

Diagnostics of Allergy to Furry Animals—Possibilities in 2024
 ,
,  , and
, and
Abstract
1. Introduction
2. Basic Diagnostic Models in Allergology
3. Review of Commercially Available Allergy Tests Useful in the Diagnostics of Allergy to Furry Animals
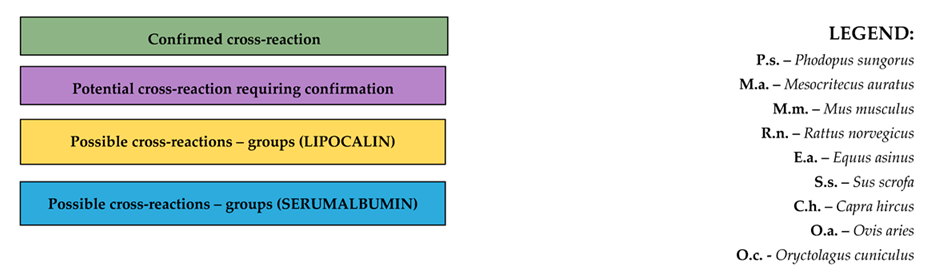
4. Cross-Reactions to Furry Animal Allergens

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Allergens | Canis familiaris | Felis catus | Cavia porcellus | P.s. | M.a. | M.m. | R.n. | Oryctolagus cuniculus | Bos domesticus | Equus caballus | E.a. | S.s. | C.h. | O.a. | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Can f 1 | Can f 2 | Can f 3 | Can f 4 | Can f 5 | Can f 6 | Can f 7 | Can f 8 | Fel d 1 | Fel d 2 | Fel d 3 | Fel d 4 | Fel d 5 | Fel d 6 | Fel d 7 | Fel d 8 | Cav p 1 | Cav p 2 | Cav p 3 | Cav p 4 | Cav p 6 | Phod s 1 | Mes a 1 | Mus m 1 | Rat n 1 | Ory c 1 | Ory c 2 | Ory c 3 | Ory c 4 | Bos d 2 | Bos d 3 | Bos d 4 | Bos d 5 | Bos d 6 | Bos d 7 | Bos d 8 | Bos d 9 | Bos d 10 | Bos d 11 | Bos d 12 | Bos d 13 | Equ c 1 | Equ c 2 | Equ c 3 | Equ c 4 | Equ c 5 | Equ c 6 | Equ a 6 | Sus s 1 | Koza | Owca | ||
| Canis familiaris | Can f 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| Can f 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Can f 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Can f 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Can f 5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Can f 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Can f 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Can f 8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Felis catus | Fel d 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| Fel d 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fel d 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fel d 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fel d 5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fel d 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fel d 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fel d 8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cavia porcellus | Cav p 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| Cav p 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cav p 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cav p 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cav p 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| P.s. | Phod s 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| M.a. | Mes a 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| M.m. | Mus m 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| R.n. | Rat n 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| O.c. | Ory c 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| Ory c 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ory c 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ory c 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos domesticus | Bos d 2 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 9 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 10 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 11 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 12 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bos d 13 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Equus caballus | Equ c 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| Equ c 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Equ c 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Equ c 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Equ c 5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Equ c 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| E.a. | Equ a 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| S.s. | Sus s 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||
