
Clinical Outcomes after Bilateral Implantation of a Wavefront-Shaping Extended Depth of Focus (EDOF) IOL with Mini-Monovision

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Surgical Technique
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Visual Acuity
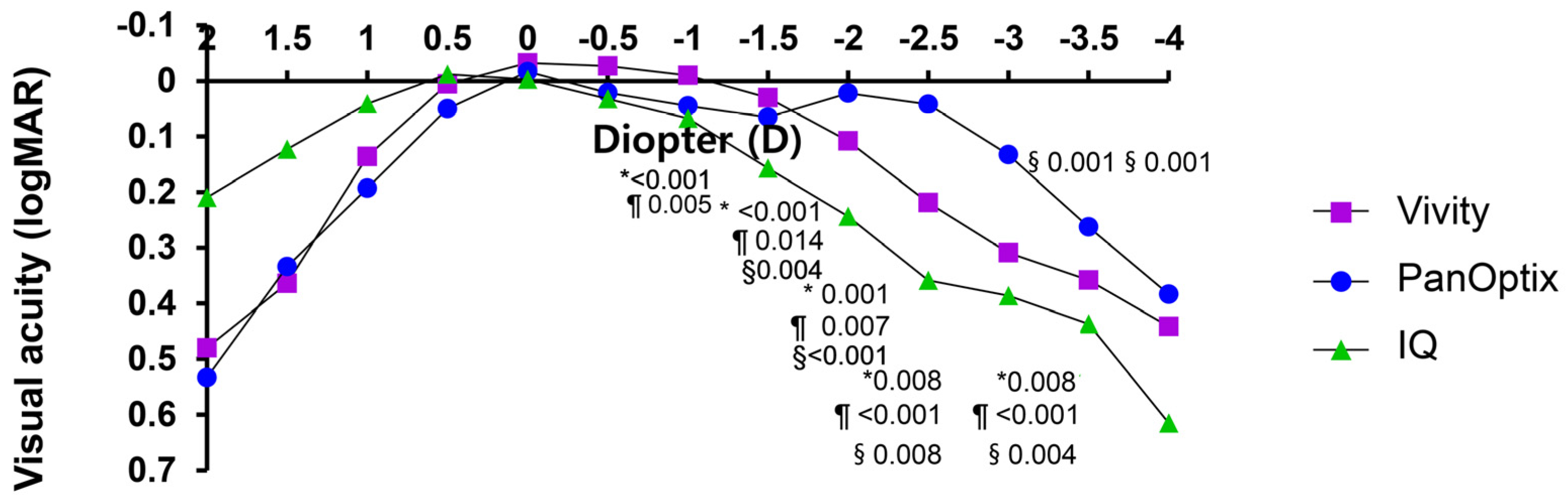
3.2. Defocus Curve
3.3. Contrast Sensitivity
3.4. Optical Quality Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations and Acronyms
| IOL | Intraocular lens |
| EDOF | Extended depth of focus |
| D | Diopter |
| IRB | Institutional Review Board |
| CDVA | Corrected distance visual acuity |
| UDVA | uncorrected distance visual acuity |
| BCVA | Best corrected visual acuity |
| Cpd | Cycles per degree |
| logMAR | Logarithm of the Minimum Angle of Resolution |
| SE | Spherical equivalent |
References
- Rodov, L.; Reitblat, O.; Levy, A.; Assia, E.I.; Kleinmann, G. Visual Outcomes and Patient Satisfaction for Trifocal, Extended Depth of Focus and Monofocal Intraocular Lenses. J. Refract. Surg. 2019, 35, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Newsom, T.H.; Potvin, R. Evaluation of Quality of Vision and Visual Outcomes with Bilateral Implantation of a Non-Diffractive Extended Vision Intraocular Lens with a Target of Slight Myopia in the Non-Dominant Eye. Clin. Ophthalmol. 2022, 16, 183–190. [Google Scholar] [CrossRef] [PubMed]
- de Vries, N.E.; Webers, C.A.; Touwslager, W.R.; Bauer, N.J.; de Brabander, J.; Berendschot, T.T.; Nuijts, R.M. Dissatisfaction after implantation of multifocal intraocular lenses. J. Cataract. Refract. Surg. 2011, 37, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Kanclerz, P.; Toto, F.; Grzybowski, A.; Alio, J.L. Extended Depth-of-Field Intraocular Lenses: An Update. Asia Pac. J. Ophthalmol. 2020, 9, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Schmid, R.; Luedtke, H.; Borkenstein, A.F. Enhanced Depth-of-focus Intraocular Lenses: Latest Wavefront-shaped Optics versus Diffractive Optics. Optom. Vis. Sci. 2022, 99, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Hovanesian, J.A.; Jones, M.; Allen, Q. The Vivity Extended Range of Vision IOL vs the PanOptix Trifocal, ReStor 2.5 Active Focus and ReStor 3.0 Multifocal Lenses: A Comparison of Patient Satisfaction, Visual Disturbances, and Spectacle Independence. Clin. Ophthalmol. 2022, 16, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, H.P.; Lane, S.; Slade, S.G.; Potvin, R.; Donnenfeld, E.D.; Solomon, K.D. Defocus Curve and Patient Satisfaction with a New Extended Depth of Focus Toric Intraocular Lens Targeted for Binocular Emmetropia or Slight Myopia in the Non-Dominant Eye. Clin. Ophthalmol. 2020, 14, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, H.P.; Lane, S.; Slade, S.; Potvin, R.; Donnenfeld, E.D.; Solomon, K.D. Extended depth-of-focus toric intraocular lens targeted for binocular emmetropia or slight myopia in the nondominant eye: Visual and refractive clinical outcomes. J. Cataract. Refract. Surg. 2019, 45, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, S.; Brar, S.; Pawar, A.; Relekar, K.J. Visual and Refractive Outcomes following Bilateral Implantation of Extended Range of Vision Intraocular Lens with Micromonovision. J. Ophthalmol. 2018, 2018, 7321794. [Google Scholar] [CrossRef]
