
The Novel Impact of Augmented Reality and 3D Printing in the Diagnosis of Complex Acetabular Fractures: A Comparative Randomized Study in Orthopedic Residents

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
- -
- CT scan (1mm layer thickness, 1 mm layer interval, and a voltage of 120 kV);
- -
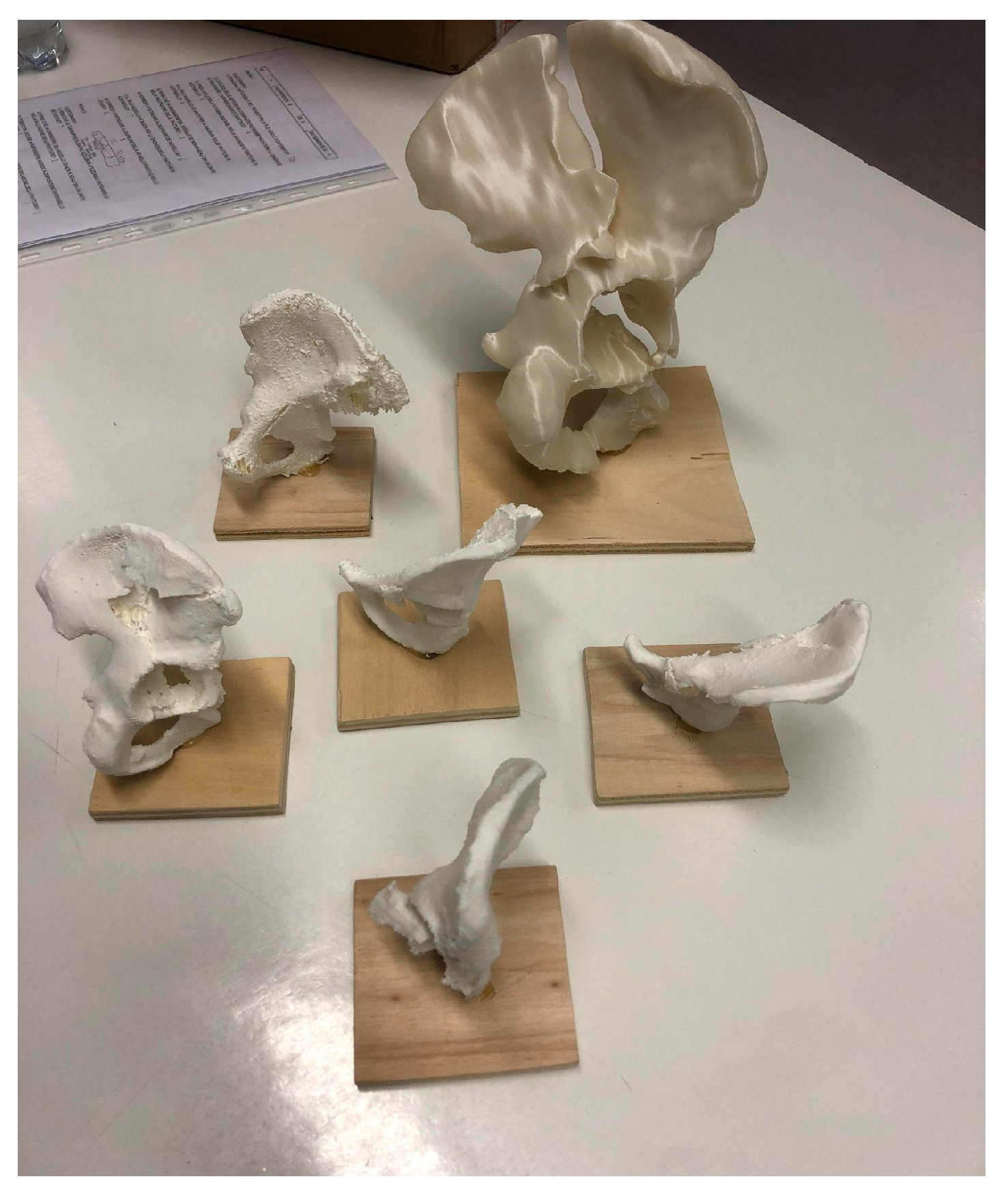
- 3DP model obtained from DICOM file using 3D planning software (Mimics-Materialise v.24.0, Meshmixer v.3.5, Cura v.5.6) with the use of segmentation applying the “region growing” function to separate the bones and soft tissues, define the fracture fragments, and build a hemipelvis digital model for each fracture that was printed in polylactic acid (PLA) (scale 1:2) using a high-precision 3D printer (Ultimaker © 2+ extended, Ultimaker, Netherland);
- -
- 3D digital rendered model (format .stl) displayed in AR with a tablet screen using Object Viewer app (by Merge EDU ©, Merge Labs Inc., San Antonio, TX, USA) Figure 1.
