
Heat Shock Protein 70 Constitutes a Promising Novel Biomarker in Differential Diagnosis between Takotsubo Syndrome and Non-ST-Segment Elevation Myocardial Infarction

 , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Measurement of Serum HSP70 Concentrations
2.3. Statistical Analysis
3. Results
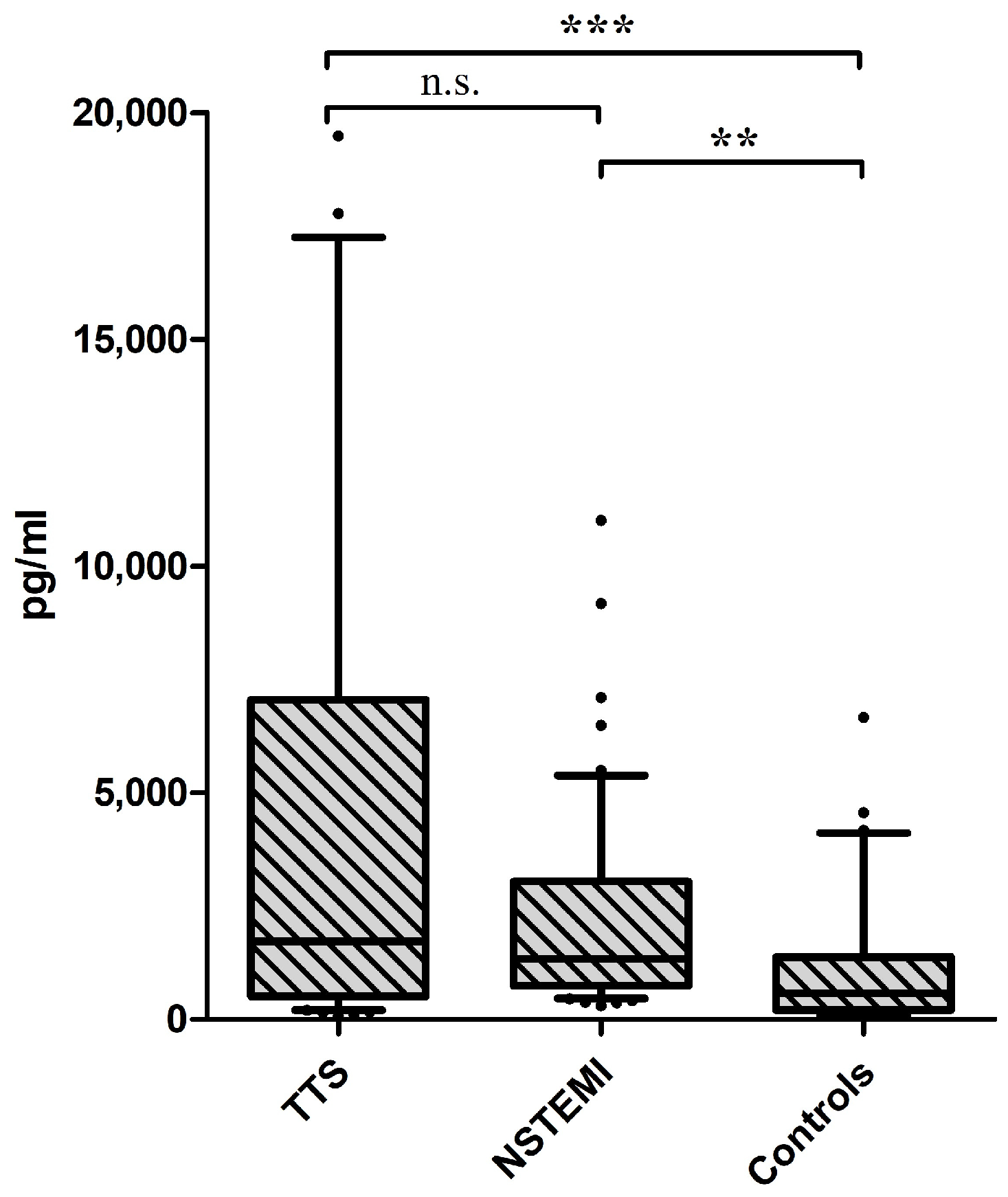
3.1. Serum Concentrations of HSP70
3.2. ROC Curve Analysis
3.3. Binary Logistic Regression Analysis
3.4. Propensity-Score-Weighted Logistic Regression Analysis
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harikrishnan, S.; Jeemon, P.; Mini, G.K.; Thankappan, K.R.; Sylaja, P.G.B.D. GBD 2017 Causes of Death Collaborators Global, Regional, and National Age-Sex-Specific Mortality for 282 Causes of Death in 195 Countries and Territories, 1980-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Kurowski, V.; Kaiser, A.; von Hof, K.; Killermann, D.P.; Mayer, B.; Hartmann, F.; Schunkert, H.; Radke, P.W. Apical and Midventricular Transient Left Ventricular Dysfunction Syndrome (Tako-Tsubo Cardiomyopathy): Frequency, Mechanisms, and Prognosis. Chest 2007, 132, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Gianni, M.; Dentali, F.; Grandi, A.M.; Sumner, G.; Hiralal, R.; Lonn, E. Apical Ballooning Syndrome or Takotsubo Cardiomyopathy: A Systematic Review. Eur. Heart J. 2006, 27, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Sugihara, H.; Katoh, S.; Azuma, A.; Nakagawa, M. Assessment of Takotsubo (Ampulla) Cardiomyopathy using99mTc-Tetrofosmin Myocardial SPECT—Comparison with Acute Coronary Syndrome. Ann. Nucl. Med. 2003, 17, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)Developed with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the Management of Acute Coronary Syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, R.; Nillegoda, N.B.; Mayer, M.P.; Bukau, B. The Hsp70 Chaperone Network. Nat. Rev. Mol. Cell. Biol. 2019, 20, 665–680. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Barua, S.; Huang, M.Y.; Park, J.; Yenari, M.A.; Lee, J.E. Heat Shock Protein 70 (HSP70) Induction: Chaperonotherapy for Neuroprotection after Brain Injury. Cells 2020, 9, 2020. [Google Scholar] [CrossRef] [PubMed]
- Singh, T.; Khan, H.; Gamble, D.T.; Scally, C.; Newby, D.E.; Dawson, D. Takotsubo Syndrome: Pathophysiology, Emerging Concepts and Clinical Implications. Circulation 2022, 145, 1002–1019. [Google Scholar] [CrossRef]
- Pasqua, T.; Filice, E.; Mazza, R.; Quintieri, A.M.; Carmela Cerra, M.; Iannacone, R.; Melfi, D.; Indiveri, C.; Gattuso, A.; Angelone, T. Cardiac and Hepatic Role of R-AtHSP70: Basal Effects and Protection against Ischemic and Sepsis Conditions. J. Cell. Mol. Med. 2015, 19, 1492–1503. [Google Scholar] [CrossRef]
