
Goal Setting for Participatory Person-Centered Geriatric Rehabilitation—From Function-Centered Rehabilitation towards Digitally Supported Personalized and Integrated Care for Older People

 , , , and
, , , and {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Results from the Literature Search
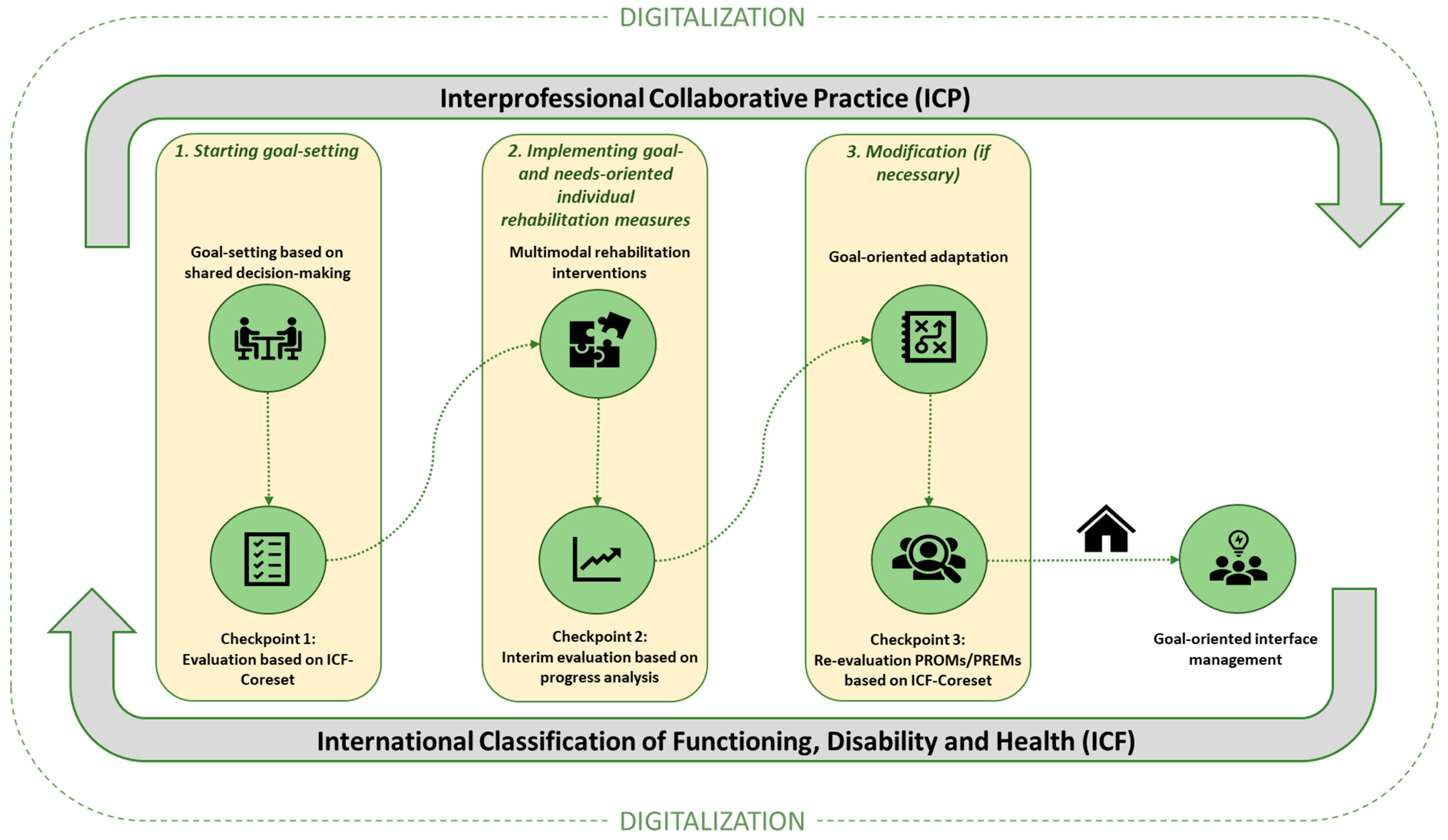
3.2. Concept of a Goal-Oriented Rehabilitation Care Process in Geriatric Rehabilitation
3.3. The Participatory Rehabilitation Approach in Geriatric Rehabilitation
3.4. What Is the Future for “Goal-Oriented and Participatory” Geriatric Rehabilitation in Digitalized Healthcare?
4. Conclusions and Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Union. Ageing Europe. Looking at the Lives of Older People in the EU, 2020th ed.; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar]
- Eurostat. Population on 1st January by Age, Sex and Type of Projection; Eurostat: Luxembourg, 2023. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Luxembourg, 2015. [Google Scholar]
- Freiberger, E.; Kemmler, W.; Siegrist, M.; Sieber, C. Frailty and exercise interventions: Evidence and barriers for exercise programs. Z. Gerontol. Geriatr. 2016, 49, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Stolz, E.; Mayerl, H.; Godin, J.; Hoogendijk, E.O.; Theou, O.; Freidl, W.; Rockwood, K. Reliability of the frailty index among community-dwelling older adults. J. Gerontol. Ser. A 2024, 79, glad227. [Google Scholar] [CrossRef]
- Stucki, G.; Cieza, A.; Melvin, J. The International Classification of Functioning, Disability and Health (ICF): A unifying model for the conceptual description of the rehabilitation strategy. J. Rehabil. Med. 2007, 39, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Achterberg, W.P.; Cameron, I.D.; Bauer, J.M.; Schols, J.M. Geriatric Rehabilitation-State of the Art and Future Priorities. J. Am. Med. Dir. Assoc. 2019, 20, 396–398. [Google Scholar] [CrossRef] [PubMed]
- Grund, S.; Gordon, A.L.; van Balen, R.; Bachmann, S.; Cherubini, A.; Landi, F.; Stuck, A.E.; Becker, C.; Achterberg, W.P.; Bauer, J.M.; et al. European consensus on core principles and future priorities for geriatric rehabilitation: Consensus statement. Eur. Geriatr. Med. 2020, 11, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Everink, I.H.; van Haastregt, J.C.; Kempen, G.I.; Schols, J.M. Building consensus on an integrated care pathway in geriatric rehabilitation: A modified Delphi study among professional experts. J. Appl. Gerontol. 2020, 39, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Everink, I.H.; van Haastregt, J.C.; Tan, F.E.; Schols, J.M.; Kempen, G.I. The effectiveness of an integrated care pathway in geriatric rehabilitation among older patients with complex health problems and their informal caregivers: A prospective cohort study. BMC Geriatr. 2018, 18, 285. [Google Scholar] [CrossRef] [PubMed]
- Gladman, J.R. The international classification of functioning, disability and health and its value to rehabilitation and geriatric medicine. J. Chin. Med. Assoc. 2008, 71, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Patrizio, E.; Calvani, R.; Marzetti, E.; Cesari, M. Physical functional assessment in older adults. J. Frailty Aging 2021, 10, 141–149. [Google Scholar] [CrossRef]
