


Exploring the Effects of Local Air Pollution on Popliteal Artery Aneurysms

 , and
on behalf of the POPART Registry
, and
on behalf of the POPART Registry
Abstract
1. Introduction
2. Methods
2.1. IRB Approval
2.2. Design
2.3. Data
2.4. Analysis
3. Results
3.1. Sample Characteristics
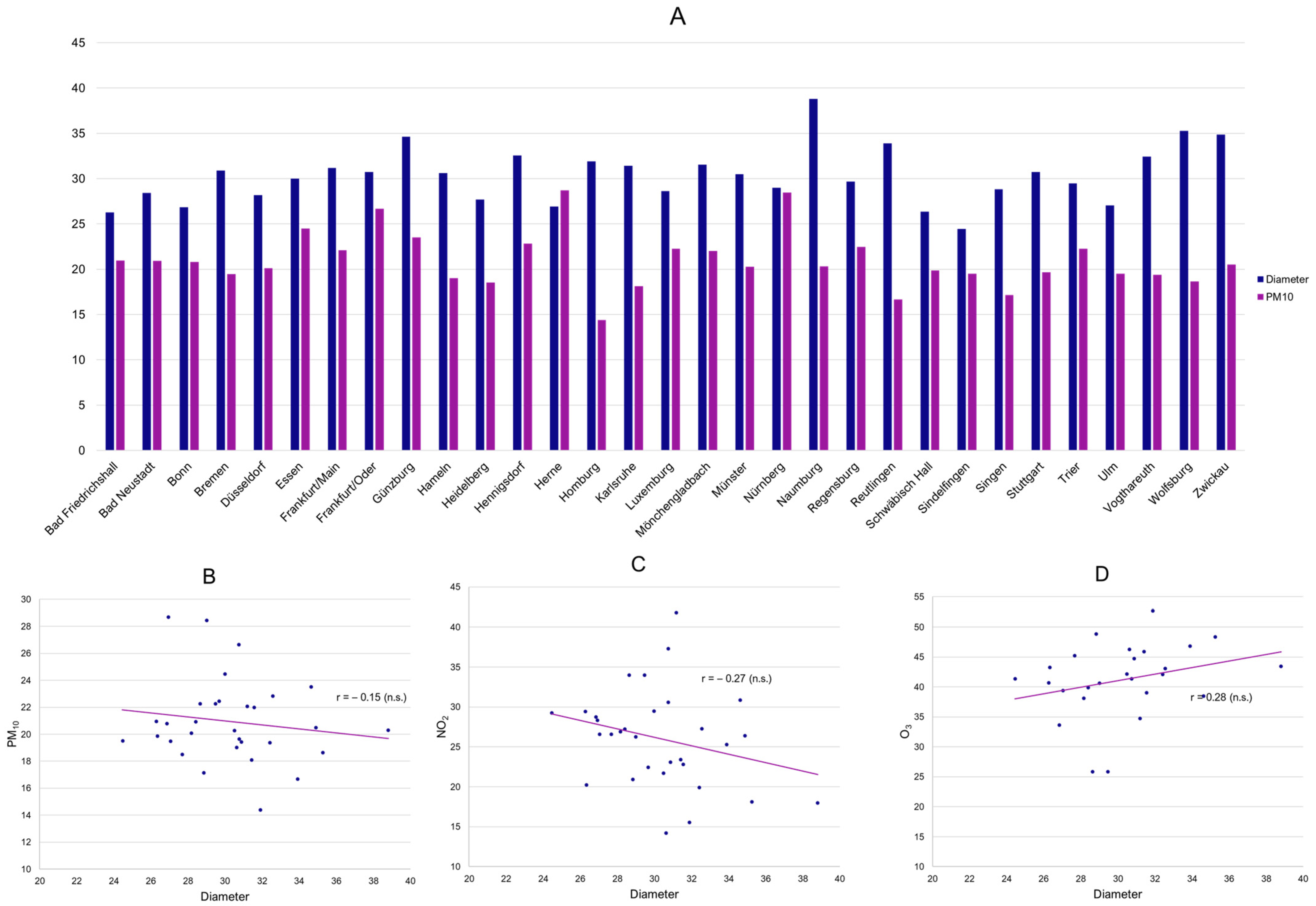
3.2. Ecological Associations
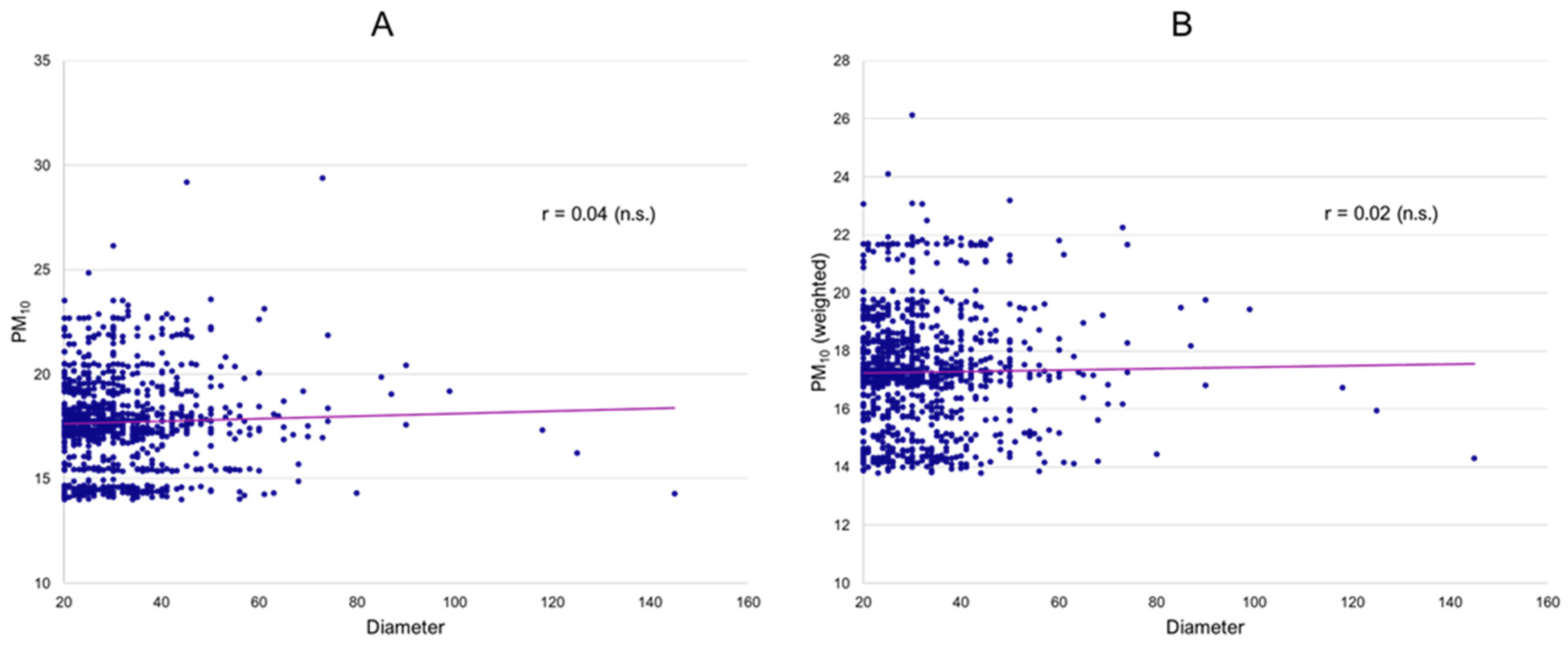
3.3. Patient-Level Analysis
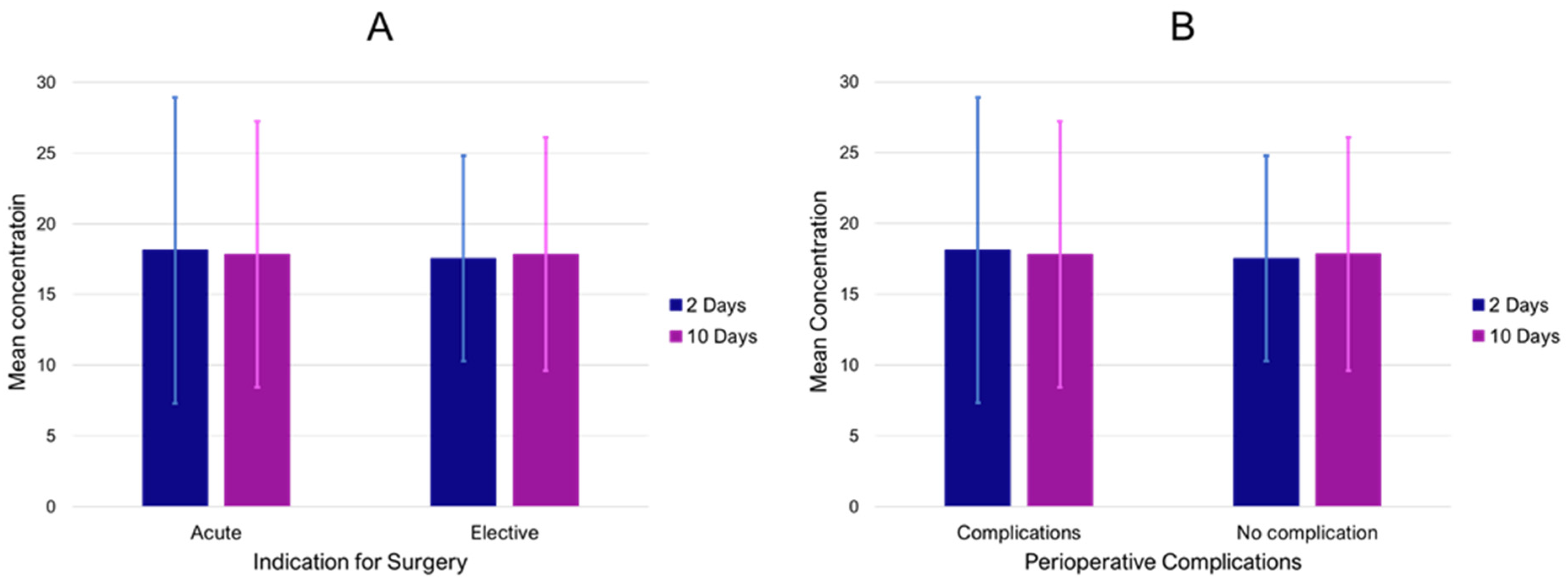
3.4. Effect of Air Pollution on Symptoms and Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brook, R.D.; Franklin, B.; Cascio, W.; Hong, Y.; Howard, G.; Lipsett, M.; Luepker, R.; Mittleman, M.; Samet, J.; Smith, S.C., Jr.; et al. Air Pollution and Cardiovascular Disease: A Statement for Healthcare Professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation 2004, 109, 2655–2671. [Google Scholar] [CrossRef] [PubMed]
- Milojevic, A.; Wilkinson, P.; Armstrong, B.; Bhaskaran, K.; Smeeth, L.; Hajat, S. Short-term effects of air pollution on a range of cardiovascular events in England and Wales: Case-crossover analysis of the MINAP database, hospital admissions and mortality. Heart 2014, 100, 1093–1098. [Google Scholar] [CrossRef]
- Thurston, G.D.; Kipen, H.; Annesi-Maesano, I.; Balmes, J.; Brook, R.D.; Cromar, K.; De Matteis, S.; Forastiere, F.; Forsberg, B.; Frampton, M.W.; et al. A joint ERS/ATS policy statement: What constitutes an adverse health effect of air pollution? An analytical framework. Eur. Respir. J. 2017, 49, 1600419. [Google Scholar] [CrossRef] [PubMed]
- Verhoeven, J.I.; Allach, Y.; Vaartjes, I.C.H.; Klijn, C.J.M.; de Leeuw, F.-E. Ambient air pollution and the risk of ischaemic and haemorrhagic stroke. Lancet Planet. Health 2021, 5, e542–e552. [Google Scholar] [CrossRef]
- Lelieveld, J.; Evans, J.S.; Fnais, M.; Giannadaki, D.; Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 2015, 525, 367–371. [Google Scholar] [CrossRef]
- Lelieveld, J.; Klingmüller, K.; Pozzer, A.; Pöschl, U.; Fnais, M.; Daiber, A.; Münzel, T. Cardiovascular disease burden from ambient air pollution in Europe reassessed using novel hazard ratio functions. Eur. Heart J. 2019, 40, 1590–1596. [Google Scholar] [CrossRef]