2.3. Methods of Assessment
- -
- The numeric fracture classification according to the Letournel classification (1: anterior wall, 2: anterior column, 3: transverse, 4: posterior wall, 5: posterior column, 6: posterior wall + posterior column, 7: anterior column + posterior hemitransverse, 8: T-shaped, 9: transverse + posterior wall, and 10: both columns);
- -
- The response time for the correct answers;
- -
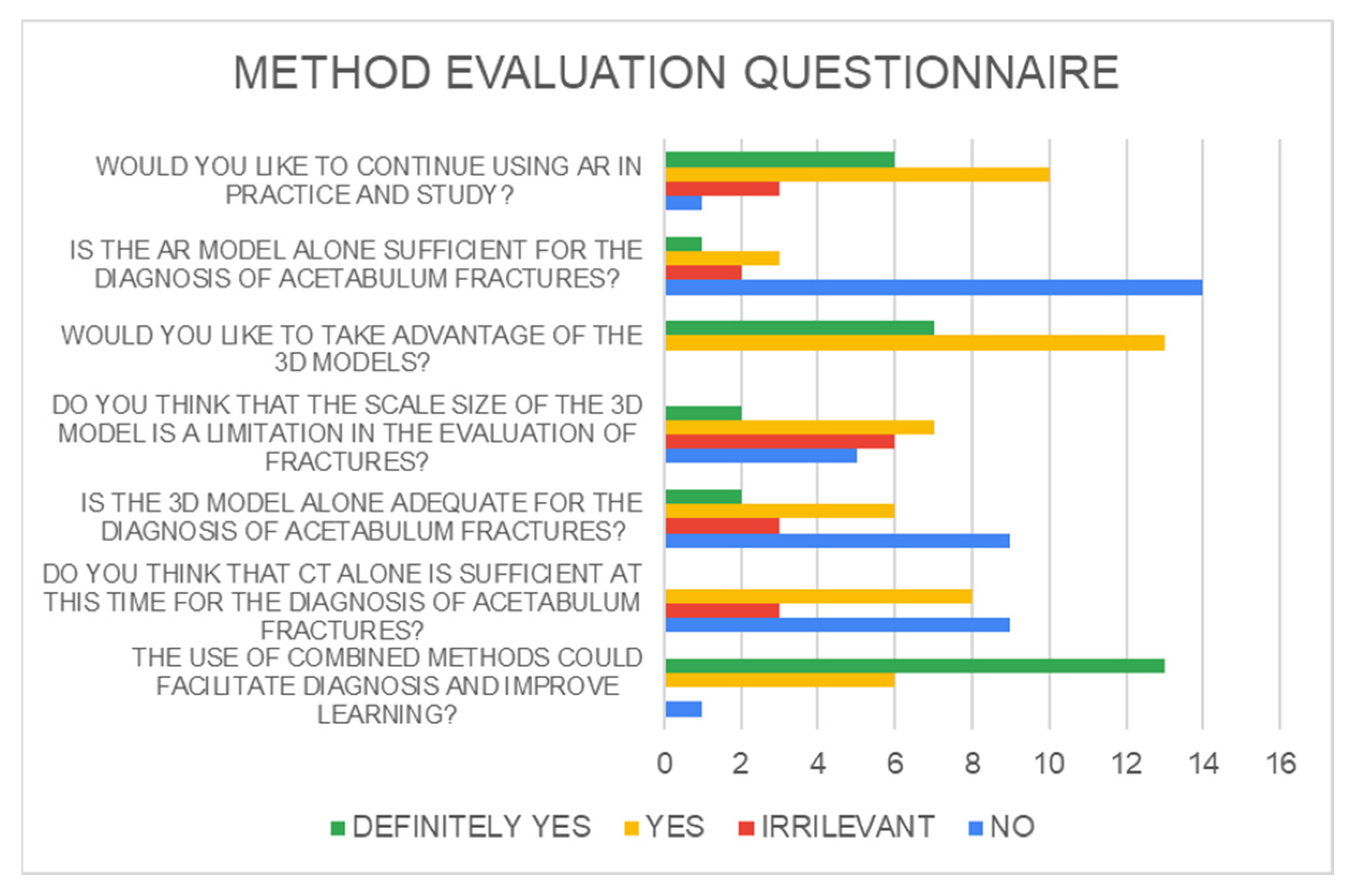
- Answers to six Likert-scale survey questions about perceived confidence in each diagnostic method.
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Judet, R.; Judet, J.; Letournel, E. Les fractures du cotyle [fractures of the acetabulum]. Acta Orthop Belg. 1964, 30, 285–293. [Google Scholar] [PubMed]
- Cimerman, M.; Kristan, A.; Jug, M.; Tomaževič, M. Fractures of the Acetabulum: From Yesterday to Tomorrow. Int. Orthop. 2021, 45, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Tile, M. Fractures of the Acetabulum. Orthop. Clin. N. Am. 1980, 11, 481–506. [Google Scholar] [CrossRef]
- Bizzotto, N.; Sandri, A.; Regis, D.; Romani, D.; Tami, I.; Magnan, B. Three-Dimensional Printing of Bone Fractures: A New Tangible Realistic Way for Preoperative Planning and Education. Surg. Innov. 2015, 22, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Lim, P.K.; Stephenson, G.S.; Keown, T.W.; Byrne, C.; Lin, C.C.; Marecek, G.S.; Scolaro, J.A. Use of 3D Printed Models in Resident Education for the Classification of Acetabulum Fractures. J. Surg. Educ. 2018, 75, 1679–1684. [Google Scholar] [CrossRef]
- Baskaran, V.; Štrkalj, G.; Štrkalj, M.; Di Ieva, A. Current Applications and Future Perspectives of the Use of 3D Printing in Anatomical Training and Neurosurgery. Front. Neuroanat. 2016, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Szary, J.; Luis, M.S.; Mikulski, S.; Patel, A.; Schulz, F.; Tretiakow, D.; Fercho, J.; Jaguszewska, K.; Frankiewicz, M.; Pawłowska, E.; et al. The Role of 3D Printing in Planning Complex Medical Procedures and Training of Medical Professionals—Cross-Sectional Multispecialty Review. Int. J. Environ. Res. Public Health 2022, 19, 3331. [Google Scholar] [CrossRef] [PubMed]