- Abdeen, H.A.; Helmy, Z.M.; Elnaggar, M.I.; Aldhahi, M.I.; Taha, M.M.; Marques-Sule, E.; Amin, D.I.; Ibrahim, B.S.; Abdel Aziz, A.; Castiglione, V. Different Continuous Training Intensities Improve Echocardiographic Parameters, Quality of Life, and Functional Capacity in Heart Failure Patients with Reduced Ejection Fraction. Int. J. Gen. Med. 2023, 16, 3933–3945. [Google Scholar] [CrossRef]
- Leonardi, M.; Lee, H.; Kostanjsek, N.; Fornari, A.; Raggi, A.; Martinuzzi, A.; Yáñez, M.; Almborg, A.-H.; Fresk, M.; Besstrashnova, Y. 20 years of ICF—International classification of functioning, disability and health: Uses and applications around the world. Int. J. Environ. Res. Public Health 2022, 19, 11321. [Google Scholar] [CrossRef]
- Skoumal, M.; Honegger, M.; Roller-Wirnsberger, R. Frailty and innovative participatory rehabilitation. J. Nutr. Health Aging 2024, 28, 100012. [Google Scholar] [CrossRef]
- Azzopardi, R.V.; Vermeiren, S.; Gorus, E.; Habbig, A.-K.; Petrovic, M.; Van Den Noortgate, N.; De Vriendt, P.; Bautmans, I.; Beyer, I.; Verté, D. Linking frailty instruments to the international classification of functioning, disability, and health: A systematic review. J. Am. Med. Dir. Assoc. 2016, 17, 1066-e1. [Google Scholar] [CrossRef] [PubMed]
- Dionyssiotis, Y.; Masiero, S.; Maccarone, M.C.; Prokopidis, K.; Dzhafer, N.; Matzaroglou, C.; Tsekoura, M.; Panayotov, K.; Papathanasiou, J. Frailty: Future prospectives in rehabilitation medicine. Eur. J. Transl. Myol. 2023, 33, 11347. [Google Scholar] [CrossRef]
- Meyer, T.; Weiss, C.; Rathore, F.A. Goal Setting In Medical Rehabilitation: A Narrative Review. J. Pak. Med. Assoc. 2023, 73, 1923–1925. [Google Scholar] [CrossRef]
- Grund, S.; van Wijngaarden, J.P.; Gordon, A.L.; Schols, J.M.G.A.; Bauer, J.M. EuGMS survey on structures of geriatric rehabilitation across Europe. Eur. Geriatr. Med. 2020, 11, 217–232. [Google Scholar] [CrossRef]
- Prins, L.A.P.; Gamble, C.J.; van Dam van Isselt, E.F.; Stammen, R.A.I.; Ettaibi, A.; Creemers, I.A.M.; van Haastregt, J.C.M. An Exploratory Study Investigating Factors Influencing the Outpatient Delivery of Geriatric Rehabilitation. J. Clin. Med. 2023, 12, 5045. [Google Scholar] [CrossRef]
- Baker, A.; Cornwell, P.; Gustafsson, L.; Stewart, C.; Lannin, N.A. Developing tailored theoretically informed goal-setting interventions for rehabilitation services: A co-design approach. BMC Health Serv. Res. 2022, 22, 811. [Google Scholar] [CrossRef]
- Pol, M.; Qadeer, A.; van Hartingsveldt, M.; Choukou, M.A. Perspectives of Rehabilitation Professionals on Implementing a Validated Home Telerehabilitation Intervention for Older Adults in Geriatric Rehabilitation: Multisite Focus Group Study. JMIR Rehabil. Assist. Technol. 2023, 10, e44498. [Google Scholar] [CrossRef]