- Spiezia, L.; Campello, E.; Bon, M.; Maggiolo, S.; Pelizzaro, E.; Simioni, P. Short-term exposure to high levels of air pollution as a risk factor for acute isolated pulmonary embolism. Thromb. Res. 2014, 134, 259–263. [Google Scholar] [CrossRef] [PubMed]
- De Miguel-Diez, J.; Blasco-Esquivias, I.; Rodriguez-Matute, C.; Bedate-Diaz, P.; Lopez-Reyes, R.; Fernandez-Capitan, C.; Garcia-Fuika, S.; Lobo-Beristain, J.L.; Garcia-Lozaga, A.; Quezada, C.A.; et al. Correlation between short-term air pollution exposure and unprovoked lung embolism. Prospective observational (Contamina-TEP Group). Thromb Res. 2020, 192, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Versaci, F.; Anticoli, S.; Pezzella, F.R.; Mangiardi, M.; Di Giosa, A.; Marchegiani, G.; Calcagno, S.; DI Pietro, R.; Frati, G.; Sciarretta, S.; et al. Impact of weather and pollution on the rate of cerebrovascular events in a large metropolitan area. Panminerva Medica 2022, 64, 17–23. [Google Scholar] [CrossRef]
- Keller, K.; Haghi, S.H.R.; Hahad, O.; Schmidtmann, I.; Chowdhury, S.; Lelieveld, J.; Muenzel, T.; Hobohm, L. Air pollution impacts on in-hospital case-fatality rate of ischemic stroke patients. Thromb. Res. 2023, 225, 116–125. [Google Scholar] [CrossRef]
- Wang, X.; Kindzierski, W.; Kaul, P. Air Pollution and Acute Myocardial Infarction Hospital Admission in Alberta, Canada: A Three-Step Procedure Case-Crossover Study. PLoS ONE 2015, 10, e0132769. [Google Scholar] [CrossRef] [PubMed]
- Weichenthal, S.; Lavigne, E.; Evans, G.; Pollitt, K.; Burnett, R. Ambient PM2.5 and Risk of Emergency Room Visits for Myocardial Infarction: Impact of Regional PM2.5 Oxidative Potential: A Case-Crossover Study. Environ. Health 2016, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Link, M.S.; Dockery, D.W. Air pollution and the triggering of cardiac arrhythmias. Curr. Opin. Cardiol. 2010, 25, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, F.; Agabiti, N. Assessing the link between air pollution and heart failure. Lancet 2013, 382, 1008–1010. [Google Scholar] [CrossRef] [PubMed]
