
Relationship between Image Quality and Reproducibility of Surgical Images in 3D Digital Surgery


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Video Recording Settings
2.3. Surgical Environment
2.4. Items for Consideration
- The surgical content was almost unrecognizable.
- I can barely understand what type of surgery is being performed.
- I can understand what is being performed during surgery, but I cannot perform the surgery based on the video.
- I can understand the details of the surgery sufficiently well to perform it because of the good image quality.
- The image quality was comparable to that of normal surgery and allowed standard surgical performance.
2.5. Statistical Analyses
3. Results
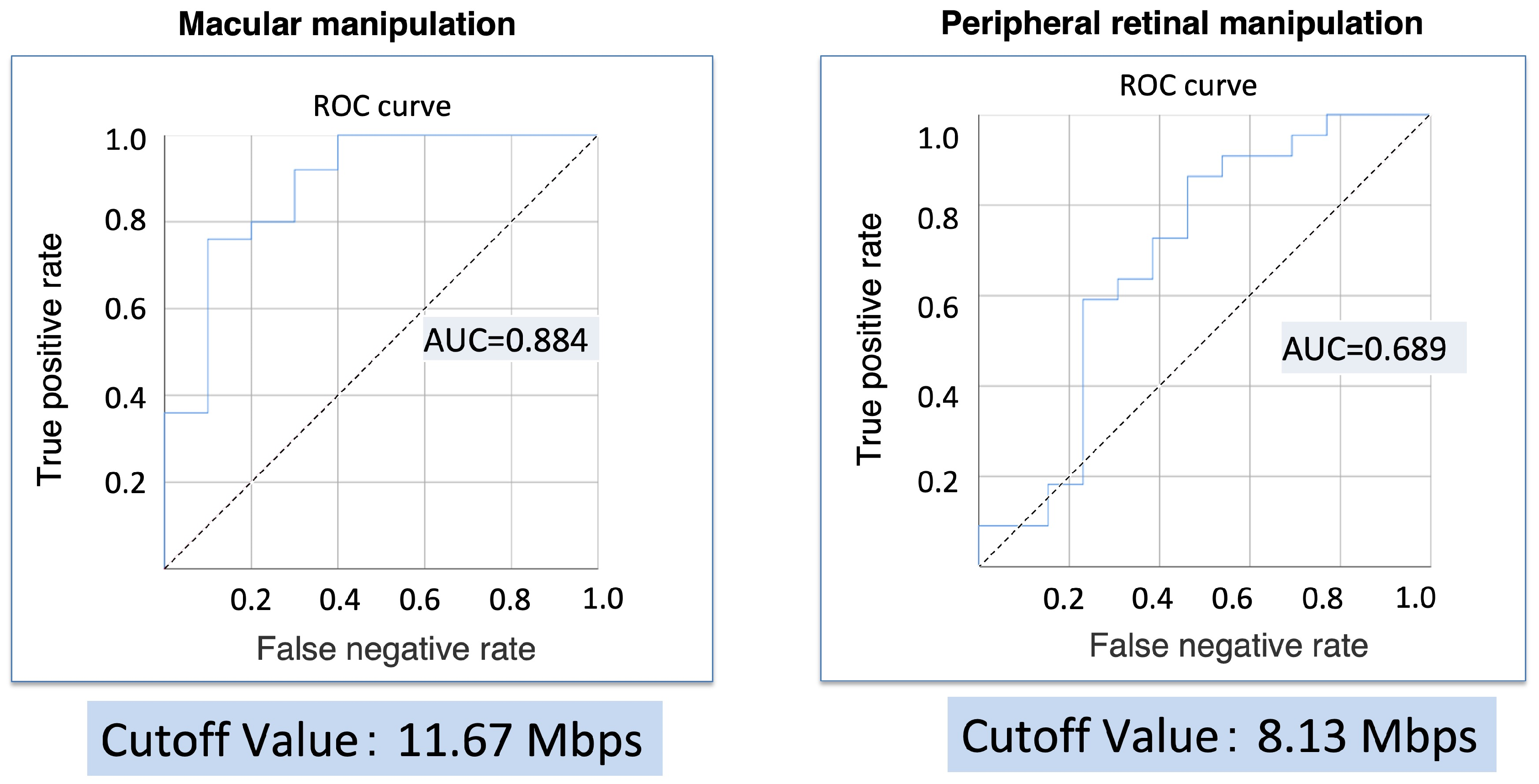
3.1. Correlation between Video Bitrate and Reproducibility Ratings for Macular Manipulation of ERM/MH Cases and Periretinal Processing of RRD Cases
3.2. Correlation between Video Bitrate and Reproducibility Ratings
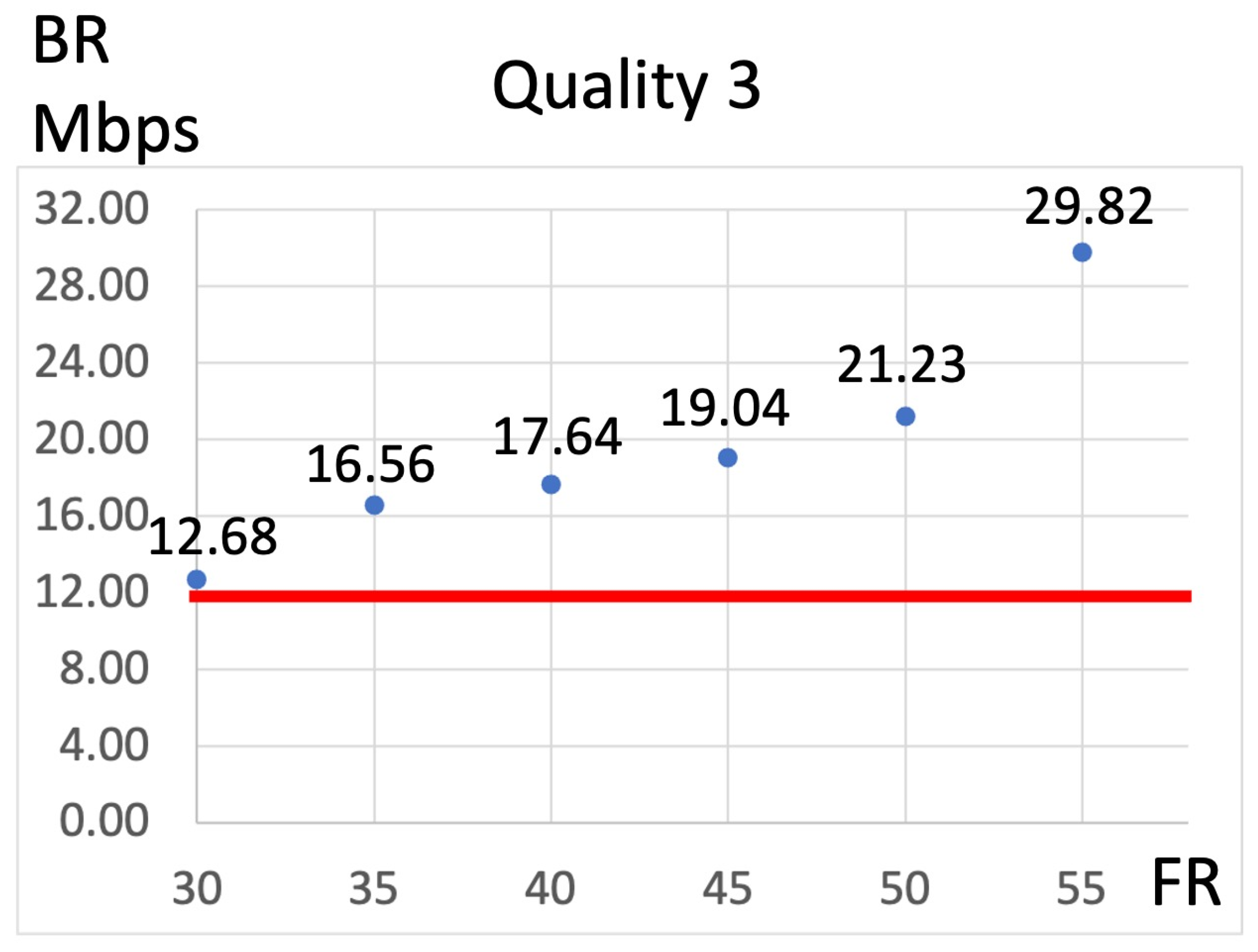
3.3. Relationship between the FR and Video Bitrate
3.4. Relationship between Q and the Video Bitrate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, A.; Hasan, N.; Kakkar, P.; Mutha, V.; Karthikeya, R.; Sundar, D.; Ravani, R. Comparison of clinical outcomes between “heads-up” 3D viewing system and conventional microscope in macular hole surgeries: A pilot study. Indian J. Ophthalmol. 2018, 66, 1816–1819. [Google Scholar] [CrossRef] [PubMed]
- Talcott, K.E.; Adam, M.K.; Sioufi, K.; Aderman, C.M.; Ali, F.S.; Mellen, P.L.; Garg, S.J.; Hsu, J.; Ho, A.C. Comparison of a three-dimensional heads-up display surgical platform with a standard operating microscope for macular surgery. Ophthalmol. Retina 2019, 3, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Melo, A.G.R.; Conti, T.F.; Hom, G.L.; Greenlee, T.E.; Cella, W.P.; Talcott, K.E.; Rachitskaya, A.; Yuan, A.; Sood, A.; Milam, R.; et al. Optimizing visualization of membranes in macular surgery with heads-up display. Ophthalmic. Surg. Lasers Imaging Retina 2020, 51, 584–587. [Google Scholar] [CrossRef] [PubMed]
- Gualino, V.; Pierne, K.; Manassero, A.; Bruneau, S.; Couturier, A.; Tadayoni, R. Comparing microscope light-associated glare and comfort between heads-up 3D digital and conventional microscopes in cataract surgery: A randomised, multicentre, single-blind, controlled trial. BMJ Open Ophthalmol. 2023, 8, e001272. [Google Scholar] [CrossRef] [PubMed]