| C.h. | Koza | |||||||||||||||||||||||||||||||||||||||||||||||||||
| O.a. | Owca | |||||||||||||||||||||||||||||||||||||||||||||||||||
 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
5. Are There Any Diagnostic Standards with Reference to Allergy to Furry Animals?
6. Summary
Funding
Conflicts of Interest
References
- Liccardi, G.; Emenius, G.; Merritt, A.S.; Salzillo, A.; D’Amato, M.; D’Amato, G. Direct and indirect exposure to horse: Risk for sensitization and asthma. Curr. Allergy Asthma Rep. 2012, 12, 429–437. [Google Scholar] [CrossRef] [PubMed]
- De Weck, A.L. Diagnostic approaches to allergy. Int. Arch. Allergy Immunol. 1993, 101, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Portnoy, J.M.; Amado, M. Evidence-based allergy diagnostic tests. Curr. Allergy Asthma Rep. 2006, 6, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Dramburg, S.; Hilger, C.; Santos, A.F.; de Las Vecillas, L.; Aalberse, R.C.; Acevedo, N.; Aglas, L.; Altmann, F.; Arruda, K.L.; Asero, R.; et al. EAACI Molecular Allergology User’s Guide 2.0. Pediatr. Allergy Immunol. 2023, 34, e13854. [Google Scholar] [CrossRef] [PubMed]
- Weghofer, M.; Grote, M.; Resch, Y.; Casset, A.; Kneidinger, M.; Kopec, J.; Thomas, W.R.; Fernández-Caldas, E.; Kabesch, M.; Ferrara, R.; et al. Identification of Der p 23, a peritrophin-like protein, as a new major Dermatophagoides pteronyssinus allergen associated with the peritrophic matrix of mite fecal pellets. J. Immunol. 2013, 190, 3059–3067. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Santos, N.; Bartolome, B.; Delgado, L.; Placido, J.L. Uncontrolled allergic rhinoconjunctivitis to pollen and a new oral allergy syndrome with fresh fruits: Should we take a top down or a bottom up approach? Allergy 2016, 71, 375–376. [Google Scholar]
- Gusenkov, S.; Stutz, H. Top-down and bottom-up characterization of nitrated birch pollen allergen Bet v 1a with CZE hyphenated to an Orbitrap mass spectrometer. Electrophoresis 2018, 39, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Mugford, M. Economic impact of allergy prevention. In Allergy Matters: New Approaches to Allergy Prevention and Management; Springer: Dordrecht, The Netherlands, 2006; pp. 163–169. [Google Scholar]
- Ownby, D.R. Allergy testing: In vivo versus in vitro. Pediatr. Clin. N. Am. 1988, 35, 995–1009. [Google Scholar] [CrossRef]
- Borghesan, F.; Bernardi, D.; Plebani, M. In vivo and in vitro allergy diagnostics: It’s time to reappraise the costs. Clin. Chem. Lab. Med. 2007, 45, 391–395. [Google Scholar] [CrossRef]
- Heinzerling, L.; Mari, A.; Bergmann, K.C.; Bresciani, M.; Burbach, G.; Darsow, U.; Durham, S.; Fokkens, W.; Gjomarkaj, M.; Haahtela, T.; et al. The skin prick test–European standards. Clin. Transl. Allergy 2013, 3, 3. [Google Scholar] [CrossRef]
- Butrym, I.; Płaczkowska, S.; Pawlik-Sobecka, L.; Smolińska, S. Podstawowe testy wykorzystywane w diagnostyce alergii IgE-zależnej i alergii kontaktowej. Diagn. Lab. 2017, 53, 169–174. [Google Scholar] [CrossRef]
- Available online: https://rejestrymedyczne.ezdrowie.gov.pl/api/rpl/medicinal-products/public-pl-report/get-xlsx (accessed on 12 August 2023).
- Available online: https://rejestrymedyczne.ezdrowie.gov.pl/api/rpl/medicinal-products/399/characteristic (accessed on 31 December 2023).
- Available online: https://rejestrymedyczne.ezdrowie.gov.pl/api/rpl/medicinal-products/17003/leaflet (accessed on 31 December 2023).
- Available online: https://rejestrymedyczne.ezdrowie.gov.pl/api/rpl/medicinal-products/12432/characteristic (accessed on 31 December 2023).
- Fatteh, S.; Rekkerth, D.J.; Hadley, J.A. Skin prick/puncture testing in North America: A call for standards and consistency. Allergy Asthma Clin. Immunol. 2014, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Heinzerling, L.; Bachert, C.; Papadopoulos, N.G.; Bousquet, P.J.; Burney, P.G.; Canonica, G.W.; Carlsen, K.H.; Cox, L.; Haahtela, T.; et al. Practical guide to skin prick tests in allergy to aeroallergens. Allergy 2012, 67, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Scichilone, N.; Callari, A.; Augugliaro, G.; Marchese, M.; Togias, A.; Bellia, V. The impact of age on prevalence of positive skin prick tests and specific IgE tests. Respir. Med. 2011, 105, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Bamps, D.; Berdon, K.; Hernandez, H.; Schrijvers, R.; de Hoon, J. Histamine Skin Prick Tests: From Established Diagnostic Technique to Advanced Experimental Biomarker. Skin Pharmacol. Physiol. 