
The Impact of Gabapentinoids on Pain-Related Outcomes after Knee and Hip Surgery: A Systematic Review with Meta-Analysis of Randomized Controlled Trials

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
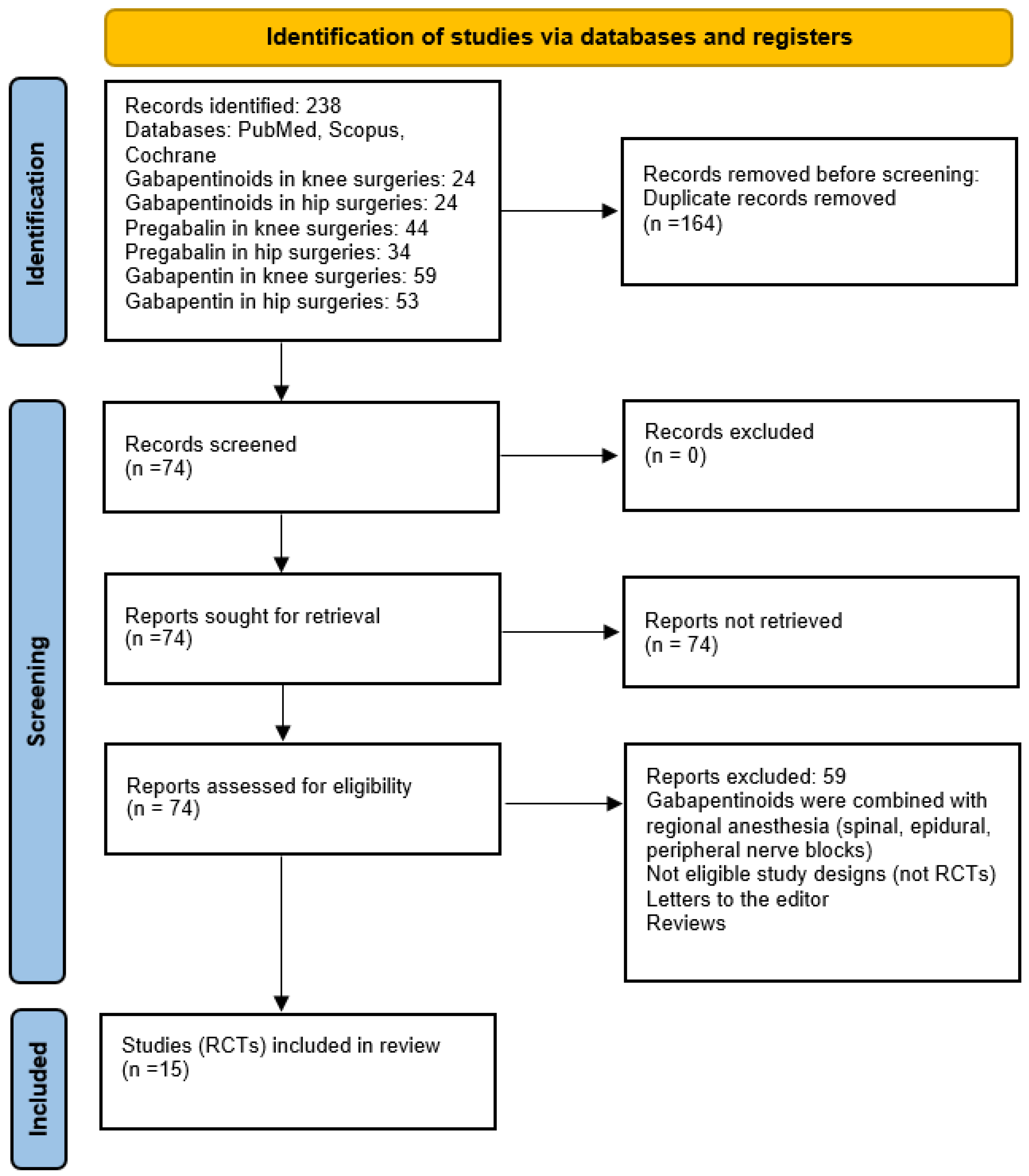
2.2. Search Strategy and Criteria
2.3. Screening
2.3.1. Inclusion Criteria
- Patients: Patients aged 18 years old and older undergoing knee or hip surgery (knee arthroplasty, total knee replacement, ligament repair; hip arthroplasty, hip replacement);
- Intervention: Analgesic use of gabapentinoids (pregabalin or gabapentin);
- Control: Placebo;
- Outcomes: Primary—acute postoperative pain intensity at rest and on movement; secondary—postoperative morphine consumption (mg), postoperative nausea and vomiting, chronic postoperative pain;
- Study design: Randomized controlled trials (RCTs).
