
Hidradenitis Suppurativa in the SARS-CoV-2 Pandemic: Investigation of Trigger Factors in a Single Center


 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Patients, and Data Collection
2.2. Study Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Personal and Clinical Characteristics of HS Patients
3.2. Impact of HS-Specific Characteristics on HS Deterioration
3.3. Impact of Lifestyle Changes on HS Exacerbation
3.4. Comparison of Medication and Ongoing Therapies from HS Patients
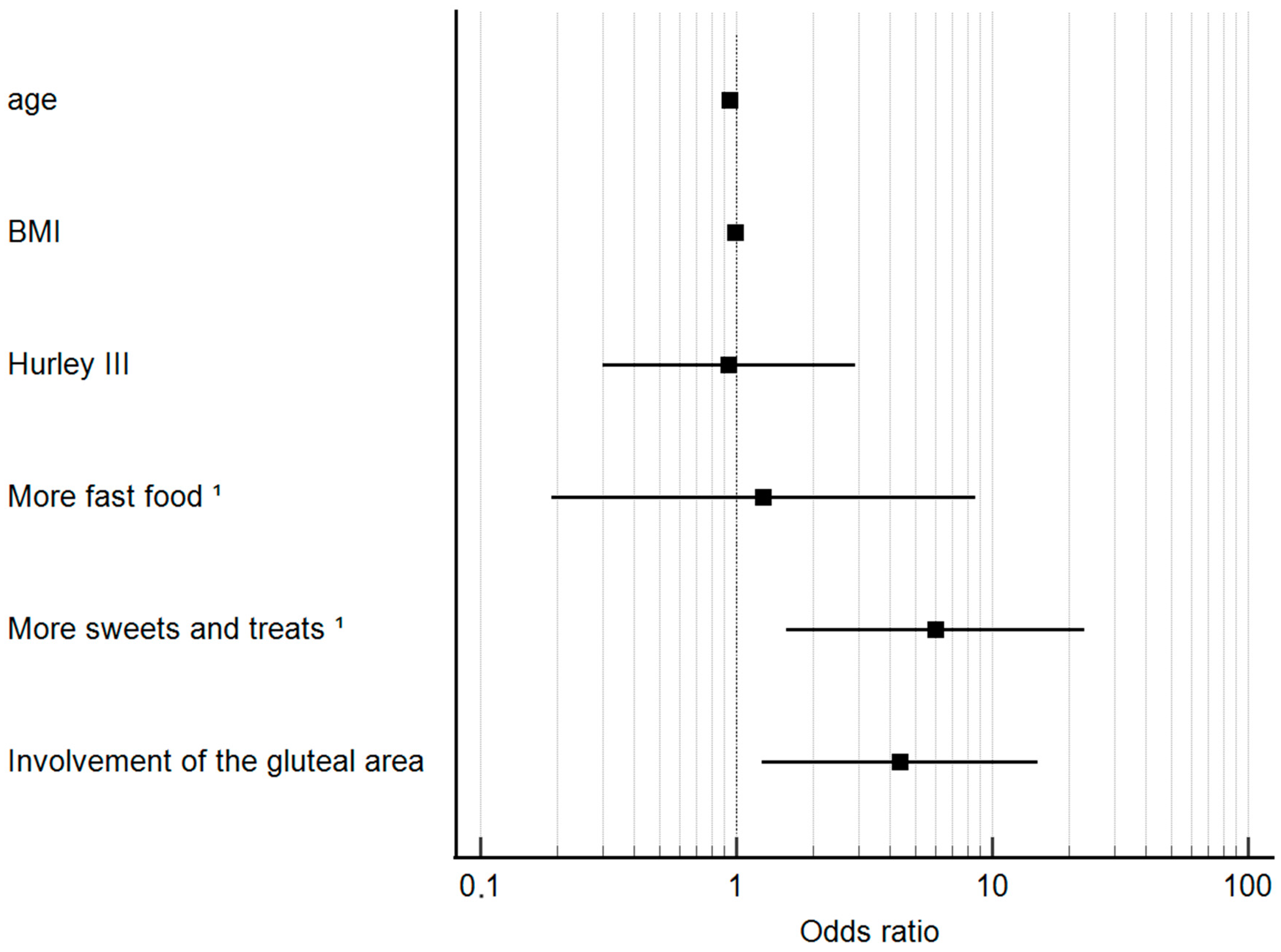
3.5. Logistic Regression Analysis for the Detection of Independent Trigger Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gooderham, M.; Papp, K. The psychosocial impact of hidradenitis suppurativa. J. Am. Acad. Dermatol. 2015, 73, S19–S22. [Google Scholar] [CrossRef]
- Frings, V.G.; Bauer, B.; Glöditzsch, M.; Goebeler, M.; Presser, D. Assessing the psychological burden of patients with hidradenitis suppurativa. Eur. J. Dermatol. 2019, 29, 294–301. [Google Scholar] [CrossRef]
- Abu Rached, N.; Gambichler, T.; Ocker, L.; Skrygan, M.; Seifert, C.; Scheel, C.H.; Stockfleth, E.; Bechara, F.G. Haptoglobin is an independent marker for disease severity and risk for metabolic complications in hidradenitis suppurativa: A prospective study. J. Eur. Acad. Dermatol. Venereol. 2024, 38, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Moltrasio, C.; Tricarico, P.M.; Romagnuolo, M.; Marzano, A.V.; Crovella, S. Hidradenitis Suppurativa: A Perspective on Genetic Factors Involved in the Disease. Biomedicines 2022, 10, 2039. [Google Scholar] [CrossRef]
- Hessam, S.; Sand, M.; Lang, K.; Käfferlein, H.U.; Scholl, L.; Gambichler, T.; Skrygan, M.; Brüning, T.; Stockfleth, E.; Bechara, F.G. Altered Global 5-Hydroxymethylation Status in Hidradenitis Suppurativa: Support for an Epigenetic Background. Dermatology 2017, 233, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Sivanand, A.; Gulliver, W.P.; Josan, C.K.; Alhusayen, R.; Fleming, P.J. Weight Loss and Dietary Interventions for Hidradenitis Suppurativa: A Systematic Review. J. Cutan. Med. Surg. 2020, 24, 64–72. [Google Scholar] [CrossRef]
- König, A.; Lehmann, C.; Rompel, R.; Happle, R. Cigarette smoking as a triggering factor of hidradenitis suppurativa. Dermatology 1999, 198, 261–264. [Google Scholar] [CrossRef]
