

Surgical Treatment of Neovascular Glaucoma Secondary to Proliferative Diabetic Retinopathy in Japanese Patients without the Use of Glaucoma Drainage Devices



Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgical Techniques
2.2.1. Pars Plana Vitrectomy with Extensive Panretinal and Ciliary Photocoagulation
2.2.2. Diode Laser Trans-Scleral Cyclophotocoagulation
2.2.3. Intravitreal Bevacizumab Injection
2.2.4. Trabeculectomy with Mitomycin C
2.3. Outcomes and Statistical Analysis
3. Results
3.1. Background and Treatment History of DR Patients with NVG
3.2. Surgical Procedures and the Numbers Performed for NVG in DR Patients
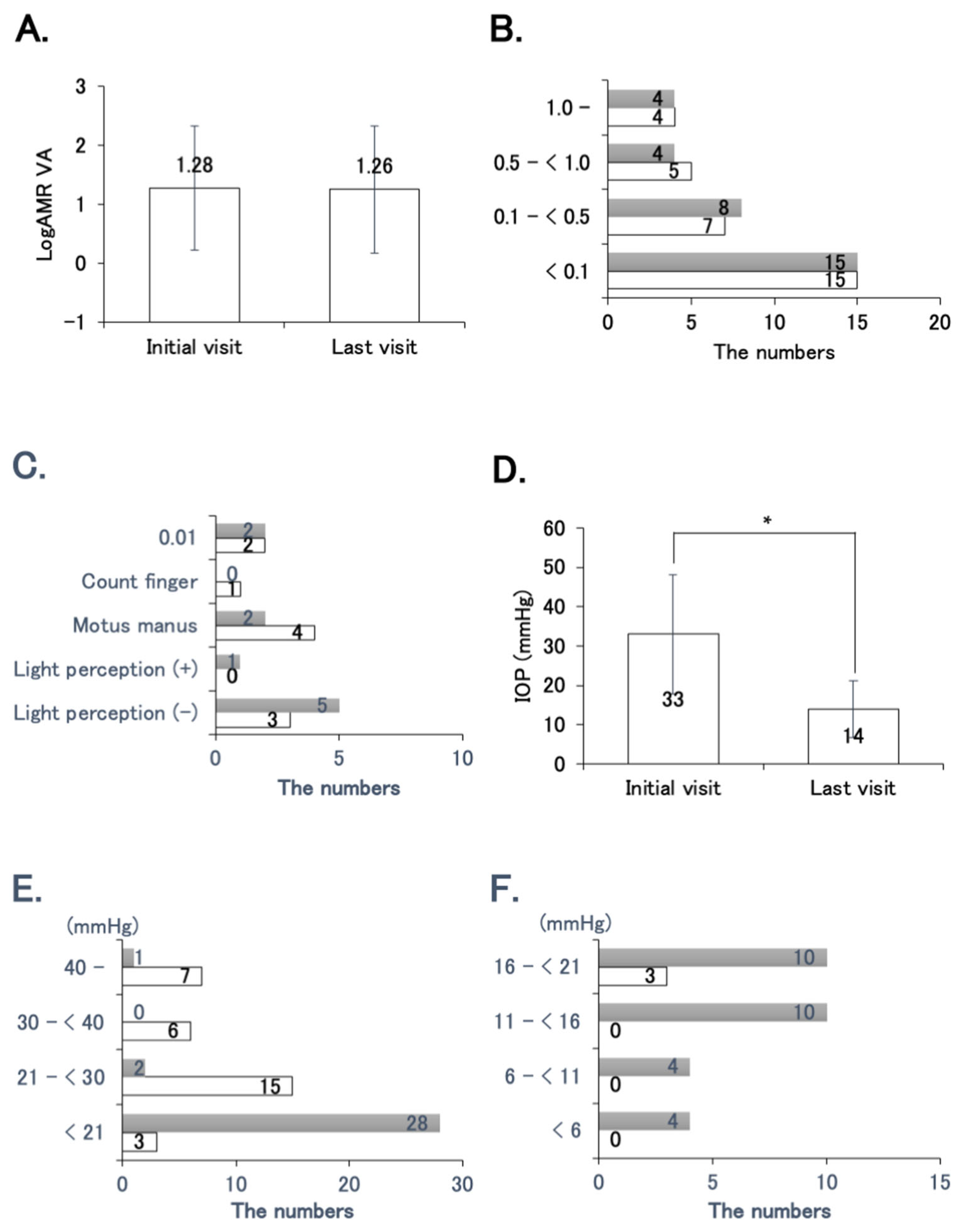
3.3. Effects of Surgical Procedures on VA and IOP in DR Patients with NVG
3.4. Comparison of TLE–MMC with Prior IVB and without IVB
3.5. Comparison between logMAR VA above 1 and 1 or below at Initial Visit
3.6. Comparison between IOP above 30 mmHg and 30 mmHg or below at Initial Visit
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tang, Y.; Shi, Y.; Fan, Z. The mechanism and therapeutic strategies for neovascular glaucoma secondary to diabetic retinopathy. Front. Endocrinol. 2023, 14, 1102361. [Google Scholar] [CrossRef]
- Sivak-Callcott, J.A.; O’Day, D.M.; Gass, J.D.; Tsai, J.C. Evidence-based recommendations for the diagnosis and treatment of neovascular glaucoma. Ophthalmology 2001, 108, 1767–1776. [Google Scholar] [CrossRef]
- John, T.; Sassani, J.W.; Eagle, R.C., Jr. The myofibroblastic component of rubeosis iridis. Ophthalmology 1983, 90, 721–728. [Google Scholar] [CrossRef]
- Tatsumi, T.; Yamamoto, S.; Uehara, J.; Sugawara, T.; Baba, T.; Inoue, M.; Hata, H.; Mitamura, Y. Panretinal photocoagulation with simultaneous cryoretinopexy or intravitreal bevacizumab for neovascular glaucoma. Graefes Arch. Clin. Exp. Ophthalmol. 2013, 251, 1355–1360. [Google Scholar] [CrossRef]
- Sato, Y.; Kojimahara, N.; Kitano, S.; Kato, S.; Ando, N.; Yamaguchi, N.; Hori, S. Multicenter randomized clinical trial of retinal photocoagulation for preproliferative diabetic retinopathy. Jpn. J. Ophthalmol. 2012, 56, 52–59. [Google Scholar] [CrossRef]
- Alkawas, A.A.; Shahien, E.A.; Hussein, A.M. Management of neovascular glaucoma with panretinal photocoagulation, intravitreal bevacizumab, and subsequent trabeculectomy with mitomycin C. J. Glaucoma 2010, 19, 622–626. [Google Scholar] [CrossRef]