- Xie, N.; Zou, L.; Ye, L. The effect of meteorological conditions and air pollution on the occurrence of type A and B acute aortic dissections. Int. J. Biometeorol. 2018, 62, 1607–1613. [Google Scholar] [CrossRef]
- Chen, J.; Lv, M.; Yao, W.; Chen, R.; Lai, H.; Tong, C.; Fu, W.; Zhang, W.; Wang, C. Association between fine particulate matter air pollution and acute aortic dissections: A time-series study in Shanghai, China. Chemosphere 2020, 243, 125357. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Huang, W.; Kou, B. Examining the Relationships between Air Pollutants and the Incidence of Acute Aortic Dissection with Electronic Medical Data in a Moderately Polluted Area of Northwest China. Inq. J. Health Care Organ. Provis. Financ. 2021, 58, 00469580211065691. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.D.; Adar, S.D.; Allen, R.W.; Barr, R.G.; Budoff, M.J.; Burke, G.L.; Casillas, A.M.; Cohen, M.A.; Curl, C.L.; Daviglus, M.L.; et al. Prospective Study of Particulate Air Pollution Exposures, Subclinical Atherosclerosis, and Clinical Cardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis and Air Pollution (MESA Air). Am. J. Epidemiol. 2012, 176, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.H.; Van Hee, V.C.; Bergen, S.; Szpiro, A.A.; DeRoo, L.A.; London, S.J.; Marshall, J.D.; Kaufman, J.D.; Sandler, D.P. Long-Term Air Pollution Exposure and Blood Pressure in the Sister Study. Environ. Health Perspect. 2015, 123, 951–958. [Google Scholar] [CrossRef]
- Ming, Y.; Zhou, X.; Liu, G.; Abudupataer, M.; Zhu, S.; Xiang, B.; Yin, X.; Lai, H.; Sun, Y.; Wang, C.; et al. PM2.5 exposure exacerbates mice thoracic aortic aneurysm and dissection by inducing smooth muscle cell apoptosis via the MAPK pathway. Chemosphere 2023, 313, 137500. [Google Scholar] [CrossRef]
- Ma, Y.; Li, D.; Cui, F.; Wang, J.; Tang, L.; Yang, Y.; Liu, R.; Tian, Y. Air pollutants, genetic susceptibility, and abdominal aortic aneurysm risk: A prospective study. Eur. Heart J. 2024, ehad886. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Gori, T.; Al-Kindi, S.; Deanfield, J.; Lelieveld, J.; Daiber, A.; Rajagopalan, S. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur. Heart J. 2018, 39, 3543–3550. [Google Scholar] [CrossRef] [PubMed]
