer, C.E.H. A comprehensive map of human elastin cross-linking during elastogenesis. FEBS J. 2019, 286, 3594–3610. [Google Scholar] [CrossRef] [PubMed]
- Heinz, A. Elastases and elastokines: Elastin degradation and its significance in health and disease. Crit. Rev. Biochem. Mol. Biol. 2020, 55, 252–273. [Google Scholar] [CrossRef] [PubMed]
- Bennike, T.B.; Carlsen, T.G.; Ellingsen, T.; Bonderup, O.K.; Glerup, H.; Bøgsted, M.; Christiansen, G.; Birkelund, S.; Stensballe, A.; Andersen, V. Neutrophil extracellular traps in ulcerative colitis: A proteome analysis of intestinal biopsies. Inflamm. Bowel Dis. 2015, 21, 2052–2067. [Google Scholar] [CrossRef] [PubMed]
- Kuckleburg, C.J.; Newman, P.J.; Sevigny, L.M.; Austin, K.M.; Zhang, P.; Kasuda, S.; Koukos, G.; Sharifi, S.; Covic, L.; Kuliopulos, A.; et al. Neutrophil proteinase 3 acts on protease-activated receptor-2 to enhance vascular endothelial cell barrier function. Arter. Thromb. Vasc. Biol. 2013, 33, 275–284. [Google Scholar] [CrossRef]
- Pender, S.L.; Li, C.; Sabatino, A.; Macdonald, T.; Buckley, M. Role of macrophage metalloelastase in gut inflammation. Ann. N. Y. Acad. Sci. 2006, 1072, 386–388. [Google Scholar] [CrossRef]
- Lobatón, T.; Bessissow, T.; De Hertogh, G.; Lemmens, B.; Maedler, C.; Van Assche, G.; Vermeire, S.; Bisschops, R.; Rutgeerts, P.; Bitton, A.; et al. The Modified Mayo Endoscopic Score (MMES): A New Index for the Assessment of Extension and Severity of Endoscopic Activity in Ulcerative Colitis Patients. J. Crohn’s Colitis 2015, 9, 846–852. [Google Scholar] [CrossRef]
- Sakurai, T.; Saruta, M. Positioning and Usefulness of Biomarkers in Inflammatory Bowel Disease. Digestion 2023, 104, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Pehrsson, M.; Alexdóttir, M.S.; Karsdal, M.A.; Thakker, P.; Mortensen, J. Novel fibro-inflammatory biomarkers associated with disease activity in patients with Crohn’s disease. Expert Rev. Gastroenterol. Hepatol. 2023, 17, 575–587. [Google Scholar] [CrossRef] [PubMed]
- Nighot, M.; Ganapathy, A.S.; Saha, K.; Suchanec, E.; Castillo, E.F.; Gregory, A.; Shapiro, S.; Ma, T.; Nighot, P. Matrix Metalloproteinase MMP-12 Promotes Macrophage Transmigration across Intestinal Epithelial Tight Junctions and Increases Severity of Experimental Colitis. J. Crohn’s Colitis 2021, 15, 1751–1765. [Google Scholar] [CrossRef] [PubMed]
- Di Sabatino, A.; Saarialho-Kere, U.; Buckley, M.G.; Gordon, J.N.; Biancheri, P.; Rovedatti, L.; Corazza, G.R.; MacDonald, T.T.; Pender, S.L. Stromelysin-1 and macrophage metalloelastase expression in the intestinal mucosa of Crohn’s disease patients treated with infliximab. Eur. J. Gastroenterol. Hepatol. 2009, 21, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Tang, G. Macrophages in intestinal fibrosis and regression. Cell. Immunol. 2022, 381, 104614. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, M.; Sahin, K.B.; West, Z.E.; Murray, R.Z. Macrophage Phenotypes Regulate Scar Formation and Chronic Wound Healing. Int. J. Mol. Sci. 2017, 18, 1545. [Google Scholar] [CrossRef] [PubMed]
- Krzyszczyk, P.; Schloss, R.; Palmer, A.; Berthiaume, F. The Role of Macrophages in Acute and Chronic Wound Healing and Interventions to Promote Pro-wound Healing Phenotypes. Front. Physiol. 2018, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Qiao, L.; Fang, L.; Zhu, J.; Xiang, Y.; Xu, H.; Sun, X.; Chen, H.; Yang, B. Total Flavone of Abelmoschus manihot Ameliorates TNBS-Induced Colonic Fibrosis by Regulating Th17/Treg Balance and Reducing Extracellular Matrix. Front. Pharmacol. 2021, 12, 769793. [Google Scholar] [CrossRef]