2023, 36, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Curin, M.; Reininger, R.; Swoboda, I.; Focke, M.; Valenta, R.; Spitzauer, S. Skin prick test extracts for dog allergy diagnosis show considerable variations regarding the content of major and minor dog allergens. Int. Arch. Allergy Immunol. 2011, 154, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Gamboa, P.M.; Sanz, M.L.; Lombardero, M.; Barber, D.; Sánchez-Monge Laguna de Rins, R.; Goikoetxea, M.J.; Antepara, I.; Ferrer, M.; Salcedo Duran, G. Component-resolved in vitro diagnosis in peach-allergic patients. J. Investig. Allergol. Clin. Immunol. 2009, 19, 13–20. [Google Scholar] [PubMed]
- Vieira, T.; Cunha, L.; Neves, E.; Falcão, H. Diagnostic usefulness of component-resolved diagnosis by skin prick tests and specific IgE to single allergen components in children with allergy to fruits and vegetables. Allergol. Immunopathol. 2014, 42, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Glück, J. Wykrywanie swoistych IgE—In vivo czy in vitro? Allergy Asthma Immunol. Res. 2012, 17, 51–56. [Google Scholar]
- Wagner, N.; Rudert, M. Sensitivity and specificity of standardised allergen extracts in skin prick test for diagnoses of IgE-mediated respiratory allergies. Clin. Transl. Allergy 2019, 9, 8. [Google Scholar] [CrossRef]
- Bignardi, D.; Comite, P.; Mori, I.; Ferrero, F.; Fontana, V.; Bruzzone, M.; Mussap, M.; Ciprandi, G. Allergen-specific IgE: Comparison between skin prick test and serum assay in real life. Allergol. Sel. 2019, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Czarnobilska, E.; Obtułowicz, K.; Wsołek, K. Type IV of hypersensitivity and its subtypes. Prz. Lek. 2007, 64, 506–508. [Google Scholar]
- Fonacier, L. A practical guide to patch testing. J. Allergy Clin. Immunol. Pract. 2015, 3, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Nečas, M. Atopy patch testing with airborne allergens. Acta Dermatovenerol. Alp. Pannonica Adriat. 2013, 22, 39–42. [Google Scholar] [PubMed]
- Fuiano, N.; Diddi, G.; Delvecchio, M.; Incorvaia, C. Diagnostic performance of the atopy patch test with inhalant allergens. J. Investig. Allergol. Clin. Immunol. 2015, 25, 34–39. [Google Scholar] [PubMed]
- Ansotegui, I.J.; Melioli, G.; Canonica, G.W.; Caraballo, L.; Villa, E.; Ebisawa, M.; Passalacqua, G.; Savi, E.; Ebo, D.; Gómez, R.M.; et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper. World Allergy Organ. J. 2020, 13, 100080. [Google Scholar] [CrossRef] [PubMed]
- Sastre, J. Molecular diagnosis in allergy. Clin. Exp. Allergy 2010, 40, 1442–1460. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, M.; Movérare, R.; Fischer, C.; Lidholm, J.; Rudengren, M.; Borres, M.P. History and Utility of Specific IgE Cutoff levels: What is the Relevance for Allergy Diagnosis? J. Allergy Clin. Immunol. Pract. 2023, 11, 3021–3029. [Google Scholar] [CrossRef]
- Producer’s Data. Available online: https://www.thermofisher.com/phadia/wo/en/product-catalog.html?solution=ImmunoCAP®ion=PL (accessed on 31 December 2023).
- Producer’s Data. Available online: https://www.polycheck.pl/oferta/alergologia (accessed on 31 December 2023).
- Producer’s Data. Available online: https://www.alextest.pl/sklad-testu/ (accessed on 31 December 2023).
- Available online: https://www.euroimmun.pl/wp-content/uploads/2023/11/Alergologiczne-testy-EUROLINE-katalog.pdf (accessed on 31 December 2023).
- Available online: https://www.abacusdx.com/media/PU_Product%20Catalogue_2024.pdf (accessed on 15 May 2024).
- Available online: https://cdn0.scrvt.com/39b415fb07de4d9656c7b516d8e2d907/1800000003516051/73f1640c25c4/160956-XC1_Allergy_Menu_OUS_Rev-01_1800000003516051.pdf (accessed on 15 May 2024).
- Available online: https://www.hycorbiomedical.com/noveosspecificigeallergens (accessed on 15 May 2024).
- Available online: https://www.euroimmun.com/documents/Indications/Allergology/IDS/LP_ML9001_I_UK_A.pdf (accessed on 15 May 2024).
- Available online: https://www.euroimmun.de/documents/Indications/Allergology/Multiplex-immunoblots/Euroline/DP_3000_I_UK_D.pdf (accessed on 15 May 2024).
- Available online: https://polycheck.de/wp-content/uploads/2016/09/181024-allergen-list.pdf (accessed on 15 May 2024).
- Available online: https://www.agnitiost.com/en/allergen.html (accessed on 15 May 2024).