- Kraaijkamp, J.J.M.; Persoon, A.; Aurelian, S.; Bachmann, S.; Cameron, I.D.; Choukou, M.-A.; Dockery, F.; Eruslanova, K.; Gordon, A.L.; Grund, S.; et al. eHealth in Geriatric Rehabilitation: An International Survey of the Experiences and Needs of Healthcare Professionals. J. Clin. Med. 2023, 12, 4504. [Google Scholar] [CrossRef]
- Lynch, A.; Flood, E.; Mello, S. 282 Self-reported quality of life in patients completing a geriatric rehabilitation program. Age Ageing 2022, 51, afac218.249. [Google Scholar] [CrossRef]
- Lozupone, M.; Panza, F. A multidimensional frailty approach in predicting and preventing dementia. Lancet Healthy Longev. 2020, 1, e49–e50. [Google Scholar] [CrossRef]
- Rose, A.; Rosewilliam, S.; Soundy, A. Shared decision making within goal setting in rehabilitation settings: A systematic review. Patient Educ. Couns 2017, 100, 65–75. [Google Scholar] [CrossRef]
- Tijsen, L.M.J.; Derksen, E.W.C.; Achterberg, W.P.; Buijck, B.I. A Qualitative Study Exploring Professional Perspectives of a Challenging Rehabilitation Environment for Geriatric Rehabilitation. J. Clin. Med. 2023, 12, 1231. [Google Scholar] [CrossRef]
- Harty, M.; Griesel, M.; van der Merwe, A. The ICF as a common language for rehabilitation goal-setting: Comparing client and professional priorities. Health Qual Life Outcomes 2011, 9, 87. [Google Scholar] [CrossRef]
- Vaalburg, A.M.; Wattel, E.; Boersma, P.; Hertogh, C.; Gobbens, R. Goal-setting in geriatric rehabilitation: Can the nursing profession meet patients’ needs? A narrative review. Nurs. Forum 2021, 56, 648–659. [Google Scholar] [CrossRef]
- Smit, E.B.; Bouwstra, H.; Hertogh, C.M.; Wattel, E.M.; van der Wouden, J.C. Goal-setting in geriatric rehabilitation: A systematic review and meta-analysis. Clin. Rehabil. 2019, 33, 395–407. [Google Scholar] [CrossRef]
- Lubbe, A.L.; van Rijn, M.; Groen, W.G.; Hilhorst, S.; Burchell, G.L.; Hertogh, C.; Pol, M.C. The quality of geriatric rehabilitation from the patients’ perspective: A scoping review. Age Ageing 2023, 52, afad032. [Google Scholar] [CrossRef]
- Okita, Y.; Kawaguchi, Y.; Inoue, Y.; Ohno, K.; Sawada, T.; Levack, W.; Tomori, K. Characteristics of goal-setting tools in adult rehabilitation: A scoping review. Clin. Rehabil. 2024, 38, 234–250. [Google Scholar] [CrossRef]
- Gutenbrunner, C.; Nugraha, B. 2.1 Rehabilitation: Rehabilitation as a Health Strategy. J. Int. Soc. Phys. Rehabil. Med. 2019, 2, S15–S18. [Google Scholar] [CrossRef]
- van Seben, R.; Smorenburg, S.M.; Buurman, B.M. A qualitative study of patient-centered goal-setting in geriatric rehabilitation: Patient and professional perspectives. Clin. Rehabil. 2019, 33, 128–140. [Google Scholar] [CrossRef] [PubMed]
- van de Pol, M.H.; Fluit, C.R.; Lagro, J.; Slaats, Y.H.; Olde Rikkert, M.G.; Lagro-Janssen, A.L. Expert and patient consensus on a dynamic model for shared decision-making in frail older patients. Patient Educ. Couns 2016, 99, 1069–1077. [Google Scholar] [CrossRef]
- Yamashita, M.; Mashizume, Y.; Yama, K.; Sasaki, S.; Uehara, D.; Kamiya, K. Protocols and Features of Goal-Setting-Based Intervention for Frail Older Adults in Community Exercise Facilities. Int. J. Environ. Res. Public Health 2023, 20, 1615. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.-Y.; Chou, M.-Y.; Liang, C.-K.; Lin, Y.-T.; Chen, R.-Y.; Wu, P.-F. Physical activity plays a crucial role in multidomain intervention for frailty prevention. Aging Clin. Exp. Res. 2023, 35, 1283–1292. [Google Scholar] [CrossRef]