- Curciarello, R.; Sobande, T.; Jones, S.; Giuffrida, P.; Di Sabatino, A.; Docena, G.H.; MacDonald, T.T.; Kok, K. Human Neutrophil Elastase Proteolytic Activity in Ulcerative Colitis Favors the Loss of Function of Therapeutic Monoclonal Antibodies. J. Inflamm. Res. 2020, 13, 233–243. [Google Scholar] [CrossRef]
- Aoyama, Y.; Inaba, T.; Takahashi, S.; Yasuhara, H.; Hiraoka, S.; Morimoto, T.; Colvin, H.S.; Wato, M.; Ando, M.; Nakamura, S.; et al. Anti-proteinase 3 antineutrophil cytoplasmic antibody reflects disease activity and predicts the response to steroid therapy in ulcerative colitis. BMC Gastroenterol. 2021, 21, 325. [Google Scholar] [CrossRef]
- Lewis, J.D.; Chuai, S.; Nessel, L.; Lichtenstein, G.R.; Aberra, F.N.; Ellenberg, J.H. Use of the noninvasive components of the Mayo score to assess clinical response in ulcerative colitis. Inflamm. Bowel Dis. 2008, 14, 1660–1666. [Google Scholar] [CrossRef]
- Ma, C.; Sandborn, W.J.; D’haens, G.R.; Zou, G.; Stitt, L.W.; Singh, S.; Ananthakrishnan, A.N.; Dulai, P.S.; Khanna, R.; Jairath, V.; et al. Discordance Between Patient-Reported Outcomes and Mucosal Inflammation in Patients With Mild to Moderate Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2020, 18, 1760–1768.e1. [Google Scholar] [CrossRef]
- Mortensen, J.H.M.; van Haaften, W.T.; Karsdal, M.A.; Bay-Jensen, A.-C.; Olinga, P.; Grønbæk, H.; Hvas, C.L.; Manon-Jensen, T.; Dijkstra, G.; Dige, A. The Citrullinated and MMP-degraded Vimentin Biomarker (VICM) Predicts Early Response to Anti-TNFα Treatment in Crohn’s Disease. J. Clin. Gastroenterol. 2021, 55, 59–66. [Google Scholar] [CrossRef]
- Mortensen, J.H.; Sinkeviciute, D.; Manon-Jensen, T.; Domislović, V.; McCall, K.; Thudium, C.S.; Brinar, M.; Önnerfjord, P.; Goodyear, C.S.; Krznarić, Ž.; et al. A specific calprotectin neo-epitope (CPa9-HNE) in serum from inflammatory bowel disease patients is associated with neutrophil activity and endoscopic severity. J. Crohn’s Colitis 2022, 16, 1447–1460. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | CD (n = 104) | UC (n = 39) | Healthy Donors (n = 29) | p-Values |
|---|---|---|---|---|
| Age, years (IQR) | 36 (17.75) | 38 (24) | 39.5 (14) | p > 0.999 |
| Gender, male, n (%) | 66 (63.5) | 23 (59) | 17 (58.6) | p = 0.829 |
| BMI, kg/m2 (IQR) | 22.9 (6.39) | 23.7 (6.3) | p = 0.934 | |
| Smoking, yes, n (%) | 23 (22.1) | 5 (12.8) | p = 0.246 | |
| Montreal L (CD), n (%) L1/L2/L3 | 17 (17.5)/17 (17.5)/63 (65.0) | / | ||
| Montreal B (CD), n (%) B1/B2/B3 | 34 (39.5)/35 (40.7)/17 (19.8) | / | ||
| Montreal E (UC), n (%) E1/E2/E3 | / | 4 (10.0)/12 (30.0)/24 (60.0) | ||
| Endoscopic activity (SES-CD and MES), n (%) Remission/mild/moderate to severe | 31 (50.8)/11 (18.0)/19 (31.1) | 6 (18.8)/9 (28.1)/17 (53.1) | ||
| Modified Mayo Endoscopic Score, n (%) Remission/mild/moderate to severe | / | 9 (28.1)/13 (40.6)/10 (31.3) | ||
| Clinical activity (CDAI and pMayo), n (%) Remission/mild/moderate to severe | 81 (77.9)/14 (13.5)/9 (8.7) | 21 (53.8)/9 (23.1)/9 (23.1) | ||
| Biological therapy, yes, n (%) | 62 (59.6) | 27 (56.3) | p = 0.336 | |
| Ileal resection, yes, n (%) | 52 (50.0) | / | ||
| Disease duration (years) (IQR) | 9.0 (12.0) | 6.0 (7.0) | p = 0.014 | |
| CRP, mg/L (IQR) | 2.5 (5.1) | 2.6 (7.8) | p = 0.884 |