- Zeka, A.; Sullivan, J.R.; Vokonas, P.S.; Sparrow, D.; Schwartz, J. Inflammatory markers and particulate air pollution: Characterizing the pathway to disease. Int. J. Epidemiol. 2006, 35, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Brauner, E.V.; Forchhammer, L.; Moller, P.; Simonsen, J.; Glasius, M.; Wahlin, P.; Raaschou-Nielsen, O.; Loft, S. Exposure to ultrafine particles from ambient air and oxidative stress-induced DNA damage. Environ. Health Perspect. 2007, 115, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Chuang, K.-J.; Chan, C.-C.; Su, T.-C.; Lee, C.-T.; Tang, C.-S. The Effect of Urban Air Pollution on Inflammation, Oxidative Stress, Coagulation, and Autonomic Dysfunction in Young Adults. Am. J. Respir. Crit. Care Med. 2007, 176, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Delfino, R.J.; Staimer, N.; Tjoa, T.; Gillen, D.L.; Polidori, A.; Arhami, M.; Kleinman, M.T.; Vaziri, N.D.; Longhurst, J.; Sioutas, C. Air Pollution Exposures and Circulating Biomarkers of Effect in a Susceptible Population: Clues to Potential Causal Component mixtures and mechanisms. Environ. Health Perspect. 2009, 117, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef]
- Prindull, G.; Ben-Ishay, Z.; Ebell, W.; Bergholz, M.; Dirk, T.; Prindull, B. CFU-F circulating in cord blood. Blut 1987, 54, 351–359. [Google Scholar] [CrossRef]
- Dawson, I.; Sie, R.B.; Van Bockel, J.H. Atherosclerotic popliteal aneurysm: Atherosclerotic Popliteal Aneurysm. Br. J. Surg. 1997, 84, 293–299. [Google Scholar] [CrossRef]
- Trickett, J.; Scott, R.; Tilney, H. Screening and management of asymptomatic popliteal aneurysms. J. Med. Screen. 2002, 9, 92–93. [Google Scholar] [CrossRef]
- Jung, G.; Leinweber, M.E.; Karl, T.; Geisbüsch, P.; Balzer, K.; Schmandra, T.; Dietrich, T.; Derwich, W.; Gray, D.; Schmitz-Rixen, T.; et al. Real-world data of popliteal artery aneurysm treatment: Analysis of the POPART registry. J. Vasc. Surg. 2022, 75, 1707–1717.e2. [Google Scholar] [CrossRef] [PubMed]