- Wu, K.-Y.; Chen, D.-R.; Chan, C.-C.; Yeh, Y.-P.; Chen, H.-H. Fear of falling as a mediator in the association between social frailty and health-related quality of life in community-dwelling older adults. BMC Geriatr. 2023, 23, 421. [Google Scholar] [CrossRef] [PubMed]
- Sadaqa, M.; Debes, W.A.; Németh, Z.; Bera-Baka, Z.; Vachtler-Szepesi, M.; Nácziné Földes, L.; Prémusz, V.; Hock, M. Multicomponent exercise intervention for preventing falls and improving physical functioning in older nursing home residents: A single-blinded pilot randomised controlled trial. J. Clin. Med. 2024, 13, 1577. [Google Scholar] [CrossRef]
- de Souza, L.F.; Canever, J.B.; Moreira, B.S.; Danielewicz, A.L.; de Avelar, N.C.P. Association Between Fear of Falling and Frailty in Community-Dwelling Older Adults: A Systematic Review. Clin. Interv. Aging 2022, 17, 129–140. [Google Scholar] [CrossRef]
- Pel-Littel, R.E.; Snaterse, M.; Teppich, N.M.; Buurman, B.M.; van Etten-Jamaludin, F.S.; van Weert, J.C.M.; Minkman, M.M.; Scholte Op Reimer, W.J.M. Barriers and facilitators for shared decision making in older patients with multiple chronic conditions: A systematic review. BMC Geriatr. 2021, 21, 112. [Google Scholar] [CrossRef] [PubMed]
- Roller-Wirnsberger, R.; Lindner, S.; Liew, A.; O’Caoimh, R.; Koula, M.-L.; Moody, D.; Espinosa, J.M.; Van Durme, T.; Dimitrov, P.; Benjak, T. European collaborative and interprofessional capability framework for prevention and management of frailty—A consensus process supported by the Joint Action for Frailty Prevention (ADVANTAGE) and the European Geriatric Medicine Society (EuGMS). Aging Clin. Exp. Res. 2020, 32, 561–570. [Google Scholar] [CrossRef]
- Jesus, T.S.; Papadimitriou, C.; Bright, F.A.; Kayes, N.M.; Pinho, C.S.; Cott, C.A. Person-Centered Rehabilitation Model: Framing the Concept and Practice of Person-Centered Adult Physical Rehabilitation Based on a Scoping Review and Thematic Analysis of the Literature. Arch. Phys. Med. Rehabil. 2022, 103, 106–120. [Google Scholar] [CrossRef]
- Anuruang, S.; Hickman, L.D.; Jackson, D.; Dharmendra, T.; Van Balen, J.; Davidson, P.M. Community-based interventions to promote management for older people: An integrative review. J. Clin. Nurs. 2014, 23, 2110–2120. [Google Scholar] [CrossRef] [PubMed]
- Smit, E.B.; Bouwstra, H.; van der Wouden, J.C.; Wattel, L.M.; Hertogh, C. Patient-centred goal setting using functional outcome measures in geriatric rehabilitation: Is it feasible? Eur. Geriatr. Med. 2018, 9, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Cameron, L.J.; Somerville, L.M.; Naismith, C.E.; Watterson, D.; Maric, V.; Lannin, N.A. A qualitative investigation into the patient-centered goal-setting practices of allied health clinicians working in rehabilitation. Clin. Rehabil. 2018, 32, 827–840. [Google Scholar] [CrossRef] [PubMed]