- Heydari, A.R.; Takahashi, R.; Gutsmann, A.; You, S.; Richardson, A. Hsp70 and Aging. Experientia 1994, 50, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.E. The HSP70 Family and Cancer. Carcinogenesis 2013, 34, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Genth-Zotz, S.; Bolger, A.P.; Kalra, P.R.; von Haehling, S.; Doehner, W.; Coats, A.J.S.; Volk, H.-D.; Anker, S.D. Heat Shock Protein 70 in Patients with Chronic Heart Failure: Relation to Disease Severity and Survival. Int. J. Cardiol. 2004, 96, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Song, Y.; Xing, R.; Yu, H.; Zhang, Y.; Li, Z.; Gao, W. Heat Shock Protein 70 Acts as a Potential Biomarker for Early Diagnosis of Heart Failure. PLoS ONE 2013, 8, e67964. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.-J.; Huang, Y.-X.; Shen, Y.; Cui, C.-J.; Zhang, X.-L.; Zhang, H.; Hu, S.-S. Proteomic Analysis Reveals Significant Elevation of Heat Shock Protein 70 in Patients with Chronic Heart Failure Due to Arrhythmogenic Right Ventricular Cardiomyopathy. Mol. Cell. Biochem. 2009, 332, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Konstantinova, E.V.; Chipigina, N.S.; Shurdumova, M.H.; Kovalenko, E.I.; Sapozhnikov, A.M. Heat Shock Protein 70 kDa as a Target for Diagnostics and Therapy of Cardiovascular and Cerebrovascular Diseases. Curr. Pharm. Des. 2019, 25, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Ranek, M.J.; Stachowski, M.J.; Kirk, J.A.; Willis, M.S. The Role of Heat Shock Proteins and Co-Chaperones in Heart Failure. Philos. Trans. R. Soc. B Biol. Sci. 2018, 373, 20160530. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; Barylski, M.; Mikhailidis, D.P.; Rysz, J.; Banach, M. HSP 70 and Atherosclerosis—Protector or Activator? Expert. Opin. Ther. Targets 2009, 13, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Costa-Beber, L.C.; Hirsch, G.E.; Heck, T.G.; Ludwig, M.S. Chaperone Duality: The Role of Extracellular and Intracellular HSP70 as a Biomarker of Endothelial Dysfunction in the Development of Atherosclerosis. Arch. Physiol. Biochem. 2022, 128, 1016–1023. [Google Scholar] [CrossRef]
- Poznyak, A.V.; Orekhova, V.A.; Sukhorukov, V.N.; Khotina, V.A.; Popov, M.A.; Orekhov, A.N. Atheroprotective Aspects of Heat Shock Proteins. Int. J. Mol. Sci. 2023, 24, 11750. [Google Scholar] [CrossRef]