- Chen, X.; Zheng, T.; Zeng, W.; Fu, X.; Wang, S.; Zeng, W.; Ke, M. Efficacy and Safety of Combined Surgeries including Intraocular Direct Cyclophotocoagulation with a 532 nm Laser to Treat Advanced Neovascular Glaucoma. J. Ophthalmol. 2021, 2021, 9938928. [Google Scholar] [CrossRef]
- Lin, S. Endoscopic cyclophotocoagulation. Br. J. Ophthalmol. 2002, 86, 1434–1438. [Google Scholar] [CrossRef]
- Iliev, M.E.; Gerber, S. Long-term outcome of trans-scleral diode laser cyclophotocoagulation in refractory glaucoma. Br. J. Ophthalmol. 2007, 91, 1631–1635. [Google Scholar] [CrossRef]
- Nabili, S.; Kirkness, C.M. Trans-scleral diode laser cyclophoto-coagulation in the treatment of diabetic neovascular glaucoma. Eye 2004, 18, 352–356. [Google Scholar] [CrossRef]
- Zemba, M.; Dumitrescu, O.M.; Vaida, F.; Dimirache, E.A.; Pistolea, I.; Stamate, A.C.; Burcea, M.; Branisteanu, D.C.; Balta, F.; Barac, I.R. Micropulse vs. continuous wave transscleral cyclophotocoagulation in neovascular glaucoma. Exp. Ther. Med. 2022, 23, 278. [Google Scholar] [CrossRef]
- Mason, J.O., 3rd; Albert, M.A., Jr.; Mays, A.; Vail, R. Regression of neovascular iris vessels by intravitreal injection of bevacizumab. Retina 2006, 26, 839–841. [Google Scholar] [CrossRef]
- Avery, R.L.; Pearlman, J.; Pieramici, D.J.; Rabena, M.D.; Castellarin, A.A.; Nasir, M.A.; Giust, M.J.; Wendel, R.; Patel, A. Intravitreal bevacizumab (Avastin) in the treatment of proliferative diabetic retinopathy. Ophthalmology 2006, 113, 1695–1705.e6. [Google Scholar] [CrossRef]
- Avery, R.L. Regression of retinal and iris neovascularization after intravitreal bevacizumab (Avastin) treatment. Retina 2006, 26, 352–354. [Google Scholar] [CrossRef]
- Silva Paula, J.; Jorge, R.; Alves Costa, R.; Rodrigues Mde, L.; Scott, I.U. Short-term results of intravitreal bevacizumab (Avastin) on anterior segment neovascularization in neovascular glaucoma. Acta Ophthalmol. Scand. 2006, 84, 556–557. [Google Scholar] [CrossRef]
- Jiang, Y.; Liang, X.; Li, X.; Tao, Y.; Wang, K. Analysis of the clinical efficacy of intravitreal bevacizumab in the treatment of iris neovascularization caused by proliferative diabetic retinopathy. Acta Ophthalmol. 2009, 87, 736–740. [Google Scholar] [CrossRef]
- Beutel, J.; Peters, S.; Luke, M.; Aisenbrey, S.; Szurman, P.; Spitzer, M.S.; Yoeruek, E.; Bevacizumab Study, G.; Grisanti, S. Bevacizumab as adjuvant for neovascular glaucoma. Acta Ophthalmol. 2010, 88, 103–109. [Google Scholar] [CrossRef]
- Ehlers, J.P.; Spirn, M.J.; Lam, A.; Sivalingam, A.; Samuel, M.A.; Tasman, W. Combination intravitreal bevacizumab/panretinal photocoagulation versus panretinal photocoagulation alone in the treatment of neovascular glaucoma. Retina 2008, 28, 696–702. [Google Scholar] [CrossRef]