2.3.2. Exclusion Criteria
- Pediatric studies;
- Other comparators;
- Non-RCTs: retrospective studies, case reports, case series, editorials, cadaver studies, and technical reports;
- Not properly described study methodology, assessment, and/or reporting methods;
- Inability to retract the full text.
2.4. Assessment of Methodologic Quality
2.5. Data Extraction and Statistical Methods
3. Results
3.1. Included Studies
3.2. Pain Intensity at Rest (0–10 Scale)
3.3. Pain Intensity Score on Movement (0–10 Scale)
3.4. Postoperative Opioid Consumption in Morphine Equivalents (mg)
3.5. Postoperative Nausea (n)
3.6. Postoperative Vomiting (n)
3.7. Subgroup Analysis for TKA and THA: Pain at Rest
3.8. Subgroup Analysis for TKA and THA: Pain on Movement
3.9. Quality Assessment
4. Discussion
4.1. Interpretations of Results
4.1.1. Pain
4.1.2. Opioid Consumption
4.1.3. Postoperative Nausea and Vomiting
4.1.4. Chronic Pain
4.2. Study Limitations
4.3. Implications for Research and Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fingar, K.R.; Stocks, C.; Weiss, A.J.; Steiner, C.A. Most Frequent Operating Room Procedures Performed in U.S. Hospitals, 2003–2012. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2006. [Google Scholar]
- Trousdale, R.T.; McGrory, B.J.; Berry, D.J.; Becker, M.W.; Harmsen, W.S. Patients’ Concerns Prior to Undergoing Total Hip and Total Knee Arthroplasty. Mayo Clin. Proc. 1999, 74, 978–982. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, C.J.; Pelt, C.E.; Gililland, J.M.; Peters, C.L. Perioperative Pain Management in Hip and Knee Arthroplasty. Orthop. Clin. N. Am. 2017, 48, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Joshi, G.P.; Ogunnaike, B.O. Consequences of Inadequate Postoperative Pain Relief and Chronic Persistent Postoperative Pain. Anesthesiol. Clin. N. Am. 2005, 23, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Clarke, H.; Pereira, S.; Kennedy, D.; Andrion, J.; Mitsakakis, N.; Gollish, J.; Katz, J.; Kay, J. Adding Gabapentin to a Multimodal Regimen Does Not Reduce Acute Pain, Opioid Consumption or Chronic Pain after Total Hip Arthroplasty. Acta Anaesthesiol. Scand. 2009, 53, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Halawi, M.J.; Vovos, T.J.; Green, C.L.; Wellman, S.S.; Attarian, D.E.; Bolognesi, M.P. Opioid-Based Analgesia: Impact on Total Joint Arthroplasty. J. Arthroplast. 2015, 30, 2360–2363. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, M.; Oderda, G.M.; Ashburn, M.A.; Lipman, A.G. Adverse Events Associated with Postoperative Opioid Analgesia: A Systematic Review. J. Pain 2002, 3, 159–180. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Iorio, R.; Specht, L.M.; Davies-Lepie, S.; Healy, W.L. Complications of Femoral Nerve Block for Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2010, 468, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Chung, K.-S.; Choi, C.H. The Effect of a Single Dose of Preemptive Pregabalin Administered with COX-2 Inhibitor: A Trial in Total Knee Arthroplasty. J. Arthroplast. 2015, 30, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Kremer, M.; Salvat, E.; Muller, A.; Yalcin, I.; Barrot, M. Antidepressants and Gabapentinoids in Neuropathic Pain: Mechanistic Insights. Neuroscience 2016, 338, 183–206. [Google Scholar] [CrossRef]