- Available online: https://peramedikal.com/BackOffice/UploadImage/Product/flyer_RIDA%20qLine_EN.pdf (accessed on 15 May 2024).
- Available online: https://www.imd-berlin.de/fileadmin/user_upload/Diag_Info_Englisch/318_ALEX_allergen_list.pdf (accessed on 15 May 2024).
- Available online: http://www.woongbee.com/0NewHome/Euroimmun/allergy_BLOT.pdf (accessed on 15 May 2024).
- Santos, A.F.; Alpan, O.; Hoffmann, H.J. Basophil activation test: Mechanisms and considerations for use in clinical trials and clinical practice. Allergy 2021, 76, 2420–2432. [Google Scholar] [CrossRef] [PubMed]
- MacGlashan, D.W., Jr. Basophil activation testing. J. Allergy Clin. Immunol. 2013, 132, 777–787. [Google Scholar] [CrossRef]
- Santos, A.F.; Douiri, A.; Bécares, N.; Wu, S.Y.; Stephens, A.; Radulovic, S.; Chan, S.M.; Fox, A.T.; Du Toit, G.; Turcanu, V.; et al. Basophil activation test discriminates between allergy and tolerance in peanut-sensitized children. J. Allergy Clin. Immunol. 2014, 134, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.F.; Shreffler, W.G. Road map for the clinical application of the basophil activation test in food allergy. Clin. Exp. Allergy 2017, 47, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Eberlein, B.; Krischan, L.; Darsow, U.; Ollert, M.; Ring, J. Double positivity to bee and wasp venom: Improved diagnostic procedure by recombinant allergen–based IgE testing and basophil activation test including data about cross-reactive carbohydrate determinants. J. Allergy Clin. Immunol. 2012, 130, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Käck, U.; Asarnoj, A.; Binnmyr, J.; Grönlund, H.; Wallén, C.; Lilja, G.; van Hage, M.; Nopp, A.; Konradsen, J.R. Basophil activation testing, IgG, and IgG4 in the diagnosis of dog allergy in children with and without a dog at home. Allergy 2020, 75, 1269–1272. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.buhlmannlabs.ch/products-solutions/cellular-allergy/cast-allergens/ (accessed on 31 December 2023).
- Bahri, R.; Custovic, A.; Korosec, P.; Tsoumani, M.; Barron, M.; Wu, J.; Sayers, R.; Weimann, A.; Ruiz-Garcia, M.; Patel, N.; et al. Mast cell activation test in the diagnosis of allergic disease and anaphylaxis. J. Allergy Clin. Immunol. 2018, 142, 485–496. [Google Scholar] [CrossRef]
- Elst, J.; van der Poorten, M.L.; Van Gasse, A.L.; De Puysseleyr, L.; Hagendorens, M.M.; Faber, M.A.; Van Houdt, M.; Passante, E.; Bahri, R.; Walschot, M.; et al. Mast cell activation tests by flow cytometry: A new diagnostic asset? Clin. Exp. Allergy 2021, 51, 1482–1500. [Google Scholar] [CrossRef]
- Ukleja-Sokołowska, N.; Bartuzi, Z. ABC—Doustnych prób prowokacyjnych—Jak, gdzie, kiedy. Alergia 2020, 1, 14–18. [Google Scholar]
- Tantilipikorn, P.; Vichyanond, P.; Lacroix, J.S. Nasal provocation test: How to maximize its clinical use. Asian Pac. J. Allergy Immunol. 2010, 28, 225–231. [Google Scholar]
- Agache, I.; Bilò, M.; Braunstahl, G.J.; Delgado, L.; Demoly, P.; Eigenmann, P.; Gevaert, P.; Gomes, E.; Hellings, P.; Horak, F.; et al. In vivo diagnosis of allergic diseases—Allergen provocation tests. Allergy 2015, 70, 355–365. [Google Scholar] [CrossRef]
- Devillier, P.; Le Gall, M.; Horak, F. The allergen challenge chamber: A valuable tool for optimizing the clinical development of pollen immunotherapy. Allergy 2011, 66, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.A. Correlation between a pollen challenge chamber and a natural allergen exposure study design for eliciting ocular and nasal symptoms: Early evidence supporting a paradigm shift in drug investigation? J. Allergy Clin. Immunol. 2012, 130, 128–129. [Google Scholar] [CrossRef] [PubMed]
