
Evaluation of the Truncated Cone–Rhomboid Pyramid Formula for Simplified Right Ventricular Quantification: A Cardiac Magnetic Resonance Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
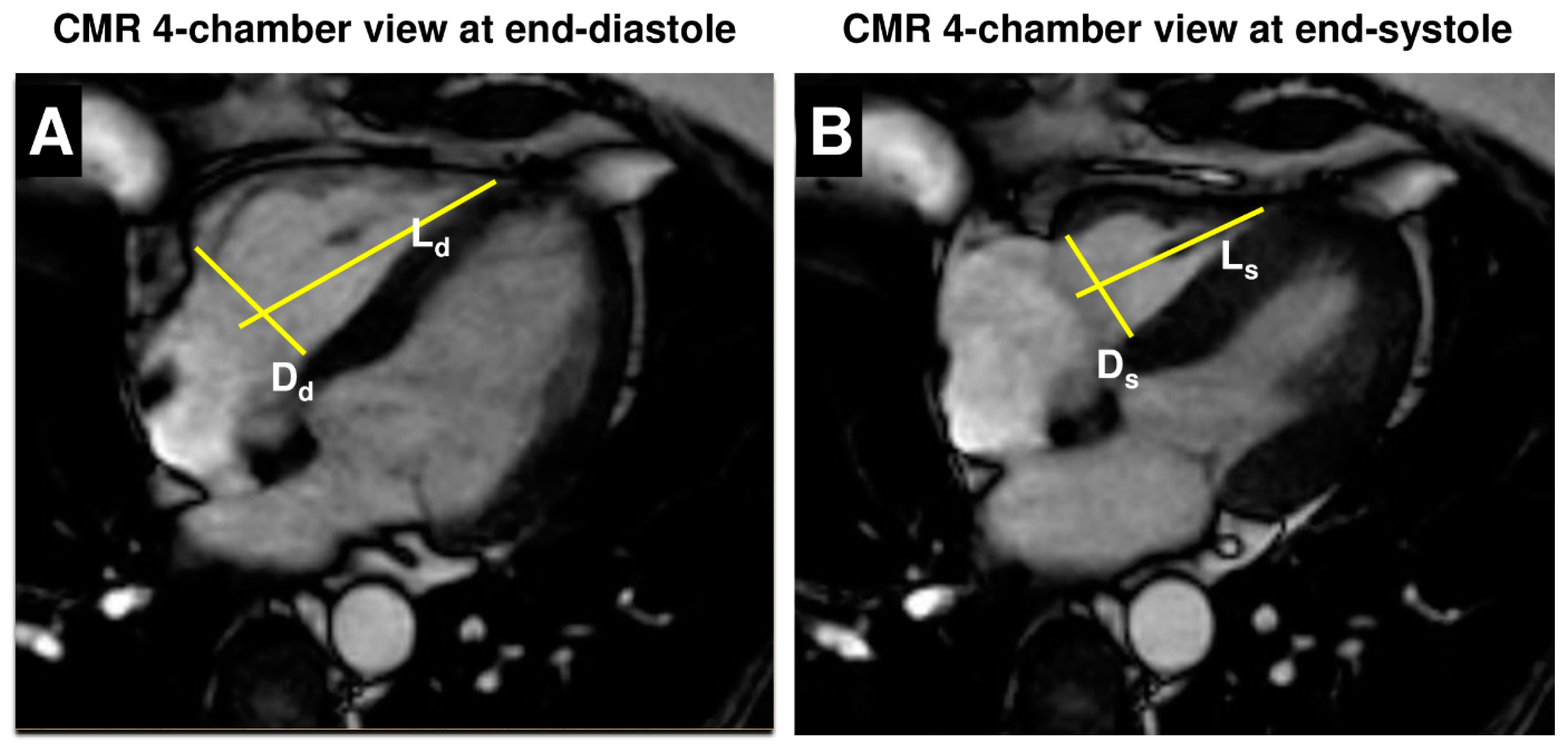
2.1. CMR Protocol
2.2. Statistical Analysis
3. Results
3.1. Comparison of RV Volumes and Function
3.2. Identification of Patients with Enlarged RV Volumes and Reduced RV Function
3.3. Intra- and Interobserver Variability
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konstam, M.A.; Kiernan, M.S.; Bernstein, D.; Bozkurt, B.; Jacob, M.; Kapur, N.K.; Kociol, R.D.; Lewis, E.F.; Mehra, M.R.; Pagani, F.D.; et al. American Heart Association Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; and Council on Cardiovascular Surgery and Anesthesia. Evaluation and Management of Right-Sided Heart Failure: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e578–e622. [Google Scholar] [PubMed]
- Helbing, W.A. Right ventricular function: The comeback of echocardiography? Eur. J. Echocardiogr. 2004, 5, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Al Ateah, G.; Kirschfink, A.; Frick, M.; Almalla, M.; Becker, M.; Cornelissen, C.; Hoffmann, R.; Marx, N.; Altiok, E. Echocardiographic determination of right ventricular volumes and ejection fraction: Validation of a truncated cone and rhomboid pyramid formula. PLoS ONE. 2023, 18, e0290418. [Google Scholar] [CrossRef] [PubMed]
- Mertens, L.L.; Friedberg, M.K. Imaging the right ventricle—Current state of the art. Nat. Rev. Cardiol. 2010, 7, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Sinclair, M.; Tarroni, G.; Oktay, O.; Rajchl, M.; Vaillant, G.; Lee, A.M.; Aung, N.; Lukaschuk, E.; Sanghvi, M.M.; et al. Automated cardiovascular magnetic resonance image analysis with fully convolutional networks. J. Cardiovasc. Magn. Reson. 2018, 20, 65. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, S.J.; Staab, W.; Steinmetz, M.; Ritter, C.O.; Lotz, J.; Hasenfuß, G.; Schuster, A.; Kowallick, J.T. Fully automated quantification of biventricular volumes and function in cardiovascular magnetic resonance: Applicability to clinical routine settings. J. Cardiovasc. Magn. Reson. 2019, 21, 24. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Patel, H.; Miller, T.; Ameyaw, K.; Narang, A.; Chauhan, D.; Anand, S.; Anyanwu, E.; Besser, S.A.; Kawaji, K.; et al. AI Based CMR Assessment of Biventricular Function: Clinical Significance of Intervendor Variability and Measurement Errors. JACC Cardiovasc. Imaging 2022, 15, 413–427. [Google Scholar] [CrossRef] [PubMed]
- Kawel-Boehm, N.; Hetzel, S.J.; Ambale-Venkatesh, B.; Captur, G.; Francois, C.J.; Jerosch-Herold, M.; Salerno, M.; Teague, S.D.; Valsangiacomo-Buechel, E.; Van der Geest, R.J.; et al. Reference ranges (“normal values”) for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 87. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Menger, J.; Bluemke, D.A.; Bremerich, J.