- Costagliola, C.; Cipollone, U.; Rinaldi, M.; della Corte, M.; Semeraro, F.; Romano, M.R. Intravitreal bevacizumab (Avastin) injection for neovascular glaucoma: A survey on 23 cases throughout 12-month follow-up. Br. J. Clin. Pharmacol. 2008, 66, 667–673. [Google Scholar] [CrossRef]
- Yazdani, S.; Hendi, K.; Pakravan, M. Intravitreal bevacizumab (Avastin) injection for neovascular glaucoma. J. Glaucoma 2007, 16, 437–439. [Google Scholar] [CrossRef]
- Amselem, L.; Montero, J.; Diaz-Llopis, M.; Pulido, J.S.; Bakri, S.J.; Palomares, P.; Garcia-Delpech, S. Intravitreal bevacizumab (Avastin) injection in ocular ischemic syndrome. Am. J. Ophthalmol. 2007, 144, 122–124. [Google Scholar] [CrossRef]
- Oshima, Y.; Sakaguchi, H.; Gomi, F.; Tano, Y. Regression of iris neovascularization after intravitreal injection of bevacizumab in patients with proliferative diabetic retinopathy. Am. J. Ophthalmol. 2006, 142, 155–158. [Google Scholar] [CrossRef]
- Saito, Y.; Higashide, T.; Takeda, H.; Ohkubo, S.; Sugiyama, K. Beneficial effects of preoperative intravitreal bevacizumab on trabeculectomy outcomes in neovascular glaucoma. Acta Ophthalmol. 2010, 88, 96–102. [Google Scholar] [CrossRef]
- Takihara, Y.; Inatani, M.; Kawaji, T.; Fukushima, M.; Iwao, K.; Iwao, M.; Tanihara, H. Combined intravitreal bevacizumab and trabeculectomy with mitomycin C versus trabeculectomy with mitomycin C alone for neovascular glaucoma. J. Glaucoma 2011, 20, 196–201. [Google Scholar] [CrossRef]
- Kitnarong, N.; Chindasub, P.; Metheetrairut, A. Surgical outcome of intravitreal bevacizumab and filtration surgery in neovascular glaucoma. Adv. Ther. 2008, 25, 438–443. [Google Scholar] [CrossRef]
- Zhou, X.; Chen, J.; Luo, W.; Du, Y. Short-Term Outcomes of Trabeculectomy with or without Anti-VEGF in Patients With Neovascular Glaucoma: A Systematic Review and Meta-Analysis. Transl. Vis. Sci. Technol. 2023, 12, 12. [Google Scholar] [CrossRef]
- Maeda, M.; Ueki, M.; Sugiyama, T.; Kohmoto, R.; Nemoto, E.; Kojima, S.; Ikeda, T. Three-Year Outcomes of Pars Plana Ahmed and Baerveldt Glaucoma Implantations for Neovascular Glaucoma in Japanese Eyes. J. Glaucoma 2022, 31, 462–467. [Google Scholar] [CrossRef]
- LaRocca, M.C.; Smith, A.K.; Minckler, D.S.; Lin, K.Y. The Incidence of Urgent Tube Shunt Surgery for Diabetic Neovascular Glaucoma at a Tertiary Academic Medical Center. Clin. Med. Insights Endocrinol. Diabetes 2023, 16, 11795514231203865. [Google Scholar] [CrossRef]