- Rodriguez-Iturbe, B.; Johnson, R.J.; Sanchez-Lozada, L.G.; Pons, H. HSP70 and Primary Arterial Hypertension. Biomolecules 2023, 13, 272. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Iturbe, B.; Lanaspa, M.A.; Johnson, R.J. The Role of Autoimmune Reactivity Induced by Heat Shock Protein 70 in the Pathogenesis of Essential Hypertension. Br. J. Pharmacol. 2019, 176, 1829–1838. [Google Scholar] [CrossRef]
- Liu, D.; Han, X.; Zhang, Z.; Tse, G.; Shao, Q.; Liu, T. Role of Heat Shock Proteins in Atrial Fibrillation: From Molecular Mechanisms to Diagnostic and Therapeutic Opportunities. Cells 2022, 12, 151. [Google Scholar] [CrossRef] [PubMed]
- Ghadri, J.-R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef]
- Martínez-Camblor, P.; Pardo-Fernández, J.C. The Youden Index in the Generalized Receiver Operating Characteristic Curve Context. Int. J. Biostat. 2019, 15, 20180060. [Google Scholar] [CrossRef]
- McCaffrey, D.F.; Griffin, B.A.; Almirall, D.; Slaughter, M.E.; Ramchand, R.; Burgette, L.F. A Tutorial on Propensity Score Estimation for Multiple Treatments Using Generalized Boosted Models. Stat. Med. 2013, 32, 3388–3414. [Google Scholar] [CrossRef]
- Doyen, D.; Moceri, P.; Chiche, O.; Schouver, E.; Cerboni, P.; Chaussade, C.; Mansencal, N.; Ferrari, E. Cardiac Biomarkers in Takotsubo Cardiomyopathy. Int. J. Cardiol. 2014, 174, 798–801. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.; Gamble, D.; Mezincescu, A.; Abbas, H.; Rudd, A.; Dawson, D. A Systematic Review of Biomarkers in Takotsubo Syndrome: A Focus on Better Understanding the Pathophysiology. Int. J. Cardiol. Heart Vasc. 2021, 34, 100795. [Google Scholar] [CrossRef]
- Wittstein, I.S.; Thiemann, D.R.; Lima, J.A.C.; Baughman, K.L.; Schulman, S.P.; Gerstenblith, G.; Wu, K.C.; Rade, J.J.; Bivalacqua, T.J.; Champion, H.C. Neurohumoral Features of Myocardial Stunning Due to Sudden Emotional Stress. N. Engl. J. Med. 2005, 352, 539–548. [Google Scholar] [CrossRef]
- Lyon, A.R.; Rees, P.S.C.; Prasad, S.; Poole-Wilson, P.A.; Harding, S.E. Stress (Takotsubo) Cardiomyopathy—A Novel Pathophysiological Hypothesis to Explain Catecholamine-Induced Acute Myocardial Stunning. Nat. Clin. Pract. Cardiovasc. Med. 2008, 5, 22–29. [Google Scholar] [CrossRef]
- Akashi, Y.J.; Nakazawa, K.; Sakakibara, M.; Miyake, F.; Musha, H.; Sasaka, K. 123I-MIBG Myocardial Scintigraphy in Patients with “Takotsubo” Cardiomyopathy. J. Nucl. Med. 2004, 45, 1121–1127. [Google Scholar] [PubMed]
- Kume, T.; Akasaka, T.; Kawamoto, T.; Yoshitani, H.; Watanabe, N.; Neishi, Y.; Wada, N.; Yoshida, K. Assessment of Coronary Microcirculation in Patients with Takotsubo-like Left Ventricular Dysfunction. Circ. J. 2005, 69, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Kaski, J.C.; Crea, F.; Camici, P.G. Pathophysiology of Takotsubo Syndrome. Circulation 2017, 135, 2426–2441. [Google Scholar] [CrossRef] [PubMed]