- Nariai, Y.; Horiguchi, M.; Mizuguchi, T.; Sakurai, R.; Tanikawa, A. Comparison of microscopic illumination between a three-dimensional heads-up system and eyepiece in cataract surgery. Eur. J. Ophthalmol. 2021, 31, 1817–1821. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.J.; Waldner, D.; Huang, J.J.; Huang, J.M.; Huang, P.; Teichman, J.C.; Darvish-Zargar, M.; Gooi, P. Comparison of 3D heads-up display system with conventional surgical microscopy for minimally invasive glaucoma surgery on an artificial eye model. Can. J. Ophthalmol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Ohno, H. Utility of three-dimensional heads-up surgery in cataract and minimally invasive glaucoma surgeries. Clin. Ophthalmol. 2019, 13, 2071–2073. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Wang, H.; Fan, H.; Lin, D.; Li, W. Three-dimensional digital visualization of phacoemulsification and intraocular lens implantation. Indian J. Ophthalmol. 2019, 67, 341–343. [Google Scholar] [CrossRef]
- Weinstock, R.J.; Diakonis, V.F.; Schwartz, A.J.; Weinstock, A.J. Heads-up cataract surgery: Complication rates, surgical duration, and comparison with traditional microscopes. J. Refract. Surg. 2019, 35, 318–322. [Google Scholar] [CrossRef]
- Bedar, M.S.; Kellner, U. Digital 3D “heads-up” cataract surgery: Safety profile and comparison with the conventional microscope system. Klin. Monbl. Augenheilkd. 2022, 239, 991–995. [Google Scholar] [CrossRef]
- González-Saldivar, G.; Chow, D.R. Optimizing visual performance with digitally assisted vitreoretinal surgery. Ophthalmic. Surg. Lasers Imaging Retina 2020, 51, S15–S21. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Do, J.R.; Shin, J.P.; Park, D.H. Customized color settings of digitally assisted vitreoretinal surgery to enable use of lower dye concentrations during macular surgery. Front. Med. 2022, 8, 810070, Erratum in Front. Med. 2022, 9, 901546. https://doi.org/10.3389/fmed.2022.901546. [Google Scholar] [CrossRef] [PubMed]