- Hossenbaccus, L.; Linton, S.; Ramchandani, R.; Burrows, A.G.; Ellis, A.K. Study of Cat Allergy Using Controlled Methodology-A Review of the Literature and a Call to Action. Front. Allergy 2022, 3, 828091. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Araruna, L.P.; de Miranda, D.F.; de Sousa Leite, E.; Veras, G.C.; de Abrantes, K.S.; Casimiro, G.S.; Bezerra, K.K.; Bezerra, A.M.; de Abreu, L.C. Oral Provocation Test on the Diagnosis of Cow’s Milk Protein Allergy in Children: Integrative Review. Int. Arch. Med. 2015, 8. [Google Scholar] [CrossRef]
- Safri, M.; Kurniati, N.; Munasir, Z. Elimination and provocation test in cow’s milk hypersensitive children. Paediatr. Indones. 2008, 48, 253–256. [Google Scholar]
- Davenport, J.; Smith, D. Equine hypersensitivity: The dark horse of allergy. Clin. Rev. Allergy Immunol. 2020, 59, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Patelis, A.; Borres, M.P.; Kober, A.; Berthold, M. Multiplex component-based allergen microarray in recent clinical studies. Clin. Exp. Allergy 2016, 46, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Bai, G.; Sun, C.; Ma, B. Recent Progress in Antibody Epitope Prediction. Antibodies 2023, 12, 52. [Google Scholar] [CrossRef]
- Hemmer, W.; Sestak-Greinecker, G.; Braunsteiner, T.; Wantke, F.; Wöhrl, S. Molecular sensitization patterns in animal allergy: Relationship with clinical relevance and pet ownership. Allergy 2021, 76, 3687–3696. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, O.B.; Binnmyr, J.; Zoltowska, A.; Saarne, T.; Van Hage, M.; Grönlund, H. Characterization of the dog lipocalin allergen C an f 6: The role in cross-reactivity with cat and horse. Allergy 2012, 67, 751–757. [Google Scholar] [CrossRef]
- Özuygur Ermis, S.S.; Borres, M.P.; Basna, R.; Ekerljung, L.; Malmhäll, C.; Goksör, E.; Wennergren, G.; Rådinger, M.; Lötvall, J.; Lundbäck, B.; et al. Sensitization to molecular dog allergens in an adult population: Results from the West Sweden Asthma Study. Clin. Exp. Allergy 2023, 53, 88–104. [Google Scholar] [CrossRef]
- Blaydon, D.C.; Nitoiu, D.; Eckl, K.M.; Cabral, R.M.; Bland, P.; Hausser, I.; Van Heel, D.A.; Rajpopat, S.; Fischer, J.; Oji, V.; et al. Mutations in CSTA, encoding Cystatin A, underlie exfoliative ichthyosis and reveal a role for this protease inhibitor in cell-cell adhesion. Am. J. Hum. Genet. 2011, 89, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Moosbrugger-Martinz, V.; Jalili, A.; Schossig, A.S.; Jahn-Bassler, K.; Zschocke, J.; Schmuth, M.; Stingl, G.; Eckl, K.M.; Hennies, H.C.; Gruber, R. Epidermal barrier abnormalities in exfoliative ichthyosis with a novel homozygous loss-of-function mutation in CSTA. Br. J. Dermatol. 2015, 172, 1628–1632. [Google Scholar] [CrossRef] [PubMed]
- Roesner, L.M.; Swiontek, K.; Lentz, D.; Begemann, G.; Kienlin, P.; Hentges, F.; Ollert, M.; Werfel, T.; Hilger, C. Atopic dermatitis patients with pet dander sensitization mount IgE and T cell responses to mammalian cystatins including the human self-protein. J. Investig. Allergol. Clin. Immunol. 2021, 32, 5. [Google Scholar]
- Cunha, I.M.; Pinto, A.R.; Bartolomé, B.; Falcão, H. Food Allergy to Sheep’s Milk Proteins with Cow’s Milk Tolerance in an Adult Patient. Acta Médica Port. 2023, 36, 68–69. [Google Scholar] [CrossRef] [PubMed]