- Dybdahl, B.; Wahba, A.; Lien, E.; Flo, T.; Waage, A.; Qureshi, N.; Sellevold, O.M.; Espevik, T.; Sundan, A. Inflammatory Response After Open Heart Surgery: Release of Heat-Shock Protein 70 and Signaling Through Toll-Like Receptor-4. Circ. J. Am. Heart Assoc. 2002, 105, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Pan, S.; Shen, Y. Cardioprotection of Exercise Preconditioning Involving Heat Shock Protein 70 and Concurrent Autophagy: A Potential Chaperone-Assisted Selective Macroautophagy Effect. J. Physiol. Sci. 2016, 68, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Wendel, H.; Vonthein, R.; Rennekampff, H.; Aebert, H. Inducible HSP70 Levels in Thoracic Wound Fluid Indicate Myocardial Damage after Open Heart Surgery. J. Cardiovasc. Surg. 2007, 48, 233–237. [Google Scholar]
- Gao, X.; Liu, W.; Huang, L.; Zhang, T.; Mei, Z.; Wang, X.; Gong, J.; Zhao, Y.; Xie, F.; Ma, J.; et al. HSP70 Inhibits Stress-Induced Cardiomyocyte Apoptosis by Competitively Binding to FAF1. Cell Stress Chaperones 2015, 20, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Latchman, D.S. Heat Shock Proteins and Cardiac Protection. Cardiovasc. Res. 2001, 51, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Taufiq, F.; Maharani, N.; Li, P.; Kurata, Y.; Ikeda, N.; Kuwabara, M.; Otani, N.; Miake, J.; Hasegawa, A.; Tsuneto, M.; et al. Uric Acid-Induced Enhancements of Kv1.5 Protein Expression and Channel Activity via the Akt-HSF1-Hsp70 Pathway in HL-1 Atrial Myocytes. Circ. J. 2019, 83, 718–726. [Google Scholar] [CrossRef]
- Fekete, A.; Vér, A.; Bögi, K.; Treszl, A.; Rigó, J. Is Preeclampsia Associated with Higher Frequency of HSP70 Gene Polymorphisms? Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 126, 197–200. [Google Scholar] [CrossRef]
- Piani, F.; Agnoletti, D.; Baracchi, A.; Scarduelli, S.; Verde, C.; Tossetta, G.; Montaguti, E.; Simonazzi, G.; Degli Esposti, D.; Borghi, C.; et al. Serum Uric Acid to Creatinine Ratio and Risk of Preeclampsia and Adverse Pregnancy Outcomes. J. Hypertens. 2023, 41, 1333–1338. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Takotsubo Syndrome | NSTEMI | Controls | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | 95% CI | Median | IQR | 95% CI | Median | IQR | 95% CI | p-Value | |
| Age (years) | 69 | 62–78 | 67–73 | 67 | 57–77 | 63–70 | 59 | 40–74 | 51–61 | 0.001 |
| BMI (kg/m2) | 25.1 | 21.8–29.2 | 24.1–26.9 | 27.8 | 25.6–30.4 | 27.1–29.8 | 26.2 | 23.5–28.5 | 25.4–27.8 | 0.018 |