- Coppola, M.; La Spina, C.; Rabiolo, A.; Querques, G.; Bandello, F. Heads-up 3D vision system for retinal detachment surgery. Int. J. Retina Vitreous 2017, 3, 46. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, K.; Watanabe, K.; Fukui, M.; Higuchi, H.; Noda, T. Quantitative evaluation of digital-image enhancement during heads-up surgery. Sci. Rep. 2019, 9, 15931. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, C.; Paulo, E.B. Heads-up surgery for vitreoretinal procedures: An experimental and clinical study. Retina 2016, 36, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.R.; Cennamo, G.; Comune, C.; Cennamo, M.; Ferrara, M.; Rombetto, L.; Cennamo, G. Evaluation of 3D heads-up vitrectomy: Outcomes of psychometric skills testing and surgeon satisfaction. Eye 2018, 32, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Gauba, V.; Tsangaris, P.; Tossounis, C.; Mitra, A.; McLean, C.; Saleh, G.M. Human reliability analysis of cataract surgery. Arch. Ophthalmol. 2008, 126, 173–177. [Google Scholar] [CrossRef]
- Hamasaki, I.; Shibata, K.; Shimizu, T.; Kono, R.; Morizane, Y.; Shiraga, F. Lights-out surgery for strabismus using a heads-up 3D vision system. Acta Med. Okayama 2019, 73, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Palácios, R.M.; Kayat, K.V.; Morel, C.; Conrath, J.; Matonti, F.; Morin, B.; Farah, M.E.; Devin, F. Clinical study on the initial experiences of French vitreoretinal surgeons with heads-up surgery. Curr. Eye Res. 2020, 45, 1265–1272. [Google Scholar] [CrossRef]
- Palácios, R.M.; de Carvalho, A.C.M.; Maia, M.; Caiado, R.R.; Camilo, D.A.G.; Farah, M.E. An experimental and clinical study on the initial experiences of Brazilian vitreoretinal surgeons with heads-up surgery. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 473–483. [Google Scholar] [CrossRef]
- Nakajima, K.; Inoue, M.; Takahashi, A.; Yoshikawa, Y.; Mizuno, M.; Koto, T.; Ishida, T.; Oshika, T. Image sharpening algorithms improve clarity of surgical field during 3D heads-up surgery. Int. J. Retina Vitreous 2023, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Imai, H.; Tetsumoto, A.; Inoue, S.; Takano, F.; Yamada, H.; Hayashida, M.; Otsuka, K.; Miki, A.; Kusuhara, S.; Nakamura, M. Intraoperative three-dimensional fluorescein angiography-guided pars plana vitrectomy for the treatment of proliferative diabetic retinopathy: The maximized utility of the digital assisted vitrectomy. Retina 2023, 43, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Imai, H.; Iwane, Y.; Kishi, M.; Sotani, Y.; Yamada, H.; Matsumiya, W.; Miki, A.; Kusuhara, S.; Nakamura, M. Color enhancement and achromatization to increase the visibility of indocyanine green-stained internal limiting membrane during digitally assisted vitreoretinal surgery. Jpn. J. Ophthalmol. 