- Cochener, B.; Concerto Study, G. Clinical outcomes of a new extended range of vision intraocular lens: International Multicenter Concerto Study. J. Cataract. Refract. Surg. 2016, 42, 1268–1275. [Google Scholar] [CrossRef]
- Cochener, B. Influence of the level of monovision on visual outcome with an extended range of vision intraocular lens. Clin. Ophthalmol. 2018, 12, 2305–2312. [Google Scholar] [CrossRef] [PubMed]
- Dolowiec-Kwapisz, A.; Piotrowska, H.; Misiuk-Hojlo, M. Evaluation of Visual and Patient-Reported Outcomes, Spectacle Dependence after Bilateral Implantation with a Non-Diffractive Extended Depth of Focus Intraocular Lens Compared to Other Intraocular Lenses. J. Clin. Med. 2022, 11, 5246. [Google Scholar] [CrossRef]
- Tomagova, N.; Elahi, S.; Vandekerckhove, K. Clinical Outcomes of a New Non-Diffractive Extended Depth-of-Focus Intraocular Lens Targeted for Mini-Monovision. Clin. Ophthalmol. 2023, 17, 981–990. [Google Scholar] [CrossRef]
- Jandewerth, T.; Biller, M.; Kohnen, T. Intolerance of a non-diffractive extended-depth-of-focus IOL with mini-monovision. Am. J. Ophthalmol. Case Rep. 2023, 29, 101770. [Google Scholar] [CrossRef] [PubMed]
- Mencucci, R.; Favuzza, E.; Caporossi, O.; Savastano, A.; Rizzo, S. Comparative analysis of visual outcomes, reading skills, contrast sensitivity, and patient satisfaction with two models of trifocal diffractive intraocular lenses and an extended range of vision intraocular lens. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 1913–1922. [Google Scholar] [CrossRef]
- Schmitz, S.; Dick, H.B.; Krummenauer, F.; Schwenn, O.; Krist, R. Contrast sensitivity and glare disability by halogen light after monofocal and multifocal lens implantation. Br. J. Ophthalmol. 2000, 84, 1109–1112. [Google Scholar] [CrossRef] [PubMed]
- McAlinden, C.; Pesudovs, K.; Moore, J.E. The development of an instrument to measure quality of vision: The Quality of Vision (QoV) questionnaire. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5537–5545. [Google Scholar] [CrossRef] [PubMed]
- Gundersen, K.G.; Potvin, R. Clinical Outcomes and Quality of Vision Associated with Bilateral Implantation of a Wavefront Shaping Presbyopia Correcting Intraocular Lens. Clin. Ophthalmol. 2021, 15, 4723–4730. [Google Scholar] [CrossRef] [PubMed]
- Sudhir, R.R.; Dey, A.; Bhattacharrya, S.; Bahulayan, A. AcrySof IQ PanOptix Intraocular Lens Versus Extended Depth of Focus Intraocular Lens and Trifocal Intraocular Lens: A Clinical Overview. Asia Pac. J. Ophthalmol. 2019, 8, 335–349. [Google Scholar] [CrossRef]
- Alio, J.L.; Plaza-Puche, A.B.; Alio Del Barrio, J.L.; Amat-Peral, P.; Ortuño, V.; Yébana, P.; Al-Shymali, O.; Vega-Estrada, A. Clinical outcomes with a diffractive trifocal intraocular lens. Eur. J. Ophthalmol. 2018, 28, 419–424. [Google Scholar] [CrossRef]
- Imburgia, A.; Gaudenzi, F.; Mularoni, K.; Mussoni, G.; Mularoni, A. Comparison of clinical performance and subjective outcomes between two diffractive trifocal intraocular lenses (IOLs) and one monofocal IOL in bilateral cataract surgery. Front. Biosci. 2021, 27, 41. [Google Scholar] [CrossRef] [PubMed]