- Bouwman, K.; Moazzen, S.; Kroah-Hartman, M.; Dijkstra, G.; Horváth, B.; Alizadeh, B.Z. Diet and physical activity as risk-reducing factors for hidradenitis suppurativa. J. Eur. Acad. Dermatol. Venereol. 2024, 38, 910–919. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lopez, O.; Martinez-Urbistondo, D.; Vargas-Nuñez, J.A.; Martinez, J.A. The Role of Nutrition on Meta-inflammation: Insights and Potential Targets in Communicable and Chronic Disease Management. Curr. Obes. Rep. 2022, 11, 305–335. [Google Scholar] [CrossRef]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Haddad, N.R.; Badiei, B.; Williams, K.L.; Garza, L.A. Positive correlation of hidradenitis suppurativa and ultra-processed foods consumption. Arch. Dermatol. Res. 2024, 316, 172. [Google Scholar] [CrossRef] [PubMed]
- Belamarić, M.; Miše, J.; Bukvić Mokos, Z. The Association Between Hidradenitis Suppurativa and Diet: An Update. Acta Dermatovenerol. Croat. 2023, 31, 213–219. [Google Scholar] [PubMed]
- Rodriguez-Leyva, D.; Pierce, G.N. The Impact of Nutrition on the COVID-19 Pandemic and the Impact of the COVID-19 Pandemic on Nutrition. Nutrients 2021, 13, 1752. [Google Scholar] [CrossRef] [PubMed]
- Woods, N.; Seabrook, J.A.; Schaafsma, H.; Burke, S.; Tucker, T.; Gilliland, J. Dietary Changes of Youth during the COVID-19 Pandemic: A Systematic Review. J. Nutr. 2024, 154, 1376–1403. [Google Scholar] [CrossRef] [PubMed]
- Wilke, J.; Rahlf, A.L.; Füzéki, E.; Groneberg, D.A.; Hespanhol, L.; Mai, P.; de Oliveira, G.M.; Robbin, J.; Tan, B.; Willwacher, S.; et al. Physical Activity During Lockdowns Associated with the COVID-19 Pandemic: A Systematic Review and Multilevel Meta-analysis of 173 Studies with 320,636 Participants. Sports Med. Open 2022, 8, 125. [Google Scholar] [CrossRef] [PubMed]
- LeWitt, T.M.; Mammis-Gierbolini, A.; Parnell, M.; Sarfo, A.; Paek, S.Y.; Benhadou, F.; del Marmol, V.; Hsiao, J.L.; Kirby, J.; Daveluy, S. International consensus definition of disease flare in hidradenitis suppurativa. Br. J. Dermatol. 2022, 187, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Finlay, A.Y.; Khan, G.K. Dermatology Life Quality Index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18.