- Turan, A.; White, P.F.; Karamanlioglu, B.; Pamukçu, Z. Premedication with Gabapentin: The Effect on Tourniquet Pain and Quality of Intravenous Regional Anesthesia. Anesth. Analg. 2007, 104, 97–101. [Google Scholar] [CrossRef]
- Han, C.; Li, X.; Jiang, H.; Ma, J.; Ma, X. The Use of Gabapentin in the Management of Postoperative Pain after Total Knee Arthroplasty. Medicine 2016, 95, e3883. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Khuong, J.N.; Liu, Z.; Borg, C.; Jackson, S.; Ramson, D.M.; Kok, J.; Douglas, N.; Penny-Dimri, J.C.; Perry, L.A. Perioperative Gabapentinoid Use Lowers Short-Term Opioid Consumption Following Lower Limb Arthroplasty: Systematic Review and Meta-Analysis. J. Opioid Manag. 2021, 17, 251–272. [Google Scholar] [CrossRef] [PubMed]
- Hannon, C.P.; Fillingham, Y.A.; Browne, J.A.; Schemitsch, E.H.; Mullen, K.; Casambre, F.; Visvabharathy, V.; Hamilton, W.G.; Della Valle, C.J. The Efficacy and Safety of Gabapentinoids in Total Joint Arthroplasty: Systematic Review and Direct Meta-Analysis. J. Arthroplast. 2020, 35, 2730–2738.e6. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Schünemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE Guidelines: A New Series of Articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally Estimating the Sample Mean from the Sample Size, Median, Mid-Range, and/or Mid-Quartile Range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Paul, J.E.; Nantha-Aree, M.; Buckley, N.; Cheng, J.; Thabane, L.; Tidy, A.; DeBeer, J.; Winemaker, M.; Wismer, D.; Punthakee, D.; et al. Gabapentin Does Not Improve Multimodal Analgesia Outcomes for Total Knee Arthroplasty: A Randomized Controlled Trial. Can. J. Anaesth. 2013, 60, 423–431. [Google Scholar] [CrossRef]
- Carmichael, N.M.E.; Katz, J.; Clarke, H.; Kennedy, D.; Kreder, H.J.; Gollish, J.; McCartney, C.J.L. An Intensive Perioperative Regimen of Pregabalin and Celecoxib Reduces Pain and Improves Physical Function Scores Six Weeks after Total Hip Arthroplasty: A Prospective Randomized Controlled Trial. Pain Res. Manag. 2013, 18, 127–132. [Google Scholar] [CrossRef]
- Paul, J.E.; Nantha-Aree, M.; Buckley, N.; Shahzad, U.; Cheng, J.; Thabane, L.; Tidy, A.; DeBeer, J.; Winemaker, M.; Wismer, D.; et al. Randomized Controlled Trial of Gabapentin as an Adjunct to Perioperative Analgesia in Total Hip Arthroplasty Patients. Can. J. Anaesth. 2015, 62, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A.F.; Moura, E.C.R.; Honda, C.A.D.O.; Pereira, E.C.; de Oliveira, C.M.B.; Leal, P.D.C.; Sakata, R.K. Evaluation of the Efficacy of Prolonged Pregabalin Administration Before and After Surgery in Patients Undergoing Arthroscopic Anterior Cruciate Ligament Repair: A Prospective, Randomized, Double-Blind Study. Clin. J. Pain 2020, 36, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, O.; Jacobsen, L.S.; Holm, H.E.; Randall, S.; Adamiec-Malmstroem, L.; Graungaard, B.K.; Holst, P.E.; Hilsted, K.L.; Dahl, J.B. Pregabalin and Dexamethasone for Postoperative Pain Control: A Randomized Controlled Study in Hip Arthroplasty. Br. J. Anaesth. 2008, 101, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, M.L.; Mathiesen, O.; Dierking, G.; Christensen, B.V.; Hilsted, K.L.; Larsen, T.K.; Dahl, J.B. Multimodal Analgesia with Gabapentin, Ketamine and Dexamethasone in Combination with Paracetamol and Ketorolac after Hip Arthroplasty: A Preliminary Study. Eur. J. Anaesthesiol. 