- Leinweber, M.-E.; Geisbuesch, P.; Balzer, K.; Schmandra, T.; Karl, T.; Popp, S.; Hoffmann, J.; Schmitz-Rixen, T.; Jung, G.; Oikonomou, K.; et al. Sex disparities in popliteal artery aneurysms. J. Vasc. Surg. 2024, 79, 1179–1186.e1. [Google Scholar] [CrossRef] [PubMed]
- Anderson, H.R. Health Effects of Air Pollution Episodes. In Air Pollution and Health; Elsevier: Amsterdam, The Netherlands, 1999; pp. 461–482. [Google Scholar]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.S.Z.S.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, B.; Moebus, S.; Mohlenkamp, S.; Stang, A.; Lehmann, N.; Dragano, N.; Schmermund, A.; Memmesheimer, M.; Mann, K.; Erbel, R.; et al. Residential Exposure to Traffic Is Associated with Coronary Atherosclerosis. Circulation 2007, 116, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Bozzani, A.; Sterpetti, A.V.; Arici, V.; Ragni, F.; Arbustini, E. Air Pollution and Rupture of Abdominal Aortic Aneurysms. J. Am. Coll. Cardiol. 2023, 81, E99. [Google Scholar] [CrossRef] [PubMed]
- Wawak, M.; Tekieli, Ł.; Badacz, R.; Pieniążek, P.; Maciejewski, D.; Trystuła, M.; Przewłocki, T.; Kabłak-Ziembicka, A. Clinical Characteristics and Outcomes of Aortic Arch Emergencies: Takayasu Disease, Fibromuscular Dysplasia, and Aortic Arch Pathologies: A Retrospective Study and Review of the Literature. Biomedicines 2023, 11, 2207. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Hansen, M.L.; Long, R.W.; Nielsen, K.R.; Eatough, N.L.; Wilson, W.E.; Eatough, D.J. Ambient particulate air pollution, heart rate variability, and blood markers of inflammation in a panel of elderly subjects. Environ. Health Perspect. 2004, 112, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Rückerl, R.; Ibald-Mulli, A.; Koenig, W.; Schneider, A.; Woelke, G.; Cyrys, J.; Heinrich, J.; Marder, V.; Frampton, M.; Wichmann, H.E.; et al. Air Pollution and Markers of Inflammation and Coagulation in Patients with Coronary Heart Disease. Am. J. Respir. Crit. Care Med. 2006, 173, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Garcidueñas, L.; Villarreal-Calderon, R.; Valencia-Salazar, G.; Henríquez-Roldán, C.; Gutiérrez-Castrellón, P.; Torres-Jardón, R.; Osnaya-Brizuela, N.; Romero, L.; Solt, A.; Reed, W. Systemic Inflammation, Endothelial Dysfunction, and Activation in Clinically Healthy Children Exposed to Air Pollutants. Inhal. Toxicol. 