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Kim, R.J.; von Knobelsdorff-Brenkenhoff, F.; Kramer, C.M.; Pennell, D.J.; et al. Standardized image interpretation and post-processing in cardiovascular magnetic resonance—2020 update: Society for Cardiovascular Magnetic Resonance (SCMR): Board of Trustees Task Force on Standardized Post-Processing. J. Cardiovasc. Magn. Reson. 2020, 22, 19. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Pan, Z.; Wang, D.; Lv, J.; Fang, J.; Xu, R.; Ding, J.; Cui, X.; Xie, X.; Wang, X.; et al. Prognostic Value of Cardiac Magnetic Resonance-Derived Right Ventricular Remodeling Parameters in Pulmonary Hypertension: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Imaging 2020, 13, e010568. [Google Scholar] [CrossRef] [PubMed]
- Purmah, Y.; Lei, L.Y.; Dykstra, S.; Mikami, Y.; Cornhill, A.; Satriano, A.; Flewitt, J.; Rivest, S.; Sandonato, R.; Seib, M.; et al. Right Ventricular Ejection Fraction for the Prediction of Major Adverse Cardiovascular and Heart Failure-Related Events: A Cardiac MRI Based Study of 7131 Patients With Known or Suspected Cardiovascular Disease. Circ. Cardiovasc. Imaging 2021, 14, e011337. [Google Scholar] [CrossRef] [PubMed]
- Papanastasiou, C.A.; Bazmpani, M.A.; Kokkinidis, D.G.; Zegkos, T.; Efthimiadis, G.; Tsapas, A.; Karvounis, H.; Ziakas, A.; Kalogeropoulos, A.P.; Kramer, C.M.; et al. The prognostic value of right ventricular ejection fraction by cardiovascular magnetic resonance in heart failure: A systematic review and meta-analysis. Int. J. Cardiol. 2022, 368, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Alfakih, K.; Plein, S.; Bloomer, T.; Jones, T.; Ridgway, J.; Sivananthan, M. Comparison of right ventricular volume measurements between axial and short axis orientation using steady-state free precession magnetic resonance imaging. J. Magn. Reson. Imaging 2003, 18, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Chauhan, D.; Patel, H.; Amir-Khalili, A.; da Silva, I.F.; Sojoudi, A.; Friedrich, S.; Singh, A.; Landeras, L.; Miller, T.; et al. Assessment of right ventricular size and function from cardiovascular magnetic resonance images using artificial intelligence. J. Cardiovasc. Magn. Reson. 2022, 24, 27. [Google Scholar] [CrossRef] [PubMed]
- Hadler, T.; Wetzl, J.; Lange, S.; Geppert, C.; Fenski, M.; Abazi, E.; Gröschel, J.; Ammann, C.; Wenson, F.; Töpper, A.; et al. Introduction of Lazy Luna an automatic software-driven multilevel comparison of ventricular function quantification in cardiovascular magnetic resonance imaging. Sci. Rep. 2022, 12, 6629. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Geva, T.; Powell, A.J.; Crawford, E.C.; Chung, T.; Colan, S.D. Evaluation of regional differences in right ventricular systolic function by acoustic quantification echocardiography and cine magnetic resonance imaging. Circulation 1998, 98, 339–345. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n = 70 |
|---|---|
| Age, years | 56 ± 15 |
| Male gender, n (%) | 49 (70) |
| NYHA class | |
| I, n (%) | 34 (49) |
| II, n (%) | 27 (39) |
| III, n (%) | 6 (9) |
| IV, n (%) | 3 (4) |