- van Amelsfort, T.; Webers, V.S.C.; Bauer, N.J.C.; Clement, L.H.; van den Biggelaar, F.J.; Nuijts, R.M. Visual outcomes of a new nondiffractive extended depth-of-focus intraocular lens targeted for minimonovision: 3-month results of a prospective cohort study. J. Cataract. Refract. Surg. 2022, 48, 151–156. [Google Scholar] [CrossRef]
- Fernandez-Vega-Cueto, L.; Madrid-Costa, D.; Alfonso-Bartolozzi, B.; Vega, F.; Millán, M.S.; Alfonso, J.F. Optical and Clinical Outcomes of an Extended Range of Vision Intraocular Lens. J. Refract. Surg. 2022, 38, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Gundersen, K.G.; Potvin, R. The Effect of Spectacle-Induced Low Myopia in the Non-Dominant Eye on the Binocular Defocus Curve with a Non-Diffractive Extended Vision Intraocular Lens. Clin. Ophthalmol. 2021, 15, 3541–3547. [Google Scholar] [CrossRef]
- USFDA AcrySof™ IQ Vivity™ Extended Vision Intraocular Lens (IOL): Summary of Safety and Effectiveness Data. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf/P930014S126B.pdf (accessed on 1 May 2023).
- Coassin, M.; Mori, T.; Di Zazzo, A.; Poddi, M.; Sgrulletta, R.; Napolitano, P.; Bonini, S.; Orfeo, V.; Kohnen, T. Effect of minimonovision in bilateral implantation of a novel non-diffractive extended depth-of-focus intraocular lens: Defocus curves, visual outcomes, and quality of life. Eur. J. Ophthalmol. 2022, 32, 2942–2948. [Google Scholar] [CrossRef] [PubMed]
- Bala, C.; Poyales, F.; Guarro, M.; Mesa, R.R.; Mearza, A.; Varma, D.K.; Jasti, S.; Lemp-Hull, J. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J. Cataract. Refract. Surg. 2022, 48, 136–143. [Google Scholar] [CrossRef]
- Asena, L.; Kirci Dogan, I.; Oto, S.; Dursun Altinors, D. Comparison of visual performance and quality of life with a new nondiffractive EDOF intraocular lens and a trifocal intraocular lens. J. Cataract. Refract. Surg. 2023, 49, 504–511. [Google Scholar] [CrossRef]
- McCabe, C.; Berdahl, J.; Reiser, H.; Newsom, T.H.; Cibik, L.; Koch, D.; Lemp-Hull, J.; Jasti, S. Clinical outcomes in a U.S. registration study of a new EDOF intraocular lens with a nondiffractive design. J. Cataract. Refract. Surg. 2022, 48, 1297–1304. [Google Scholar] [CrossRef]
- Scheepers, M.A.; Hall, B. Randomized and double-blind comparison of clinical visual outcomes of 2 EDOF intraocular lenses. J. Cataract. Refract. Surg. 2023, 49, 354–359. [Google Scholar] [CrossRef]
- Song, M.Y.; Kang, K.H.; Lee, H.; Koh, K. A Comparative Study of Two Extended Depth of Focus Intraocular Lenses. Eye Contact Lens 2022, 48, 433–438. [Google Scholar] [CrossRef]
- Guarro, M.; Sararols, L.; Londono, G.J.; Goñi, I.; Vázquez, M.; Ruiz, S.; López, S. Visual disturbances produced after the implantation of 3 EDOF intraocular lenses vs 1 monofocal intraocular lens. J. Cataract. Refract. Surg. 2022, 48, 1354–1359. [Google Scholar] [CrossRef] [PubMed]