| Disease Scoring | Patient Grouping | Biomarker | AUC | AUC CI | Sensitivity (95% CI) | Specificity (95% CI) | Youden Index | p-Value |
|---|---|---|---|---|---|---|---|---|
| SES-CD | Remission vs. active | ELP-3 | 0.59 | 0.45 to 0.71 | 93.5 (78.6–99.2) | 28.6 (13.2–48.7) | <110.27 | p = 0.260 |
| ELM-12 | 0.61 | 0.47 to 0.73 | 38.7 (21.8–57.8) | 85.7 (67.3–96.0) | ≥6.29 | p = 0.141 | ||
| Remission and mild vs. moderate and severe | ELP-3 | 0.69 | 0.56 to 0.80 | 82.9 (67.9–92.8) | 50.0 (26.0–74.0) | <96.50 | p = 0.015 | |
| ELM-12 | 0.73 | 0.60 to 0.84 | 51.2 (35.1–67.1) | 94.4 (72.7–99.9) | ≥5.83 | p = 0.001 | ||
| CDAI | Remission vs. active | ELP-3 | 0.68 | 0.58 to 0.76 | 83.9 (74.1–91.2) | 56.5 (34.5–76.8) | <96.50 | p = 0.015 |
| ELM-12 | 0.52 | 0.42 to 0.62 | 35.80 (25.4–47.2) | 82.6 (61.2–95.0) | ≥5.83 | p = 0.801 | ||
| Remission and mild vs. moderate and severe | ELP-3 | 0.77 | 0.68 to 0.85 | 84.2 (75.3–90.9) | 77.8 (40.0–97.2) | <98.95 | p = 0.006 | |
| ELM-12 | 0.54 | 0.44 to 0.64 | 67.4 (57.0–76.6) | 55.6 (21.2 86.3) | ≥5.70 | p = 0.689 |
| Disease Scoring | Patient Grouping | Biomarker | AUC | AUC CI | Sensitivity (95% CI) | Specificity (95% CI) | Youden Index | p-Value |
|---|---|---|---|---|---|---|---|---|
| mMES | Remission vs. active | ELP-3 | 0.52 | 0.33 to 0.70 | 11.1 (0.3–48.2) | 60.9 (38.5–80.3) | <54.88 | p = 0.875 |
| ELM-12 | 0.57 | 0.38 to 0.74 | 66.7 (29.9–92.5) | 60.9 (38.5–80.3) | ≥4.32 | p = 0.539 | ||
| Remission and mild vs. moderate and severe | ELP-3 | 0.52 | 0.34 to 0.70 | 59.1 (36.4–79.3) | 60.0 (26.2–87.8) | <82.91 | p = 0.846 | |
| ELM-12 | 0.62 | 0.43 to 0.78 | 59.1 (36.4–79.3) | 80.0 (44.4–97.5) | ≥4.32 | p = 0.261 | ||
| pMayo | Remission vs. active | ELP-3 | 0.87 | 0.72 to 0.96 | 76.2 (52.8–91.8) | 83.3 (58.6–96.4) | <73.15 | p < 0.0001 |
| ELM-12 | 0.65 | 0.48 to 0.79 | 90.5 (69.6–98.8) | 50.0 (26.0–74.0) | <5.59 | p = 0.107 | ||
| Remission and mild vs. moderate and severe | ELP-3 | 0.65 | 0.48 to 0.79 | 36.7 (19.9–56.1) | 100.0 (66.4–100.0) | <40.97 | p = 0.139 | |
| ELM-12 | 0.68 | 0.51 to 0.82 | 83.3 (65.3–94.4) | 66.7 (29.9–92.5) | <5.59 | p = 0.142 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pehrsson, M.; Domislovic, V.; Alexdottir, M.S.; Brinar, M.; Karsdal, M.A.; Barisic, A.; Krznaric, Z.; Mortensen, J.H. Blood-Based Biomarkers Reflecting Protease 3 and MMP-12 Catalyzed Elastin Degradation as Potential Noninvasive Surrogate Markers of Endoscopic and Clinical Disease in Inflammatory Bowel Disease. J. Clin. Med. 2024, 13, 21. https://doi.org/10.3390/jcm13010021
Pehrsson M, Domislovic V, Alexdottir MS, Brinar M, Karsdal MA, Barisic A, Krznaric Z, Mortensen JH. Blood-Based Biomarkers Reflecting Protease 3 and MMP-12 Catalyzed Elastin Degradation as Potential Noninvasive Surrogate Markers of Endoscopic and Clinical Disease in Inflammatory Bowel Disease. Journal of Clinical Medicine. 2024; 13(1):21. https://doi.org/10.3390/jcm13010021
Chicago/Turabian StylePehrsson, Martin, Viktor Domislovic, Marta Sorokina Alexdottir, Marko Brinar, Morten Asser Karsdal, Ana Barisic, Zeljko Krznaric, and Joachim Høg Mortensen. 2024. "Blood-Based Biomarkers Reflecting Protease 3 and MMP-12 Catalyzed Elastin Degradation as Potential Noninvasive Surrogate Markers of Endoscopic and Clinical Disease in Inflammatory Bowel Disease" Journal of Clinical Medicine 13, no. 1: 21. https://doi.org/10.3390/jcm13010021