- Lebowitz, C.; Massaglia, J.; Hoffman, C.; Lucenti, L.; Dheer, S.; Rivlin, M.; Beredjiklian, P. The Accuracy of 3D Printed Carpal Bones Generated from Cadaveric Specimens. Arch. Bone Jt. Surg. 2021, 9, 432–438. [Google Scholar] [CrossRef]
- Moldovan, F.; Gligor, A.; Bataga, T. Structured Integration and Alignment Algorithm: A Tool for Personalized Surgical Treatment of Tibial Plateau Fractures. J. Pers. Med. 2021, 11, 190. [Google Scholar] [CrossRef]
- Garrett, J.; Halvorson, J.; Carroll, E.; Webb, L.X. Value of 3-D CT in Classifying Acetabular Fractures During Orthopedic Residency Training. Orthopedics 2012, 35, e615–e620. [Google Scholar] [CrossRef]
- Salta, K.; Paschalidou, K.; Tsetseri, M.; Koulougliotis, D. Shift from a Traditional to a Distance Learning Environment during the COVID-19 Pandemic: University Students’ Engagement and Interactions. Sci. Educ. 2022, 31, 93–122. [Google Scholar] [CrossRef]
- Jud, L.; Fotouhi, J.; Andronic, O.; Aichmair, A.; Osgood, G.; Navab, N.; Farshad, M. Applicability of Augmented Reality in Orthopedic Surgery—A Systematic Review. BMC Musculoskelet. Disord. 2020, 21, 103. [Google Scholar] [CrossRef]
- Verhey, J.T.; Haglin, J.M.; Verhey, E.M.; Hartigan, D.E. Virtual, Augmented, and Mixed Reality Applications in Orthopedic Surgery. Int. J. Med. Robot. 2020, 16, e2067. [Google Scholar] [CrossRef]
- Moro, C.; Štromberga, Z.; Raikos, A.; Stirling, A. The Effectiveness of Virtual and Augmented Reality in Health Sciences and Medical Anatomy: VR and AR in Health Sciences and Medical Anatomy. Am. Assoc. Anat. 2017, 10, 549–559. [Google Scholar] [CrossRef]
- Dhar, P.; Rocks, T.; Samarasinghe, R.M.; Stephenson, G.; Smith, C. Augmented Reality in Medical Education: Students’ Experiences and Learning Outcomes. Med. Educ. Online 2021, 26, 1953953. [Google Scholar] [CrossRef]
- Puglisi, G.; Montemagno, M.; Denaro, R.; Condorelli, G.; Caruso, V.F.; Vescio, A.; Testa, G.; Pavone, V. 3D-Printed Models versus CT Scan and X-Rays Imaging in the Diagnostic Evaluation of Proximal Humerus Fractures: A Triple-Blind Interobserver Reliability Comparison Study. Adv. Orthop. 2022, 2022, 5863813. [Google Scholar] [CrossRef]
- Sebaaly, A.; Riouallon, G.; Zaraa, M.; Upex, P.; Marteau, V.; Jouffroy, P. Standardized Three Dimensional Computerised Tomography Scanner Reconstructions Increase the Accuracy of Acetabular Fracture Classification. Int. Orthop. 2018, 42, 1957–1965. [Google Scholar] [CrossRef]