2024, 68, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.; Gomel, N.; Loewenstein, A.; Barak, A. Use of a novel beyeonics one three-dimensional head-mounted digital visualization platform in vitreoretinal surgeries. Eur. J. Ophthalmol. 2024, 34, 880–883. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | N = 129 |
| Sex (men/women) | 76/53 |
| Age (years) ± SD | 67.3 ± 12.3 |
| Disease | Eyes |
| Epiretinal membrane | 22 |
| Macular hole | 13 |
| Rhegmatogenous retinal detachment | 33 |
| Intraocular lens dislocation | 12 |
| Proliferative diabetic retinopathy | 24 |
| Others | 25 |
| Macular Manipulation | |||
|---|---|---|---|
| p Value | Odds Ratio | 95% CI | |
| Quality | 0.007 * | 3.618 | 1.423–9.198 |
| Frame rate | 0.942 | 0.995 | 0.880–1.126 |
| Peripheral Processing | |||
| p Value | Odds Ratio | 95% CI | |
| Quality | 0.025 * | 3.612 | 1.179–11.063 |
| Frame rate | 0.019 * | 1.271 | 1.040–1.554 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakanishi, Y.; Usui-Ouchi, A.; Morita, S.; Sakuma, T.; Ebihara, N. Relationship between Image Quality and Reproducibility of Surgical Images in 3D Digital Surgery. J. Clin. Med. 2024, 13, 3051. https://doi.org/10.3390/jcm13113051
Sakanishi Y, Usui-Ouchi A, Morita S, Sakuma T, Ebihara N. Relationship between Image Quality and Reproducibility of Surgical Images in 3D Digital Surgery. Journal of Clinical Medicine. 2024; 13(11):3051. https://doi.org/10.3390/jcm13113051
Chicago/Turabian StyleSakanishi, Yoshihito, Ayumi Usui-Ouchi, Shuu Morita, Toshiro Sakuma, and Nobuyuki Ebihara. 2024. "Relationship between Image Quality and Reproducibility of Surgical Images in 3D Digital Surgery" Journal of Clinical Medicine 13, no. 11: 3051. https://doi.org/10.3390/jcm13113051
APA StyleSakanishi, Y., Usui-Ouchi, A., Morita, S., Sakuma, T., & Ebihara, N. (2024). Relationship between Image Quality and Reproducibility of Surgical Images in 3D Digital Surgery. Journal of Clinical Medicine, 13(11), 3051. https://doi.org/10.3390/jcm13113051