| Coronary artery disease, n | 25 (36%) |
| Pericarditis/myocarditis, n | 8 (11%) |
| Cardiomyopathy, n | 31 (44%) |
| Diabetes mellitus, n | 9 (13%) |
| Arterial hypertension, n | 28 (40%) |
| Dyslipidemia, n | 19 (27%) |
| Smoking, n | 26 (37%) |
| COPD/bronchial asthma, n | 5 (7%) |
| CMR, standard method | |
| LV-EDV, mL | 208.0 ± 101.5 |
| LV-EDV index, mL/m2 | 104.2 ± 46.5 |
| LV-ESV, mL | 127.9 ± 94.9 |
| LV-ESV index, mL/m2 | 63.9 ± 45.4 |
| LV-EF, % | 44.0 ± 16.2 |
| RV-EDV, mL | 162.6 ± 56.4 |
| RV-EDV index, mL/m2 | 81.7 ± 24.1 |
| RV-ESV, mL | 89.4 ± 50.7 |
| RV-ESV index, mL/m2 | 44.5 ± 23.2 |
| RV-EF, % | 48.4 ± 13.7 |
| RV Dd, cm | 4.2 ± 0.6 |
| RV Ds, cm | 3.5 ± 0.6 |
| RV Ld, cm | 7.7 ± 1.1 |
| RV Ls, cm | 6.5 ± 1.2 |
| Standard CMR Analysis | CPF-Based CMR Analysis | Difference | Correlation Coefficient r | |
|---|---|---|---|---|
| RV-EDV index, mL/m2 | 81.7 ± 24.1 | 86.2 ± 29.4 | −4.5 ± 19.0 | 0.765 |
| RV-ESV index, mL/m2 | 44.5 ± 23.2 | 51.5 ± 22.5 | −7.0 ± 14.4 | 0.801 |
| RV-EF, % | 48.4 ± 13.7 | 41.1 ± 13.5 | 7.2 ± 9.6 | 0.746 |
| Observer 1 | Observer 2 | ||||
|---|---|---|---|---|---|
| CPF Analysis 1 | CPF Analysis 2 | IntraobserverICC with 95%-CI | CPF Observer 2 | InterobserverICC with 95%-CI | |
| RV-EDV, mL | 171.2 ± 62.9 | 171.8 ± 64.1 | 0.9949 [0.9894–0.9976] | 184.1 ± 65.2 | 0.9650 [0.9279–0.9832] |
| RV-ESV, mL | 102.8 ± 44.8 | 101.1 ± 45.3 | 0.9959 [0.9915–0.9981] | 94.3 ± 41.8 | 0.9574 [0.9126–0.9795] |
| RV-EF, % | 40.3 ± 13.8 | 41.7 ± 12.6 | 0.9684 [0.9348–0.9849] | 49.9 ± 11.1 | 0.7982 [0.6184–0.8986] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kirschfink, A.; Frick, M.; Al Ateah, G.; Kneizeh, K.; Alnaimi, A.; Dettori, R.; Schuett, K.; Marx, N.; Altiok, E. Evaluation of the Truncated Cone–Rhomboid Pyramid Formula for Simplified Right Ventricular Quantification: A Cardiac Magnetic Resonance Study. J. Clin. Med. 2024, 13, 2850. https://doi.org/10.3390/jcm13102850
Kirschfink A, Frick M, Al Ateah G, Kneizeh K, Alnaimi A, Dettori R, Schuett K, Marx N, Altiok E. Evaluation of the Truncated Cone–Rhomboid Pyramid Formula for Simplified Right Ventricular Quantification: A Cardiac Magnetic Resonance Study. Journal of Clinical Medicine. 2024; 13(10):2850. https://doi.org/10.3390/jcm13102850
Chicago/Turabian StyleKirschfink, Annemarie, Michael Frick, Ghazi Al Ateah, Kinan Kneizeh, Anas Alnaimi, Rosalia Dettori, Katharina Schuett, Nikolaus Marx, and Ertunc Altiok. 2024. "Evaluation of the Truncated Cone–Rhomboid Pyramid Formula for Simplified Right Ventricular Quantification: A Cardiac Magnetic Resonance Study" Journal of Clinical Medicine 13, no. 10: 2850. https://doi.org/10.3390/jcm13102850
APA StyleKirschfink, A., Frick, M., Al Ateah, G., Kneizeh, K., Alnaimi, A., Dettori, R., Schuett, K., Marx, N., & Altiok, E. (2024). Evaluation of the Truncated Cone–Rhomboid Pyramid Formula for Simplified Right Ventricular Quantification: A Cardiac Magnetic Resonance Study. Journal of Clinical Medicine, 13(10), 2850. https://doi.org/10.3390/jcm13102850