- Butler, B.A.; Lawton, C.D.; Hashmi, S.Z.; Stover, M.D. The Relevance of the Judet and Letournel Acetabular Fracture Classification System in the Modern Era: A Review. J. Orthop. Trauma. 2019, 33, S3–S7. [Google Scholar] [CrossRef]
- Goyal, S.; Chua, C.; Chen, Y.; Murphy, D.; O’Neill, G. Utility of 3D Printed Models as Adjunct in Acetabular Fracture Teaching for Orthopaedic Trainees. BMC Med. Educ. 2022, 22, 595. [Google Scholar] [CrossRef] [PubMed]
- Hurson, C.; Tansey, A.; O’Donnchadha, B.; Nicholson, P.; Rice, J.; McElwain, J. Rapid Prototyping in the Assessment, Classification and Preoperative Planning of Acetabular Fractures. Injury 2007, 38, 1158–1162. [Google Scholar] [CrossRef] [PubMed]
- Prevezas, N.; Antypas, G.; Louverdis, D.; Konstas, A.; Papasotiriou, A.; Sbonias, G. Proposed Guidelines for Increasing the Reliability and Validity of Letournel Classification System. Injury 2009, 40, 1098–1103. [Google Scholar] [CrossRef]
- Brandser, E.; Marsh, J.L. Acetabular Fractures: Easier Classification with a Systematic Approach. Am. J. Roentgenol. 1998, 171, 1217–1228. [Google Scholar] [CrossRef]
- Hansen, E.; Marmor, M.; Matityahu, A. Impact of a Three-Dimensional “Hands-On” Anatomic Teaching Module on Acetabular Fracture Pattern Recognition by Orthopaedic Residents. J. Bone Jt. Surg. 2012, 94, e177. [Google Scholar] [CrossRef]
- Boboc, R.G.; Băutu, E.; Gîrbacia, F.; Popovici, N.; Popovici, D.-M. Augmented Reality in Cultural Heritage: An Overview of the Last Decade of Applications. Appl. Sci. 2022, 12, 9859. [Google Scholar] [CrossRef]
- Kong, X.; Nie, L.; Zhang, H.; Wang, Z.; Ye, Q.; Tang, L.; Li, J.; Huang, W. Do Three-Dimensional Visualization and Three-Dimensional Printing Improve Hepatic Segment Anatomy Teaching? A Randomized Controlled Study. J. Surg. Educ. 2016, 73, 264–269. [Google Scholar] [CrossRef]
- Encarnacion Ramirez, M.; Ramirez Pena, I.; Barrientos Castillo, R.E.; Sufianov, A.; Goncharov, E.; Soriano Sanchez, J.A.; Colome-Hidalgo, M.; Nurmukhametov, R.; Cerda Céspedes, J.R.; Montemurro, N. Development of a 3D Printed Brain Model with Vasculature for Neurosurgical Procedure Visualisation and Training. Biomedicines 2023, 11, 330. [Google Scholar] [CrossRef]