- Lee, J.S.; Lee, Y.B.; Kim, T.W.; Park, K.H. Visual prognosis and surgical timing of Ahmed glaucoma valve implantation for neovascular glaucoma secondary to diabetic vitrectomy. BMC Ophthalmol. 2023, 23, 107. [Google Scholar] [CrossRef]
- Medert, C.M.; Sun, C.Q.; Vanner, E.; Parrish, R.K.; Wellik, S.R. The influence of etiology on surgical outcomes in neovascular glaucoma. BMC Ophthalmol. 2021, 21, 440. [Google Scholar] [CrossRef]
- Iwasaki, K.; Komori, R.; Arimura, S.; Orii, Y.; Takamura, Y.; Inatani, M. Long-term outcomes of Baerveldt glaucoma implant surgery in Japanese patients. Sci. Rep. 2023, 13, 14312. [Google Scholar] [CrossRef]
- Hayashi, T.; Mizuki, N. Ocular Manifestations in Behçet’s Disease. JMAJ 2006, 49, 260–268. [Google Scholar]
- Hayreh, S.S. Neovascular glaucoma. Prog. Retin. Eye Res. 2007, 26, 470–485. [Google Scholar] [CrossRef]
- Grover, S.; Fishman, G.A.; Anderson, R.J.; Tozatti, M.S.; Heckenlively, J.R.; Weleber, R.G.; Edwards, A.O.; Brown, J., Jr. Visual acuity impairment in patients with retinitis pigmentosa at age 45 years or older. Ophthalmology 1999, 106, 1780–1785. [Google Scholar] [CrossRef]
- Group, D.R.S.R. Photocoagulation Treatment of Proliferative Diabetic Retinopathy: Clinical Application of Diabetic Retinopathy Study (DRS) Findings, DRS Report Number 8. Ophthalmology 1981, 88, 583–600. [Google Scholar] [CrossRef]
- Vogt, A. Versuche zur intraokularen druckherabsetzung mittelst diathermieschädigung des corpus ciliare (Zyklodiathermiestichelung). Klin. Monatsbl. Augenheilkd. 1936, 97, e673. [Google Scholar]
- Fong, A.W.; Lee, G.A.; O’Rourke, P.; Thomas, R. Management of neovascular glaucoma with transscleral cyclophotocoagulation with diode laser alone versus combination transscleral cyclophotocoagulation with diode laser and intravitreal bevacizumab. Clin. Exp. Ophthalmol. 2011, 39, 318–323. [Google Scholar] [CrossRef]
- Oguri, A.; Takahashi, E.; Tomita, G.; Yamamoto, T.; Jikihara, S.; Kitazawa, Y. Transscleral cyclophotocoagulation with the diode laser for neovascular glaucoma. Ophthalmic Surg. Lasers 1998, 29, 722–727. [Google Scholar] [CrossRef]
- Ramli, N.; Htoon, H.M.; Ho, C.L.; Aung, T.; Perera, S. Risk factors for hypotony after transscleral diode cyclophotocoagulation. J. Glaucoma 2012, 21, 169–173. [Google Scholar] [CrossRef]
- Strzalkowski, P.; Strzalkowska, A.; Gobel, W.; Loewen, N.A.; Hillenkamp, J. Combined vitrectomy, near-confluent panretinal endolaser, bevacizumab and cyclophotocoagulation for neovascular glaucoma—A retrospective interventional case series. F1000Research 2020, 9, 1236. [Google Scholar] [CrossRef]