- Spitzauer, S. Allergy to mammalian proteins: At the borderline between foreign and self? Int. Arch. Allergy Immunol. 1999, 120, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, L.; Lundgren, T.; Olsson, P.; Sundberg, M.; Lidholm, J. Molecular and immunological characterization of Can f 4: A dog dander allergen cross-reactive with a 23 kDa odorant-binding protein in cow dander. Clin. Exp. Allergy 2010, 40, 1276–1287. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, L.; Lundgren, T.; Everberg, H.; Larsson, H.; Lidholm, J. Prostatic kallikrein: A new major dog allergen. J. Allergy Clin. Immunol. 2009, 123, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Popescu, F.D.; Ganea, C.S.; Panaitescu, C.; Vieru, M. Molecular diagnosis in cat allergy. World J. Methodol. 2021, 11, 46. [Google Scholar] [CrossRef] [PubMed]
- Swaisgood, H.E. Review and update of casein chemistry. J. Dairy Sci. 1993, 76, 3054–3061. [Google Scholar] [CrossRef]
- Nascimento, L.G.; Casanova, F.; Silva, N.F.; de Carvalho Teixeira, A.V.; de Carvalho, A.F. Casein-based hydrogels: A mini-review. Food Chem. 2020, 314, 126063. [Google Scholar] [CrossRef]
- Smith, W.; O’Neil, S.E.; Hales, B.J.; Chai, T.L.; Hazell, L.A.; Tanyaratsrisakul, S.; Piboonpocanum, S.; Thomas, W.R. Two newly identified cat allergens: The von Ebner gland protein Fel d 7 and the latherin-like protein Fel d 8. Int. Arch. Allergy Immunol. 2011, 156, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Hilger, C.; Kuehn, A.; Hentges, F. Animal lipocalin allergens. Curr. Allergy Asthma Rep. 2012, 12, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Hilger, C.; Kohnen, M.; Grigioni, F.; Lehners, C.; Hentges, F. Allergic cross-reactions between cat and pig serum albumin: Study at the protein and DNA levels. Allergy 1997, 52, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann-Sommergruber, K.; de las Vecillas, L.; Dramburg, S.; Hilger, C.; Matricardi, P.; Santos, A.F. Molecular Allergology User’s Guide 2.0. Cow’s milk allergy. EAACI 2022, 34, 285–294. [Google Scholar]
- Trzil, J.E. Feline Asthma: Diagnostic and Treatment Update. Vet. Clin. N. Am. Small Anim. Pract. 2020, 50, 375–391. [Google Scholar] [CrossRef] [PubMed]
- van Hage, M.; Käck, U.; Asarnoj, A.; Konradsen, J.R. An update on the prevalence and diagnosis of cat and dog allergy—Emphasizing the role of molecular allergy diagnostics. Mol. Immunol. 2023, 157, 1–7. [Google Scholar] [CrossRef] [PubMed]




| Type of Tests | ||
|---|---|---|
| In Vitro | In Vivo | Ex Vivo |
| Total IgE (tIgE) level | Atopy patch tests (APTs) | Basophil activation test (BAT) |
| Allergen-specific IgE (sIgE) level | Skin prick tests (SPTs) | Mast cell activation test (MAT) |
| Level of IgE specific for allergen molecules (molecular diagnostics) | Provocation tests | |
| Allergen Extract | Allergopharma GmbH & Co. KG | Stallergenes S.A. | HAL Allergy B.V. |
|---|---|---|---|
| Animal-derived allergen extracts (selected) | |||
| Hamster fur | X | X | |
| Dog fur | X | X | X |
| Rabbit fur | X | X | |
| Cat fur | X | X | X |
| Mouse fur | X | ||
| Guinea-pig fur | X | X | |
| Horse fur | X | X | |
| Rat fur | X | ||
| Cow fur | X | ||
| Sheep wool | X | X | |
| Pig fur | X | ||
| Goat fur | X | X | |
| Food allergen extracts (selected) | |||
| Mutton/lamb | X | X | |
| Horsemeat | X | ||
| Beef | X | ||
| Pork | X | X | |
| Cow’s milk | X | ||
| Goat’s milk | X | ||
| Animal-derived mixture of allergen extracts | |||
| Furs I | X | ||
| Hamster | |||
| Dog | |||