- Hugelius, K.; Harada, N.; Marutani, M. Consequences of visiting restrictions during the COVID-19 pandemic: An integrative review. Int. J. Nurs. Stud. 2021, 121, 104000. [Google Scholar] [CrossRef]
- Hu, Z.; Lin, X.; Chiwanda Kaminga, A.; Xu, H. Impact of the COVID-19 Epidemic on Lifestyle Behaviors and Their Association with Subjective Well-Being among the General Population in Mainland China: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e21176. [Google Scholar] [CrossRef]
- Flanagan, E.W.; Beyl, R.A.; Fearnbach, S.N.; Altazan, A.D.; Martin, C.K.; Redman, L.M. The Impact of COVID-19 Stay-at-Home Orders on Health Behaviors in Adults. Obesity 2021, 29, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Kharel, M.; Sakamoto, J.L.; Carandang, R.R.; Ulambayar, S.; Shibanuma, A.; Yarotskaya, E.; Basargina, M.; Jimba, M. Impact of COVID-19 pandemic lockdown on movement behaviours of children and adolescents: A systematic review. BMJ Glob. Health 2022, 7, e007190. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.M.; Rytgaard, H.; Mogensen, U.B.; Miller, E.; Ring, H.C.; Ellervik, C.; Jemec, G.B. Body composition and basal metabolic rate in Hidradenitis Suppurativa: A Danish population-based and hospital-based cross-sectional study. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Kromann, C.B.; Ibler, K.S.; Kristiansen, V.B.; Jemec, G.B.E. The influence of body weight on the prevalence and severity of hidradenitis suppurativa. Acta Derm. Venereol. 2014, 94, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Theut Riis, P.; Saunte, D.M.; Benhadou, F.; Del Marmol, V.; Guillem, P.; El-Domyati, M.; Abdel-Wahab, H.; Antoniou, C.; Dessinioti, C.; Gürer, M.A.; et al. Low and high body mass index in hidradenitis suppurativa patients-different subtypes? J. Eur. Acad. Dermatol. Venereol. 2018, 32, 307–312. [Google Scholar] [CrossRef]
- Chierici, A.; Bulsei, J.; de Fatico, S.; Alromayan, M.; Alamri, A.; Pavone, G.; Liddo, G.; Fontas, E.; Iannelli, A. Effects of bariatric surgery on severe suppurative hidradenitis: Results of a nationwide administrative data study in France. J. Eur. Acad. Dermatol. Venereol. 2024, 38, e359–e361. [Google Scholar] [CrossRef]
- Boer, J.; Jemec, G.B.E. Mechanical forces and Hidradenitis Suppurativa. Exp. Dermatol. 2021, 30, 212–215. [Google Scholar] [CrossRef] [PubMed]
- de Winter, K.; van der Zee, H.H.; Prens, E.P. Is mechanical stress an important pathogenic factor in hidradenitis suppurativa? Exp. Dermatol. 2012, 21, 176–177. [Google Scholar] [CrossRef]