- Ramji, S.; Nagi, G.; Ansari, A.S.; Kailani, O. A systematic review and meta-analysis of randomised controlled trials in the management of neovascular glaucoma: Absence of consensus and variability in practice. Graefes Arch. Clin. Exp. Ophthalmol. 2023, 261, 477–501. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.T.; Liang, H.J.; An, M.; Wang, D.B. Efficacy and safety of intravitreal ranibizumab with panretinal photocoagulation followed by trabeculectomy compared with Ahmed glaucoma valve implantation in neovascular glaucoma. Int. J. Ophthalmol. 2017, 10, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Xu, Y.; Huang, Z.; Wang, X. Intravitreal ranibizumab injection combined trabeculectomy versus Ahmed valve surgery in the treatment of neovascular glaucoma: Assessment of efficacy and complications. BMC Ophthalmol. 2016, 16, 65. [Google Scholar] [CrossRef]
- Shchomak, Z.; Cordeiro Sousa, D.; Leal, I.; Abegão Pinto, L. Surgical treatment of neovascular glaucoma: A systematic review and meta-analysis. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 1079–1089. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| DR Patients with NVG (n = 31) | |
|---|---|
| Age (years) | 64.2 ± 12.0 * (63, 41–85) † |
| Male/Female | 22/9 |
| Follow-up periods (weeks) | 34.8 ± 36.0 |
| Clinical factors | |
| FBS (mg/dL) | 147.9 ± 38.8 (147, 82–255) |
| HbA1c (%) | 7.4 ± 1.5 (7.6, 5.0–12.6) |
| Creatinine (mg/dL) | 2.1 ± 3.0 (1.0, 0.5–12.7) |
| BUN (mg/dL) | 26.7 ± 16.6 (21.5, 10–80) |
| eGFR (mL/min/1.73 m2) | 55.1 ± 27.7 (59, 3.9–105.5) |
| Ocular conditions | |
| LogMAR VA | 1.28 ± 1.05 (1.0, 0–2.89) |
| IOP (mmHg) | 33.0 ± 15.2 (28.3, 16.5–78) |
| Treatment history in ophthalmology | |
| Anti-glaucoma eye drops | 31 (100) § |
| PRP | 25 (80.6) |
| Cataract surgery | 23 (74.2) |
| PPV | 18 (58.1) |
| DCPC | 0 (0) |
| TLE | 0 (0) |
| Number (%) | |
|---|---|
| PPV–PRCP | 24 (77.4) |
| 0 | 7 (22.6) |
| 1 | 9 (29.0) |
| 2 | 10 (32.2) |
| 3 | 3 (9.7) |
| 4 | 2 (6.5) |
| Average number of times per eye | 1.5 ± 1.2 |
| DCPC | 11 (35.5) |
| 0 | 20 (64.5) |
| 1 | 11 (35.5) |
| Average number of times per eye | 0.4 ± 0.5 |
| IVB | 13 (41.9) |
| 0 | 18 (58.1) |
| 1 | 11 (35.5) |
| 2 | 2 (6.5) |
| Average number of times per eye | 0.5 ± 0.6 |
| TLE–MMC | 27 (87.1) |
| 0 | 4 (12.9) |
| 1 | 22 (71.0) |
| 2 | 2 (6.5) |
| 3 | 2 (6.5) |
| 4 | 1 (3.2) |