- Zhao, X.; Zhao, H.; Zheng, W.; Gohritz, A.; Shen, Y.; Xu, W. Clinical Evaluation of Augmented Reality-Based 3D Navigation System for Brachial Plexus Tumor Surgery. World J. Surg. Onc 2024, 22, 20. [Google Scholar] [CrossRef]
- Capello, K.; Tremblay, M.; Schiebelbein, A.; Janzen, N. 3D Printed Lung Phantom for Individual Monitoring. Health Phys. 2024, 126, 292–295. [Google Scholar] [CrossRef]
- Assink, N.; Reininga, I.H.F.; ten Duis, K.; Doornberg, J.N.; Hoekstra, H.; Kraeima, J.; Witjes, M.J.H.; de Vries, J.-P.P.M.; IJpma, F.F.A. Does 3D-Assisted Surgery of Tibial Plateau Fractures Improve Surgical and Patient Outcome? A Systematic Review of 1074 Patients. Eur. J. Trauma Emerg. Surg. 2022, 48, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- Alemayehu, D.G.; Zhang, Z.; Tahir, E.; Gateau, D.; Zhang, D.-F.; Ma, X. Preoperative Planning Using 3D Printing Technology in Orthopedic Surgery. BioMed Res. Int. 2021, 2021, 7940242. [Google Scholar] [CrossRef] [PubMed]
- Ejnisman, L.; Gobbato, B.; de França Camargo, A.F.; Zancul, E. Three-Dimensional Printing in Orthopedics: From the Basics to Surgical Applications. Curr. Rev. Musculoskelet. Med. 2021, 14, 1–8. [Google Scholar] [CrossRef]
- Montgomery, S.J.; Kooner, S.S.; Ludwig, T.E.; Schneider, P.S. Impact of 3D Printed Calcaneal Models on Fracture Understanding and Confidence in Orthopedic Surgery Residents. J. Surg. Educ. 2020, 77, 472–478. [Google Scholar] [CrossRef]
- Samaila, E.M.; Negri, S.; Zardini, A.; Bizzotto, N.; Maluta, T.; Rossignoli, C.; Magnan, B. Value of Three-Dimensional Printing of Fractures in Orthopaedic Trauma Surgery. J. Int. Med. Res. 2020, 48, 300060519887299. [Google Scholar] [CrossRef]
- Keltz, E.; Keshet, D.; Peled, E.; Zvi, Y.; Norman, D.; Keren, Y. Interobserver and Intraobserver Agreement for Letournel Acetabular Fracture Classification System Using 3-Dimensional Printed Solid Models. World J. Orthop. 2021, 12, 82–93. [Google Scholar] [CrossRef]
- Beaulé, P.E.; Dorey, F.J.; Matta, J.M. Letournel Classification for Acetabular Fractures. Assessment of Interobserver and Intraobserver Reliability. J. Bone Jt. Surg. Am. 2003, 85, 1704–1709. [Google Scholar] [CrossRef]