2010, 27, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Jolly, A.; Bholla, V.; Adatia, S.; Sood, J. Evaluation of Efficacy of Oral Pregabalin in Reducing Postoperative Pain in Patients Undergoing Total Knee Arthroplasty. Indian J. Orthop. 2012, 46, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Martinez, V.; Cymerman, A.; Ben Ammar, S.; Fiaud, J.F.; Rapon, C.; Poindessous, F.; Judet, T.; Chauvin, M.; Bouhassira, D.; Sessler, D.; et al. The Analgesic Efficiency of Combined Pregabalin and Ketamine for Total Hip Arthroplasty: A Randomised, Double-Blind, Controlled Study. Anaesthesia 2014, 69, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Yik, J.H.; Tham, W.Y.W.; Tay, K.H.; Shen, L.; Krishna, L. Perioperative Pregabalin Does Not Reduce Opioid Requirements in Total Knee Arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2104–2110. [Google Scholar] [CrossRef] [PubMed]
- Singla, N.K.; Chelly, J.E.; Lionberger, D.R.; Gimbel, J.; Sanin, L.; Sporn, J.; Yang, R.; Cheung, R.; Knapp, L.; Parsons, B. Pregabalin for the Treatment of Postoperative Pain: Results from Three Controlled Trials Using Different Surgical Models. J. Pain Res. 2015, 8, 9–20. [Google Scholar] [CrossRef] [PubMed]
- YaDeau, J.T.; Lin, Y.; Mayman, D.J.; Goytizolo, E.A.; Alexiades, M.M.; Padgett, D.E.; Kahn, R.L.; Jules-Elysee, K.M.; Ranawat, A.S.; Bhagat, D.D.; et al. Pregabalin and Pain after Total Knee Arthroplasty: A Double-Blind, Randomized, Placebo-Controlled, Multidose Trial. Br. J. Anaesth. 2015, 115, 285–293. [Google Scholar] [CrossRef]
- Buvanendran, A.; Kroin, J.S.; Della Valle, C.J.; Kari, M.; Moric, M.; Tuman, K.J. Perioperative Oral Pregabalin Reduces Chronic Pain after Total Knee Arthroplasty: A Prospective, Randomized, Controlled Trial. Anesth. Analg. 2010, 110, 199–207. [Google Scholar] [CrossRef]
- Clarke, H.; Pagé, G.M.; McCartney, C.J.L.; Huang, A.; Stratford, P.; Andrion, J.; Kennedy, D.; Awad, I.T.; Gollish, J.; Kay, J.; et al. Pregabalin Reduces Postoperative Opioid Consumption and Pain for 1 Week after Hospital Discharge, but Does Not Affect Function at 6 Weeks or 3 Months after Total Hip Arthroplasty. Br. J. Anaesth. 2015, 115, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Ma, J.; Kuang, M.; Jiang, X.; Wang, Y.; Lu, B.; Zhao, X.; Sun, L.; Ma, X. The Efficacy of Pregabalin for the Management of Postoperative Pain in Primary Total Knee and Hip Arthroplasty: A Meta-Analysis. J. Orthop. Surg. Res. 2017, 12, 49. [Google Scholar] [CrossRef] [PubMed]
- Verret, M.; Lauzier, F.; Zarychanski, R.; Perron, C.; Savard, X.; Pinard, A.-M.; Leblanc, G.; Cossi, M.-J.; Neveu, X.; Turgeon, A.F.; et al. Perioperative Use of Gabapentinoids for the Management of Postoperative Acute Pain: A Systematic Review and Meta-Analysis. Anesthesiology 2020, 133, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Evoy, K.E.; Peckham, A.M.; Covvey, J.R.; Tidgewell, K.J. Gabapentinoid Pharmacology in the Context of Emerging Misuse Liability. J. Clin. Pharma 2021, 61, S89–S99. [Google Scholar] [CrossRef]
- Mao, Y.; Wu, L.; Ding, W. The Efficacy of Preoperative Administration of Gabapentin/Pregabalin in Improving Pain after Total Hip Arthroplasty: A Meta-Analysis. BMC Musculoskelet. Disord. 2016, 17, 373. [Google Scholar] [CrossRef]