| Average number of times per eye | 1.2 ± 0.9 |
| IVB (+) (n = 13) | IVB (−) (n = 14) | p Value | |
|---|---|---|---|
| Age (years) | 62.6 ± 10.4 * | 67.1 ± 12.9 | 0.2536 |
| Male/Female | 9/4 | 10/4 | 0.9006 |
| Follow-up periods (weeks) | 29.4 ± 34.1 | 29.4 ± 31.0 | 0.8841 |
| The initial presentation | |||
| LogMAR VA | 1.28 ± 1.01 (1.05, 0–2.89) † | 1.34 ± 1.10 (1.20, 0–2.89) | 0.9418 |
| IOP | 35.2 ± 12.1 (31.0, 21–60) | 33.9 ± 18.8 (27.5, 16.5–78) | 0.3438 |
| PRP | 12 (92.3) § | 11 (78.6) | 0.3154 |
| Cataract surgery | 10 (76.9) | 11 (78.6) | 0.9180 |
| PPV | 9 (69.2) | 9 (64.3) | 0.7854 |
| FBS (mg/dL) | 145.7 ± 28.1 | 152.4 ± 47.4 | 0.7709 |
| HbA1c (%) | 7.2 ± 1.1 | 7.9 ± 1.8 | 0.2637 |
| Creatinine (mg/dL) | 2.6 ± 3.5 | 2.0 ± 3.1 | 0.9806 |
| BUN (mg/dL) | 30.1 ± 15.5 | 24.5 ± 19.4 | 0.1234 |
| eGFR (mL/min/1.73 m2) | 56.7 ± 30.9 | 53.3 ± 27.1 | 0.6799 |
| The last presentation | |||
| LogMAR VA | 1.44 ± 1.06 (1.05, 0–2.89) | 1.19 ± 1.06 (0.85, −0.08–2.89) | 0.5110 |
| IOP (mmHg) | 11.4 ± 4.8 (11, 3–21) | 15.9 ± 9.1 (16, 3–42.3) | 0.0613 |
| Cataract surgery | 13 (100) | 14 (100) | 1 |
| PPV with PRCP | 1.7 ± 1.2 | 1.6 ± 1.2 | 0.8204 |
| DCPC | 0.31 ± 0.48 | 0.37 ± 0.50 | 0.7266 |
| TLE + MMC | 1.31 ± 0.85 | 1.0 ± 0.88 | 0.1978 |
| LogMAR VA > 1 (n = 15) | LogMAR VA ≤ 1 (n = 16) | p Value | |
|---|---|---|---|
| Age (years) | 62.5 ± 12.8 * | 65.8 ± 11.4 | 0.4642 |
| Male/Female | 8/7 | 14/2 | 0.0362 |
| Follow-up periods (weeks) | 34.0 ± 32.9 | 30.0 ± 33.4 | 0.6779 |
| The initial presentation | |||
| IOP | 40.5 ± 18.4 (38.0, 21–78) † | 26.0 ± 5.9 (24.3, 16.5–38) | 0.0167 |
| PRP | 11 (73.3) § | 14 (87.5) | 0.3184 |
| Cataract surgery | 10 (66.7) | 13 (81.3) | 0.3538 |
| PPV | 8 (53.3) | 10 (62.5) | 0.6052 |
| FBS (mg/dL) | 159.0 ± 40.0 | 137.6 ± 35.8 | 0.1989 |
| HbA1c (%) | 7.6 ± 1.7 | 7.2 ± 1.2 | 0.8123 |
| Creatinine (mg/dL) | 1.7 ± 1.6 | 2.6 ± 3.9 | 0.2767 |
| BUN (mg/dL) | 23.5 ± 13.9 | 29.9 ± 18.9 | 0.2992 |
| eGFR (mL/min/1.73 m2) | 60.9 ± 30.0 | 49.7 ± 25.1 | 0.3529 |
| The last presentation | |||
| LogMAR VA | 1.86 ± 1.01 (2, 0.15–2.89) | 0.70 ± 0.82 (0.61, −0.18–2.89) | 0.0026 |
| IOP (mmHg) | 12.4 ± 6.6 (13.0, 3–22) | 15.5 ± 8.0 (14.6, 6–42.3) | 0.4884 |
| IVB | 0.6 ± 0.7 | 0.4 ± 0.5 | 0.4544 |
| Cataract surgery | 15 (100) | 16 (100) | 1 |
| PPV with PRCP | 1.6 ± 1.3 | 1.4 ± 1.0 | 0.6084 |
| DCPC | 5 (33.3) | 6 (37.5) | 0.8085 |
| TLE + MMC | 1.3 ± 1.0 | 1.1 ± 0.8 | 0.6746 |
| IOP > 30 mmHg (n = 13) | IOP ≤ 30 mmHg (n = 18) | p Value | |
|---|---|---|---|