| Creatinine (mg/dL) | 0.76 | 0.68–0.90 | 0.75–0.89 | 0.78 | 0.67–1.00 | 0.81–1.01 | 0.96 | 0.86–1.09 | 0.13–3.55 | <0.0001 |
| CRP (mg/dL) | 0.50 | 0.20–0.90 | 0.50–2.38 | 3.50 | 0.00–7.45 | 3.16–9.87 | 0.10 | 0.10–0.30 | 0.17–0.63 | <0.0001 |
| pBNP (ng/L) | 2866 | 665–4920 | 2623–4810 | 293 | 152–1142 | 375–1380 | 66 | 164–1466 | 95–1061 | <0.0001 |
| hsTnT (ng/L) | 162 | 53–395 | 207–392 | 678 | 131–1223 | 528–2373 | 6 | 5–14 | 8–12 | <0.0001 |
| EF (%) | 40 | 35–46 | 40–44 | 50 | 40–63 | 47–55 | 50 | 45–57 | 45–55 | 0.001 |
| % | n | % | n | % | N | p-value | ||||
| Atrial fibrillation | 9.8 | 5 | 13.3 | 6 | 1.9 | 1 | 0.097 | |||
| Sex (female) | 94.1 | 48 | 34.0 | 17 | 45.5 | 25 | <0.0001 | |||
| Diabetes | 5.9 | 3 | 23.3 | 10 | 14.5 | 8 | 0.056 | |||
| Hypertension | 74.5 | 38 | 86.0 | 43 | 54.5 | 30 | 0.001 | |||
| Smoker | 29.4 | 15 | 44.2 | 19 | 29.1 | 16 | 0.220 | |||
| NSTEMI | |||
| B | SE | p-value | |
| HSP70, z-score | −0.354 | 0.24 | 0.142 |
| pBNP, z-score | −1.579 | 0.54 | 0.003 |
| hsTnT, z-score | 5.477 | 1.07 | <0.0001 |
| Takotsubo Syndrome | |||
| B | SE | p-value | |
| HSP70 (pg/mL) | 0.634 | 0.22 | 0.004 |
| pBNP (pg/mL) | 2.216 | 0.57 | <0.0001 |
| hsTnT, z-score | −0.564 | 0.51 | 0.266 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demirel, O.; Paar, V.; Tolnai, P.; Topf, A.; Hoppe, U.C.; Lichtenauer, M.; Mirna, M. Heat Shock Protein 70 Constitutes a Promising Novel Biomarker in Differential Diagnosis between Takotsubo Syndrome and Non-ST-Segment Elevation Myocardial Infarction. J. Clin. Med. 2024, 13, 4152. https://doi.org/10.3390/jcm13144152
Demirel O, Paar V, Tolnai P, Topf A, Hoppe UC, Lichtenauer M, Mirna M. Heat Shock Protein 70 Constitutes a Promising Novel Biomarker in Differential Diagnosis between Takotsubo Syndrome and Non-ST-Segment Elevation Myocardial Infarction. Journal of Clinical Medicine. 2024; 13(14):4152. https://doi.org/10.3390/jcm13144152
Chicago/Turabian StyleDemirel, Ozan, Vera Paar, Philipp Tolnai, Albert Topf, Uta C. Hoppe, Michael Lichtenauer, and Moritz Mirna. 2024. "Heat Shock Protein 70 Constitutes a Promising Novel Biomarker in Differential Diagnosis between Takotsubo Syndrome and Non-ST-Segment Elevation Myocardial Infarction" Journal of Clinical Medicine 13, no. 14: 4152. https://doi.org/10.3390/jcm13144152
APA StyleDemirel, O., Paar, V., Tolnai, P., Topf, A., Hoppe, U. C., Lichtenauer, M., & Mirna, M. (2024). Heat Shock Protein 70 Constitutes a Promising Novel Biomarker in Differential Diagnosis between Takotsubo Syndrome and Non-ST-Segment Elevation Myocardial Infarction. Journal of Clinical Medicine, 13(14), 4152. https://doi.org/10.3390/jcm13144152