| Rabbit | |||
| Cat | |||
| Guinea pig | |||
| Furs II | X | ||
| Horse | |||
| Cow | |||
| Sheep | |||
| Pig | |||
| Goat | |||
| Mixture of food allergen extracts (selected) | |||
| Meat I | X | ||
| Mutton | |||
| Beef | |||
| Pork |
| Singleplex | Multiplex | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Allergen Source (Allergen Number) | Extract/Molecule | ImmunoCAP (Thermo Scientific 1) | Immulite2000 (Siemens 2) | Noveos (HYCOR 3) | IDS (Immunodiagnostic Systems 4) | EUROLINE (Euroimmun 5) | POLYCHECK (Biocheck 6) | BioIC (AGNITIO 7) | RIDA qLine (R-Biopharm 8) | ALEX 2 (MADX 9) | ISACE112i (Thermo Scientific 1) |
| Dog (Canis familiaris) | |||||||||||
| Dog dander (E5) | EXTRACT | E | E | E | E | E | |||||
| Dog epithelium (E2) | E | E | |||||||||
| Dog dander (E5) and Dog epithelium (E2) | EXTRACT | E | E | ||||||||
| Dog urine (including Can f 5) | EXTRACT | E | |||||||||
| Can f Fel d 1-like | Secretoglobin | R | |||||||||
| Can f 1 | Lipocalin | R | N | R | N | R | R | ||||
| Can f 2 | Lipocalin | R | R | R | R | ||||||
| Can f 3 | Serum albumin | N | N | N | N | N | |||||
| Can f 4 | Lipocalin | R | R | R | |||||||
| Can f 5 | Arginine esterase, prostatic kallikrein | R | R | R | |||||||
| Can f 6 | Lipocalin | R | R | R | |||||||
| Cat (Felis domesticus) | |||||||||||
| Cat dander (E1) | EXTRACT | E | E | E | E | E | E | E | E | ||
| Fel d 1 | Uteroglobin (chain 1) | R | N | R | N | R | R | ||||
| Fel d 2 (E220) | Serum albumin | R | N | N | N | R | |||||
| Fel d 4 | Lipocalin | R | R | R | R | ||||||
| Fel d 7 | Lipocalin | R | R | ||||||||
| Guinea pig (Cavia procellus) | |||||||||||
| Guinea pig epithelium (E6) | EXTRACT | E | E | E | E | E | E | ||||
| Cav p 1 | Lipocalin | R | |||||||||
| Cav p 2 | Lipocalin | ||||||||||
| Cav p 3 | Lipocalin | ||||||||||
| Cav p 4 | Serum albumin | ||||||||||
| Cav p 6 | Lipocalin | ||||||||||
| HAMSTERS (Phodopus sungorus (Phod s), Mesocricetus auratus (Mes a), Cricetus cricetus (Cir c) | |||||||||||
| Hamster epithelium (E84) | EXTRACT | E (?) | E (Cir c) | E (?) | E (?) | E (Mes a) | |||||
| Phod s 1 | Lipocalin | R | |||||||||
| Mes a 1 | Lipocalin | ||||||||||
| Mouse (Muse musculus) | |||||||||||
| Mouse epithelium (E71) | EXTRACT | E | E | E | E | E | |||||
| Mouse urine proteins (E72) | EXTRACT | E | E | E | |||||||
| Mouse serum proteins (E76) | EXTRACT | E | E | E | |||||||
| Mus m 1 | Lipocalin and urinary prealbumin | N | R | ||||||||
| Rat (Rattus norvegicus, Rattus rattus) | |||||||||||
| Rat epithelium (E73) | EXTRACT | E | E | E | E | E | |||||
| Rat urine protein (E74) | EXTRACT | E | E | E | |||||||
| Rat serum protein (E75) | EXTRACT | E | E | E | |||||||
| Rabbit (Oryctolagus cuniculus) | |||||||||||
| Rabbit epithelium (E82) | EXTRACT | E | E | E | E | E | E | ||||
| Rabbit urine protein | E | E | |||||||||
| Rabbit serum protein | E | E | |||||||||
| Rabbit meat | E | E | E | ||||||||
| Ory c 1 | Lipocalin | R | |||||||||
| Ory c 2 | Lipocalin | R | |||||||||
| Ory c 3 | Lipophilin/Uteroglobin | R | |||||||||
| Chinchilla (Chinchilla chinchilla) | |||||||||||
| Chinchilla epithelium (E208) | EXTRACT | E | |||||||||
| Ferret (Mustela furo) | |||||||||||
| Ferret epithelium (E217) | EXTRACT | E | |||||||||
| Gerbil (Meriones unguiculatus) | |||||||||||
| Gerbil epithelium (E209) | EXTRACT | E | E | ||||||||
| Mink (Neogale vison, Mustela lutreola) | |||||||||||
| Mink epithelium (E203) | EXTRACT | E | E | ||||||||
| Cow (Bos domesticus) | |||||||||||