- Laigaard, J.; Pedersen, C.; Rønsbo, T.N.; Mathiesen, O.; Karlsen, A.P.H. Minimal Clinically Important Differences in Randomised Clinical Trials on Pain Management after Total Hip and Knee Arthroplasty: A Systematic Review. Br. J. Anaesth. 2021, 126, 1029–1037. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country, Study Design | Study Goals | Age | N of Patients: Total (Intervention/Control) | Surgery; Groups | Type of Pain; ASA Status | Dose Regiment | Study Conclusions |
|---|---|---|---|---|---|---|---|
| Buvanendran et al., 2010 [31] USA, RCT | To determine if pregabalin has analgesic effects given preoperatively | 64 (8.3), 63.3 (8.9) | 240 (120/120) | TKA; pregabalin, placebo | Neuropathic pain; I, II, III | Pregabalin 300 mg orally | Perioperative pregabalin reduces the incidence of chronic neuropathic pain |
| Carmichael et al., 2013 [21], Canada, RCT | To assess pain (VAS, 0–10), morphine use, physical function, adverse events | 18–80 pregabalin: 59.1 (10.1) placebo: 61.3 (15.1) | R: 47 (23/24) A: 31 (15/16) | THA; pregabalin, placebo | I–III | Pregabalin 75 mg twice daily, celecoxib 100 mg twice daily, 14 d preop, 2 h preop, during hospitalization, and 3 w after discharge | Pregabalin and celecoxib improves pain and physical function |
| Clarke et al., 2009 [5], Canada, RCT | To determine if gabapentin reduces pain and opioid use and find the efficient time of consumption | 61.3 (10.7), 58.9 (9.4), 60.4 (8.1) | 126 (42/42/42) | THA; gabapentin 600 mg/placebo, placebo/gabapentin 600 mg, placebo/placebo | Neuropathic pain | Gabapentin before surgery 19.06 ± 19.9 mg, after surgery 34.8 ± 13.1 mg in the first 24 h | No effect from gabapentin on morphine consumption or pain scores preoperatively/postoperatively |
| Clarke et al., 2015 [32], Canada, RCT | To study the effects of pregabalin on pain and functional outcomes | 60.1 (8.8), 60.2 (9.5) | 184 (92/92) | THA; pregabalin, placebo | Neuropathic pain; I, II, III | Pregabalin 150 mg p.o | No improvement in physical function |
| Jain et al., 2012 [26], India, RCT | To evaluate pain at rest and on movement (VRS, 0–10), morphine use, rescue analgesic use, patient satisfaction, sedation, adverse events | 18–75 pregabalin: 59.7 (8.63) placebo: 57.1 (8.81) | 40 (20/20) | TKA; pregabalin, placebo | I, II | Pregabalin 75 mg twice a day 2 h preop; 2 d postop | Pregabalin reduces opioid use, improves postop analgesia, and yields higher patient satisfaction |
| Martinez et al., 2014 [27], France, RCT | To assess pain at rest and on movement (NRS, 0–10), morphine use, side effects, pressure pain thresholds, secondary hyperalgesia | 18–80 placebo: 64 (11) ketamine: 60 (17) pregabalin: 64 (9) ketamine + pregabalin: 59 (12) | 142 (38/34/35/35) (placebo/ketamine/pregabalin/ketamine + pregabalin) | THA; placebo; ketamine; pregabalin; ketamine + pregabalin | I–III | Pregabalin 150 mg preop | The combination of pregabalin and ketamine has a small, beneficial clinical effect |