| Age (years) | 59.7 ± 12.0 * | 67.4 ± 11.1 | 0.0624 |
| Male/Female | 9/4 | 13/5 | 0.8563 |
| Follow-up periods (weeks) | 36.8 ± 35.6 | 28.5 ± 31.3 | 0.5613 |
| The initial presentation | |||
| LogMAR VA | 1.62 ± 1.04 (1.52, 0.10–2.89) † | 1.03 ± 1.02 (0.85, 0–2.89) | 0.0840 |
| IOP (mmHg) | 46.2 ± 15.4 (42.0, 30.7–78) | 23.5 ± 3.5 (23.2, 16.5–29.3) | <0.0001 |
| PRP | 9 (69.2) § | 16 (88.9) | 0.1716 |
| Cataract surgery | 9 (69.2) | 14 (77.8) | 0.5915 |
| PPV | 9 (69.2) | 9 (50.0) | 0.2843 |
| FBS (mg/dL) | 145.3 ± 37.3 | 149.8 ± 40.8 | 0.7793 |
| HbA1c (%) | 7.3 ± 1.1 | 7.5 ± 1.7 | 0.9202 |
| Creatinine (mg/dL) | 3.1 ± 4.4 | 1.4 ± 1.3 | 0.6887 |
| BUN (mg/dL) | 31.7 ± 22.0 | 22.9 ± 10.1 | 0.3713 |
| eGFR (mL/min/1.73 m2) | 52.9 ± 34.8 | 56.7 ± 22.2 | 0.9697 |
| The last presentation | |||
| LogMAR VA | 1.81 ± 1.03 (2.0, 0.52–2.89) | 0.87 ± 0.96 (0.76, −0.18–2.89) | 0.0286 |
| IOP (mmHg) | 12.4 ± 5.6 (12.0, 3–21) | 15.2 ± 8.4 (14.6, 4–42.3) | 0.4343 |
| IVB | 0.8 ± 0.7 | 0.3 ± 0.5 | 0.0410 |
| Cataract surgery | 13 (100) | 18 (100) | 1 |
| PPV with PRCP | 1.9 ± 1.3 | 1.2 ± 0.9 | 0.1055 |
| TLE + MMC | 1.4 ± 1.0 | 1.0 ± 0.8 | 0.2500 |
| DCPC | 4 (30.8) | 7 (38.9) | 0.6410 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeuchi, M.; Kanda, T.; Harimoto, K.; Sora, D.; Okazawa, R.; Sato, T. Surgical Treatment of Neovascular Glaucoma Secondary to Proliferative Diabetic Retinopathy in Japanese Patients without the Use of Glaucoma Drainage Devices. J. Clin. Med. 2024, 13, 3252. https://doi.org/10.3390/jcm13113252
Takeuchi M, Kanda T, Harimoto K, Sora D, Okazawa R, Sato T. Surgical Treatment of Neovascular Glaucoma Secondary to Proliferative Diabetic Retinopathy in Japanese Patients without the Use of Glaucoma Drainage Devices. Journal of Clinical Medicine. 2024; 13(11):3252. https://doi.org/10.3390/jcm13113252
Chicago/Turabian StyleTakeuchi, Masaru, Takayuki Kanda, Kozo Harimoto, Daisuke Sora, Rina Okazawa, and Tomohito Sato. 2024. "Surgical Treatment of Neovascular Glaucoma Secondary to Proliferative Diabetic Retinopathy in Japanese Patients without the Use of Glaucoma Drainage Devices" Journal of Clinical Medicine 13, no. 11: 3252. https://doi.org/10.3390/jcm13113252
APA StyleTakeuchi, M., Kanda, T., Harimoto, K., Sora, D., Okazawa, R., & Sato, T. (2024). Surgical Treatment of Neovascular Glaucoma Secondary to Proliferative Diabetic Retinopathy in Japanese Patients without the Use of Glaucoma Drainage Devices. Journal of Clinical Medicine, 13(11), 3252. https://doi.org/10.3390/jcm13113252