2008, 20, 499–506. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate Matter Air Pollution and Cardiovascular Disease: An Update to the Scientific Statement From the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef]
- Newby, D.E.; Mannucci, P.M.; Tell, G.S.; Baccarelli, A.; Brook, R.D.; Donaldson, K.; Forastiere, F.; Franchini, M.; Franco, O.; Graham, I.; et al. Expert position paper on air pollution and cardiovascular disease. Eur. Heart J. 2014, 36, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Baccarelli, A.; Zanobetti, A.; Martinelli, I.; Grillo, P.; Hou, L.; Giacomini, S.; Bonzini, M.; Lanzani, G.; Mannucci, P.M.; Bertazzi, P.A.; et al. Effects of exposure to air pollution on blood coagulation. J. Thromb. Haemost. 2007, 5, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Vermylen, J.; Nemmar, A.; Nemery, B.; Hoylaerts, M.F. Ambient air pollution and acute myocardial infarction. J. Thromb. Haemost. 2005, 3, 1955–1961. [Google Scholar] [CrossRef]
- Peters, A.; Fröhlich, M.; Döring, A.; Immervoll, T.; Wichmann, H.E.; Hutchinson, W.L.; Pepys, M.B.; Koenig, W. Particulate air pollution is associated with an acute phase response in men. Results from the MONICA–Augsburg Study. Eur. Heart J. 2001, 22, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Brook, J.R.; Urch, B.; Vincent, R.; Rajagopalan, S.; Silverman, F. Inhalation of fine particulate air pollution and ozone causes acute arterial vasoconstriction in healthy adults. Circulation 2002, 105, 1534–1536. [Google Scholar] [CrossRef]
- Meraz-Cruz, N.; Manzano-León, N.; Sandoval-Colin, D.E.; García de León Méndez, M.D.; Quintana-Belmares, R.; Tapia, L.S.; Osornio-Vargas, A.R.; Buxton, M.A.; O’Neill, M.S.; Vadillo-Ortega, F. Effects of PM10 Airborne Particles from Different Regions of a Megacity on In Vitro Secretion of Cytokines by a Monocyte Line during Different Seasons. Toxics 2024, 12, 149. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wang, W.; Lei, L.; Lan, Y.; Liu, Q.; Ren, L.; Wu, S. Association between short-term exposure to ambient air pollution and biomarkers of coagulation: A systematic review and meta-analysis. Environ. Res. 2022, 215, 114210. [Google Scholar] [CrossRef] [PubMed]