| Cow dander (E4) | EXTRACT | E | E | E | E | E | |||||
| Bos d 2 | Lipocalin | R | |||||||||
| Cow’s milk | EXTRACT | E | E | E | E | E | E | E | |||
| Cow’s milk whey | EXTRACT | E | |||||||||
| Cow’s whey | EXTRACT | E | |||||||||
| Boild milk | EXTRACT | E | E | ||||||||
| Milk powder | E | ||||||||||
| Bos d 2 | Lipocalin | R | |||||||||
| Bos d 4 | α-lactalbumin | N | X | N | X | N | N | X | X | N | N |
| Bos d 5 | β-lactoglobulin | N | X | N | X | N | N | X | X | N | N |
| Bos d 8 | Casein | N | X | N | X | N | N | X | N | N | |
| Beef | EXTRACT | E | E | E | E | E | E | ||||
| Bos d 6 | Serum albumin | N | N | N | X | X | N | N | |||
| Bos d LTF | Laktoferyna | N | N | N | |||||||
| Horse (Equus caballus) | |||||||||||
| Horse dander (E3) | EXTRACT | E | E | E | E | E | E | ||||
| Equine meat | EXTRACT | E | |||||||||
| Mare’s milk | EXTRACT | E | E | ||||||||
| Equ c 1 | Lipocalin | R | R | R | R | ||||||
| Equ c 2 | Lipocalin | ||||||||||
| Equ c 3 | Serum albumin | R | N | ||||||||
| Equ c 4 | Latherin | R | |||||||||
| Goat (Capra hircus) | |||||||||||
| Goat epithelium (E80) | EXTRACT | E | E | E | |||||||
| Goat’s milk | EXTRACT | E | E | E | E | E | |||||
| Sheep (Ovis spp., Ovis aries) | |||||||||||
| Ship epithelium (E81) | EXTRACT | E | E | E | E | ||||||
| Ship’s milk | EXTRACT | E | E | E | |||||||
| Sheep’s whey | EXTRACT | E | |||||||||
| Mutton/Lamb (F88) | EXTRACT | E | E | E | E | E | |||||
| Pig (Sus scrofa domesticus) | |||||||||||
| Pig epithelium (E83) | EXTRACT | E | E | E | |||||||
| Pork | EXTRACT | E | E | E | E | E | E | ||||
| Sus s 1 (E222) | Serum albumin | N | X | R | |||||||
| Camel (Camelus bactrianus, domesticus) | |||||||||||
| Camel’s milk | E | ||||||||||
| Mixes | |||||||||||
| (E1, E3, E4, E5) | EXTRACTS | Mix | Mix | Mix | |||||||
| (E1, E5, E6, E87, E88) | EXTRACTS | Mix | Mix | ||||||||
| (E6, E82, E84, E87, E88) | EXTRACTS | Mix | Mix | ||||||||
| Rat epithelium, serum and urine protein (E87) | EXTRACTS | E | Mix | Mix | |||||||
| Muse epithelium, serum and urine protein (E88) | EXTRACTS | E | Mix | Mix | |||||||
| (E4, E80, E81) | Mix | ||||||||||
| rCan f 1 nCan f 3 rCan f 5 | MOLECULES | Mix | |||||||||
| Allergens—The BAT | |
|---|---|
| BAG-E1 | Cat epithelium |
| BAG2-FELD1 | rFEL D 1, cat |
| BAG-E2 | Dog epithelium |
| BAG-F1 | Egg white |
| BAG-F75 | Egg yolk |
| BAG-F2 | Cow’s milk |
| BAG-F76 | Alpha-lactalbumin |
| BAG-F77 | Beta-lactoglobulin |
| BAG-F78 | Casein |
| BAG-F27 | Beef |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosada, T.; Lis, K.; Bartuzi, Z.; Grześk-Kaczyńska, M.; Ukleja-Sokołowska, N. Diagnostics of Allergy to Furry Animals—Possibilities in 2024. J. Clin. Med. 2024, 13, 3239. https://doi.org/10.3390/jcm13113239
Rosada T, Lis K, Bartuzi Z, Grześk-Kaczyńska M, Ukleja-Sokołowska N. Diagnostics of Allergy to Furry Animals—Possibilities in 2024. Journal of Clinical Medicine. 2024; 13(11):3239. https://doi.org/10.3390/jcm13113239
Chicago/Turabian StyleRosada, Tomasz, Kinga Lis, Zbigniew Bartuzi, Magdalena Grześk-Kaczyńska, and Natalia Ukleja-Sokołowska. 2024. "Diagnostics of Allergy to Furry Animals—Possibilities in 2024" Journal of Clinical Medicine 13, no. 11: 3239. https://doi.org/10.3390/jcm13113239
APA StyleRosada, T., Lis, K., Bartuzi, Z., Grześk-Kaczyńska, M., & Ukleja-Sokołowska, N. (2024). Diagnostics of Allergy to Furry Animals—Possibilities in 2024. Journal of Clinical Medicine, 13(11), 3239. https://doi.org/10.3390/jcm13113239