| Mathiesen et al., 2008 [24], Denmark, RCT | To examine morphine use, pain at rest and during mobilization (VAS, 0–100), PONV, sedation, dizziness, and ondansetron use | 55–75 placebo: 66 (63–71) pregabalin: 67 (62–71) pregabalin + dexamethasone: 68 (64–71) median (range) | R: 126 (42/42/42) A: 120 (38/40/42) (placebo/pregabalin/pregabalin + dexamethasone) | THA; placebo, pregabalin, pregabalin + dexamethasone | I–III | Pregabalin 300 mg 1 h preop | Pregabalin reduced postop morphine use. This was not associated with a reduced PONV. Pregabalin resulted in increased sedation. Pregabalin and dexamethasone provided no effects on pain or opioid use |
| Lee et al., 2015 [9], Korea, RCT | To study the postoperative pain, analgesic drug consumption, and functional outcomes after pregabalin | Pregabalin: 63.38 (10.71), placebo: 67.60 (8.98) | 87 (45/42) | TKA; pregabalin, control | Neuropathic pain; I, II, III | 400 mg celecoxib plus 150 mg pregabalin—1 h prior to the operation | No difference between the two groups in functional recovery |
| Paul et al., 2013 [20], Canada, RCT | To assess morphine use, pain (NRS, 0–10) at rest and movement, side effects, patient satisfaction, knee ROM, hemodynamics | 19–90 gabapentin: 62.1 (6.4) placebo: 63.5 (6.7) | 101 (52/49) | TKA; gabapentin, placebo | I–IV | 600 mg gabapentin 2 h preop; 8 h for 2 postop days | No effect on postoperative morphine consumption, pain, patient satisfaction, or length of hospital stay |
| Paul et al., 2015 [22], Canada, RCT | To determine if gabapentin preoperatively or postoperatively would decrease postoperative morphine consumption | 60.9 (9.1), 60.5 (8.5) | 102 (48/54) | THA; gabapentin, placebo | Neuropathic pain | 600 mg of gabapentin | No difference between placebo in morphine consumption, side effects, or pain scores |
| Rasmussen et al., 2010 [25], Denmark, RCT | To assess morphine use, pain at rest and during mobilization (VAS, 0–100), PONV, sedation, dizziness, hallucination, and ondansetron use | 55–85 gabapentin: 72 (68–77) placebo: 70 (67–75) median (IQR) | 42 (24/18) | THA; gabapentin, placebo | I–III | 1200 mg gabapentin preop | Preop gabapentin, reduced pain, but not morphine use |
| Singla et al., 2014 [29], USA, RCT | To assess pain (0–10), knee ROM, opioid use, safety | 18–80 150 mg: 63 (8.5) 300 mg: 63.7 (8.3) placebo: 63.3 (9.5) | 292 (98/96/98) (150 mg/300 mg/placebo) | TKA; pregabalin 150, pregabalin 300, placebo | 150 mg pregabalin (75 mg bid) or 300 mg pregabalin (150 mg bid) 12 h and 2 h preop, 6 w postop | No significant differences between pregabalin and placebo | |
| Tobias et al., 2019 [23], Brazil, RCT | To determine if preoperative and postoperative pregabalin is associated with a reduction in postoperative pain episodes | Pregabalin: 31 (7), placebo: 30 (7) | 50 (25/25) | Knee ligament repair; pregabalin, control | Neuropathic pain; I or II | Pregabalin, 75 mg/d 7 days before and 7 days after surgery | Pregabalin decreased the consumption of analgesics with side effects of dizziness |
| Yadeau et al., 2015 [30], USA, RCT | To determine if postoperative pain could be reduced and to determine the side effects | 66 (34–79) | 120 (30/30/30/30) | TKA; placebo, pregabalin 50 mg, pregabalin 100 mg, pregabalin 150 mg | Neuropathic pain; I–III | 0, 50, 100, and 150 mg pregabalin | No analgesic effect of pregabalin; side effects—reduced satisfaction with analgesia and increased drowsiness |