- Naik, H.B.; Alhusayen, R.; Frew, J.; Guilbault, S.; Hills, N.K.; Ingram, J.R.; Kudlinski, M.V.; Lowes, M.A.; Marzano, A.V.; Paul, M.; et al. Biologic therapy is not associated with increased COVID-19 severity in patients with hidradenitis suppurativa: Initial findings from the Global Hidradenitis Suppurativa COVID-19 Registry. J. Am. Acad. Dermatol. 2022, 86, 249–252. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Tzellos, T.; Kyrgidis, A.; Jemec, G.B.E.; Bechara, F.G.; Giamarellos-Bourboulis, E.J.; Ingram, J.R.; Kanni, T.; Karagiannidis, I.; Martorell, A.; et al. Development and validation of the International Hidradenitis Suppurativa Severity Score System (IHS4), a novel dynamic scoring system to assess HS severity. Br. J. Dermatol. 2017, 177, 1401–1409. [Google Scholar] [CrossRef]
- Hessam, S.; Scholl, L.; Sand, M.; Schmitz, L.; Reitenbach, S.; Bechara, F.G. A Novel Severity Assessment Scoring System for Hidradenitis Suppurativa. JAMA Dermatol. 2018, 154, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Nazzaro, G.; Passoni, E.; Muratori, S.; Moltrasio, C.; Guanziroli, E.; Barbareschi, M.; Veraldi, S.; Marzano, A.V. Comparison of clinical and sonographic scores in hidradenitis suppurativa and proposal of a novel ultrasound scoring system. Ital. J. Dermatol. Venerol. 2021, 156, 235–239. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameter | Value (s) | |
|---|---|---|
| sex, n (%) | female | 59 (53.6) |
| male | 51 (43.4) | |
| age, median (ICR), y | 41 (31–51.8) | |
| disease duration, median (IQR), y | 14 (8–22.8) | |
| BMI, median (ICR), kg/m2 | 30.1 (26.9–35.4) | |
| smoker, n (%) | current smoker | 41 (37.2) |
| not specified | 9 (8.2) | |
| non-smoker | 60 (54.6) | |
| subjective deterioration of HS, n (%) | Yes | 22 (20) |
| no | 88 (80) | |
| Hurley classification, n (%) | Hurley I | 9 (8.2) |
| Hurley II | 49 (44.6) | |
| Hurley III | 51 (47.2) |
| Parameter | HS Patients with Worsening HS (n = 22) | HS Patients without Worsening HS (n = 88) | p Value |
|---|---|---|---|
| Male vs. female, n (%) | 12 (23.5) vs. 10 (17) | 39 (76.5) vs. 49 (83.1) | 0.39 |
| BMI, median (ICR), kg/m2 | 31.6 (27.7–35.3) | 30.1 (26.5–35.3) | 0.5 |
| age, median (ICR), y | 35 (27.3–47.8) | 42.5 (32.5–52.3) | 0.08 |
| current smoker, n (%) | 7 (31.8) | 34 (38.6) | 0.18 |
| Disease duration, median (ICR), y | 12 (7–23) | 14.5 (8–22.3) | 0.62 |
| Hurley III, n (%) | 11 (50) | 41 (46.6) | 0.8 |
| More pain than before the pandemic, n (%) | 11 (50) | 5 (5.7) | <0.001 * |
| Avoidance of visits to the doctor, n (%) | 10 (45.5) | 16 (18.2) | 0.007 * |
| Involvement of the axillary region, n (%) | 8 (22.2) | 14 (18.9) | 0.7 |
| Involvement of the inguinal and thigh area, n (%) | 18 (81.2) | 64 (72.7) | 0.38 |
| Involvement of the gluteal area, n (%) | 11 (50) | 25 (28.4) | 0.05 |
| Involvement of the perianal or perineal area, n (%) | 9 (40.9) | 32 (36.3) | 0.69 |
| Involvement of the genital area, n (%) | 7 (31.8) | 38 (43.1) | 0.33 |
| Involvement of the Mons pubis, n (%) | 4 (18.2) | 26 (29.6) | 0.28 |
| Involvement of atypical localizations, n (%) | 0 (0) | 13 (14.8) | 0.06 |