- Yun, D.; Choi, J. Person-centered rehabilitation care and outcomes: A systematic literature review. Int. J. Nurs. Stud. 2019, 93, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Levack, W.M.; Weatherall, M.; Hay-Smith, J.C.; Dean, S.G.; McPherson, K.; Siegert, R.J. Goal setting and strategies to enhance goal pursuit in adult rehabilitation: Summary of a Cochrane systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2016, 52, 400–416. [Google Scholar] [PubMed]
- Dutzi, I.; Schwenk, M.; Kirchner, M.; Bauer, J.M.; Hauer, K. “What would you like to achieve?” Goal-Setting in Patients with Dementia in Geriatric Rehabilitation. BMC Geriatr. 2019, 19, 280. [Google Scholar] [CrossRef] [PubMed]
- Gißke, C.; Liu, J.; Gand, K. Applying Goal-Oriented Modelling for Machine Learning Based Rehabilitation Care. In Challenges of Trustable AI and Added-Value on Health; IOS Press: Amsterdam, The Netherlands, 2022; pp. 342–346. [Google Scholar]
- Strubbia, C.; Levack, W.M.M.; Grainger, R.; Takahashi, K.; Tomori, K. Use of technology in supporting goal setting in rehabilitation for adults: A scoping review. BMJ Open 2020, 10, e041730. [Google Scholar] [CrossRef] [PubMed]
- Alhasani, R.; George, N.; Radman, D.; Auger, C.; Ahmed, S. Methodologies for Evaluating the Usability of Rehabilitation Technologies Aimed at Supporting Shared Decision-Making: Scoping Review. JMIR Rehabil. Assist. Technol. 2023, 10, e41359. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, A.; Roberts, A.; Freeman, J. ‘Finding a balance’in involving patients in goal setting early after stroke: A physiotherapy perspective. Physiother. Res. Int. 2014, 19, 147–157. [Google Scholar] [CrossRef]
- Dicianno, B.E.; Henderson, G.; Parmanto, B. Design of mobile health tools to promote goal achievement in self-management tasks. JMIR mHealth and uHealth 2017, 5, e7335. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skoumal, M.; Lindner-Rabl, S.; Honegger, M.; Pertinatsch, C.; Kadane, C.; Neubacher, B.; Herzog, C.; Roller-Wirnsberger, R. Goal Setting for Participatory Person-Centered Geriatric Rehabilitation—From Function-Centered Rehabilitation towards Digitally Supported Personalized and Integrated Care for Older People. J. Clin. Med. 2024, 13, 4134. https://doi.org/10.3390/jcm13144134
Skoumal M, Lindner-Rabl S, Honegger M, Pertinatsch C, Kadane C, Neubacher B, Herzog C, Roller-Wirnsberger R. Goal Setting for Participatory Person-Centered Geriatric Rehabilitation—From Function-Centered Rehabilitation towards Digitally Supported Personalized and Integrated Care for Older People. Journal of Clinical Medicine. 2024; 13(14):4134. https://doi.org/10.3390/jcm13144134
Chicago/Turabian StyleSkoumal, Martin, Sonja Lindner-Rabl, Martina Honegger, Christoph Pertinatsch, Christof Kadane, Britta Neubacher, Carolin Herzog, and Regina Roller-Wirnsberger. 2024. "Goal Setting for Participatory Person-Centered Geriatric Rehabilitation—From Function-Centered Rehabilitation towards Digitally Supported Personalized and Integrated Care for Older People" Journal of Clinical Medicine 13, no. 14: 4134. https://doi.org/10.3390/jcm13144134