| Yik et al., 2019 [28], Singapore, RCT | To determine if pregabalin preoperatively with PCA morphine, paracetamol, and etoricoxib is effective for decreasing the morphine and if it decreases the pain scores | Pregabalin: 65.1 (50–80), placebo: 66.6 (50–83) | 87 (45/42) | TKA; pregabalin, control | I, II, III | 1 h before surgery: 75 mg pregabalin orally; 48 h after surgery: 75 mg dose per night | No effect on postoperative opioid dose, pain scores, or functional outcomes |
| Study Reference | D1 | D2 | D3 | D4 | D5 | Overall | ||
|---|---|---|---|---|---|---|---|---|
| YaDeau et al., 2015 [30] |  |  |  |  |  |  |  | Low risk |
| Buvanendran et al., 2010 [31] |  |  |  |  |  |  |  | Some concerns |
| Clarke et al., 2009 [5] |  |  |  |  |  |  |  | High risk |
| Paul et al., 2015 [22] |  |  |  |  |  |  | ||
| Clarke et al., 2015 [32] |  |  |  |  |  |  | D1 | Randomization process |
| Tobias et al., 2019 [23] |  |  |  |  |  |  | D2 | Deviations from the intended interventions |
| Yik et al., 2019 [28] |  |  |  |  |  |  | D3 | Missing outcome data |
| Lee et al., 2015 [9] |  |  |  |  |  |  | D4 | Measurement of the outcome |
| Paul et al., 2013 [20] |  |  |  |  |  |  | D5 | Selection of the reported result |
| Jain et al., 2012 [26] |  |  |  |  |  |  | ||
| Martinez et al., 2014 [27] |  |  |  |  |  |  | ||
| Singla et al., 2014 [29] |  |  |  |  |  |  | ||
| Carmichael et al., 2014 [21] |  |  |  |  |  |  | ||
| Mathiesen et al., 2008 [24] |  |  |  |  |  |  | ||
| Rasmussen et al., 2010 [25] |  |  |  |  |  |  |
| Outcome | Study Design | N of Patients (Studies) | Mean Difference/Relative Risk [95% CI] | Certainty of Evidence (GRADE) |
|---|---|---|---|---|
| Overall pain scores at rest (0–10) | RCT | 1868 (11) | −0.30 [−0.55, −0.05] | ⨁⨁⨁◯ Moderate |
| Overall pain scores on movement (0–10) | RCT | 1415 (8) | −0.41 [−0.68, −0.13] | ⨁⨁⨁◯ Moderate |
| Overall postoperative opioid use in morphine equivalent (mg) | RCT | 2081 (12) | −6.42 [−9.07, −3.78] | ⨁⨁⨁◯ Moderate |
| Overall postoperative nausea | RCT | 1471 (11) | 0.69 [0.55, 0.86] | ⨁⨁⨁⨁ High |
| Overall postoperative vomiting | RCT | 1173 (11) | 0.72 [0.46, 1.14] | ⨁⨁⨁⨁ High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viderman, D.; Aubakirova, M.; Salamat, A.; Kaldybayev, D.; Sadir, N.; Tankacheyev, R.; Abdildin, Y.G. The Impact of Gabapentinoids on Pain-Related Outcomes after Knee and Hip Surgery: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2024, 13, 4205. https://doi.org/10.3390/jcm13144205
Viderman D, Aubakirova M, Salamat A, Kaldybayev D, Sadir N, Tankacheyev R, Abdildin YG. The Impact of Gabapentinoids on Pain-Related Outcomes after Knee and Hip Surgery: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2024; 13(14):4205. https://doi.org/10.3390/jcm13144205
Chicago/Turabian StyleViderman, Dmitriy, Mina Aubakirova, Azamat Salamat, Dastan Kaldybayev, Nurzhamal Sadir, Ramil Tankacheyev, and Yerkin G. Abdildin. 2024. "The Impact of Gabapentinoids on Pain-Related Outcomes after Knee and Hip Surgery: A Systematic Review with Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 13, no. 14: 4205. https://doi.org/10.3390/jcm13144205
APA StyleViderman, D., Aubakirova, M., Salamat, A., Kaldybayev, D., Sadir, N., Tankacheyev, R., & Abdildin, Y. G. (2024). The Impact of Gabapentinoids on Pain-Related Outcomes after Knee and Hip Surgery: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine, 13(14), 4205. https://doi.org/10.3390/jcm13144205