- Farber, A.; Angle, N.; Avgerinos, E.; Dubois, L.; Eslami, M.; Geraghty, P.; Haurani, M.; Jim, J.; Ketteler, E.; Pulli, R.; et al. The Society for Vascular Surgery clinical practice guidelines on popliteal artery aneurysms. J. Vasc. Surg. 2021, 75, 109S–120S. [Google Scholar] [CrossRef] [PubMed]
- Indoor Air Pollution to Total Inhalation Exposure STRATEX; Dictus Publishing: Chisinau, Moldova, 2011.
- Gwon, J.G.; Park, J.H.; Kim, J.S.; Seo, H.-M. Exposure to Long-Term Air Pollution and Incidence of Peripheral Arterial Disease in the General Population: A Korean National Population-Based Retrospective Cohort Study. Angiology 2022, 74, 721–727. [Google Scholar] [CrossRef]
- Yazdi, M.D.; Wang, Y.; Di, Q.; Zanobetti, A.; Schwartz, J. Long-term exposure to PM2.5 and ozone and hospital admissions of Medicare participants in the Southeast USA. Environ. Int. 2019, 130, 104879. [Google Scholar] [CrossRef]
- Cesaroni, G.; Forastiere, F.; Stafoggia, M.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; de Faire, U.; Erbel, R.; Eriksen, K.T.; et al. Long term exposure to ambient air pollution and incidence of acute coronary events: Prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ 2013, 348, f7412. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Li, Z. Mathematical modeling of plaque progression and associated microenvironment: How far from predicting the fate of atherosclerosis? Comput. Methods Programs Biomed. 2021, 211, 106435. [Google Scholar] [CrossRef] [PubMed]
- De Bont, J.; Jaganathan, S.; Dahlquist, M.; Persson, Å.; Stafoggia, M.; Ljungman, P. Ambient air pollution and cardiovascular diseases: An umbrella review of systematic reviews and meta-analyses. J. Intern. Med. 2022, 291, 779–800. [Google Scholar] [CrossRef] [PubMed]
- EU Air Quality Standards. Available online: https://environment.ec.europa.eu/topics/air/air-quality/eu-air-quality-standards_en (accessed on 11 March 2024).