- Negrillo-Cárdenas, J.; Jiménez-Pérez, J.-R.; Feito, F.R. The Role of Virtual and Augmented Reality in Orthopedic Trauma Surgery: From Diagnosis to Rehabilitation. Comput. Methods Programs Biomed. 2020, 191, 105407. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Accuracy Difference | Mean Difference | t-Test | p |
|---|---|---|---|
| CT vs. AR | −0.30 | −0.508 | 0.61 |
| CT vs. 3DP | 0.80 | 1.66 | 0.052 |
| 3DP vs. AR | 0.120 | 2.04 | 0.048 |
| Group | Mean | SD | t-Test | p | |
|---|---|---|---|---|---|
| CT Accuracy | JUN | 0.200 | 0.0943 | −1.964 | 0.050 |
| SEN | 0.320 | 0.169 | |||
| 3DP accuracy | JUN | 0.120 | 0.1687 | −1.800 | 0.08 |
| SEN | 0.240 | 0.126 | |||
| AR accuracy | JUN | 0.280 | 0.2150 | −0.198 | 0.84 |
| SEN | 0.300 | 0.236 | |||
| Overall accuracy | JUN | 0.178 | 0.0909 | −2.267 | 0.036 |
| SEN | 0.290 | 0.127 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montemagno, M.; Testa, G.; Panvini, F.M.C.; Puglisi, G.; Papotto, G.; Marchese, E.; Pavone, V. The Novel Impact of Augmented Reality and 3D Printing in the Diagnosis of Complex Acetabular Fractures: A Comparative Randomized Study in Orthopedic Residents. J. Clin. Med. 2024, 13, 3059. https://doi.org/10.3390/jcm13113059
Montemagno M, Testa G, Panvini FMC, Puglisi G, Papotto G, Marchese E, Pavone V. The Novel Impact of Augmented Reality and 3D Printing in the Diagnosis of Complex Acetabular Fractures: A Comparative Randomized Study in Orthopedic Residents. Journal of Clinical Medicine. 2024; 13(11):3059. https://doi.org/10.3390/jcm13113059
Chicago/Turabian StyleMontemagno, Marco, Gianluca Testa, Flora Maria Chiara Panvini, Gianluca Puglisi, Giacomo Papotto, Emanuele Marchese, and Vito Pavone. 2024. "The Novel Impact of Augmented Reality and 3D Printing in the Diagnosis of Complex Acetabular Fractures: A Comparative Randomized Study in Orthopedic Residents" Journal of Clinical Medicine 13, no. 11: 3059. https://doi.org/10.3390/jcm13113059
APA StyleMontemagno, M., Testa, G., Panvini, F. M. C., Puglisi, G., Papotto, G., Marchese, E., & Pavone, V. (2024). The Novel Impact of Augmented Reality and 3D Printing in the Diagnosis of Complex Acetabular Fractures: A Comparative Randomized Study in Orthopedic Residents. Journal of Clinical Medicine, 13(11), 3059. https://doi.org/10.3390/jcm13113059