| Parameter | HS Patients with Worsening HS (n = 22) | HS Patients without Worsening HS (n = 88) | p Value |
|---|---|---|---|
| Diet change, n (%) | 14 (63.6) | 30 (34.1) | 0.011 * |
| More fast food 1, n (%) | 4 (18.2) | 6 (6.8) | 0.1 |
| More meat 1, n (%) | 1 (4.6) | 1 (1.1) | 0.28 |
| More vegetables 1, n (%) | 5 (22.7) | 13 (14.8) | 0.37 |
| More sweets and treats 1, n (%) | 8 (36.4) | 12 (13.6) | 0.013 * |
| Less sport and movement 1, n (%) | 9 (40.9) | 29 (33) | 0.48 |
| Sport activity per day 2, median (ICR), h | 2 (1–8.5) | 2.25 (1–8) | 0.82 |
| Weight gain 1, median (range), kg | 0 (−8 to +25) | 0 (−20 to +25) | 0.63 |
| Relationship with the partner has changed 1, n (%) | 2 (9.1) | 6 (6.8) | 0.7 |
| Parameter | HS Patients with Worsening HS (n = 22) | HS Patients without Worsening HS (n = 88) | p Value |
|---|---|---|---|
| No therapy 1, n (%) | 9 (40.9) | 36 (40.9) | >0.9 |
| Oral zinc gluconate with triclosan local therapy, n (%) | 2 (9.1) | 6 (6.8) | 0.7 |
| Antibiotics with clindamycin and rifampicin, n (%) | 0 (0) | 4 (4.6) | 0.31 |
| Antibiotic therapy, n (%) | 0 (0) | 5 (5.7) | 0.25 |
| Ongoing therapy with biologic, n (%) | 11 (50) | 41 (46.6) | 0.8 |
| Parameters | Odds Ratio (OR) | 95% Confidence Interval (CI) | p Value |
|---|---|---|---|
| age | 0.945 | 0.9–0.991 | 0.021 * |
| BMI | 0.99 | 0.92–1.07 | 0.8 |
| Hurley III | 0.93 | 0.3–2.93 | 0.9 |
| More fast food 1 | 1.27 | 0.19–8.64 | 0.8 |
| More sweets and treats 1 | 6.01 | 1.57–23 | 0.009 * |
| Involvement of the gluteal area | 4.36 | 1.26–15.1 | 0.02 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scholl, L.; Abu Rached, N.; Stockfleth, E.; Cramer, P.; Ocker, L.; Stranzenbach, R.; Garcovich, S.; Hessam, S.; Bechara, F.G. Hidradenitis Suppurativa in the SARS-CoV-2 Pandemic: Investigation of Trigger Factors in a Single Center. J. Clin. Med. 2024, 13, 4074. https://doi.org/10.3390/jcm13144074
Scholl L, Abu Rached N, Stockfleth E, Cramer P, Ocker L, Stranzenbach R, Garcovich S, Hessam S, Bechara FG. Hidradenitis Suppurativa in the SARS-CoV-2 Pandemic: Investigation of Trigger Factors in a Single Center. Journal of Clinical Medicine. 2024; 13(14):4074. https://doi.org/10.3390/jcm13144074
Chicago/Turabian StyleScholl, Lisa, Nessr Abu Rached, Eggert Stockfleth, Philipp Cramer, Lennart Ocker, René Stranzenbach, Simone Garcovich, Schapoor Hessam, and Falk G. Bechara. 2024. "Hidradenitis Suppurativa in the SARS-CoV-2 Pandemic: Investigation of Trigger Factors in a Single Center" Journal of Clinical Medicine 13, no. 14: 4074. https://doi.org/10.3390/jcm13144074
APA StyleScholl, L., Abu Rached, N., Stockfleth, E., Cramer, P., Ocker, L., Stranzenbach, R., Garcovich, S., Hessam, S., & Bechara, F. G. (2024). Hidradenitis Suppurativa in the SARS-CoV-2 Pandemic: Investigation of Trigger Factors in a Single Center. Journal of Clinical Medicine, 13(14), 4074. https://doi.org/10.3390/jcm13144074