- Kohnen, T.; Petermann, K.; Bohm, M.; Hemkeppler, E.; Ahmad, W.; Hinzelmann, L.; Pawlowicz, K.; Jandewerth, T.; Lwowski, C. Nondiffractive wavefront-shaping extended depth-of-focus intraocular lens: Visual performance and patient-reported outcomes. J. Cataract. Refract. Surg. 2022, 48, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Liu, Y.; Liu, X.; Yuan, Z.; Luo, L.; Xia, Y.; Zeng, Y. Aberration and contrast sensitivity comparison of aspherical and monofocal and multifocal intraocular lens eyes. Clin. Exp. Ophthalmol. 2007, 35, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Rocha, K.M.; Chalita, M.R.; Souza, C.E.; Soriano, E.S.; Freitas, L.L.; Muccioli, C.; Belfort, R. Postoperative wavefront analysis and contrast sensitivity of a multifocal apodized diffractive IOL (ReSTOR) and three monofocal IOLs. J. Refract. Surg. 2005, 21, S808–S812. [Google Scholar] [CrossRef]
- Monaco, G.; Gari, M.; Di Censo, F.; Poscia, A.; Ruggi, G.; Scialdone, A. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses: Trifocal versus extended range of vision. J. Cataract. Refract. Surg. 2017, 43, 737–747. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Vivity (Group 1) | PanOptix (Group 2) | IQ Monofocal (Group 3) | p Value * | |
|---|---|---|---|---|
| Patients, N | 27 | 33 | 29 | |
| Age (year) | ||||
| Mean ± SD | 63.19 ± 3.95 | 59.55 ± 6.24 | 72.79 ± 7.45 | 0.063 |
| Range | [44, 74] | [49, 68] | [50, 86] | |
| Gender (Female), n (%) | 16 (59.3%) | 24 (72.7%) | 15 (52.7%) | |
| UDVA (logMAR) | ||||
| Mean ± SD | 0.43 ± 0.33 | 0.44 ± 0.45 | 0.47 ± 0.30 | 0.950 |
| Range | [0.10, 1.00] | [0.05, 1.40] | [0.09, 1.30] | |
| Preoperative SE (D) | 0.002 | |||
| Mean ± SD | 0.42 ± 1.53 | −0.56 ± 3.09 | 0.73 ± 1.83 | |
| Range | [−4.875, 2.75] | [−13.75, 3.5] | [−6.5, 3.5] | |
| Target (Barrett) | −0.21 | −0.06 | −0.18 | 0.054 |
| CDVA (logMAR) | ||||
| Mean ± SD | 0.13 ± 0.17 | 0.14 ± 0.14 | 0.20 ± 0.19 | 0.195 |
| Range | [0.00, 0.52] | [0.00, 0.82] | [0.00, 0.82] | |
| AXL (mm) | ||||
| Mean ± SD | 23.39 ± 0.84 | 23.82 ± 1.38 | 23.49 ± 0.87 | 0.121 |
| Range | [21.94, 28.31] | [20.91, 28.35] | [22.02, 26.71] | |
| ACD (mm) | ||||
| Mean ± SD | 3.10 ± 0.30 | 3.27 ± 0.61 | 3.04 ± 0.44 | 0.074 |
| Range | [2.49, 3.95] | [2.38, 4.18] | [2.47, 4.31] | |
| Flat K (D) | ||||
| Mean ± SD | 43.79 ± 1.27 | 43.87 ± 1.62 | 43.62 ± 1.38 | 0.634 |
| Range | [40.91, 46.72] | [40.06, 47.12] | [41.82, 46.66] | |
| Steep K (D) | ||||
| Mean ± SD | 44.38 ± 1.33 | 44.62 ± 1.75 | 44.52 ± 1.39 | 0.690 |
| Range | [41.70, 47.36] | [40.36, 48.07] | [42.81, 47.15] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Won, Y.K.; Choi, S.H.; Chung, T.-Y.; Lim, D.H. Clinical Outcomes after Bilateral Implantation of a Wavefront-Shaping Extended Depth of Focus (EDOF) IOL with Mini-Monovision. J. Clin. Med. 2024, 13, 3225. https://doi.org/10.3390/jcm13113225
Won YK, Choi SH, Chung T-Y, Lim DH. Clinical Outcomes after Bilateral Implantation of a Wavefront-Shaping Extended Depth of Focus (EDOF) IOL with Mini-Monovision. Journal of Clinical Medicine. 2024; 13(11):3225. https://doi.org/10.3390/jcm13113225
Chicago/Turabian StyleWon, Yeo Kyoung, Sung Ho Choi, Tae-Young Chung, and Dong Hui Lim. 2024. "Clinical Outcomes after Bilateral Implantation of a Wavefront-Shaping Extended Depth of Focus (EDOF) IOL with Mini-Monovision" Journal of Clinical Medicine 13, no. 11: 3225. https://doi.org/10.3390/jcm13113225