{kind=link}
{kind=link}
{kind=link}
| N = 1193 | |
|---|---|
| Female:Male | 53 (4.4%):1140 (95.6%) |
| Age | 69 (62–77) |
| Left:Right | 595 (49.9%):598 (50.1%) |
| PAA diameter (mm) | 27 (21–35) |
| Runoff vessels | |
| none | 72 (6.0%) |
| 1 | 233 (19.5%) |
| 2 | 377 (31.6%) |
| 3 | 511 (42.8%) |
| Hypertension (%) | 67.4 |
| Cardiac comorbidity (%) | 36.4 |
| CKD (%) | 12.3 |
| Diabetes (%) | 17.0 |
| Concomitant AAA (%) | 32.6 |
| Smoking (%) | 32.1 |
| ALI (%) | 15.5 |
| Endovascular interventions (%) | 11.1 |
| Complications (open surgery) (%) | 16.8 |
| PAA Diameter | Runoff | |
|---|---|---|
| PM10 | 0.04 (−0.02–0.09) | 0.08 (0.02–0.13) |
| PM10 (weighted) | 0.01 (−0.04–0.07) | 0.08 (0.03–0.14) |
| NO2 | 0.00 (−0.05–0.06) | 0.08 (0.02–0.14) |
| O3 | −0.02 (−0.08–0.05) | −0.09 (−0.15–−0.02) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leinweber, M.E.; Meisenbacher, K.; Schmandra, T.; Karl, T.; Torsello, G.; Walensi, M.; Geisbuesch, P.; Schmitz-Rixen, T.; Jung, G.; Hofmann, A.G., on behalf of the POPART Registry. Exploring the Effects of Local Air Pollution on Popliteal Artery Aneurysms. J. Clin. Med. 2024, 13, 3250. https://doi.org/10.3390/jcm13113250
Leinweber ME, Meisenbacher K, Schmandra T, Karl T, Torsello G, Walensi M, Geisbuesch P, Schmitz-Rixen T, Jung G, Hofmann AG on behalf of the POPART Registry. Exploring the Effects of Local Air Pollution on Popliteal Artery Aneurysms. Journal of Clinical Medicine. 2024; 13(11):3250. https://doi.org/10.3390/jcm13113250
Chicago/Turabian StyleLeinweber, Maria Elisabeth, Katrin Meisenbacher, Thomas Schmandra, Thomas Karl, Giovanni Torsello, Mikolaj Walensi, Phillip Geisbuesch, Thomas Schmitz-Rixen, Georg Jung, and Amun Georg Hofmann on behalf of the POPART Registry. 2024. "Exploring the Effects of Local Air Pollution on Popliteal Artery Aneurysms" Journal of Clinical Medicine 13, no. 11: 3250. https://doi.org/10.3390/jcm13113250
APA StyleLeinweber, M. E., Meisenbacher, K., Schmandra, T., Karl, T., Torsello, G., Walensi, M., Geisbuesch, P., Schmitz-Rixen, T., Jung, G., & Hofmann, A. G., on behalf of the POPART Registry. (2024). Exploring the Effects of Local Air Pollution on Popliteal Artery Aneurysms. Journal of Clinical Medicine, 13(11), 3250. https://doi.org/10.3390/jcm13113250